
Abstract
This article investigates whether there are differences in religious and spiritual (R/S) beliefs, attitudes, practices, training, and self-assessed competence between counselors and psychologists in Canada. Researchers surveyed 307 mental health professionals in Canada with two standardized measures (the Assessment of Spirituality and Religious Sentiments Scale and the Duke University Religion Index) and various other questions corresponding to variables investigated or alluded to in past research. We hypothesized that, compared with psychologists, counselors would (a) have stronger personal R/S beliefs, (b) demonstrate more positive attitudes about the appropriateness of using R/S techniques with clients, (c) utilize R/S techniques more in sessions, (d) possess more positive attitudes toward training in this area, and (e) have higher self-assessed competence for working with R/S clients. These hypotheses were generally supported except for the last one: there were no significant differences found between counselors and psychologists in self-assessed competence in working with R/S clients. We compare our findings to those of extant research, particularly the study by Plumb who examined counselors in Canada. On the basis of our findings, we advocate for more systematic cultivation of R/S competence in programs for both counselors and psychologists in Canada.
From the very outset of counseling and psychotherapy services, understanding a client’s religion and spirituality (R/S) is important for contextualizing the presenting concerns that bring them to counseling or psychotherapy (e.g. depression, anxiety, grief), including whether certain beliefs are normative given a client’s R/S or more symptomatic of a clinical diagnosis (Gill et al., 2020; O’Connor & Vandenberg, 2005). Therefore, it has been recommended that mental health professionals routinely assess clients’ R/S during intake (Post & Wade, 2009; Terepka & Hatfield, 2020), which also signifies to the client that it is appropriate to discuss R/S in session (Post & Wade, 2014). This is important because some clients have reported fears that mental health professionals will ignore or be insensitive to their R/S beliefs, or judge them negatively for following a religion (Mayers et al., 2007). In addition, religious and spiritual clients usually prefer that their psychological treatments incorporate their R/S practices and tend to favor interventions that accommodate or incorporate aspects of their R/S (Harris et al., 2016; Stanley et al., 2011). In support of meeting this demand, many religious accommodative therapies as well as nonreligious spirituality therapies have been empirically supported by rigorous research (Captari et al., 2018, 2022). Therefore, psychologists and counselors 1 have an ethical imperative to provide R/S competent and maximally effective services (Canadian Psychological Association, 2017).
Counselors and psychologists tend to agree, in principle, about the importance of competently working with R/S issues in session, but generally remain reluctant to incorporate them into their own practice. Frazier and Hansen (2009) found a consistent disparity between positive attitudes and actual implementation regarding 29 recommended R/S psychotherapy behaviors among US psychologists. Similar attitude–practice disparities have been found among American counselors (Cashwell et al., 2013; Giordano et al., 2016). Looking beyond the United States, Plumb’s (2011) results also point to a disparity appearing to be present among counselors in British Columbia (BC), Canada.
Some evidence suggests that when distinctions are made between R/S, religion is the more likely construct of the pair to be neglected by mental health professionals (Gockel, 2009). For example, in Plumb’s (2011) study, two-thirds of the sampled counselors felt it was appropriate to initiate discussions on spirituality, but less than half believed the same about religion. At least in the United States, neglect of client R/S is particularly prevalent among mental health professionals with the highest level of training. American psychologists, who possess doctorate degrees, have shown lower rates of integrating client R/S into treatment than related groups such as counselors, social workers, advanced practice nurses, and marriage and family therapists (MFTs), who generally hold master’s degrees, despite comparable verbalized support across mental health disciplines for the importance of R/S competency (Oxhandler & Parrish, 2018). However, this research was limited to the United States and the situation in other countries, including Canada, remains unknown.
Although an increase in R/S-related training may be the most apparent actionable solution to help overcome their neglect (Jafari, 2016; Schafer et al., 2011; Vogel et al., 2013), part of a more complete explanation may have to do with the religiosity and spirituality of these professionals themselves. Frazier and Hansen (2009) found that the more religious or spiritual a US psychologist was, the more likely this professional would report employing recommended behaviors related to R/S in the session. Similarly, Cornish et al. (2012) showed a significant positive correlation between counselor R/S and both their perceptions of appropriateness and actual use of R/S interventions in the United States. These quantitative findings fit well with more recent qualitative evidence that clinicians’ own personal R/S supports their integration of the client’s R/S in therapy (Oxhandler et al., 2019).
Mental health professionals in general have long been found to be less religious than the general population (Bergin & Jensen, 1990; Young et al., 2007), with psychologists being among the least (Bergin & Jensen, 1990; Sheridan et al., 1992). Perceptions (van Nieuw Amerongen-Meeuse et al., 2018) and evidence of such a religiosity gap relative to the public have also been noted in Europe (Mandelkow et al., 2022). At a time when 88% of Americans identified with a religion, and 87% viewed religion as very or fairly important in their lives (Gallup, 2002), Young and colleagues (2007) found only 48% of those who were American Counseling Association (ACA) members in 2002 identified as religious. In 2003, only 21% of APA members claimed religion was very important in their lives, compared with 61% of the general US population (Delaney et al., 2007; Gallup, 2002). In 2011, Plumb (2011) found only 24% of clinical counselors in BC, Canada, identified as religious and this can be compared to a study by Clark and Schellenberg (2006), who found 34% of their general sample of individuals living in BC were religious. Therefore, the limited consideration of R/S provided by counselors and psychologists is consistent with their own lower levels of R/S.
Purpose of the study
The purpose of this study was to update, attempt to conceptually replicate, and expand upon a previous investigation of Canadian counselors’ views and practices regarding R/S and integrating R/S into counseling. Plumb’s (2011) study recruited 341 counselors from the British Columbia Association of Clinical Counsellors (BCACC) registry. Plumb’s (2011) questionnaire was derived from questions developed by Prest et al. (1999), and Plumb descriptively examined and grouped the answers to each question individually but did not create a formal scale/standardized measure with her selected questions to assess any higher order constructs or use inferential analyses. Most counselors in Plumb’s (2011) study reported that spirituality, but not usually religion, was important to their lives. Although they typically had positive attitudes about most spirituality-related counseling interventions, less than half of them mentioned using these spirituality-related interventions in professional practice. Her participants also reported fewer positive attitudes about religion-related interventions and infrequently reported using them in their practice.
Plumb’s findings may be outdated, being over a decade old. In addition, Plumb remarked that a limitation of her study was the inability to differentiate results between those who were educated in faith-based programs or received supervised training in faith-based practicums or internships. 2 We noticed three other important limitations of her study that call for a conceptual replication and expansion of her original study. Plumb only sampled from one (BCACC) of two major local associations affiliating graduate-level counselors, resulting in questions about how much of her conclusions apply to local counselors in general versus just counselors who belong to that one particular organization. Moreover, Plumb did not employ any standardized measures in her study to confirm that the constructs she was assessing were being measured in a valid and reliable manner. Finally, by only including counselors, Plumb was not able to make conclusions about any other mental health professionals so as to better describe the overall mental health treatment landscape of what clients seeking counseling or psychotherapy are likely to experience. The present study is the first that has investigated R/S-associated personal and professional differences between psychologists and counselors in Canada. In addition, this study also investigates these potential differences using a standardized measure that has previously been shown to validly and reliably differentiate spirituality from religiosity, something that is done less frequently in research.
Research questions and hypotheses
Our research questions are as follows: (a) Do counselors or psychologists possess higher personal R/S? (b) Do counselors or psychologists have more positive attitudes about the appropriateness of using R/S-associated interventions with clients? (c) Do counselors or psychologists utilize R/S interventions more in sessions? (d) Do counselors or psychologists possess more positive attitudes about training to work with religious and spiritual clients? and (e) Do counselors or psychologists view themselves as more competent to address R/S-related issues in counseling and psychotherapy?
In light of prior studies showing less religiosity among psychologists than counselors in the United States (Bergin & Jensen, 1990; Oxhandler et al., 2019; Sheridan et al., 1992) noting that, as cited above, ACA members were more religious than APA members, and we hypothesized that BC’s counselors’ personal religiosity (H1) and spirituality (H2) scores would be higher than those of psychologists. Although prior research had not specifically compared the spirituality of counselors and psychologists or its relationship to incorporating R/S into sessions, we believed that it would behave similarly to religiosity, given the close relationship of the two constructs (Koenig, 2009).
Because personal R/S has shown a positive relationship with whether a practitioner incorporates R/S into practice (Frazier & Hansen, 2009), we further hypothesized that counselors would report more positive attitudes toward the appropriateness of using religious (H3) and spiritual (H4) interventions as well as be more likely to actually use religious (H5) and spiritual (H6) interventions in session. Similarly, we also hypothesized that counselors would have more positive attitudes toward training to work with religion (H7) and spirituality (H8) in session, as well as greater self-assessed competence in working with religious (H9) and spiritual (H10) clients. In summary, in all five comparisons (personal R/S, attitude about appropriateness, utilization, beliefs about training, and self-assessed competence), we hypothesized that counselors would exceed psychologists.
Method
Participants
At the time of the study, 5395 registered (BC Registered Clinical Counsellors) or certified (Canadian-Certified Counsellors in BC) and 650 BC Psychological Association (BCPA) registered psychologists (combined total: 6,045) were listed active in their respective directories. Compared to counselors, psychologists in British Columbia, obtain further doctoral training and are capable of diagnosing psychological disorders (College of Psychologists of British Columbia, 2014). Counselors in our study reported seeing a mean of 97.3 clients in the past year (SD = 130.2), compared with 97.1 clients seen by the psychologists (SD = 109.3). Thus, caseloads were similar between these groups, with counselors collectively serving more clients than psychologists due to there being substantially more counselors than psychologists practicing in British Columbia. The study sample consisted of 307 participants: 220 counselors (75.0% of whom were registered counselors) and 87 psychologists. This results in an overall representation rate of 5.1%, overall broken down into 4.1% for registered or certified counselors and 13.4% for BCPA-registered psychologists.
The average age was 49 years old (SD = 12.7) with 79 men (25.7%), 224 women (73.0%), and four individuals who identified as nonbinary (1.3%) participating. The sample was 80.1% of European descent (n = 246) followed by mixed (n = 19, 6.2%), and South Asian and East Asian (n = 12 each, 3.9% from each). Other ethnicities of participants at 1.9% or less each included First Nation/Indigenous, Middle Eastern, Jewish, Black, and Hispanic. When asked about their religious affiliation, 58.0% (n = 178) of the sample identified with a specific religion. Christianity was the most frequent religious affiliation (n = 102, 57.3%) followed by “other” (n = 32, 18.0%), Buddhism (n = 19, 10.7%), Judaism (n = 13, 7.3%), Sikhism (n = 6, 3.4%), Islam (n = 4, 2.3%), and Hinduism (n = 2, 1.1%). Responses belonging to “other” included First Nations Spirituality, Paganism, or combinations of religions. Four psychologists (4.6% of sampled psychologists) and 40 counselors (18.3% of sampled counselors) reported receiving their training or graduate education at a faith-based institution. Similarly, four psychologists (4.6%) and 25 counselors (11.4%) completed their practicum or internship at a faith-based organization.
Statistical power of the study
Using G*Power, an a priori power analysis revealed that 210 participants were required to detect a medium effect size of d = 0.5 at α = 0.05 with a power of 0.95, assuming 105 participants in each group (counselors and psychologists). For the allocation ratio of our actually obtained samples (N2/N1 = 223/87 = 0.3901), the same power calculation would recommend minimum subsamples of 187 counselors and 73 psychologists to reach a power of 0.95, which we exceeded in this study, supporting the adequacy of our obtained sample.
Procedures
The study was approved by the institutional research ethics board of the three authors. Participation in the study was voluntary and anonymous with no personally identifying information being collected from respondents. We administered the survey through the online platform Qualtrics. The survey was offered in English. We emailed survey invitations twice to all the registered or certified practitioners listed in the publicly available registries of the BCACC, BC Chapter of the CCPA, and the BCPA list who provided official email addresses. In addition, the CCPA BC Chapter Executive Committee further directly distributed the survey one time to their members on our behalf. Finally, the BCPA and BCACC advertised the survey link through their respective monthly newsletter. Duplicate names of counselors or psychologists were excluded upon cross-checking of the listings, such that those listed on multiple registrars were only surveyed once. Participants that completed less than 96% of the survey and those that completed the survey within an unrealistic time frame (e.g. 2 min) were excluded from analyses.
Measures
Questionnaire
We employed the same definitions of religion and spirituality that Plumb (2011) used, which she derived from Prest and colleagues (1999). Religion was defined as “the formal institutional contexts for spiritual beliefs and practices” (Plumb, 2011; Prest et al., 1999, p. 64). Also consistent with Plumb, spirituality was defined as the “human experience of discovering meaning, purpose, and values, which may or may not include the concept of God or the transcendent being” (Plumb, 2011; Prest et al., 1999, p. 64). These definitions were provided to participants in the survey.
Our questionnaire included 71 closed-ended questions that were modeled closely after the questionnaire used by Plumb (2011). Questions were multiple choice and included 5-point Likert-type scales and check-boxes. We modified some existing questions and added some new questions based on pilot testing and feedback from a small focus group of individuals. First, we adapted the wording of several of Plumb’s questions for clarity and precision. Second, we added questions to address the limitations of her study that Plumb mentioned herself about not being able to differentiate between those with education or training from faith-based and non-faith-based institutions. Third, we added sample descriptor questions around the license/certification of the practitioner, religious affiliation and, if they held a specific religious affiliation, how they would describe their religious orientation. Fourth, for questions asking respondents to rate the appropriateness of the list of R/S-related interventions used in Plumb’s survey, we used the anchors “Strongly Disagree,” “Disagree,” “Not Sure,” “Agree,” and “Strongly Agree.” This involved changing the middle anchor to “Not sure” from Plumb’s “Neutral/Depends on Client” to avoid conflating two different responses into one response option and also to avoid any participants responding that every intervention depends on the client, which would not provide useful information for this study. Fifth, Plumb used an open-ended question to ask participants to list which of the listed R/S-interventions they have used, but to reduce the ambiguity of nonresponses and increase the thoroughness of responses, we used check-boxes to ask whether respondents have used each intervention, one by one.
ASPIRES
ASPIRES is a 35-item self-report instrument designed to measure personal religiosity and spirituality (Piedmont, 2004). It consists of two dimensions: Spiritual Transcendence (ST) containing 23 items and Religious Sentiments (RS) containing 12 items. RS reflect how actively involved a person is in religious rituals and activities and the extent of any difficulties or conflicts with their religion or faith community. ST reflects an individual’s efforts to create a broad sense of personal meaning for life that goes beyond their immediate sense of time and place. These two dimensions consist of five subscales: Religious Involvement and Religious Crisis (composing RS); and Prayer Fulfillment, Universality, and Connectedness (composing ST). Personal spirituality and religiosity are indicated through the score of the Total Spiritual Transcendence scale (a composite of ST’s three subscales) and the score of the Religious Involvement subscale, respectively. The ASPIRES has been found to have solid psychometric support in past research with reliabilities of 0.86–0.94 and both discriminant and incremental validity through predicting psychosocial outcomes and constructs like emotional well-being, psychological maturity, or life satisfaction (Miller, 2012; Piedmont, 2012). ASPIRES has also been found to be both reliable and valid in individuals across a diversity of faiths and across various age groups (Bernt & Schoenrade, 2014; Miller, 2012). We slightly modified two of the ASPIRES items that mention specific religious texts to include other religious texts by adding “holy scriptures” in brackets beside the list of religious texts. We also omitted the demographic questions built into the ASPIRES measure in favor of our own.
DUREL
The Duke University Religion Index (DUREL) is a five-item self-report standardized measure assessing religious involvement (Koenig & Büssing, 2010). It contains subscales assessing each of three dimensions of religion: organizational religious activity (ORA), nonorganizational religious activity (NORA), and intrinsic religiosity (IR). The scale has been successfully used with a wide range of religions and ages (Lace & Handal, 2018). The DUREL has been found to have convergent validity for the three dimensions, high test–retest reliability (r = 0.91), and strong internal consistency (Cronbach’s alpha = 0.78–0.91; Koenig & Büssing, 2010; Lace & Handal, 2018). As Koenig and Büssing (2010) note, certain religious terminology—for example, Bible—may be replaced with Torah or Koran, or church with temple or mosque to better suit the sample. As such, we opted for the term “scripture” to represent all religious texts and included the terms mosque and temple to the item asking for religious attendance.
Data analysis
We computed descriptive and inferential statistics using SPSS-27. Given a large number of comparisons (134), we limited type I statistical errors using the Benjamini–Hochberg procedure with a false discovery rate parameter Q of 0.1 (Benjamini & Hochberg, 1995; Verhoeven et al., 2005). This method safeguards against the unacceptably large increase in type II errors that would be incurred by familywise error rate methods such as the Bonferroni Correction. Its use led us to reject as nonsignificant all tests with p > 0.0284.
Results
Psychologists generally showed lower scores for both religiosity and spirituality than counselors. This was evident not only in the main ASPIRES measures we examined (Total Spiritual Transcendence and Religious Involvement) but also in all three DUREL subscales of religiosity, the ASPIRES prayer fulfillment subscale, and the individual questionnaire items “I am a spiritual person” and “I regularly spend time getting in touch with my spirituality.” These results are shown in Table 1. In addition to being less religious and spiritual, psychologists also described their religious orientation as more liberal than counselors M = 1.39, SD = 0.83 for psychologists (scale = 1, very liberal to 5, very conservative), compared with M = 1.82, SD = 1.83 for counselors; t(148.6) = 3.434, p = 0.001, d = 0.435).
Spirituality and religiosity of counselors and psychologists.
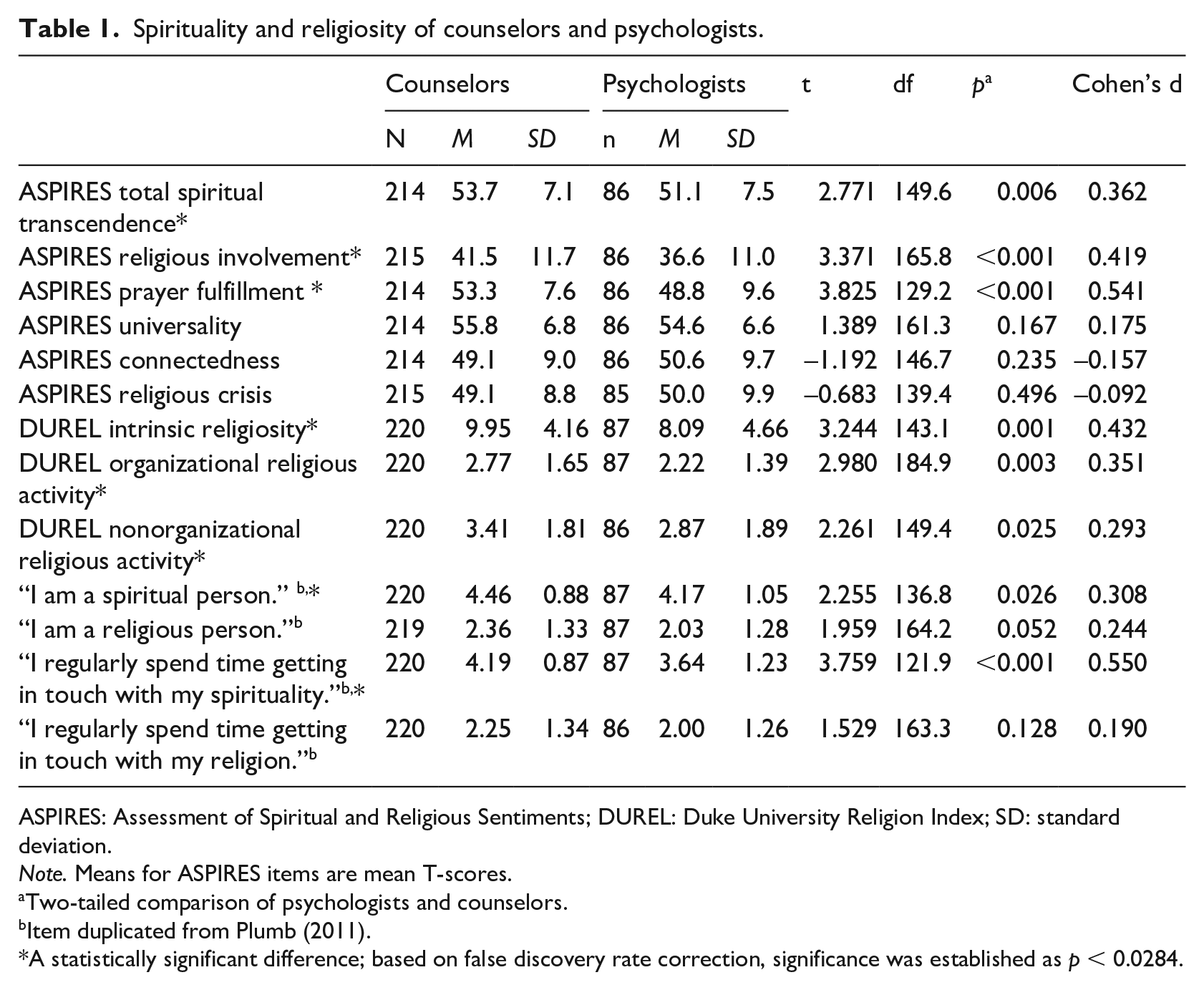
ASPIRES: Assessment of Spiritual and Religious Sentiments; DUREL: Duke University Religion Index; SD: standard deviation.
Note. Means for ASPIRES items are mean T-scores.
Two-tailed comparison of psychologists and counselors.
Item duplicated from Plumb (2011).
A statistically significant difference; based on false discovery rate correction, significance was established as p < 0.0284.
We were curious whether the differences in practitioner religiosity and spirituality could potentially be explained by there being more religious institutions in BC training counselors than psychologists and thus a greater number and proportion of local counselors receiving training in religious institutions. Therefore, we also ran these same comparisons of practitioners’ personal R/S excluding the 44 participants (counselors and psychologists) who attended religious training institutions. This made most personal R/S differences between counselors and psychologists nonsignificant. Those that remained significant were all spirituality-oriented: the ASPIRES prayer fulfillment subscale, claiming to be a spiritual person, and regularly spending time to get in touch with one’s spirituality.
Comparisons between counselors and psychologist on their ratings of the appropriateness of a list of techniques is presented in Table 2. There were nine techniques that counselors viewed as more appropriate: pray together with the client (d = 0.819), recommend a spiritual book (d = 0.519), discuss own spirituality (d = 0.491), use or recommend religious books (d = 0.472), talk with the client about God (d = 0.471), discuss my own religious beliefs (d = 0.349) recommend a spiritual program (d = 0.334), recommend a client join a religion (d = 0.291), and wait until client brings up their religion first (d = 0.140). All remained significant when we excluded from the analysis the participants who were trained in religious institutions (results not shown in the article). Comparisons between counselors and psychologist on their self-reported use of R/S techniques is presented in Table 3. There were three techniques that psychologists reported incorporating significantly less than counselors: using spiritual language or concepts (OR = 0.519, φ = –0.143), pray together with the client (OR = 0.068, φ = –0.195), and talk with the client about God (OR = 0.457, φ = –0.164). All remained significant when we excluded the participants who were trained in religious institutions (results not shown in the article). Comparisons between counselors and psychologists in their attitudes around training to work with R/S clients are shown in Table 4. Counselors were much more inclined to believe in a connection between spiritual and mental health (d = 0.735) and were more interested than psychologists in learning more about integrating client R/S into practice (d = 0.344). These variables remained significant when we excluded the participants who were trained in religious institutions (results not shown in the article). Both counselors and psychologists appeared equally satisfied “with the content related to R/S” presented in their graduate program. Comparisons between counselors and psychologists’ variables reflecting self-assessed competence are presented in Table 4. Counselors and psychologists reported similar levels of comfort when working with religious and spiritual clients, and confidence in their ability to effectively incorporate R/S into practice (Table 4).
Opinions on appropriateness of spiritual and religious techniques.
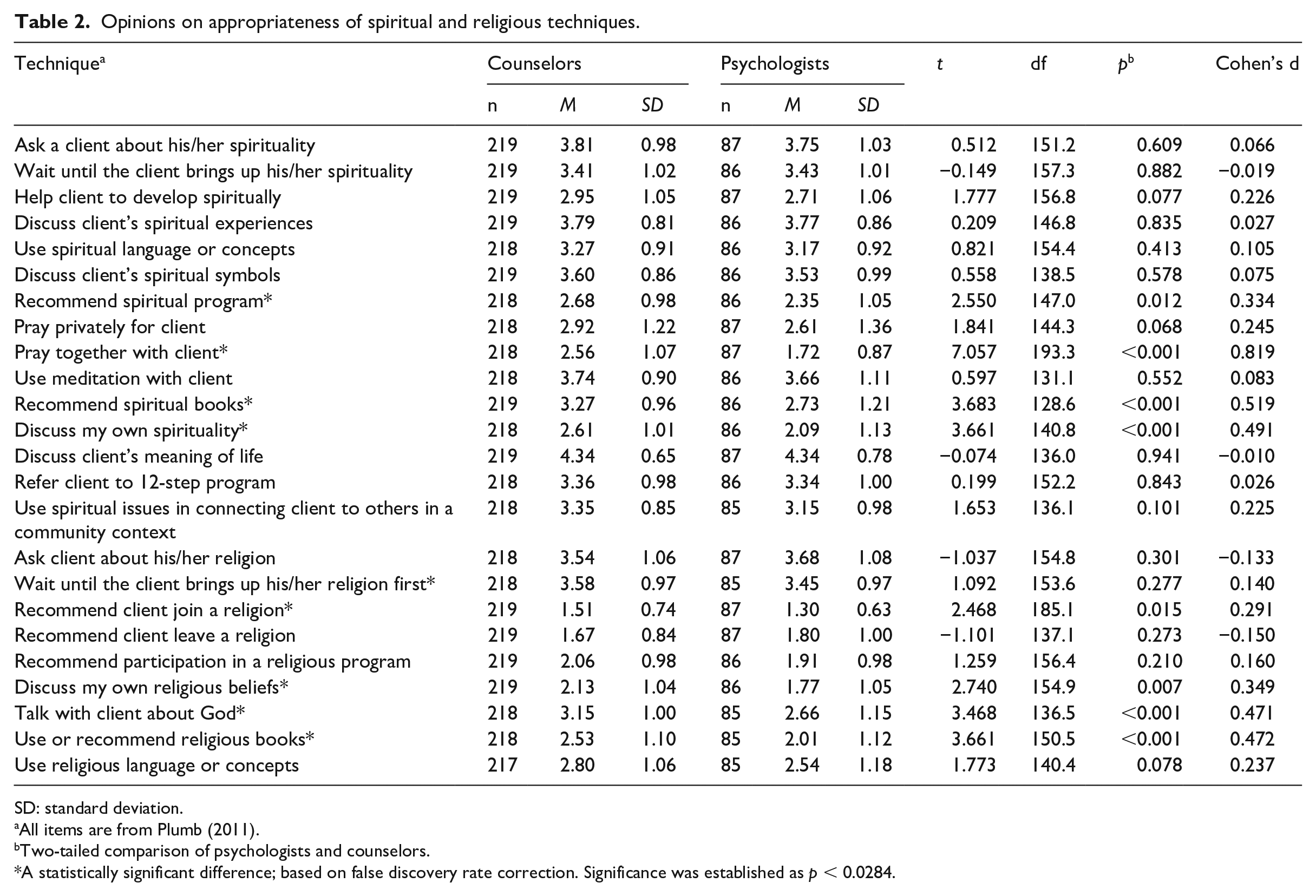
SD: standard deviation.
All items are from Plumb (2011).
Two-tailed comparison of psychologists and counselors.
A statistically significant difference; based on false discovery rate correction. Significance was established as p < 0.0284.
Frequencies and Fisher’s exact test results for counselors’ and psychologists’ use of R/S techniques.
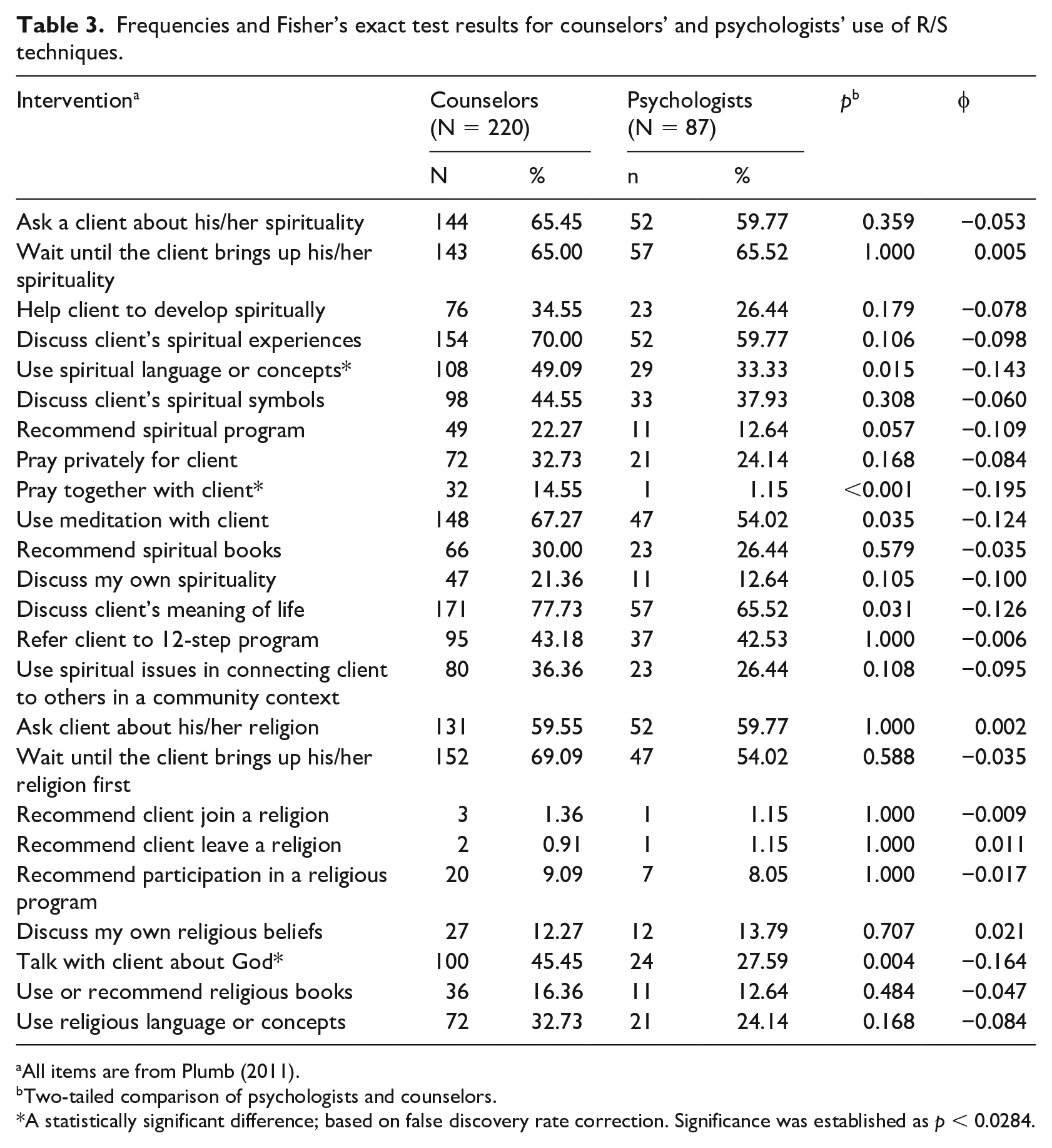
All items are from Plumb (2011).
Two-tailed comparison of psychologists and counselors.
A statistically significant difference; based on false discovery rate correction. Significance was established as p < 0.0284.
Counselors’ and psychologists’ attitudes related to training on R/S and perceived competence.
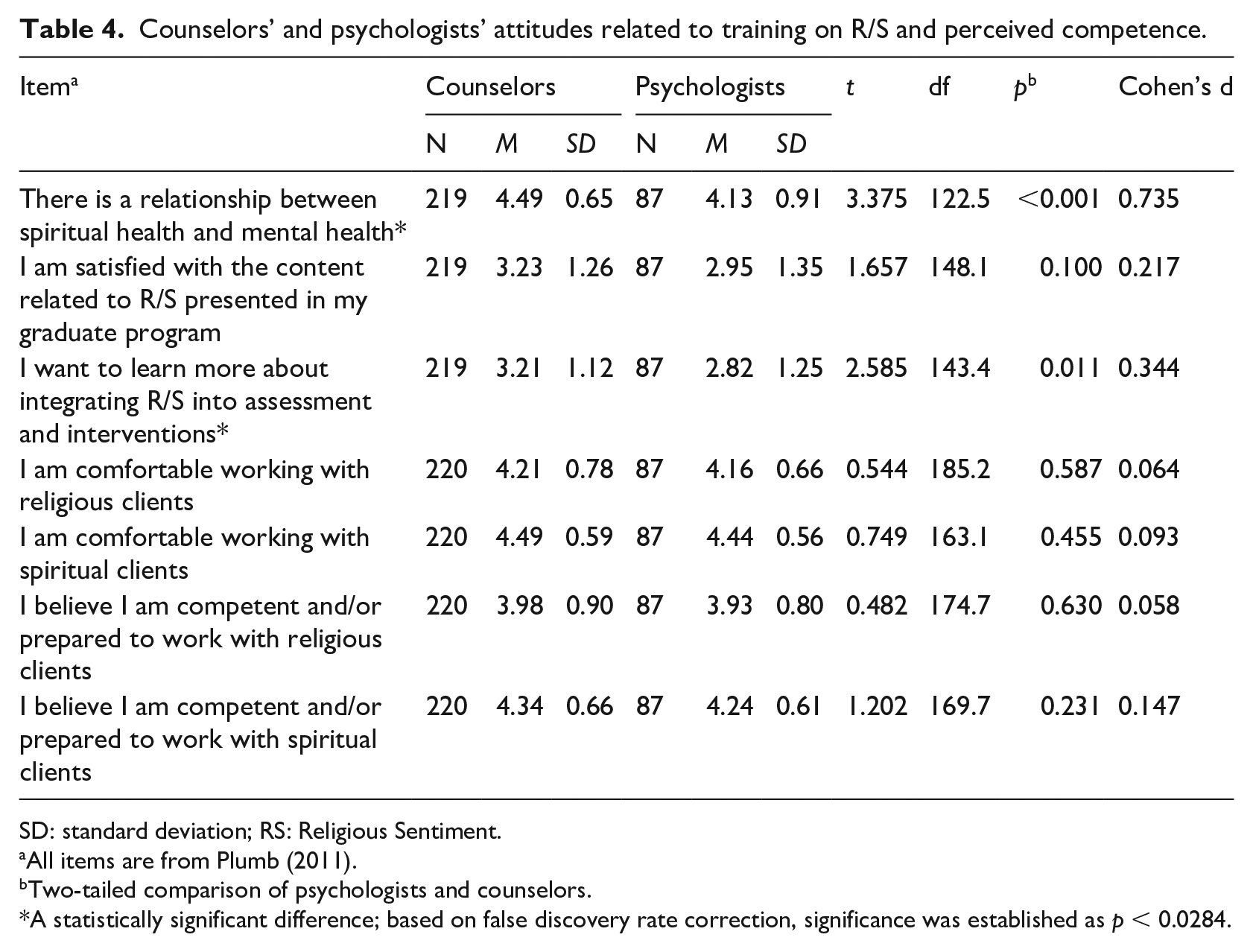
SD: standard deviation; RS: Religious Sentiment.
All items are from Plumb (2011).
Two-tailed comparison of psychologists and counselors.
A statistically significant difference; based on false discovery rate correction, significance was established as p < 0.0284.
Discussion
Researchers have often recognized greater therapeutic benefits when interventions that explicitly address R/S are incorporated into counseling and psychotherapy (Captari et al., 2022; Harris et al., 2016). Unfortunately, most mental health professionals rarely do this (Oxhandler & Parrish, 2018; Plumb, 2011). This discrepancy merits further investigation, including if there are subgroups of mental health professionals with lower usage, who especially could be targeted for increased R/S competency training and attitude change interventions.
The primary purpose of this study was to update, attempt to conceptually replicate, and expand upon a previous investigation of Canadian counselors’ views and practices regarding R/S and integrating R/S into counseling. Plumb’s (2011) results are over a decade old and contained several resolvable limitations that she reported as directions for future research (e.g. assessment of the impact of being trained in a religious institution). In addition, we uncovered several additional limitations of her study that prevented confident generalization of her findings but could also be resolved with modifications to the research design (e.g. sampling both major types of counselors in the local area, use of standardized measures with previous evidence of reliability and validity, use of measures that validly differentiate between religiosity and spirituality). Moreover, by only including counselors, Plumb was not able to make conclusions about any other mental health professionals or differences between mental health professionals, and therefore able to better describe the overall mental health treatment landscape of what clients seeking counseling or psychotherapy are likely to experience. The present study is the first study that has investigated R/S-associated personal and professional differences between psychologists and counselors in Canada. We set out to investigate if there were differences between counselors and psychologists with respect to (a) personal R/S, (b) attitudes about the appropriateness of R/S interventions, (c) usage of R/S interventions, (d) positive attitudes toward training in R/S interventions, and (e) self-assessed competence to work with R/S clients. We hypothesized that counselors would be higher on all variables for both R/S. These hypotheses were all generally supported except the last one: there was no significant difference in self-assessed competence in working with R/S clients.
Religiosity and spirituality of mental health professionals
Consistent with earlier findings from the United States (e.g. Oxhandler et al., 2019), we found that psychologists in BC are less religious than counselors, confirming our first hypothesis. Earlier studies were conducted in the United States, and thus, our study verifies that the trend of lower levels of religiosity among psychologists compared to other mental health professionals extends beyond the borders of the United States. Similarly, we found psychologists to be less spiritual than counselors, confirming our second hypothesis. Although differences were not always statistically significant, the trend was generally consistent and these findings were supported across a diverse set of R/S measures, and more clearly with relatively sophisticated measures such as ASPIRES and DUREL than with more basic self-identification questions.
Based on the ASPIRES subscales, the difference in spirituality between professions can be largely attributed to a difference in the Prayer Fulfillment subscale, whereas the two professions were comparable in terms of the Universality and Connectedness subscales. The Prayer Fulfillment subscale reflects the extent to which a person finds contentment and joy through prayer (Piedmont & Wilkins, 2019, p. 123). Because we also found it to be more common for counselors than psychologists to believe in the divine, perhaps praying makes sense to more counselors than psychologists, making them more likely to pray, and thus to find more opportunities for joy and contentment from prayer. This would suggest that the differences in spirituality result from differences in whether participants tend to pray, which could stem from differences in whether they believe they have someone (or something) to pray to.
Relative to the norms established for the ASPIRES, both counselors and psychologists had quite low averages in religious involvement compared to the general population, reflecting below-average participation in, and importance accorded to, religious activities (Piedmont, 2004, 2012). These findings suggest that mental health professionals in BC may be no less spiritual than other people in the terms used by ASPIRES, but both tend to be decidedly less religious than the general public. Our findings regarding participants’ epistemological views concerning spirituality and religion suggest that belief in a personal God, traditionally predominant in the western world, has been receding over time among mental health professionals, at least in BC. Only 27.1% of counselors in our study believe in a personal God, compared to 34% in Plumb (2011). While such monotheism seems to be receding among BC mental health professionals, most continue to maintain spiritual worldviews; the decline in monotheism has been accompanied by an increasing affirmation of belief in “a transcendent or divine dimension found in all manifestations of nature.” This later position was affirmed by 43.4% of counselors in our study and 38% in Plumb (2011). No prior research on psychologists’ religiosity has been conducted in Canada to compare. However, a similar pattern of reduction is evident for psychologists in our study when compared with Sheridan et al. (1992), who conducted a study in the United States, a country highly culturally similar to Canada. Sheridan’s study found 34% of mental health professionals (almost half of who were psychologists in the sample) had belief in a personal God, compared to only 16.1% of psychologists in our study. Sheridan et al., also found 30% held belief in a transcendent dimension found throughout nature compared to only 39% in the current study. So while mental health professionals may be becoming less religious in Canada, they seem to be becoming more spiritual. These patterns may reflect the broader trend in society of decreasing religiosity (Jones & Cox, 2017; Lipka & Gecewicz, 2017), while also confirming that belief in the transcendent or divine is still less prevalent in psychologists than counselors. Our findings further imply that the lower prevalence of religiosity among mental health practitioners, and particularly psychologists, is a matter not only of involvement in religious activities but also of worldview.
Why would mental health professionals, and psychologists, in particular, be less religious than other members of society? One potential explanation has to do with ways of knowing. It has been suggested that universities’ emphasis on empirical, logical sources of knowledge and the scientific method may especially put the more highly university-educated psychologists at odds with modes of understanding that tend to support religious belief (Jafari, 2016). The longer one is in higher education, the more one is likely socialized into accepting an epistemology divergent with the one most associated with religious faith. Another explanation may be related to prejudice in admissions. Composition of the professoriate on university campuses have become almost entirely ideologically liberal (e.g. Inbar & Lammers, 2012). Academics in a broad variety of disciplines have been found to harbor negative attitudes toward conservatives (e.g. Honeycutt & Freberg, 2017), and religious conservatives in particular (Yancey, 2011), including an inclination to discriminate against them (Honeycutt & Freberg, 2017; Inbar & Lammers, 2012). Perhaps, these attitudes have led to discrimination by the admission gatekeepers of mental health fields or served as a deterrent to a substantial subset of religious people who might otherwise have joined these fields. One example of this may be the increasing practice of requiring a personal statement related to diversity, equity, and inclusion (DEI) for admissions and for the hiring of faculty. Many conservatives and some nonconservative scholars (e.g. Flier, 2019; Small, 2021) believe that these statements implicitly require one to essentially pledge allegiance to and conform to hegemonic liberal viewpoints privileged in academia, particularly those associated with critical race theory—an overall ideology that may not align with the belief systems of highly religious individuals or those that endorse a conservative view of social justice, such as Fretheim (2021) and Thyer (2010). Such dynamics could help explain why only 19 counselors and 4 psychologists self-identified as religiously conservative.
Integration of R/S: attitudes, training, practices, and competence
Plumb (2011) reported that counselors were generally positive or neutral about the appropriateness of spirituality-related techniques and mostly neutral or negative about those related to religion. Counselors in our study generally had similar attitudes to Plumb’s but appeared less enthusiastic about many practices; such as helping clients develop spiritually or discussing clients’ spiritual experiences. By contrast, they appear more positive than in Plumb (2011) about using meditation with clients. This may have to do with the continued rise in the popularity of mindfulness meditation as a general therapeutic technique across various psychotherapeutic approaches since the time of her study (Van Dam et al., 2017).
Compared with psychologists, counselors were more positive about the appropriateness of nine R/S techniques (presented in order of effect size from largest to smallest: pray with client, recommend a spiritual book, discuss own spirituality, recommend religious books, talk about God, discuss own religious beliefs, recommend a spiritual program, recommend a client join a religion, and wait for the client to bring up their religion). The sampled counselors were also more likely to use R/S-related interventions in session, particularly (presented in decreasing magnitude of effect size: praying with a client, talking with a client about God, and using spiritual language and concepts). By contrast, there were no R/S techniques for which psychologists scored significantly higher than counselors—whether in their attitudes or their actual use in practice.
Prior research has highlighted a positive association between psychologists’ personal R/S and use of R/S-informed techniques (Frazier & Hansen, 2009; Oxhandler et al., 2019). Thus, differences in professionals’ own R/S (our study found personal R/S to be higher in counselors) could help explain the difference in clinical attitudes and practices between psychologists and counselors. A plausible explanation could have to do with differences in training. Only 4.6% of psychologists received education from faith-based institutions, compared with 18.3% of counselors. In addition to attracting more religious students, it is very plausible that such programs may often integrate more faith-related considerations into their training than secular programs. However, when we reconducted significance tests after removing practitioners who attended religious institutions, the same differences were generally observed between counselors and psychologists. Training from religious institutions cannot solely explain the differences between psychologists and counselors in how they approach R/S interventions.
Psychologists and counselors both tend to firmly believe in a relationship between spiritual health and mental health, so both presumably would regard navigating the nexus between them to be highly relevant to their training and request more. But counselors believed in the strength of this connection much more (almost a large effect size), resulting in a moderately greater interest in learning more about how to integrate R/S in counseling and psychotherapy. Interestingly, both groups reported very similar levels self-perceived competence for working with R/S clients. However, their notably different attitudes and practices regarding client R/S, with psychologists seeing R/S interventions as less appropriate and using fewer R/S interventions with clients, imply a different story, suggesting differences in understanding what competent practice around client R/S means. It may be relevant to consider the large and growing research base that self-reported high multicultural competence (typically researched with respect to race and ethnicity but generalizable to R/S using a frame of R/S as culture in the general sense) is often not found to be highly related to culturally competent conceptualizations, practices, and client outcomes (e.g. Wilcox et al., 2020). Therefore, equating self-perceived competence with actual counseling/psychotherapy cultural competence with religious and spiritual clients should be done quite cautiously, and the results in our study around personal R/S, training and actual usage of R/S interventions point to the greater competence of counselors over psychologists, as a group—a proposition testable through future research.
The marked discrepancy between counselors and psychologists in personal R/S, positive attitudes toward using R/S interventions, more frequent training in religious institutions, greater usage of R/S interventions in practice, and potentially greater R/S practice competence is not likely to change given current circumstances. The psychologists in this study felt comparable comfort and as competent with R/S interventions and just as competent as counselors despite psychologists’ seemingly lesser training in R/S interventions. These psychologists were also less interested in learning more about integrating R/S into assessments and interventions than the sampled counselors were. These attitudes and belief systems could present a challenge for improving psychologists’ R/S competence in particular.
Limitations and recommendations for future research
Just over 5% of locally practicing counselors and psychologists participated in this study (but 13.4% of BCPA psychologists in particular). Without reliable information about who did not respond to the survey request (we tried sending an extremely short, non-response survey asking why someone chose not to do the survey along with a few demographic questions but only received 35 responses), we are unable to determine if there is a self-selection bias in sampling. It is possible that those who chose to respond to the survey believe and behave differently than those who chose not to respond. This study would benefit from replication, particularly with a greater representation of the local population to assess if sampling bias is present in this study. Providing honorariums to participants in future research for survey completion could help increase response rate. Furthermore, the sampling frame limits the generalizability of the results beyond counselors and psychologists outside of British Columbia. British Columbia has been noted as having the lowest rates of religion of all the provinces in Canada, and this difference warrants further caution when generalizing from our study to other parts of Canada or other countries (Clark & Schellenberg, 2006; Cornelissen, 2021). To overcome these limitations, future research should also expand the sampling frame beyond BC and to other mental health disciplines.
As mentioned in the results section, it was found that psychologists scored lower on R/S measures, engaged in fewer R/S practices, viewed R/S techniques as less appropriate and incorporated them less in practice than counselors. Psychologists also reported having limited education and training on the subject matter. Despite these differences, psychologists viewed themselves as equally competent to address R/S content with clients. This discrepancy is worthy of further inquiry and recommended for future research. For example, do counselors and psychologists demonstrate equal therapeutic outcomes with highly religious and spiritual clients despite these differences between them related to R/S? In addition, future research should investigate potential reasons why counselors possess higher R/S than psychologists.
An additional limitation of our study, due to the focus on replicating Plumb (2011), is that we did not systematically inquire into practitioners’ use of various existing sets of best practices for competent handling of client R/S, such as the Association for Spiritual, Ethical and Religious Values in Counseling (ASERVIC) competencies (Cashwell et al., 2013) or the set of competencies devised for psychologists by Vieten et al. (2016). While our selection of interventions assessed in this study, taken from Plumb (2011), are grounded in face validity, and mostly overlap with existing lists of evidence-based best practices, it is possible that assessing a larger or different list of interventions could lead to different results and conclusions.
If, as our study suggests, there are ongoing deficiencies in practitioners’ inclination and ability to appropriately integrate client R/S into care, perhaps the best context to begin to address such deficiencies is the graduate program. As multicultural practice is becoming more normative and North American populations continue to become more diverse, we contend that a lack of training in the integration of client R/S is increasingly indefensible. Barriers and reservations concerning such training merit further attention and inquiry. We would encourage graduate programs for both psychologists and counselors to ensure that their curricula systematically include content targeting the development of R/S competencies in practitioners. It would be helpful to address not only concerns about general approaches to the topic such as asking clients about their R/S, but also develop best practices concerning creating deeper engagement with client R/S and address any trainee fears, concerns, or biases against doing so. Time may also need to be spent addressing any possible attitudinal or valuing barriers that may prevent many psychologists from implementing appropriate R/S interventions in sessions even after obtaining additional training.
Footnotes
Data availability statement
The primary data reported is original and has not been published elsewhere.
Ethical approval
Conduct of the research was in accordance with and approved by the associated institution’s research ethics board.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.