
Abstract
The aim of this study is to investigate death anxiety (DA) and related factors among critical care nurses. Using a cross-sectional research design, 325 critical care nurses in eight hospitals in Iran enrolled in the study. Multiple logistic regression analysis showed that deputy head nurse (OR = 18.299; CI: 1.764–189.817; p = .015), shift morning fixed (OR = 8.061; CI: 1.503–43.243; p = .015), surviving parents (OR = 3.281; CI: 1.072–10.037; p = .037), number of children (OR = 1.866; CI: 1.157–3.010; p = .011), years of working experience (OR = 1.143; CI: 1.048–1.246; p = .003), number of end-of-life patient care in the last 3 months (OR = .900; CI: .828–0.977; p = .012), age (OR = .809; CI: .732–.893; p < .001), CCU nurses (OR = .250; CI: .100–.628; p = .003), and mild stressful life events (SLEs) (OR = .167; CI: .046–.611; p = .007) were significantly related to high DA. Therefore, nurse managers and policymakers should pay special attention to these related factors in developing programs to maintain and promote the health of critical care nurses to improve the quality of nursing care.
Introduction
Death is a biological and inevitable phenomenon that causes different reactions in individuals (Arab et al., 2019; Betriana & Kongsuwan, 2020). The thought of death can have adverse psychological effects on people’s lives. Stress and fear caused by thoughts of death and the process of dying can lead a type of anxiety called death anxiety (DA). DA is defined in the nursing outcomes classification guide as “a vague, uneasy feeling of discomfort or dread generated by perceptions of a real or imagined threat to one’s existence” (Sharif Nia et al., 2020).
Critical care nurses experience higher DA levels due to their close association with critically ill and dying patients and their professional roles for critically ill individuals (Jang et al., 2019). A study found that nurses experience high levels of DA, with a score of 4.15 out of 7 (Kagan, 2020). Another study showed that 36 and 39% of critical care nurses perceive moderate to severe DA levels, respectively (Dadgari et al., 2015). In addition, 68.7% of Iranian critical care nurses suffer from high levels of DA (Moudi et al., 2017). Perceptions of high levels of DA among nurses can lead to adverse outcomes such as poor communication between the nurse and the patient, reduced quality of nursing care (Peters et al., 2013) and patients’ quality of life (Zhang et al., 2019). Therefore, identifying DA and the related factors in critical care nurses is very important because of the potential impact on patients’ health consequences. As a result, there is a positive association between perceived stress and DA (Abdollahi et al., 2019; Sharif Nia et al., 2020). The scoping review results showed that some individual-social factors such as age, sex, and religiosity are associated with DA in nurses (Pandya & Kathuria, 2021). In addition, previous experiences with death, work experience in palliative care, and religion can influence attitudes toward death (Deffner & Bell, 2005). Also, DA is influenced by attitudes toward death, religiosity, and religious coping strategies that can vary in different societies and cultures (Pandya & Kathuria, 2021).
To the best of our knowledge, limited literature has specifically addressed DA among critical care nurses (Dadgari et al., 2015; Kagan, 2020; Peters et al., 2013). Assessment of DA and related factors such as perceived stress among critical care nurses is essential for planning their mental health. Therefore, the aim of this study is to investigate DA and related factors among critical care nurses.
Methods
Study Design and Subjects
Using a cross-sectional research design, 325 out of 386 critical care nurses working in ICU, CCU, emergency, and dialysis wards in eight hospitals in Iran enroll in the study. Data were collected using census sampling from June to September 2020. Inclusion criteria included at least six months of work experience in the above wards, while participants who did not consent to participate in the study were excluded.
The Research Ethics Committee of XXX University of Medical Sciences approved this research. The purpose of the study was explained to the participants. After obtaining informed consent, the nurses completed the questionnaires in a private room without a research team. In order to ensure the confidentiality of the information, the surnames of the participants were removed from the questionnaires.
Questionnaires and Data Collection
Data were collected using a three-part questionnaire including demographic characteristics, the Persian version of Death Anxiety Scale-Extended (DAS-E), and the Social Readjustment Rating Scale (SRRS).
Nurses who consented to participate in the study were asked about demographic characteristics such as age, sex, marital status, level of education, number of children, surviving parents, type of ward, years of working experiences as a nurse, and years of working experience in current wards. Other demographic data collected included organizational position, type of shift, number of patients monitored per shift, number of direct contributions to cardiopulmonary resuscitation (CPR) in the last 3 months, number of end-of-life patients cared for in the last 3 months, and the number of deaths observed in the last 3 months.
DAS-E consists of 51 items in the form of self-report. Participants responded to each tool item on a five-point Likert scale from strongly disagree (1) to strongly agree (5). In calculating the total score, the scores of negative items (2, 5, 6, 7, and 15) were reversed. The minimum and maximum scores in this questionnaire were 51 and 255, respectively. Higher scores indicate higher death anxiety (Templer et al., 2006). DAS-E internal consistency in Iran was confirmed by Soleimani et al. (2016). In the present study, the tool was confirmed using a pilot study of 30 critical care nurses with a Cronbach’s alpha of .86.
The SRRS was designed to assess stressful life events (SLEs) over the past year (Holmes & Rahe, 1967). This scale includes 41 events with intensities of 0 to 100 for each event. This scale is scored at stress levels: very low (0–149), mild (150–199), moderate (200–299), and severe (above 300). In the study of Rezakhani, this tool was confirmed with Cronbach’s alpha of .79–.97 (Rezakhani, 2011).
Statistical analysis
The SPSS software package (version 16.0, SPSS Inc, Chicago, IL, USA) was used to analyze the data. Quantitative and qualitative variables were presented via mean (standard deviation) and frequency (percentage). Kolmogorov–Smirnov test was used to evaluate the normality of DA score. Kruskal–Wallis and Mann–Whitney U tests were used to compare DA scores according to individual and occupational characteristics in participants. Kruskal–Wallis test was used to compare DA according to the severity of SLEs. Multiple Logistic Regression test (Enter method) was also used to assess the factors associated with DA. The multicollinearity was assessed by calculating collinearity diagnostics using tolerance and variance inflation factor (VIF). A tolerance<.1 and/or VIF >5 indicates a multicollinearity problem. All variables were included in logistic regression analysis. The 95% confidence interval (CI) was used to estimate the precision of odds ratios (OR). A large CI indicates low OR precision and a small CI indicates high OR accuracy. The significance level was considered less than .05.
Results
Participants
Individual and occupational characteristics of participants and their relationship with death anxiety (N = 325).
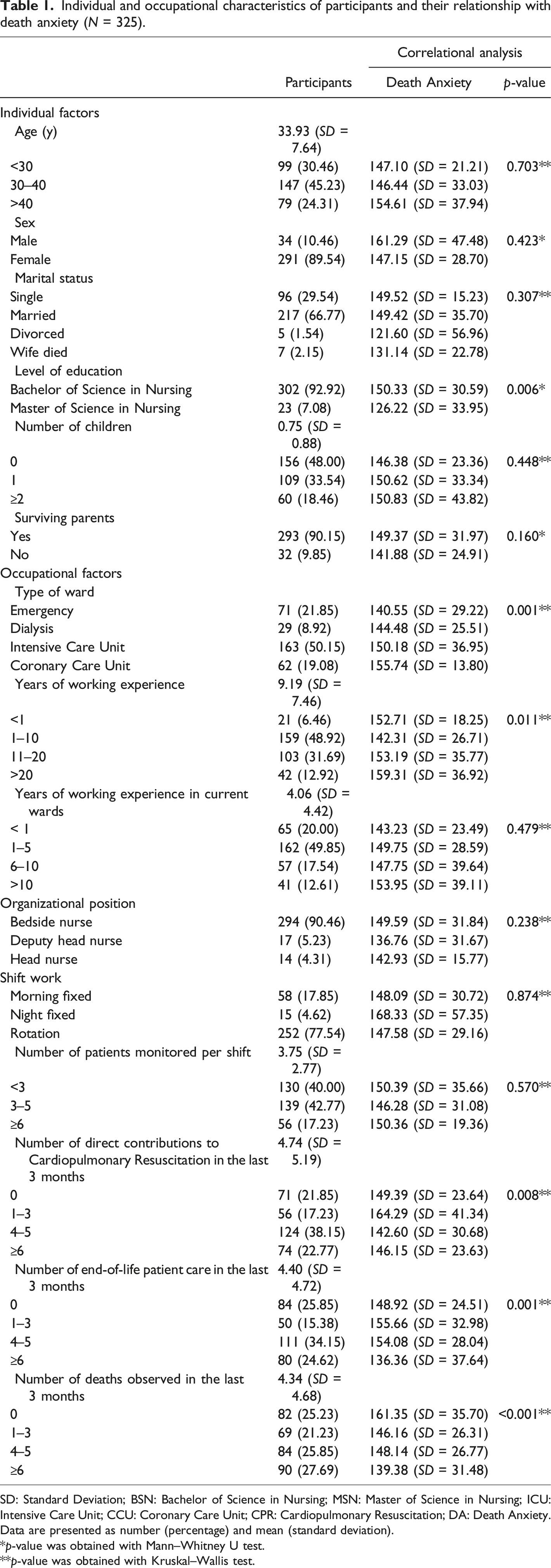
SD: Standard Deviation; BSN: Bachelor of Science in Nursing; MSN: Master of Science in Nursing; ICU: Intensive Care Unit; CCU: Coronary Care Unit; CPR: Cardiopulmonary Resuscitation; DA: Death Anxiety.
Data are presented as number (percentage) and mean (standard deviation).
*p-value was obtained with Mann–Whitney U test.
**p-value was obtained with Kruskal–Wallis test.
Death Anxiety and Stressful Life Events Among critical Care nurses
Death anxiety and the severity of stressful life events of participants (N = 325).
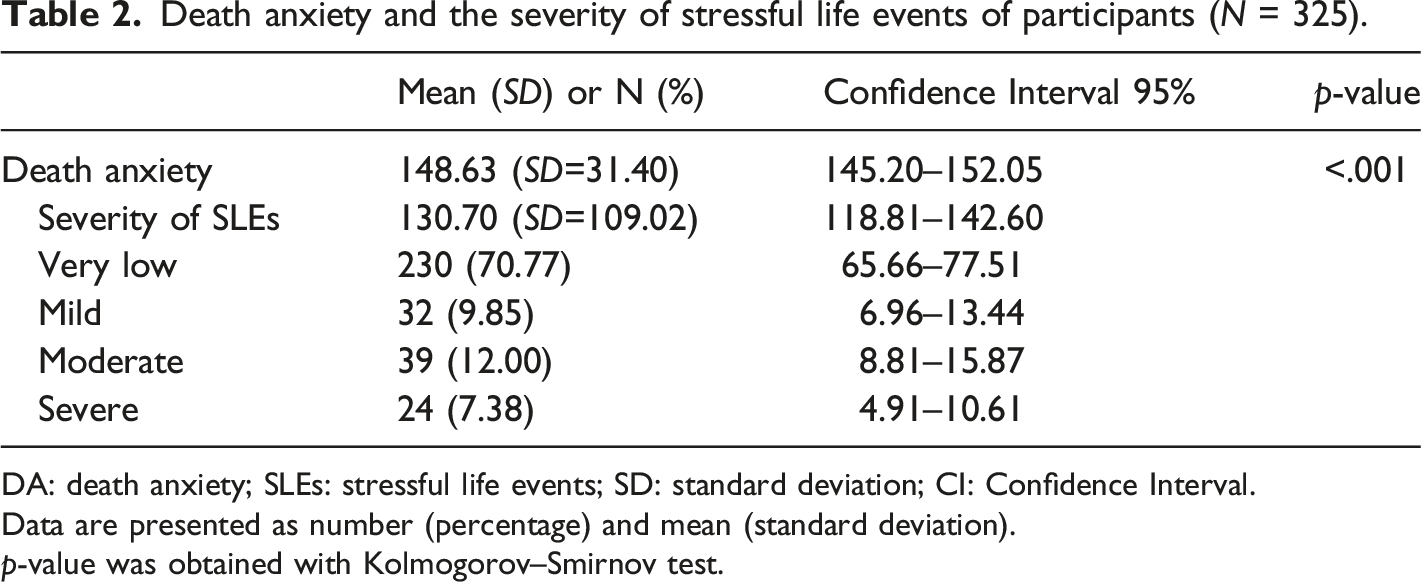
DA: death anxiety; SLEs: stressful life events; SD: standard deviation; CI: Confidence Interval.
Data are presented as number (percentage) and mean (standard deviation).
p-value was obtained with Kolmogorov–Smirnov test.
Death anxiety according to the severity of stressful life events (N=325).
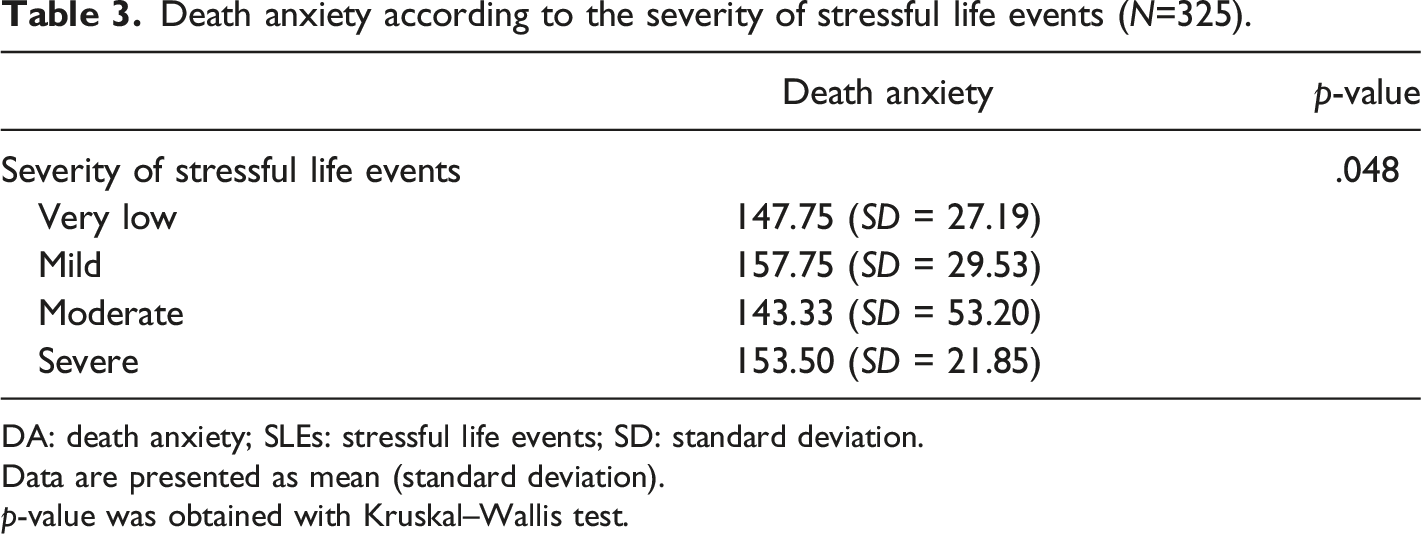
DA: death anxiety; SLEs: stressful life events; SD: standard deviation.
Data are presented as mean (standard deviation).
p-value was obtained with Kruskal–Wallis test.
Death Anxiety and Its Relationship With Individual and Occupational Variables
Table 1 shows the relationship between DA and individual and occupational variables. Nurses with a BSN degree had a higher DA than nurses with an MSN degree (p = .006). CCU nurses had higher DA than others (p = .001). Nurses with more than 20 years of work experience had a higher DA than others (p = .011). Nurses who did not see any deaths in the last three months had a higher DA than others (p < .001). There was also a significant relationship between DA and the number of direct contributions to CPR in the last 3 months (p = .008) and the number of end-of-life patient care in the last 3 months (p = .001).
Factors Associated With Death Anxiety of Critical Care Nurses
Factors associated with DA of critical care nurses (N = 325).
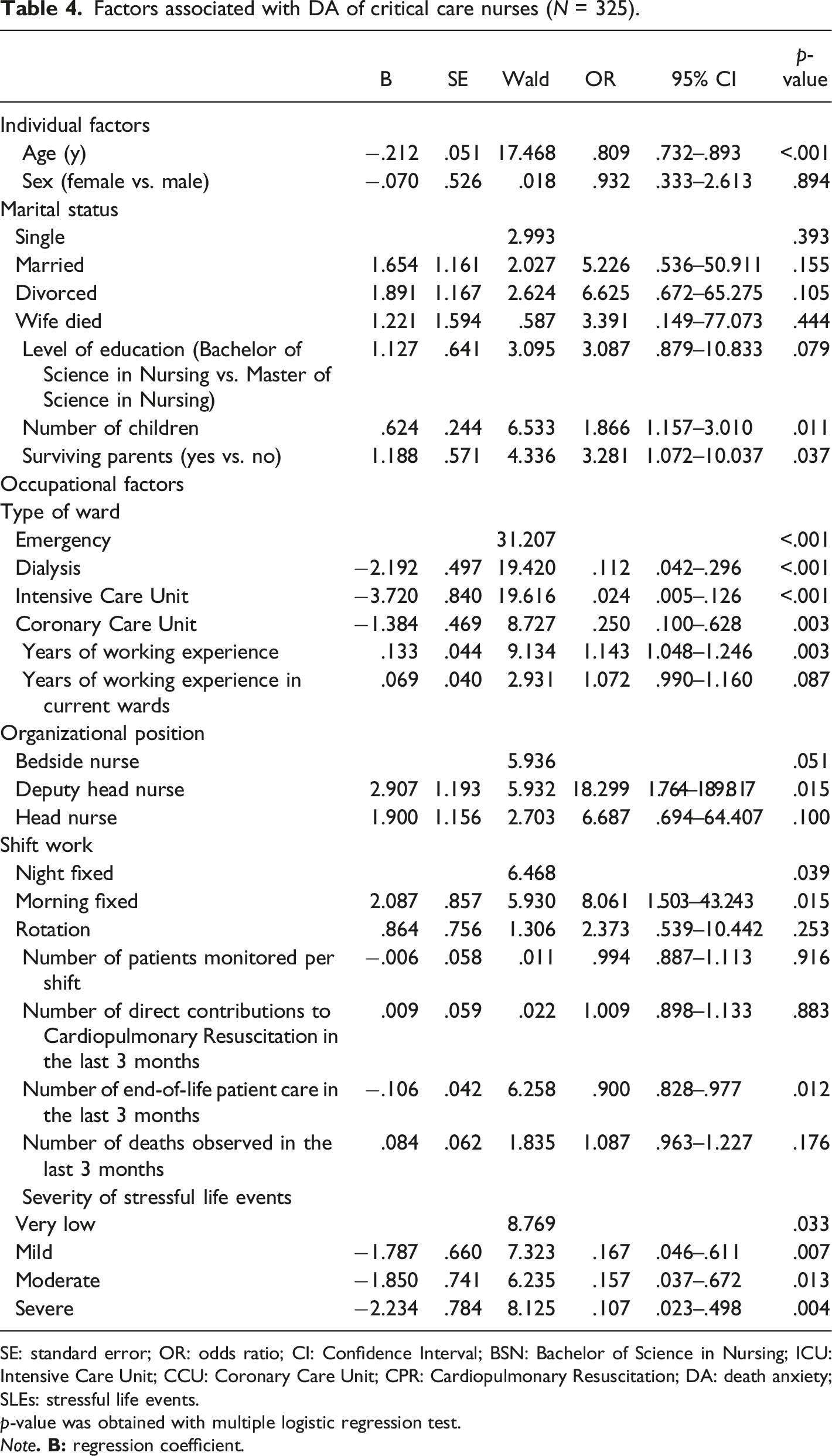
SE: standard error; OR: odds ratio; CI: Confidence Interval; BSN: Bachelor of Science in Nursing; ICU: Intensive Care Unit; CCU: Coronary Care Unit; CPR: Cardiopulmonary Resuscitation; DA: death anxiety; SLEs: stressful life events.
p-value was obtained with multiple logistic regression test.
Note
Discussion
Findings indicated that critical care nurses had a moderate level of DA. Multiple logistic regression analysis revealed that deputy head nurse, shift morning fixed, surviving parents, the number of children, years of working experience, number of end-of-life patient care in the last 3 months, age, CCU nurses, and mild SLEs were significantly related to high DA.
The present study results showed that the level of DA in critical care nurses was moderate. Published studies are minimal concerning DA among critical care nurses. Another study in Iran showed that 36 and 39% of critical care nurses perceive moderate and severe DA levels, respectively (Dadgari et al., 2015). In addition, 68.7% of Iranian critical care nurses suffer from high levels of DA (Moudi et al., 2017). Nurses, especially critical care nurses as crucial members of health care workers who spend the most time with patients, may be more exposed to DA due to the stress of caring for dying patients (McKenzie & Brown, 2017; Nia et al., 2016). Nurses may be at higher risk of DA due to a lack of preparation to communicate effectively with dying patients and their families (Betriana & Kongsuwan, 2019; Parola et al., 2018). Lack of human resources, continuous shifts, and the high workload of critical care nurses can be mentioned as possible reasons for the high perception of DA among critical care nurses (Hassanzadeh et al., 2017). There have been few studies comparing DA in ICU nurses and nurses in other hospital wards, so it is recommended that future studies be performed to compare DA in ICU and other ward nurses.
Multiple logistic regression analysis showed that individual factors such as surviving parents, number of children, and age were significantly related to high DA. The present study showed that having surviving parents is a strong predictor of DA among critical care nurses, an apparent discrepancy with the findings in (Dadgari et al., 2015). This discrepancy may be due to individual differences among nurses, such as marital status, number of children, culture, and religion (Xu et al., 2019). The number of children was another predictor of DA among critical care nurses in this study. Consistent with this finding, a study in Turkey (Sahin et al., 2017) found that female critical care nurses who had children experience more DA. Inconsistent with this finding, a study in Iran (Dadgari et al., 2015) showed that there is no significant relationship between the DA of critical care nurses and individual variables. In fact, critical care units are often stressful. On the other hand, nurses who have children are under the stress of caring for the child and protecting them from trauma and mortality, which can impose DA on these nurses at higher levels (Sahin et al., 2017). Individual differences among nurses, such as marital status and the number and gender of children may be the causes of these contradictions (Dadgari et al., 2015; Pandya & Kathuria, 2021). Age was a predictor of DA among critical care nurses in the present study. Consistent with this finding, a study in the United States found that aging is directly related to DA (Black, 2007), which may be due to older nurses thinking more about death (Kuru Alıcı et al., 2018).
In contrast, another study in the United States showed an inverse relationship between age and DA (Deffner & Bell, 2005). Differences in sample size, tools, religion, and different views of death may affect this relationship (Arab et al., 2019; Black, 2007). On the other hand, psychological maturity due to aging can be another reason for the inverse relationship between age and DA (Taywade, 2018).
Multiple logistic regression analysis showed that occupational factors such as deputy head nurse, shift morning fixed, years of working experience, the number of end-of-life patient care in the last 3 months, CCU nurses, and mild SLEs were significantly related to high DA. In the present study, organizational positions were predictors of DA among critical care nurses, where deputy head nurses were significantly related to high DA. This finding was not supported by a previous study in Iran (Dadgari et al., 2015). The contradiction can be due to differences in attitudes toward death, religiosity, and religious coping strategies. In this study, shift morning fixed was another predictor of DA among critical care nurses. This finding may be due to the higher occurrence of mortality and CPR during morning shifts (Ni et al., 2019). Years of working experience were another predictor of DA among critical care nurses in the present study due to a more negative attitude toward death among nurses with higher work experience. There is a direct relationship between negative attitudes toward death and DA, which this factor was not assessed in the present study (Wang et al., 2018).
In contrast with this finding, studies in Iran (Arab et al., 2019) and Turkey (Sahin et al., 2017) showed no relationship between work experience and DA among critical care nurses. Also, the results of a study in the United States (Dunn et al., 2005) showed that nurses with more work experience in caring for dying patients had lower DAs than less experienced nurses. In order to explain this discrepancy, it can be concluded that work experience is associated with aging and older people are more prone to DA. However, if a person succeeds in using adaptive mechanisms to deal with DA, that person will have less DA (Nia et al., 2016). Numerous factors such as culture, religion, and education can influence attitudes and perceptions of death and DA (Pandya & Kathuria, 2021). In this study, the attitude to death was not assessed. Therefore, it is suggested as a focus to be considered in future studies. Another predictor of DA in this study was the number of end-of-life patient care in the last three months. The results of a systematic review showed that adequate experience of end-of-life patient care and palliative care and participation in more direct contributions to CPR is associated with lower DA in nurses. Also, the end-of-life patient care experience is usually more in critical care units, and finally, the DA of critical care nurses is high (Nia et al., 2016). In the present study, the type of ward was a predictor of DA among critical care nurses, where CCU nurses were significantly related to high DA. Nurses working in the CCU and ICU are more likely to associate with patients with more critical conditions. On the other hand, daily exposure to death, care of dying patients, the need for quick decisions, and the impact of their decisions on the life and death of patients, are influential factors for high DA in critical care nurses (Aghajani et al., 2010). Therefore, nurses working in these wards are expected to experience higher DA levels. This finding was supported by a study in Iran (Khanlarzade et al., 2016). Therefore, paying attention to the DA of critical care nurses is inevitable. Mild SLEs were a predictor of DA among critical care nurses in this study. A study in Iran showed that nurses’ DA was significantly associated with SLEs. Coping with stress affects nurses' mental health and predisposes them to become vulnerable in the face of death and ultimately causes DA among nurses (Zahedi Bidgol et al., 2020); further studies are needed to confirm the results of the present study.
This study had several limitations. The present study results cannot be generalized to all critical care nurses due to cultural differences, attitudes toward death, religiosity, and religious coping strategies. Also, the self-report nature of the questionnaires and the lack of assessment of attitudes toward death in the present study may have impacted the results.
Clinical Implication
To our knowledge, DA is commonly expected among critical care nurses, which is less considered by researchers. High levels of DA among nurses can lead to adverse outcomes such as poor communication between nurse and patient, reduced quality of nursing care, and reduced quality of life of patients. In addition, DA is influenced by attitudes toward death, religiosity, and religious coping strategies that can vary in different societies and cultures. In fact, religiosity and religious coping strategies can be used as a potentially effective intervention to alleviate DA. However, future interventions need to evaluate the effectiveness of religious and spiritual interventions to reduce DA among critical care nurses. Therefore, nursing managers and policymakers should pay special attention to these related factors in developing programs to maintain and promote the health of critical care nurses to increase the quality of nursing care. Periodic assessment of mental health and nurses’ ability to deal with DA through continuing education programs can optimize the workforce and increase the quality of nursing care in critical care wards.
Conclusion
Overall, findings demonstrated that critical care nurses had a moderate level of DA. Also, deputy head nurse, shift morning fixed, surviving parents, the number of children, years of working experience, end-of-life patient care in the last 3 months, age, CCU nurses, and mild SLEs were significantly related to high DA. It is suggested that researchers in future studies design effective interventions to reduce DA in critical care nurses. A qualitative study to assess the impact of coping with death on the psychological status of critical care nurses can greatly help nurses reduce DA.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The Research Ethics Committee of Guilan University of Medical Sciences approved this research (IR.GUMS.REC.6971.370).