
Abstract
Orthorexia Nervosa (ON) is characterized by an excessive preoccupation with healthy eating, accompanied by increasingly restrictive dietary practices over time. In light of the increased attention to ON, it is noteworthy that the existing body of research, specifically with regard to mindfulness and self-compassion remains constrained in scope and depth. A total of 151 participants over the age of 18 completed scales measuring Orthorexia, Self-Compassion, Mindfulness, and Perfectionism. The findings revealed that individuals exhibiting high levels of ON tended to have low levels of self-compassion and mindfulness, along with high levels of perfectionism. Furthermore, the results indicated that self-compassion and mindfulness acted as mediators in the relationship between perfectionism and orthorexia nervosa. These findings deepen our comprehension of orthorexia and underscore the role of self-compassion and mindfulness, or their absence, as mediating factors in this context. The implications of these results and potential future directions are discussed.
Introduction
Healthy diets have become increasingly popular in recent years as means of achieving optimal health and a desire to improve current health or as a preventative measure however these are common underlying features which may lead to orthorexic tendencies (Dunn & Bratman, 2016). Orthorexia nervosa (ON) was first introduced by Bratman in 1997 (Bratman, 2017), who described ON as an obsessive fixation on healthy eating. While healthy eating is a desirable health behaviour for some individuals the drive for healthy eating may include obsessive thoughts, compulsive behaviours and self-punishment and these are symptoms which collectively have been defined as ON (Bratman, 2017). Individuals with orthorexic tendencies focus purely on food quality and purity (Koven & Abry, 2015) and spend significant time planning and preparing meals that adhere to their food rules. Many individuals who display ON eliminate specific food groups which they consider unhealthy (Dunn & Bratman, 2016). Over time, these restrictions become more extreme resulting in the lack of enjoyment of food, as well as potentially resulting in malnutrition and further medical complications (Brytek-Matera et al., 2017; Cena et al., 2018; Dunn & Bratman, 2016).
The clinical recognition of Orthorexia Nervosa (ON) as an eating disorder remains debated despite the proposal of multiple diagnostic criteria; its absence in the DSM-5 is noteworthy (Donini et al., 2004; Koven & Abry, 2015). ON shares characteristics with established eating disorders (Bartel et al., 2020), and research indicates a link between prior eating disorders and ON development, manifesting as a shift from quantity to quality of food obsession, serving as a socially acceptable weight control strategy for those with disordered eating histories (e.g. Hanganu-Bresch, 2019; McComb & Mills, 2019). Considering the common characteristics between eating disorders and orthorexia, it is important to explore factors that have led to the development and maintenance of eating disorders. One of these factors is perfectionism, perfectionism is a construct with multiple components including high personal standards, excessive concern over mistakes, fear of negative evaluations and self-criticism (Frost et al., 1990). It has been extensively researched in the development and maintenance of eating disorders (e.g., Bardone-Cone et al., 2007; Brown et al., 2012; Franco-Paredes et al., 2004; Rand-Giobannetti et al., 2022), as well as treatment of eating disorders (Bardone-Cone et al., 2009; Egan et al., 2011; Goldstein et al., 2014). A recent systematic review has suggested that perfectionism interventions have been shown to reduce disordered eating and Bulimia Nervosa (Robinson & Wade, 2021). One of the main features of ON is the strict adherence to dietary rules and experiencing self-criticism when deviating from these rules (Bratman, 2017; Mathieu, 2005), this aligns with the components of perfectionism outlined earlier (Frost et al., 1990).
Several researchers have investigated ON and perfectionism (e.g., Barnes & Caltabiano, 2016; Miley et al., 2022; Pratt et al., 2023; Yung & Tabri, 2022). Barnes and Caltabiano (2016) found that elevated levels of perfectionism have been associated with greater orthorexic tendencies. These findings were corroborated by Novara and colleagues (2022) who conducted a cross-sectional study investigating perfectionism and orthorexia and found that individuals classified under a high orthorexic group demonstrated higher levels of perfectionism compared to those in a lower orthorexic group, individuals with orthorexic tendencies scored highest on the subscales of personal standards and organisation. Additionally, they found that those higher in the orthorexic group displayed higher levels of depression (Novara et al., 2022) suggesting that individuals could experience compromised social functioning and depressive mood, which is central to ON (Oberle et al., 2020). This suggests that perfectionism influences orthorexia. However, research has also suggested that the relationship between orthorexia and perfectionism is weaker compared to other eating disorders (Bartel et al., 2020). Given that perfectionism is a significant factor in eating disorders, and considering that orthorexia shares similar characteristics with such eating disorders, it becomes essential to explore perfectionism further within the context of orthorexia.
Mindfulness and self-compassion are closely correlated constructs that have been extensively researched in the context of eating disorders, disordered eating and perfectionism (e.g., Braun et al., 2016; Ferreira et al., 2014; Manova & Khoury, 2023; Tobin & Dunkley, 2021). According to Kabat-Zinn (2003), mindfulness is a psychological concept that entails paying conscious attention to both internal and exterior phenomena such as feelings, thoughts, and bodily sensations without passing judgment. Neff (2003a) has defined self-compassion as understanding that suffering and failure are all part of the human experience, with three key components of self-kindness, shared humanity and mindfulness. As these are closely related there are key differences between the constructs, self-compassion is utilised when facing challenges, personal failures, inadequacies and alleviating suffering
The primary objective of this investigation was to examine the connections between orthorexia nervosa (ON), mindfulness, self-compassion, and perfectionism. Notably, no prior research has explored the interrelationships among all of these constructs. Based on existing literature, it is hypothesized that ON will exhibit negative correlations with mindfulness and self-compassion (Kalika et al., 2022, 2023), while showing positive correlations with perfectionism (e.g.,Merhy et al., 2023; Miley et al., 2022; Novara et al., 2021). The secondary goal of this study was to investigate the mediating power of mindfulness in the association between perfectionism and orthorexia nervosa. The final objective was to investigate self-compassion as the potential mediator of the relationship between perfectionism and orthorexia nervosa. The complex connections between perfectionism, orthorexia, mindfulness, and self-compassion warrant thorough examination. This study represents the inaugural exploration of these interconnected concepts which will aid in further understanding of orthorexia nervosa.
Methods
Participants
The present study looked at the general population in terms of orthorexia nervosa. A total of 224 participants were initially recruited for the study. However, 73 participants who did not complete the entire study were excluded from the final sample. The sample (n = 151) for the present study consisted of 116 females, 31 males, 2 prefer to self-describe as non-binary and 2 participants who preferred not to say, who were all adults (18 years- 67 years; M = 30.47, SD = 10.84 with a mean Body Mass Index (BMI) of M = 23.40 kg/m2 (SD = 4.73). Correlation with 4 variables based on a power of .8 for medium effect size and set with the significance of .05 comes to a minimum of 118 participants (Cohen, 1992). A total of 111 participants identified as White, 27 as Asian, 5 as Black, 7 as Mixed and 1 as Other, Furthermore, the type of diet was also collected, the sample consisted of 82 Omnivores, 20 occasional omnivores, 16 semi-vegetarians, 6 pescatarians, 10 lacto-ove-vegetarians, 7 lacto-vegetarians and 10 as vegans. Participants were recruited through volunteering sampling by advertising the study on several social media platforms and forums such as Facebook, Instagram, Twitter and LinkedIn. The advertisement on Facebook has been posted in eating groups requesting individuals to participate in the study. Individuals were also recruited through the university’s Research Participation Scheme. Those who participated in the scheme were rewarded with research credits upon completion of the study. Participants were informed via the information sheet that the inclusion criteria for this study required them to be over the age of 18, have good knowledge of the English language and not be diagnosed with an eating disorder.
Materials
Orthorexia Nervosa Inventory (ONI)
The scale was developed by Oberle et al. (2020). It is a measure of ON symptomatology which includes 24 items assessing 3 factors of orthorexic behaviours such as impairments, behaviours and emotions. It utilises a 4-point Likert scale with the following responses: 1 (not at all true) to 4 (very true). The higher total score indicates a greater severity of ON, Oberle et al. (2020) has suggested a score of minimum of 72 to indicate orthorexic tendencies. Sample question are “My healthy eating is a significant source of stress in my relationships” and “I follow a healthy diet with many rules”. The Cronbach alpha for the present study was .97 Additionally, the Cronbach alpha was calculated for the subscales; impairments was .94, behaviours was .92 and emotions was .89. Previous studies have looked at psychometrics of this scale indicating good convergent and criterion validity (Oberle et al., 2020; Zagaria et al., 2023) with Messer et al. (2023) utilising this scale for further validation of orthorexia nervosa symptoms.
Five-Facet Mindfulness Questionnaire- Short Form (FFMQ)
This is a shorter version of the original 39-item FFMQ. This scale was developed by Baer et al. (2008) and includes 15 items that measure five facets Observing, Describing, Acting with Awareness, Non-Judging and non-reactivity. This scale utilises a 5-point Likert scale with the following responses: 1 (never true) to 5 (always true). A score is combined for each facet of the scale, with no minimum threshold. Sample questions include “I do jobs or tasks automatically without being aware of what I’m doing” and “I find myself doing things without paying attention”. The Cronbach alpha for the present study was .67. Additionally, the Cronbach alpha was calculated for the subscales; observing was .56, describing was .73, acting with awareness .80, non-judging of inner experience was .86 and non-reactivity was .67. The convergent and discriminant validity of the scale was established in previous research (Bohlmeijer et al., 2011).
Self-Compassion Scale (SCS)
This is the original 26-item SCS, it was developed by Neff (2003b) to measure self-compassion. The items are rated on a 5-point Likert scale with the following responses, 1 (never) to 5 (always). This scale includes three compassionate components and three uncompassionate components; the uncompassionate components are reversed scored, these components are self-kindness, self-judgement, common humanity, isolation, mindfulness, and over-identification. Sample questions include “When I fail at something important to me I become consumed by feelings of inadequacy” and “I try to be loving towards myself when I’m feeling emotional pain”. The Cronbach alpha for the present study was .93. Additionally, the Cronbach’s alpha was calculated for the subscales; self-kindness was .83, self-judgement was .84, common humanity was .81, mindfulness was .75 and over-identified was .71. This scale is a valid measure of self-compassion as research indicates strong predictive validity such as group validity (Neff, 2003b, 2015; Neff & Pommier, 2013) and good convergent validity (Neff et al. 2007).
Frost Multidimensional Perfectionism Scale (FMPS)
This scale was originally developed by Frost et al. (1990), however, the current study is looking at Stöber (1998) version which contains four subscales instead of six. There are 35 items measuring perfectionism. The subscales are Concern over Mistakes and doubts about actions, Excessive concern with parents' expectations and evaluations, Excessively high personal standards and Concern with precision, order and organisation. Each item is scored on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Sample questions include “My parents wanted me to be the best at everything” and “I am very good at focusing my efforts on attaining a goal”. The Cronbach alpha for the present study was .95. Additionally, the subscales were calculated Concern over Mistakes and doubts about actions had .93, Excessive concern with parents' expectations and evaluations had .93, Excessively high personal standards had .83 and Concern with precision, order and organisation had .88. The validity of the measure was tested by Hewitt et al. (1991) indicating that the scale has good validity.
Procedure
The study received Ethical approval from the ethical committee of an institution based in the midland region of the United Kingdom. Participants were recruited through social media groups and were encouraged to share the study with their connections. They were provided with information about the study, including the criteria for inclusion and exclusion, and the hyperlink to Qualtrics where they could access the questionnaire. Additionally, the university’s Research Participation Scheme was employed offering research credits to individuals who participated. Participants were given a Participant Information Sheet to read, prior to consenting. Participants consented and created a unique code for identifying data in the event of withdrawal. Participants were asked to complete demographic information, ONI, FFMQ, SCS-SF and FMPS. After completion, participants were provided with a debrief form explaining the objectives of the study and the withdrawal process. The study consisted of a single 20-minute online session.
Data Analysis
Bivariate Correlations Between ONI, BMI, FFMQ, SCS and FMPS and Descriptive Statistics.
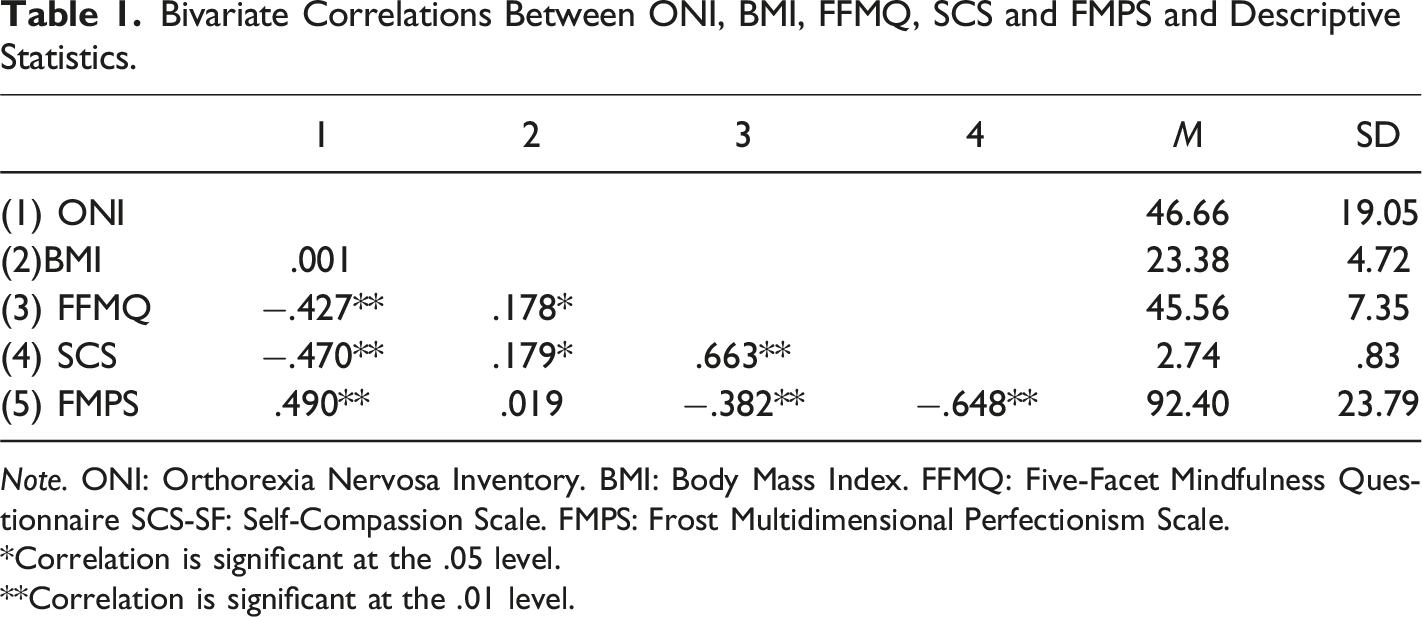
Note. ONI: Orthorexia Nervosa Inventory. BMI: Body Mass Index. FFMQ: Five-Facet Mindfulness Questionnaire SCS-SF: Self-Compassion Scale. FMPS: Frost Multidimensional Perfectionism Scale.
*Correlation is significant at the .05 level.
**Correlation is significant at the .01 level.
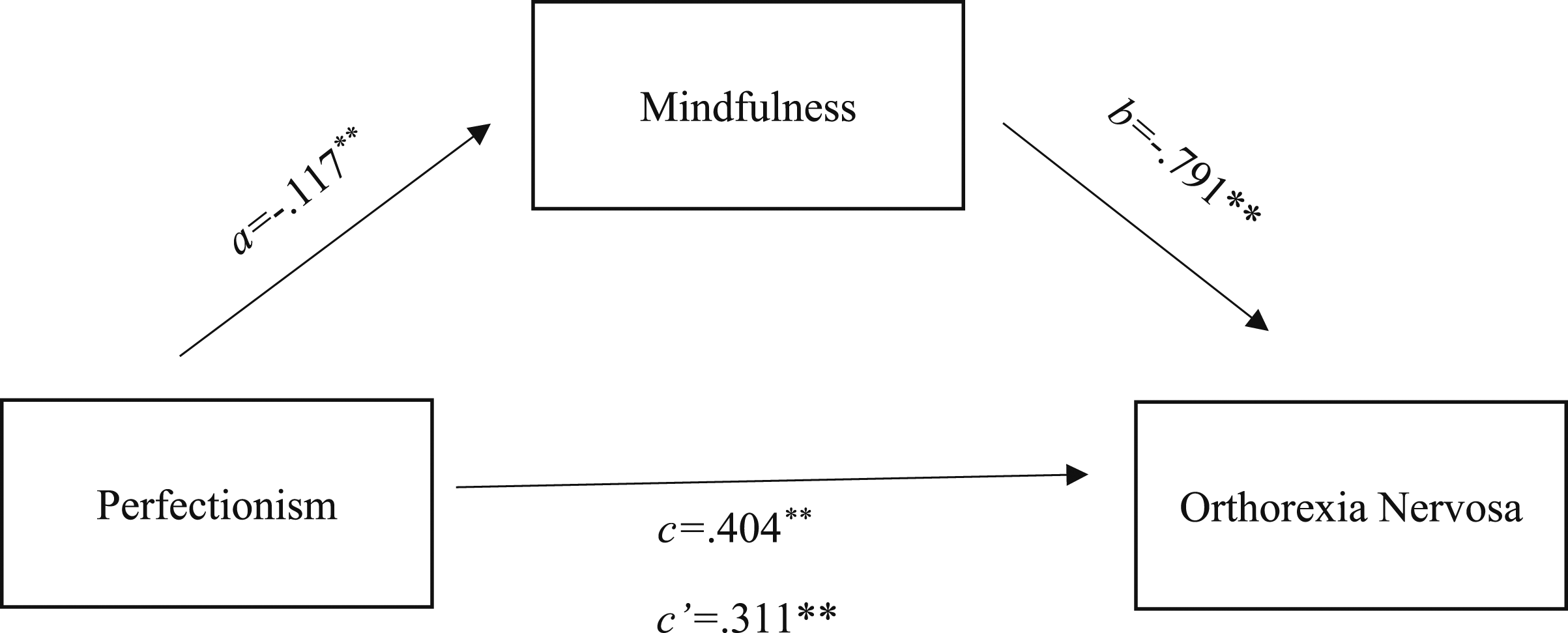
Furthermore, mediation analysis was used to evaluate the indirect effects (via self-compassion and mindfulness) of perfectionism on orthorexia nervosa (see Figure 1 and 2). Hayes’ (Preacher & Hayes, 2008) PROCESS macro (v3.3) was installed on SPSS (version 25.0) and was used to conduct mediation analyses (model 4) using 10,000 bootstrapping resamples to generate 95% bias-corrected confidence intervals for the indirect effect (Preacher & Hayes, 2008). According to specified guidelines using mediation analyses, Fritz and MacKinnon (2007) suggested that a sample size of 148 participants would enable research to observe an indirect effect of a small-medium sized alpha pathway coefficient (i.e. predictor to mediator) and a small-medium sized beta pathway coefficient (i.e. mediator to criterion) at 80% power using bias-corrected bootstrapping estimating procedures. Parallel mediation using standardized regression coefficients to examine the interaction of self-compassion in the relationship between a) Perfectionism and b) orthorexia nervosa. Notes: a is the effect of perfectionism on self-compassion; b is the effect of self-compassion on orthorexia nervosa; c is the effect of perfectionism on orthorexia nervosa; c’ is effect of perfectionism on orthorexia nervosa with self-compassion in the model. Parallel mediation using standardized regression coefficients to examine the interaction of mindfulness in the relationship between a) Perfectionism and b) orthorexia nervosa. Notes: a is the effect of perfectionism on mindfulness; b is the effect of mindfulness on orthorexia nervosa; c is the effect of perfectionism on orthorexia nervosa; c’ is effect of perfectionism on orthorexia nervosa with mindfulness in the model.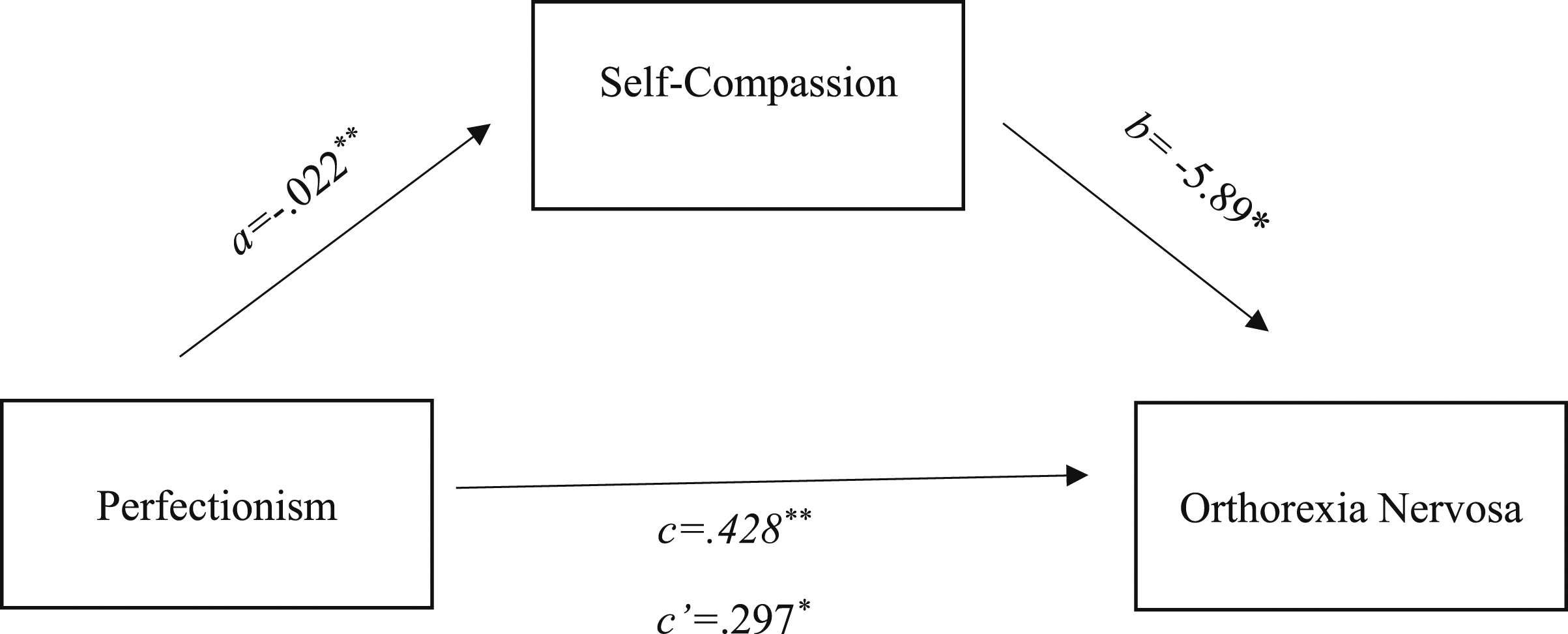
Results
A multiple correlation analysis has been used to identify which scales (BMI, SCS, FFMQ and FMPS) relate to ONI.
Inter-correlations between ONI, BMI, SCS, FFMQ and FMPS, are presented in Table 1 with r < 0.3 indicating a weak correlation, 0.3 ≤ r < 0.5 indicating a moderate correlation and r ≥ 0.5 indicating a strong correlation (Ratner, 2009). Findings indicate that there are significant negative relationships between ONI and FFMQ (p < .001), SCS (p < .001) and FMPS (p < .001) Only BMI was not significant concerning ONI. In addition, correlational analysis on the subscales of ONI was performed results are presented in Supplementary Table 2 found in supplementary materials. A further correlation analysis has been conducted between the ONI, and subscales of FFMQ, SCS and FMPS, the findings are presented in Supplementary Table 3 found in supplementary materials.
The mediational model analyses (see Figure 1) used orthorexia as the dependent variable, perfectionism as independent variable, and self-compassion as potential mediator. The c indicated a significant relationship between perfectionism and orthorexia b = .428, p < .001, 95%CI [.309, .548]. Pathway a showed that perfectionism predicted self-compassion b = −.022, p < .001, 95%CI [-.027, −.018], however for pathway b self-compassion did predict orthorexia b = -5.89, p < .05, 95%CI [-10.37, −1.42]. When self-compassion was included in the mediation model, it remained significant b = .297, p < .005, 95%CI [.143, .451], this therefore suggests that the relationship between restrained eating and orthorexia is mediated by self-compassion.
The second mediational model analyses (see Figure 2) used orthorexia as the dependent variable, perfectionism as an independent variable, and mindfulness as potential mediator. The c indicated a significant relationship between perfectionism and orthorexia b = .404, p < .001, 95%CI [.284, .523]. Pathway a showed that perfectionism predicted mindfulness b = −.117, p < .001, 95%CI [-.166, −.069], however for pathway b mindfulness did predict orthorexia b = -.791, p < .005, 95%CI [-1.19, −.389]. When mindfulness was included in the mediation model, it remained significant b = .311, p < .001, 95%CI [.187, .434], this therefore suggests that the relationship between perfectionism and orthorexia is mediated by mindfulness.
Discussion
This study represents the inaugural exploration of the connections between orthorexia nervosa, perfectionism, mindfulness and self-compassion, with the potential to develop further relevant research and interventions. The results of this study corroborate prior findings demonstrating a consistent negative relationship between mindfulness and self-compassion and orthorexia nervosa (Kalika et al., 2022, 2023; Stahler, 2020). Findings suggest that individuals who display higher levels of orthorexic tendencies display lower levels of self-compassion and mindfulness. These results also align with existing research on eating behaviours and mindfulness, as mindfulness has been linked to lower levels of disordered eating (Beshara et al., 2013; Dutt et al., 2019; Mantzios et al., 2018, 2019; Mantzios & Wilson, 2013, 2014, 2015). Three of the subscales were negatively correlated with ON, these were non-judgement, acting with awareness and describing, which follows recent findings (Kalika et al., 2022). Unsurprisingly individuals with orthorexic tendencies display high levels of judgement as research has shown that those who violate their food rules display elevated levels of distress, self-judgement and self-punishment (Bratman, 2017; Koven & Abry, 2015).
A key concept of self-compassion is self-kindness (Neff, 2003a), the present study has found that the self-kindness subscale had the lowest levels in relation to orthorexia. Having lower levels of self-compassion might indicate that individuals with orthorexic tendencies will not view orthorexic eating as a way of being kind to themselves as research suggests that they engage in their eating as a means of improving their health (which could be viewed as an act of self-kindness. A qualitative study done by Lewthwaite and LaMarre (2022) supports these findings as they have found that orthorexic individuals acknowledged that restrictive eating was not viewed as an act of self-kindness. However, others recognised that having dietary flexibility where they consumed treats and occasional unhealthy foods was an act of self-kindness as it allowed them to become more healthful individuals. This could potentially mean that there is a distinctive difference between healthy orthorexia and orthorexia nervosa proposed by Roncero et al. (2021). Healthy orthorexia refers to non-pathological healthy eating and interest in nutrition, whereas orthorexia nervosa refers to disordered eating that is characterised by obsessive preoccupation with healthy eating (Zickgraf & Barrada, 2021). Therefore, those who display healthy orthorexia could have higher levels of self-compassion and mindfulness as they acknowledge that there needs to be flexibility in terms of eating (Lewthwaite & LaMarre, 2022) whereas those with orthorexia nervosa could potentially have low levels of self-compassion and mindfulness.
Investigating perfectionism was also one of the main aims of this study. The present study reveals that individuals with higher orthorexic tendencies display higher levels of perfectionism. The findings are replicated in accordance with findings in past literature (e.g., Merhy et al., 2023; Miley et al., 2022; Novara et al., 2021). Furthermore, the subscales are also positively correlated with ON except for the Organisation subscale, which is no surprise as the Organisation subscale is removed from the total score (Stöber, 1998) due to not being problematic and a subscale designed for the assessment of constructive qualities. Concern over mistakes and doubts subscale had the highest positive correlation out of all of the subscales followed by the Excessive concern with parent’s expectations which is an unexpected finding. High levels of Concern over mistakes and doubts have been associated with higher levels of anorexia nervosa and bulimia nervosa (e.g., Boisseau et al., 2013; Bulik et al., 2003) and eating pathology (Davies et al., 2009; Egan et al., 2011). Due to ON having similar characteristics to other eating disorders, this relationship aligns with past literature. Furthermore, individuals with high orthorexic tendencies set themselves strict dietary rules that require them to spend a significant amount of time researching to choose the most appropriate foods according to their rules (Bratman, 2017). If they do not adhere to their rules then the individual experiences self-hatred, self-criticism and guilt (Bratman, 2017; Mathieu, 2005). High scores on Excessive concern with parental expectations subscale is an unexpected finding. Research has suggested that ON is mostly influenced by desire to achieve optimal health, improving general health (Bratman, 2017; Dunn & Bratman, 2016) and social media exposure (Turner & Lefevre, 2017). However, a qualitative study done by Cheshire and colleagues (2020) highlighted that parental influences emerged as significant in the development of orthorexia, this could either be the extreme religious beliefs in the family, parental dietary choices or challenging relationships with parents thus expressing themselves through eating. However, the sample of this study included health care professionals and those who self-diagnosed with orthorexia nervosa, potentially suggesting that the sample might not entirely reflect a true representation of orthorexia nervosa. Additionally, majority of the sample was female therefore the findings could potentially not be replicated in a male sample. This is the only study that has highlighted a link between parental expectations and orthorexia, therefore further explorations should be conducted in a sample that consists of individuals who score highly on diagnostic measures of orthorexia nervosa.
Additionally, the present study has conducted two mediations where self-compassion and mindfulness acted as mediators in the relationship between perfectionism and orthorexia nervosa. Both self-compassion and mindfulness were significant mediators, which is a novel finding in relation to orthorexia research. Based on the past literature both of these concepts have been successful mediators where perfectionism was one of the variables. For example, Manove and Khoury (2023) found that mindfulness was a successful mediator between perfectionism and societal anxiety, according to the diagnostic criteria distress or impairment of social functioning is a characteristic of orthorexia nervosa (Dunn & Bratman, 2016) Furthermore, mindfulness was also a successful mediator between perfectionism and negative thoughts (Short & Mazmanian, 2013), highlighting that mindfulness could be a significant mediator as orthorexic individuals experience negative thoughts when deviating from their dietary rules (Dunn & Bratman, 2016). Additionally, self-compassion was a successful mediator in the relationship between restrictive eating and orthorexia nervosa (Kalika et al., 2022). The significant mediating roles of self-compassion and mindfulness underscore their potential importance in understanding the mechanisms underlying orthorexia, and the alignment with prior research on perfectionism.
Limitations
The present study has a number of limitations. There is a debate in terms of which orthorexia measure seems more viable. The current study has used the Orthorexia Nervosa Inventory (Oberle et al., 2020) which is the newest measure of orthorexia, therefore, has been used a limited amount in the research (Kalika et al., 2022; Kaya et al., 2021; Oberle et al., 2020). As previously discussed, there could be differences between mindfulness and self-compassion if other measures of orthorexia are used. For example, Kalika et al. (2023) demonstrated that there was no association between mindful eating and orthorexia when using the Dusseldorf Orthorexia Scale; however, Kalika et al. (2022) used the ONI which demonstrated a positive correlation with mindful eating. Therefore, future research into self-compassion and mindfulness should utilise other measures of orthorexia to establish if the findings are replicated. A prospective avenue for further exploration lies in examining the ramifications of healthy orthorexia and the dual capacity of mindfulness-based constructs to both foster and undermine manifestations of both constructive and detrimental forms of orthorexia.
A caution should be taken when interpreting the results due to the small number of participants in this study as well as ratio between the genders. Future studies should utilise higher sample size as well as making sure that the gender ratio is equal as these are important for the generalizability of the study.
Future Directions
As demonstrated by the present study, self-compassion and mindfulness have a mediating capacity with orthorexia. Future research should look into experimental approaches utilising mindfulness and self-compassion-based interventions to determine their effectiveness in reducing orthorexic tendencies. Orthorexia nervosa has gained a lot of popularity with research looking at cross-sectional data, therefore utilising an experimental approach will add further insight into many much-needed interventions for orthorexia.
Furthermore, there is a need for qualitative research when it comes to mindfulness and self-compassion in the orthorexic population. Currently, there is limited literature that explored orthorexia qualitatively (e.g., Cheshire et al., 2020; Valente et al., 2020; White et al., 2021) and to date, no one looked at mindfulness, self-compassion and ON specifically. Gaining a deeper understanding of those concepts would allow further development of potential interventions for the orthorexic population.
Conclusion
In conclusion, ON is positively correlated with perfectionism and negatively correlated to mindfulness and self-compassion. The present study has also conducted a mediation analysis which revealed that mindfulness and self-compassion can successfully mediate the relationship between perfectionism and orthorexia nervosa. The study offers a novel approach to understanding perfectionism with orthorexia, highlighting that self-compassion and mindfulness can be used as key components in much-needed interventions for orthorexia nervosa. Further research needs to explore these concepts further, especially experimentally and qualitatively as this would aid in further understanding of orthorexia nervosa.
Supplemental Material
Supplemental Material - Exploration of the Mediating Role of Self-Compassion and Mindfulness on Orthorexia Nervosa and Perfectionism
Supplemental Material for Exploration of the Mediating Role of Self-Compassion and Mindfulness on Orthorexia Nervosa and Perfectionism by Eliza Kalika, Misba Hussain, Helen Egan, Michail Mantzios in Psychological Reports
Footnotes
Acknowledgements
Thank you to all of the participants who gave up their time to participate in this study.
Author Contributions
Eliza Kalika designed the study, collected data, conducted data analyses, and wrote the manuscript. Michail Mantzios, Helen Egan and Misba Hussain supported the study and critically reviewed the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.