
Abstract
Objective
Orthorexia nervosa is an eating disorder characterized by a rigid preoccupation with a perceived healthy diet. However, little is known about healthy orthorexia compared to orthorexia nervosa. The current study examined the relationship between healthy orthorexia and orthorexia nervosa and personality traits in a Turkish sample.
Methods
Three hundred fifty participants from a community sample aged 18-65 were included in the study. Participants completed a sociodemographic data collection form, Beck Depression Inventory (BDI), Beck Anxiety Inventory (BAI), Teruel Orthorexia Scale (TOS), and the 10-Item Personality Inventory (TIPI).
Results
The frequency of healthy orthorexia was 32.3% and orthorexia nervosa was 10.2%. There were no differences between genders regarding healthy orthorexia and orthorexia nervosa scores. Healthy orthorexia symptoms were negatively correlated with depression and anxiety (r = -0.11 and r = -0.20, respectively, P < .05), while they were positively correlated with agreeableness (r = 0.17), conscientiousness (r = 0.14), and extraversion (r = 0.15). Orthorexia nervosa symptoms were positively associated with anxiety (r = 0.12), depression (r = 0.10), and healthy orthorexia (r = 0.55). Hierarchical regression analyses demonstrated that depression was negatively associated with healthy orthorexia symptoms, explaining 4% of the variance. The agreeableness trait was positively associated with healthy orthorexia symptoms, explaining 4% of the variance. However, no specific personality trait was associated with orthorexia nervosa symptoms.
Conclusion
To our knowledge, the present study is the first to examine the relationships between personality traits, healthy orthorexia, and orthorexia nervosa symptoms in a Turkish sample. Sociocultural factors may be important for understanding orthorexia nervosa and healthy eating behaviors in this population.
Introduction
Orthorexia Nervosa is an eating disorder characterized by a rigid preoccupation with a perceived healthy diet and overvalued nutritional beliefs that cause adverse weight and dietary outcomes and impairment in psychosocial domains. 1 Orthorexia was first defined in 1997 as an unhealthy obsession with healthy nutrition. 2 Individuals with orthorexia meticulously scrutinize food choices, invest significant time in food sourcing, and adhere strictly to meal planning. Anxiety and guilt arise when they deviate from their healthy eating habits, leading to feelings of disappointment. Paradoxically, this excessive focus on healthy eating can lead to adverse consequences, such as nutritional deficiencies, unintentional weight loss, and malnutrition. 3
Though orthorexia has gained recognition, its diagnostic criteria remain controversial, and it is not officially classified in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Some studies argue whether it should be regarded as a variant of an existing eating disorder or an obsessive-compulsive disorder (OCD).4,5 Shared features between orthorexia and anorexia nervosa, such as perfectionism, the desire for control, and the value placed on body appearance, further add to the complexity. 6 Unlike anorexia and bulimia nervosa, orthorexia nervosa involves qualitative evaluation of food (ie, good or bad) rather than quantitative assessment (ie, amount of food consumed). Intrusive thoughts and ritualistic behaviors related to meal preparation and consumption are similar to those observed in OCD. 7
Another related condition, Avoidant/Restrictive Food Intake Disorder (ARFID), shares diagnostic similarities with orthorexia nervosa. ARFID is characterized by avoidant or restrictive food intake due to sensory characteristics of food (eg, color, smell, texture, taste) or conditioned negative responses to eating, such as choking or vomiting, leading to significant weight loss and nutritional deficiencies. 8 Patients with ARFID follow a rigid but not shape or weight-motivated diet, similar to orthorexia nervosa. Food restriction in orthorexia nervosa is based on food quality and obsessed thoughts and rituals about a healthy diet. However, food restriction in ARFID is associated with aversive sensorial experiences or lack of appetite. It should be kept in mind that patients with eating disorders (anorexia, bulimia, binge-eating disorder, and ARFID) have higher orthorexia nervosa scores compared to patients without eating disorders. 9
An intriguing dimension of orthorexia nervosa is healthy orthorexia, wherein individuals exhibit a healthy interest in eating nutritious food as part of their identity. 10 In healthy orthorexia, dealing with healthy nutrition is an essential part of people’s lives, and people spend a lot of time and effort on it. This interest of individuals is suitable for their selfs’; in other words, it is ego-syntonic, as they define their attitude towards healthy food as a lifestyle. 10 Unlike orthorexia nervosa, healthy orthorexia is not associated with other eating disorders, obsessive-compulsive symptoms, or negative affect.10–12
The significance of sociocultural factors in shaping attitudes towards food, health, and individual roles must also be considered when assessing orthorexia nervosa and healthy orthorexic attitudes. 12 Possible cultural differences can also explain the inconsistency of orthorexia prevalence between studies.13,14
Gender is one of these sociocultural factors commonly associated with orthorexia nervosa. Social stigmas regarding women’s bodies and their internalization may contribute to a higher prevalence of orthorexia nervosa in women. 15 The societal expectation that women act as role models for their families can also impact orthorexia prevalence. While some studies have reported a higher prevalence of orthorexia nervosa in women, others found higher rates in men or no significant gender difference.6,16–22
Personality traits are also considered to link to unhealthy eating attitudes. 23 Attie and Brooks-Gunn 24 (1989) demonstrated that individuals with unhealthy eating attitudes and behaviors might experience perfectionism, depressive symptoms, impulse control problems, and emotion dysregulation. However, there are only a few studies exploring the relationship between general dimensions of personality and orthorexia. 25 The Big Five model of personality is the most prominent, encompassing 5 factors: extraversion, conscientiousness, openness, agreeableness, and neuroticism. 26 As far as we know, only 2 studies have examined the Big Five personality traits with orthorexia nervosa and healthy orthorexia.12,27 Additionally, another study assessed orthorexia nervosa, healthy orthorexia, and personality traits using the dimensional personality model of DSM-5. 25 This model defines the twenty-five personality facets and 5 personality traits that represent maladaptive forms of the big 5 personality dimensions. 8 However, these studies yielded inconsistent results. Some researchers found a significant relationship between neuroticism and orthorexia nervosa. Similarly, other studies found robust significant correlations between orthorexia nervosa, healthy orthorexia, and neuroticism, agreeableness, and extraversion (r > .20).12,28 On the other hand, Roncero et al 25 found a relationship between orthorexia nervosa and negative affectivity, psychoticism, and between healthy orthorexia and low disinhibition, psychoticism. Given the inconsistent findings in the literature, there is a need for further investigation into the relationship between personality traits and orthorexic eating attitudes. Based on previous data, we aim to rapidly and reliably examine personality traits in our culture using a short and valid questionnaire, the Ten-Item Personality Inventory (TIPI). 29
The present study aims to explore healthy orthorexia and orthorexia nervosa in a Turkish sample, examine gender differences with these attitudes, and assess the associations between personality traits and healthy orthorexia and orthorexia nervosa. We hypothesized that: • Anxiety and depression scores negatively correlated with healthy orthorexia scores. • Anxiety and depression scores positively correlated with orthorexia nervosa scores. • Emotional stability, extraversion, and openness to experience negatively correlated with orthorexia nervosa scores and positively correlated with healthy orthorexia scores. • Orthorexia nervosa scores are significantly higher in women compared to men. • Anxiety and depression scores, emotional stability, and extraversion are associated with orthorexia nervosa and healthy orthorexia scores.
Method
Sample
A total of 350 nonclinical participants between the ages of 18 and 65, who were literate, were included in the study. Recruitment of participants was done through various social media platforms and email lists.
The study was conducted in Gaziantep, Turkey. Gaziantep is a member of the Creative Cities Network of the United Nations Educational, Scientific, and Cultural Organization (UNESCO) by its distinguished gastronomy. Since sociocultural factors and eating habits could affect healthy diet behaviors, we want to examine orthorexia nervosa and healthy orthorexia in Eastern diet culture.
Participants completed the measurements through an online survey portal. Prior to beginning the survey, participants received a form ensuring the confidentiality of their personal information. They were informed that continuing with the survey would be considered as giving informed consent. Exclusion criteria encompassed psychiatric illness diagnosis, organic mental diseases (eg, delirium, mental disability), medical conditions with significant cognitive effects, epilepsy, dementia, and active alcohol or substance use disorders. The participants were not paid for their contribution to the study. The ethics committee of Kalyoncu University approved the procedures and the purposes of the study (decision date and number: 17/10/2022, e-97105791-050.01.01-24613).
Measurements
The sociodemographic data form: This form collected personal information such as age, sex, body mass index (BMI), level of education, and history of psychiatric treatment.
Beck Anxiety Inventory (BAI): BAI is a 21-item and 4-point Likert-type scale assessing anxiety levels. The scale was developed by Beck et al 30 and adapted to Turkish by Ulusoy and colleagues. 31 The maximum score that can be obtained from the scale is 63, and high scores indicate higher anxiety severity.
Beck Depression Inventory (BDI): BDI was developed by Beck and colleagues 32 to measure depression levels. This test consists of 21 items scored on a 4-point Likert-type scale. The Turkish version was adapted by Hisli. 33 Higher scores indicate higher depression severity, with a maximum score of 63.
Teruel Orthorexia Scale (TOS): TOS is a 17-item, 4-point Likert-type scale developed to assess orthorexia. It comprises 2 subscales: healthy orthorexia and orthorexia nervosa. 10 While the healthy orthorexia subscale evaluates the tendency to be interested in healthy foods and healthy eating, the orthorexia nervosa subscale evaluates the negative social and emotional effects of trying to reach a pure/healthy way of eating. Healthy orthorexia consists of 9 items for a maximum score of 27 (eg, I think that my way of eating is healthier than that of most people). Orthorexia nervosa consists of 8 items for a maximum score of 24 (eg, My social relationships have been negatively affected by my concern about eating healthy food). In this context, high scores from the healthy orthorexia subscale indicate higher interest in healthy eating. High scores from the orthorexia nervosa subscale indicate higher levels of pathological interest in healthy eating and the tendency to orthorexia nervosa. The Turkish validity and reliability study of the scale was performed in 2021 by Asarkaya and Arcan. 34 The Cronbach alpha score in this study was .88 for healthy orthorexia and .87 for orthorexia nervosa.
Ten-Item Personality Inventory (TIPI): TIPI was developed by Gosling et al 29 This scale measures 5 personality traits: openness to experience, conscientiousness, extraversion, agreeableness, and emotional stability. The scale includes ten items scored on a 7-point Likert type -ranging from 1 (disagree strongly) to 7 (agree strongly)-. Each subscale contains 2 items. The validity and reliability study of the scale was conducted by Atak. 35 The Cronbach alpha score in this study was .63.
Statistical Analyses
IBM SPSS Statistics for Windows v.25.0 was utilized to analyze the data (IBM Corp., Armonk, NY, USA). Descriptive statistics were employed to summarize the study group’s characteristics. The Pearson correlation coefficient was used to examine relationships between scale scores. Independent samples t-tests were conducted to assess gender differences in orthorexia nervosa and healthy orthorexia scores.
As there are no specific cutoffs to categorize TOS scores, participants were grouped based on their likelihood of displaying behaviors associated with orthorexia nervosa and healthy orthorexia. Scores were assigned percentile values (25th, 50th, and 75th) on the Likert-type response scale of the TOS: scores ≤.25 were classified as extremely unlikely, scores .25 to 50 were classified as unlikely, scores .50 to .75 were classified as likely, and scores >75 were classified as extremely likely. Participants falling into the ‘likely’ and ‘extremely likely’ categories were considered to exhibit healthy orthorexia and orthorexia nervosa behaviors. 36
Lastly, hierarchical regression analysis was performed to examine the associations between orthorexia nervosa and healthy orthorexia scores. Assumptions of multicollinearity, linearity, and homoscedasticity were assessed to ensure the validity of the regression analysis. 37 After the assumptions testing, 2 different hierarchical regression analyses were carried out for the dependent variables of orthorexia nervosa and healthy orthorexia. In the models, orthorexia nervosa and healthy orthorexia scores were entered as the dependent variables, and age, gender, BAI, BDI, and personality trait scores were entered as the regressors. The significance level was considered as .05.
Results
The Sociodemographic Data and Descriptive Statistics
The Sociodemographic Data.
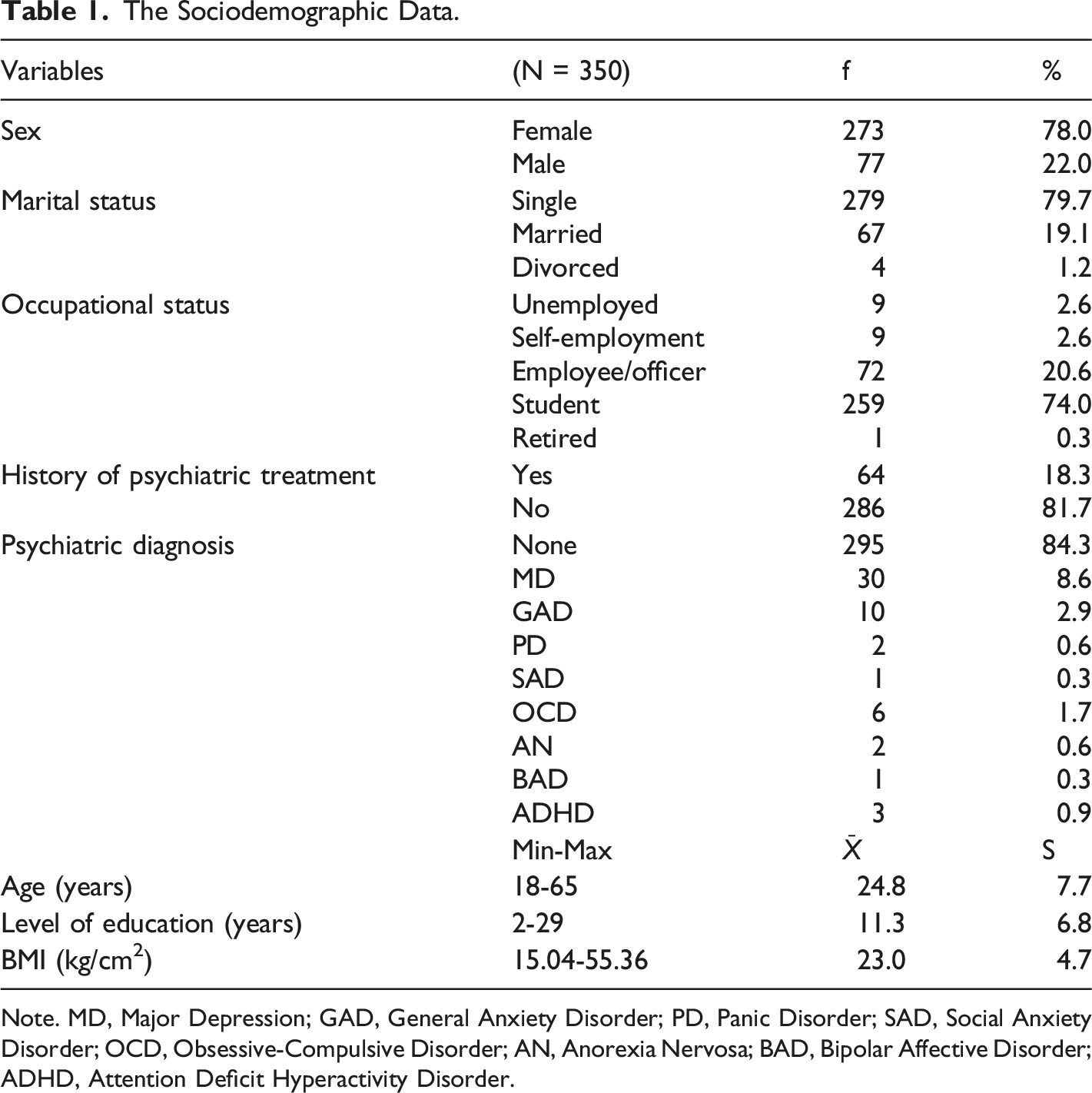
Note. MD, Major Depression; GAD, General Anxiety Disorder; PD, Panic Disorder; SAD, Social Anxiety Disorder; OCD, Obsessive-Compulsive Disorder; AN, Anorexia Nervosa; BAD, Bipolar Affective Disorder; ADHD, Attention Deficit Hyperactivity Disorder.
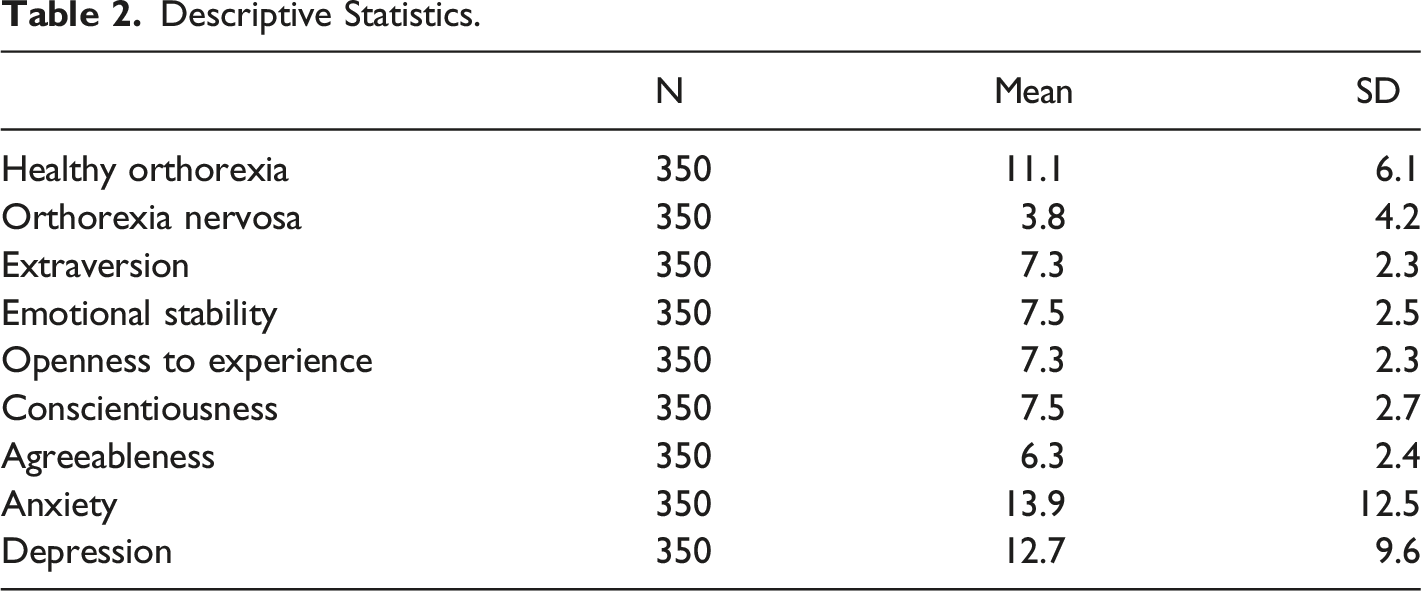
Descriptive Statistics.
Correlational Analyses
Correlation Matrix.
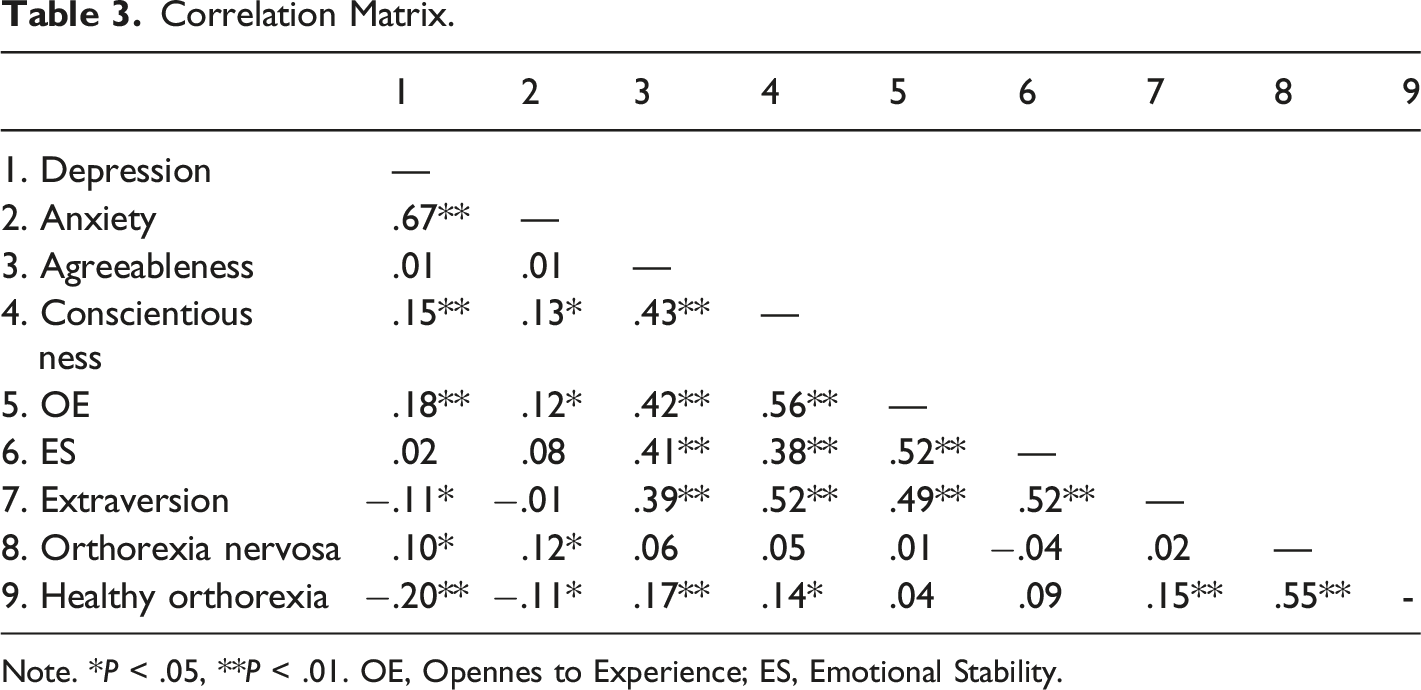
Note. *P < .05, **P < .01. OE, Opennes to Experience; ES, Emotional Stability.
Gender Differences
Independent samples t-tests revealed no significant differences in healthy orthorexia levels between males (x̄ = 11.9, SD = 6.4) and females (x̄ = 10.8, SD = 6.0), nor in orthorexia nervosa levels between males (x̄ = 4.3, SD = 3.6) and females (x̄ = 3.6, SD = 4.3).
The Distribution of the Participants According to Orthorexia Scores
Distribution of Participants According to the Classifications From the Orthorexia Nervosa and Healthy Orthorexia.
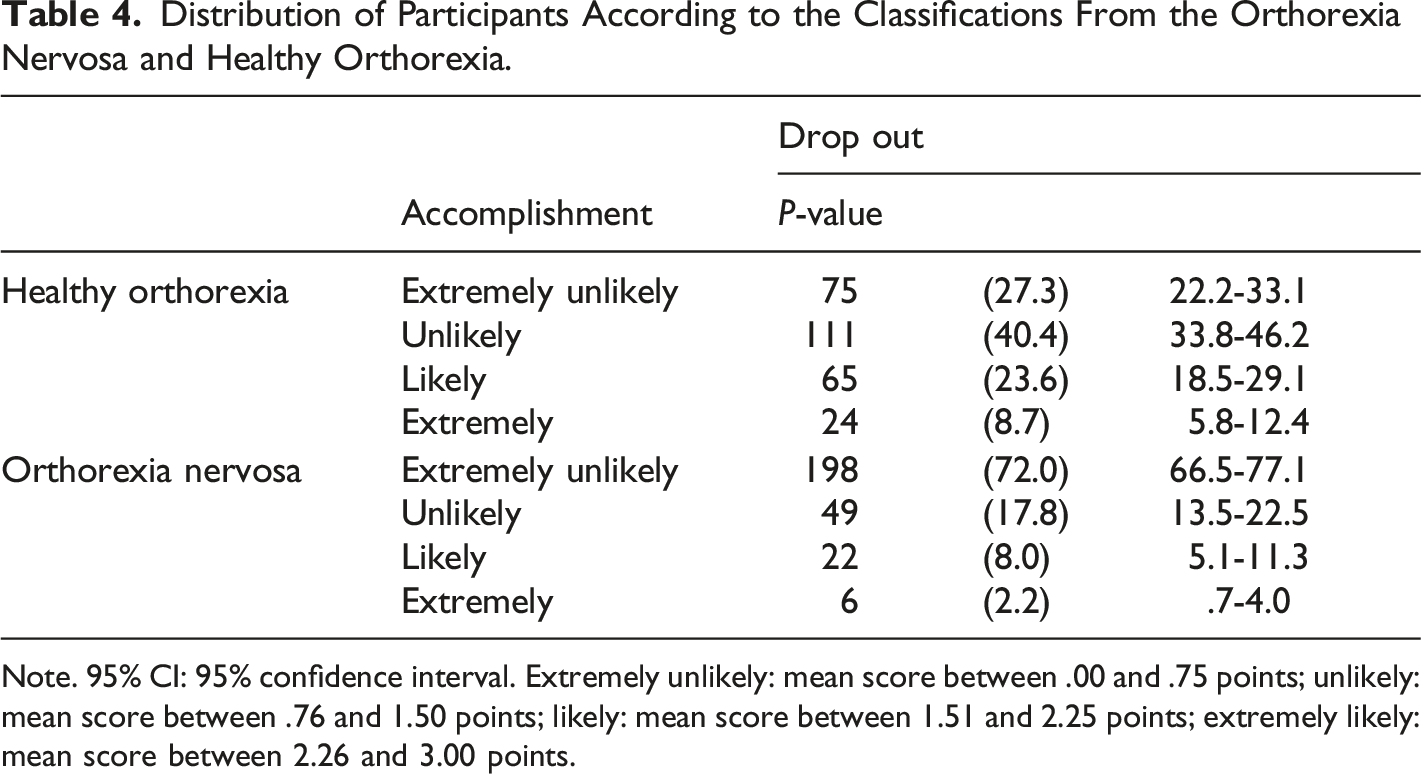
Note. 95% CI: 95% confidence interval. Extremely unlikely: mean score between .00 and .75 points; unlikely: mean score between .76 and 1.50 points; likely: mean score between 1.51 and 2.25 points; extremely likely: mean score between 2.26 and 3.00 points.
Hierarchical Regression Analyses
Three-stage hierarchical regression analyses were conducted to investigate the effects of anxiety, depression, and personality traits on orthorexia nervosa and healthy orthorexia symptoms.
For orthorexia nervosa symptoms, age and gender did not significantly contribute to the model in the first stage, accounting for nearly 0% of the variance. In the second stage, depression and anxiety scores were included, contributing to a 2% variance in orthorexia nervosa symptoms, which was significant. However, in the final step, where personality traits were added, the model only accounted for an additional 1% variance, which was not significant. Thus, none of the variables were significantly associated with orthorexia nervosa symptoms.
Regarding healthy orthorexia symptoms, age and gender did not significantly contribute to the model in the first stage, explaining 1% of the variance. In the second stage, depression and anxiety scores were added, accounting for an additional 4% of the variance in healthy orthorexia symptoms, which was significant. Finally, personality traits were added in the last step, explaining an additional 4% of the variance. All variables in the model accounted for 9% of the variance in healthy orthorexia symptoms. Depression level and agreeableness were associated with healthy orthorexia symptoms.
Hierarchical Regression Analysis for Orthorexia Nervosa.
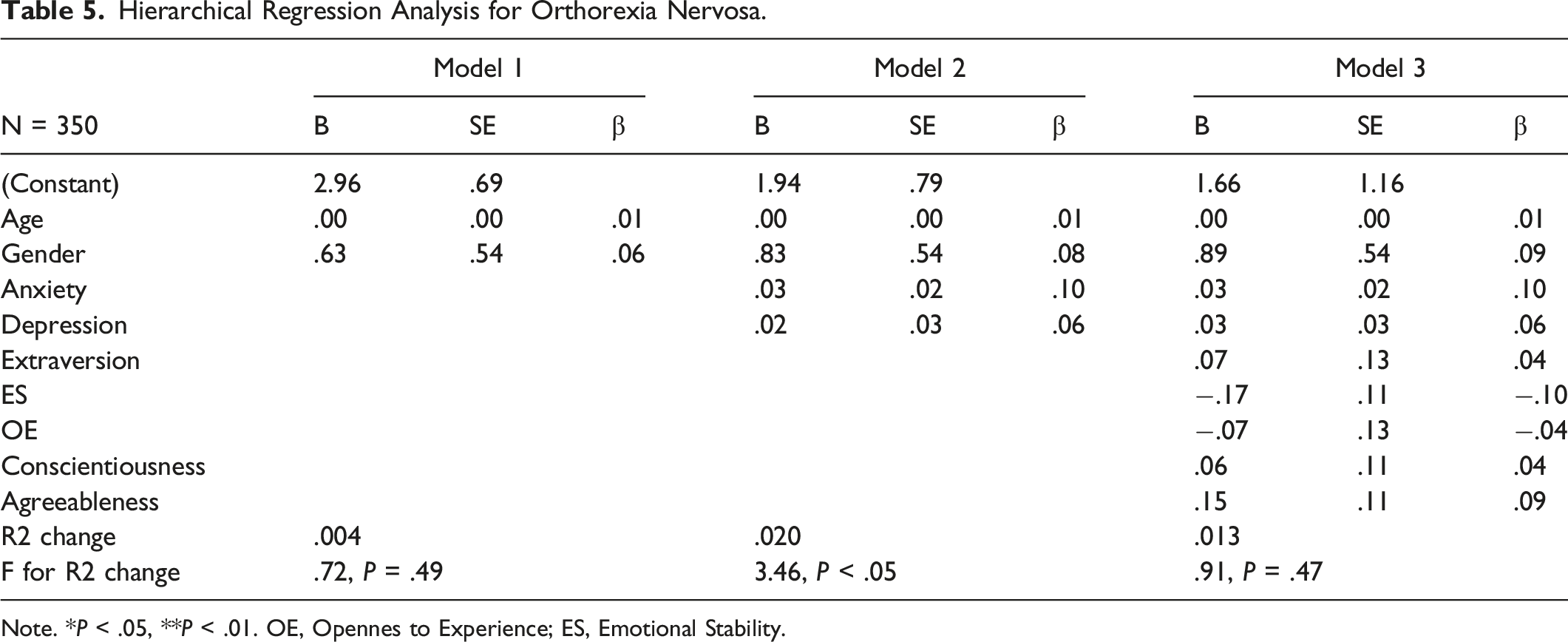
Note. *P < .05, **P < .01. OE, Opennes to Experience; ES, Emotional Stability.
Hierarchical Regression Analysis for Healthy Orthorexia.
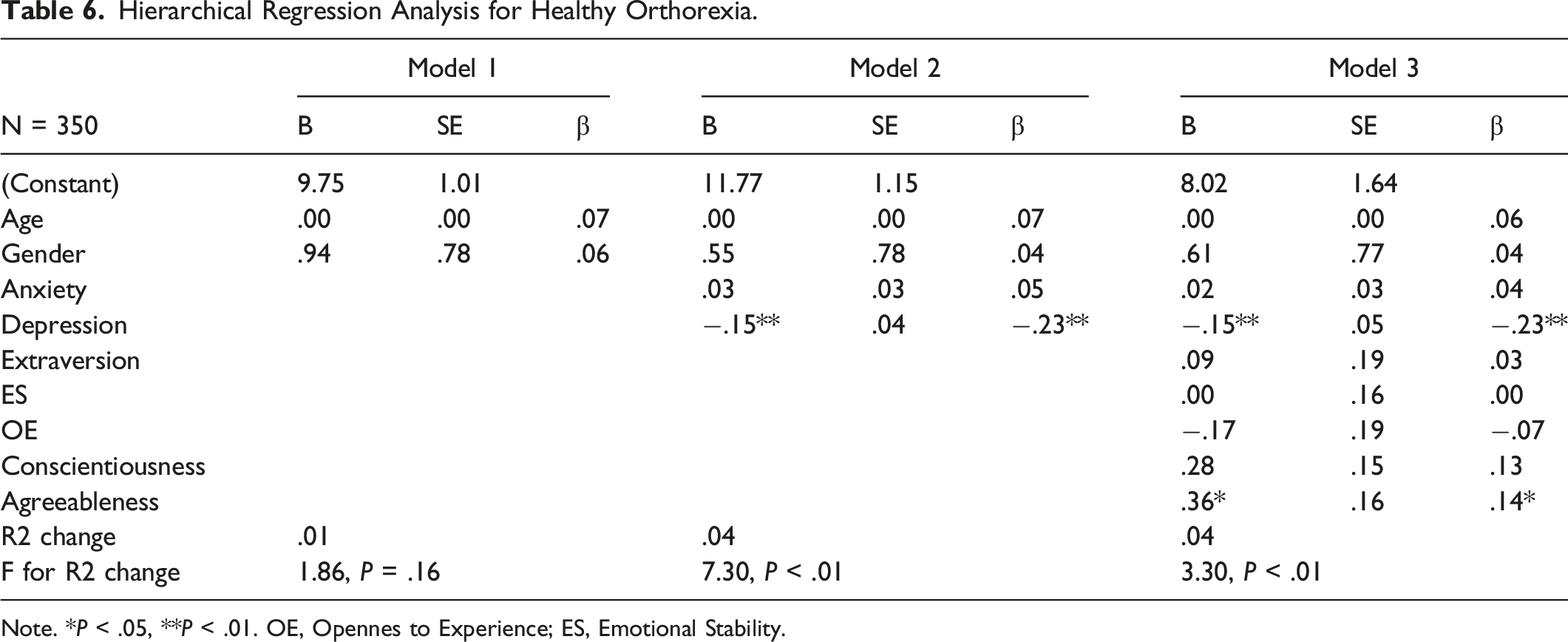
Note. *P < .05, **P < .01. OE, Opennes to Experience; ES, Emotional Stability.
Discussion
The current study aimed to investigate the associations between anxiety and depression levels, personality traits, and healthy orthorexia and orthorexia nervosa symptoms in a community sample. Additionally, gender differences were examined regarding healthy orthorexia and orthorexia nervosa symptoms. The study also explored the correlational relationships between anxiety, depression, personality traits, healthy orthorexia, and orthorexia nervosa scores.
There were no differences in healthy orthorexia and orthorexia nervosa levels regarding gender. Previous literature proposes heterogeneous results in terms of gender differences. Some researchers reported that healthy orthorexia scores did not differ between males and females.20,38,39 Conversely, Donini et al 40 found that men’s orthorexia nervosa prevalence was higher than women’s. Some sociocultural factors seem to be potential reasons for these mixed results. Future studies need to examine the underlying mechanism of the gender-orthorexia relationship.
Healthy orthorexia scores were positively correlated with extraversion, agreeableness, and conscientiousness, consistent with previous research. For instance, Roncero and colleagues found that healthy orthorexia correlated negatively with disinhibition, a maladaptive form of conscientiousness.25,41 Another study examining the German and Lebanese populations found that healthy orthorexia correlated positively with conscientiousness in both samples. 12 They also found a positive relationship between extraversion and healthy orthorexia in the German sample. Contrary to the previous results, there was no relationship between orthorexia nervosa and personality traits. 12 The absence of specific relationships between orthorexia nervosa levels and personality traits could be interpreted as the sociocultural features of the selected sample.
In line with previous studies, we found that healthy orthorexia symptoms are associated negatively with depression and anxiety levels.10,42,43 Healthy orthorexia assesses the interests of a healthy diet and is a separate construct from psychopathology. In addition, orthorexia nervosa symptoms correlated positively with depression and anxiety levels. It could be suggested that orthorexic attitudes can cause obsessive eating behaviors and social isolation-related depression. 8 This finding is consistent with previous research showing associations between anxiety, restrictive eating behaviors and health-related anxiety with orthorexia nervosa.44,45
Our regression analysis results were consistent with the literature partially. Agreeableness is one of the major personality traits in the Big Five Personality Model. People with higher agreeableness are characterized as pleasant, altruistic, sympathetic, and cooperative in their relations with others. 46 Personality traits such as extraversion, openness to experience, or agreeableness are associated with preferences to choose healthy nutrition, where health benefits become the primary goal. 47 Researchers showed that individuals with higher agreeableness tend to choose healthier diets, including more fruits and vegetables and less red meat. 48 In people with low levels of agreeableness, negative attitudes in interpersonal relationships can lead to isolation, which, in turn, can affect their eating patterns. 49
There are limited data exploring the association between healthy orthorexia and personality in different cultures. Roncero and colleagues 25 found that psychoticism and low disinhibition are associated with healthy orthorexia symptoms. However, previous data with orthorexia nervosa and personality traits support our results and limited healthy orthorexia data. In a Lebanese sample study, negative affectivity and agreeableness were found to predict the severity of orthorexia nervosa negatively, and this relationship was more evident in the Lebanese sample than in the German sample. 12 Additionally, a study in Poland showed that the risk of developing orthorexia nervosa was higher in individuals with low agreeableness. 49 Therefore, we could interpret our findings in light of previous data, suggesting that people with higher agreeableness tend to have healthier eating attitudes and behaviors than those with lower agreeableness. The ‘agreeableness’ trait may be exhibited differently across different cultures. In Eastern countries like Lebanon or Turkey, altruistic and collectivistic cultural features related to agreeableness could be more associated with healthy eating behaviors than other personality traits. 12
The number of studies examining psychopathology and healthy orthorexia is limited. A healthy diet pattern, which includes more fruits, vegetables, fish, and whole grains, is associated with decreased depressive symptoms. 50 Thus, our hierarchical regression results are in line with the limited literature.
Surprisingly, none of the personality traits, depression, and anxiety scores were associated with orthorexia nervosa symptoms. Previous data showed neuroticism, openness to experience, and conscientiousness are positively associated with orthorexia nervosa. 28 However, Strahler and colleagues 12 found that orthorexia nervosa is negatively associated with antagonism. Another study with 297 participants from the general population reported that psychoticism and negative affectivity are associated with orthorexia nervosa. 25 In line with the previous study, Awad and colleagues 51 found that high sensation seeking and low negative affectivity are associated with higher orthorexia nervosa scores. A study conducted with college students reported that all maladaptive personality traits (negative affectivity, detachment, disinhibition, psychoticism, antagonism) show higher scores in people with higher orthorexic tendencies than those with lower tendencies. 52 Several reasons could explain the differences between our results and previous data. First, our study’s mean orthorexia nervosa scores were lower than in previous studies.12,51 Second, when we look at the studies conducted in other cultures, the prevalence of orthorexia nervosa is higher in Poland, Hungary, Lebanon, and Germany compared to Italy, the USA, and Turkey.21,53–58 Moreover, the ORTO-15/ORTO-11-Hu scale was used to evaluate orthorexia nervosa in the studies mentioned above. Criticisms about the validity of the ORTO questionnaire in the literature add value to our study.59–61 The easy access to delicious and healthy food in Mediterranean countries, such as Italy and Turkey, may explain why orthorexia nervosa scores are lower than in Western countries and why orthorexia nervosa is not associated with personality traits. Despite the belief that Western diet culture is more accepted and applied by Eastern countries, our study results show the opposite. 62 In conclusion, our study’s cultural factors and scale features could explain our results.
Study Limitations
Several limitations of our study should be declared. First, our study had a cross-sectional design. Second, we examined our hypothesis in a nonclinical sample mainly consisting of university students, and we could not generalize the findings to a clinical sample. Third, the measurement tools are self-report questionnaires, which could cause a bias. Lastly, behaviors like exercise and eating could be influenced by cultural norms, religion, and social standards. 63 Furthermore, the region where we conducted our study has a rich diet culture. The uniqueness of the city could be the reason for the findings. Thus, orthorexic and non-orthorexic eating beliefs and behaviors could be related to these factors, and our study design or orthorexia nervosa measures in our study do not consider cultural or religious factors.
Conclusions
In conclusion, to the best of our knowledge, our study is the first to examine personality, orthorexia nervosa, and healthy orthorexia in a Turkish sample. We found no gender differences in healthy orthorexia and orthorexia nervosa. Our results revealed an association between depression and agreeableness with healthy orthorexia. However, we could not find an association between orthorexia nervosa and personality traits. Despite the limitations, our study sheds light on the orthorexia literature concerning gender and personality traits.
Future research should focus on the diagnosis of orthorexia nervosa and its relationship with other eating disorders. In addition, researchers should explore the effects of cultural factors on eating behaviors. If we understand the association between orthorexia nervosa and these factors, we could assess patients more individually. Also, further studies are needed to evaluate the relationship between psychopathology and orthorexia nervosa and healthy orthorexia. Repetition of our results in large, more homogenous clinical samples is crucial for generalizability.
Footnotes
Author Contributions
All authors contributed to the study’s conception and design. Material preparation, data collection, and analysis were performed by [principal author: Kübra Sezer Katar], [Mustafa Batuhan Kurtoğlu], [Başak Şahin]. The first draft of the manuscript was written by [principal author: Kübra Sezer Katar], and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The ethics committee of Hasan Kalyoncu University approved the procedures and the purposes of the study (decision date and number: 17/10/2022, e-97105791-050.01.01-24613). Written informed consent was obtained from participants.