
Abstract
In South African higher education, students encounter numerous challenges that affect their mental health and well-being. This study examined the incidence and predictors of mental health among 1,366 students at a public, in-contact South African university. A quantitative cross-sectional survey design was employed, using the Mental Health Continuum Short Form alongside measures of life satisfaction, sexual well-being, health literacy, and psychosocial and institutional factors. Descriptive findings indicated that most (66%) students reported moderate mental health, with 28% flourishing and 6% languishing. Bivariate correlations showed strong positive associations between mental health and life satisfaction, sexual well-being, and health literacy. While small significant differences were found across demographic groups, hierarchical regression revealed that psychosocial factors, particularly life satisfaction, components of health literacy, and social support, were the strongest predictors, accounting for the largest proportion of variance in mental health (R² = .61), whereas structural and academic factors played smaller roles. A two-step cluster analysis identified two distinct profiles: a ‘Strained and Stressed’ group characterised by structural disadvantage and fewer psychosocial support, and a ‘Resourced and Supported’ group with greater resource security and psychosocial resources. Cluster membership explained over 12% of the variance in mental health, underscoring the interplay of structural and psychosocial factors in shaping student well-being. Results suggest that interventions designed to strengthen psychosocial resources such as social connection, health literacy, and life satisfaction may enhance students’ mental health and mitigate the effects of structural disadvantages.
Keywords
Introduction
Student mental health and well-being have gained increasing attention globally, as tertiary institutions recognise their impact on academic performance, engagement, and degree completion (Baik et al., 2019; Hernández-Torrano et al., 2020). The World Health Organization (World Health Organization (WHO), 2022) acknowledges that mental health is more than the absence of mental illness and defines mental health as a state of well-being characterised by an individual’s recognition of their own capacities, their ability to manage normative life stressors, to function productively, and to contribute meaningfully to their community. This aligns with Keyes’ (2002, 2005) dual continuum model of mental health which considers positive mental health and mental illness as two independent but related concepts. According to this model, positive mental health (from here on referred to as mental health) comprises both eudaimonic (psychological and social) well-being and hedonic (emotional) well-being. Psychological well-being represents an individual’s intrapersonal and interpersonal functioning (Ryff, 1989), while social well-being (SWB) indicates an individual’s subjective evaluation of their life circumstances and functioning in society (Keyes, 1998). Furthermore, emotional well-being refers to the presence of positive affect and life satisfaction and the absence of negative affect (Diener, 1984). Individuals who experience high levels of psychological, social, and emotional well-being are described as flourishing, while those with low levels of well-being are referred to as languishing (Keyes, 2002). Flourishing appears to protect against mental illness and is associated with lower prevalence of mental disorders as well as superior psychosocial functioning (Keyes et al., 2020; Keyes, 2002). This highlights the importance of promoting mental health and well-being to reduce the risk and severity of mental health issues. While studies have explored mental illness among South African (SA) students (Bantjes et al., 2023; Makhubela, 2021), literature on student mental health and well-being remains limited, with most studies conducted during the COVID-19 pandemic (Graham & Eloff, 2022; Visser & Law-van Wyk, 2021; Wilson Fadiji et al., 2025).
The SA context, characterised by inequality, diversity, and resource constraints, presents specific psychosocial and economic stressors that could affect student well-being (Bantjes et al., 2023). Although previous studies have explored the influence of specific demographic, socioeconomic, or situational factors on SA students’ well-being (Visser & Law-van Wyk, 2021; Wilson Fadiji et al., 2025), this study offers a holistic perspective on the predictors of mental health as defined by Keyes (2002, 2005). It focuses on three interconnected domains that are relevant to SA students: intrapersonal resources, interpersonal factors, and institutional/psychosocial contexts.
First, at the intrapersonal level, cognitive appraisals and personal competencies are central. Life satisfaction, as a subjective hedonic evaluation of one’s life against personal standards (Diener, 1984), is an important indicator of student well-being and is associated with academic performance and mental health (Balkis & Duru, 2017). For SA students facing financial constraints, academic performance, as a potential pathway to economic stability, may be an important domain that influences judgements of life satisfaction. Equally important is health literacy (HL): the ability to access, process, appraise, and understand information about health (Osborne et al., 2022). Maintaining a healthy lifestyle holds psychological benefits, reducing anxiety, stress, and depression (Guntzviller et al., 2017; Jiménez-Pavón et al., 2020). Research on well-being and HL is limited, but findings support the notion that higher HL predicts better well-being, particularly among university students, as their health-related decisions are associated with academic performance, and impact their future health (Whatnall et al., 2022; Zhang et al., 2021). In low-income contexts like Africa, reducing health problems may promote overall well-being. Students thus require adequate levels of HL to be active role players in managing their physical and mental health (Rababah et al., 2019).
Second, the interpersonal domain, often underrepresented in traditional models, is vital for holistic well-being. Traditional models of well-being have largely neglected sexual health and pleasure. There is a growing interest in the ways that sexual well-being shapes holistic health and well-being (Mitchell et al., 2021; Sundgren et al., 2022). Sexual well-being encompasses not only the absence of disease or dysfunction but also the presence of positive aspects such as sexual pleasure, satisfaction, and the ability to form and maintain meaningful sexual relationships as well as to feel comfortable, safe, and respected in sexual relationships (Lorimer et al., 2019). Integrating sexual well-being into analyses of student well-being offers insight into how this factor relates to mental health, particularly considering the rates of sexual violence reported by SA university students (Machisa et al., 2022).
Finally, students’ well-being may be shaped by their broader institutional and psychosocial context. Factors such as sense of belonging, institutional support, and exposure to financial stress may interact with individual resources and thus influence overall well-being (Bantjes et al., 2023). Therefore, to address the gap in holistic, contextually responsive research, this study explored SA student mental health and well-being through the integrative lens of Keyes’s dual continuum model. It examines how predictors from intrapersonal (life satisfaction, health literacy), interpersonal (sexual well-being), and institutional/psychosocial domains contribute to student well-being to guide policy development and inform mental health support services.
The current study explored students’ mental health and well-being from a multidimensional perspective. These research questions guided the study:
Method
Ethical Considerations
The study was approved by the University of Pretoria Faculty of Humanities Ethics Committee (HUM043/0824). Before proceeding with the survey, participants received the study information and gave online consent. Participation was voluntary and confidentiality and anonymity were maintained as no personally identifiable information was collected.
Procedure
This study used data from a student population at a public, in-contact, South African university in Gauteng province. Purposive sampling was used to recruit registered students over 18 years. Participants were recruited during April–June 2025 and the study invitation, including the link to the online Qualtrics survey, was distributed through the university’s student communication channels and social media platforms to all registered undergraduate and postgraduate students.
Participants
G*Power software (version 3.1; Faul et al., 2009) was used to conduct an a priori power analysis to estimate the minimum required sample size for the primary analyses aligned with the study’s objectives. Based on a medium anticipated effect size (f² = .15), an alpha of .05, power of .80, and 11 predictors in the regression model, the power analysis indicated that a minimum sample of 159 participants would be required. The final sample included 1,366 participants. The sample was predominantly composed of cisgender women (assigned female at birth) (80.1%) and students who identified as heterosexual (80.2%). The majority of participants identified as Black African (63.5%) or White (27.5%). Just over half of the students (50.3%) self-reported coming from a middle socioeconomic status (SES) background. The sample was primarily undergraduate students (87.6%), and the most common primary funding sources were the National Student Financial Aid Scheme (NSFAS) (35.8%) and family or partners (31.3%). A full breakdown of all demographic characteristics is available in the Supplementary Materials (Supplemental Table S1).
Measures
Demographic and Institutional Information
Participants completed a demographic questionnaire. Students were also asked to select the extent to which they perceived several institutional factors to influence their well-being using a Likert-type scale from 1 (not at all) to 5 (a great extent): academic pressure (stress/expectations related to academic performance); academic pace (deadlines/speed of modules/assessments); adaptation/adjusting to university life; loneliness; food security; finances; and living situation. These items captured students’ subjective appraisals of these factors, rather than objective measures of the factors themselves. Higher scores suggested a greater perceived influence of a specific item on a student’s well-being. Students also reported on their ability to balance family, studies, and work life. A 3-point scale was used with 1 (rarely), 2 (about half the time), and 3 (most of the time). Higher scores meant better ability to manage family, work, and studies. The single-item measures were chosen to capture students’ subjective appraisals of these domains and were deemed acceptable for this exploratory study, as multi-item scales would increase survey length and potentially contribute to attrition.
The Mental Health Continuum Short Form
The Mental Health Continuum Short Form (MHC-SF) (Keyes, 2009) consists of 14 items that measure different facets of well-being, including emotional well-being (EWB), psychological well-being (PWB), and SWB. Participants responded to several statements using a 6-point Likert-type scale ranging from 0 (never) to 5 (everyday). For continuous scoring, a total score was calculated, ranging from 0 to 70, with higher scores indicating better overall mental health. A categorical diagnosis of flourishing was made when participants responded ‘every day’ or ‘almost every day’ on at least one of the three hedonic well-being (EWB) items and six of the 11 eudaimonic well-being (PWB and SWB) items, with a possible total score ranging between 35 and 70. Participants languished when they responded ‘never’ or ‘once or twice’ on at least one of the three hedonic well-being items and six of the 11 eudaimonic well-being items, with a possible total score between 7 and 14. Participants who were neither languishing nor flourishing were categorised as having moderate mental health (Keyes, 2009). Similar thresholds have been used in previous studies involving South African students (Wilson Fadiji et al., 2025). The MHC-SF has been used in various contexts and has demonstrated good psychometric properties in both international (Lamers et al., 2011) and South African samples (Keyes et al., 2008). Internal consistency in the current sample was robust (Cronbach’s α = .911).
The Satisfaction With Life Scale
The Satisfaction With Life Scale (SWLS) is a five-item instrument measuring global life satisfaction, a component of subjective well-being (Diener, 1984). Items are evaluated on a 7-point Likert-type scale and total scores range between 5 and 35, with higher scores suggesting higher levels of life satisfaction. The SWLS has demonstrated good internal reliability (Pavot & Diener, 2008) and has been validated for use in South Africa (Wissing et al., 2010). Internal consistency in this study was good (α = .843).
The Natsal Sexual Well-Being Measure
The Natsal Sexual Well-Being Measure (Natsal-SW) is a 13-item measure of sexual well-being that captures seven conceptual domains of sexual safety and security, sexual respect, sexual self-esteem, sexual resilience, sexual forgiveness, sexual self-determination, and sexual comfort (Mitchell et al., 2023). Responses are given on a 5-point Likert-type scale, ranging from 1 (strongly agree) to 5 (strongly disagree). The scale has demonstrated a good internal consistency, with a Cronbach’s alpha of .82 reported (de Oliveira et al., 2025). For the present study, positively worded items were reverse coded, so higher scores indicate greater sexual well-being. A mean composite score was then calculated across all 13 items. Internal consistency in the present sample was acceptable (α = .732).
The Health Literacy Questionnaire
The Health Literacy Questionnaire (HLQ) is a multidimensional tool that assesses several domains of health literacy among the general population (Osborne et al., 2013). It has been widely used to measure HL (Leslie et al., 2020; Sarhan et al., 2020). For the current study, only two of the nine subscales were included: Scale 3 – Actively managing my health (AMH) – (Cronbach α = .87) and Scale 4 – Social support for health (SSH) – (Cronbach α = .84). Most HLQ subscales focus specifically on health-related information and activities (i.e., interactions with health care providers, appraisal of health information and using the health care system), which were not relevant to the current study. Active health management and health-related social support have been linked to well-being (Zhang et al., 2021). All nine subscales are independent and can be used separately depending on the research question and aim of the study (Morris et al., 2017; Osborne et al., 2013).
Scale 3 measures the value of health and taking responsibility for health, while Scale 4 concerns people’s support system and whether they receive the support they need. Both scales include five items where participants rate their level of agreement with each statement using a 4-point Likert-type scale ranging from strongly disagree (1) to strongly agree (4).
Analysis
Analyses were conducted using IBM SPSS Statistics version 29 (IBM Corp. 2022). Prior to analysis, all scale-based variables were screened for missingness, internal reliability, and distributional assumptions. Missing data across predictors were low (<1%–2%), and listwise deletion resulted in N = 1,347 for multivariate analyses. Examination of residuals and variance inflation factors (all VIFs < 2) indicated that normality, linearity, homoscedasticity, and multicollinearity assumptions for the regression analyses were adequately met.
Descriptive and inferential statistical analyses were conducted. Bivariate Pearson correlations were conducted to assess the relationships between students’ mental health, life satisfaction, sexual well-being, and HL. One-way analyses of variance (ANOVAs) and multivariate analyses of variance (MANOVAs) were used to examine differences in overall mental health scores (MHC-SF total) across demographic characteristics.
Hierarchical regression analysis and two-step cluster analysis were conducted. The hierarchical regression assessed the extent to which structural (Block 1: SES, food security, financial strain, living situation), academic (Block 2: academic pressure, academic pace, university adjustment), and psychosocial (Block 3: life satisfaction, loneliness, sexual well-being, health literacy, and balance) factors account for variance in overall mental health. The block order was chosen to enter structural and academic contextual factors first, followed by psychosocial variables, so that the incremental contribution of these domains to overall mental health could be examined.
The two-step cluster analysis considers whether naturally occurring subgroups of students can be identified based on the same set of predictors and whether these subgroups differ in their overall mental health. Variables were standardised, and the log-likelihood distance measure was used. Automatic model selection using the Bayesian information criterion (BIC) identified a two-cluster solution. Differences in overall mental health across clusters were then examined to determine whether these subgroups differed meaningfully on well-being outcomes.
Results
Only statistically significant findings with medium to large effect sizes are presented in detail. Additional analyses, and results, are available in the supplementary materials.
Descriptive Statistics and Correlations
Participants reported moderate levels of overall mental health (M = 3.39, SD = 1.05), as well as moderate life satisfaction (M = 3.78, SD = 1.39) and relatively high sexual well-being (M = 3.64, SD = 0.62). Regarding mental health subdomains, PWB was highest (M = 3.73, SD = 1.15), followed by EWB (M = 3.58, SD = 1.29) and SWB (M = 2.87, SD = 1.17). Scores on the two HL domains were also moderate: participants reported average levels of AMH (M = 2.63, SD = 0.69) and SSH (M = 2.85, SD = 0.66). Regarding students’ perceptions of their context, academic pressure (M = 4.33, SD = 0.90) and academic pace (M = 3.99, SD = 1.03) were perceived as having the greatest influence on their well-being, with mean scores approaching ‘quite a bit’ to ‘a great extent’. Difficulty adjusting to university life (M = 3.17, SD = 1.25), financial strain (M = 3.37, SD = 1.33), and loneliness (M = 3.07, SD = 1.45) were rated as having a moderate influence. Food insecurity (M = 2.46, SD = 1.42), living situation (M = 2.57, SD = 1.42), and difficulty balancing life, study, and work (M = 1.93, SD = 0.68) were rated as having relatively lower perceived influence on well-being (see Supplemental Table 2). Descriptions such as ‘low’, ‘moderate’, or ‘high’ levels of variables reflect descriptive interpretations based on sample means relative to the midpoint of each scale.
Bivariate Pearson correlations revealed significant positive associations between overall mental health and life satisfaction (r = .69, p < .001), sexual well-being (r = .39, p < .001), and both health literacy subscales (active management: r = .42, p < .001; social support: r = .54, p < .001).
Based on MHC-SF cut-offs, 28.2% (n = 385) of students were classified as flourishing, 66.2% (n = 905) as having moderate mental health, and 5.6% (n = 77) as languishing.
Group Differences in Mental Health
A series of one-way ANOVAs and MANOVAs were conducted to examine differences in mental health scores across demographic characteristics. While results showed several statistically significant group differences, the effect sizes were consistently small (η² ranging from 0.7% and 2.1%) indicating demographic characteristics alone explained very little of the variance in overall mental health. SES, sexual orientation, and degree programme consistently emerged as the strongest and most interpretable predictors across the mental health subscales (for full results, including non-significant group differences, see Supplemental Table S3).
Predictors and Profiles of Mental Health and Well-Being
To evaluate the relative contribution of structural, academic, and psychosocial variables to students’ overall mental health, a three-step hierarchical multiple regression was conducted using listwise deletion. All predictors, including both significant and non-significant coefficients, are reported in Table 1, although the narrative below focuses on statistically significant effects.
Hierarchical Multiple Regression Predicting Overall Mental Health.
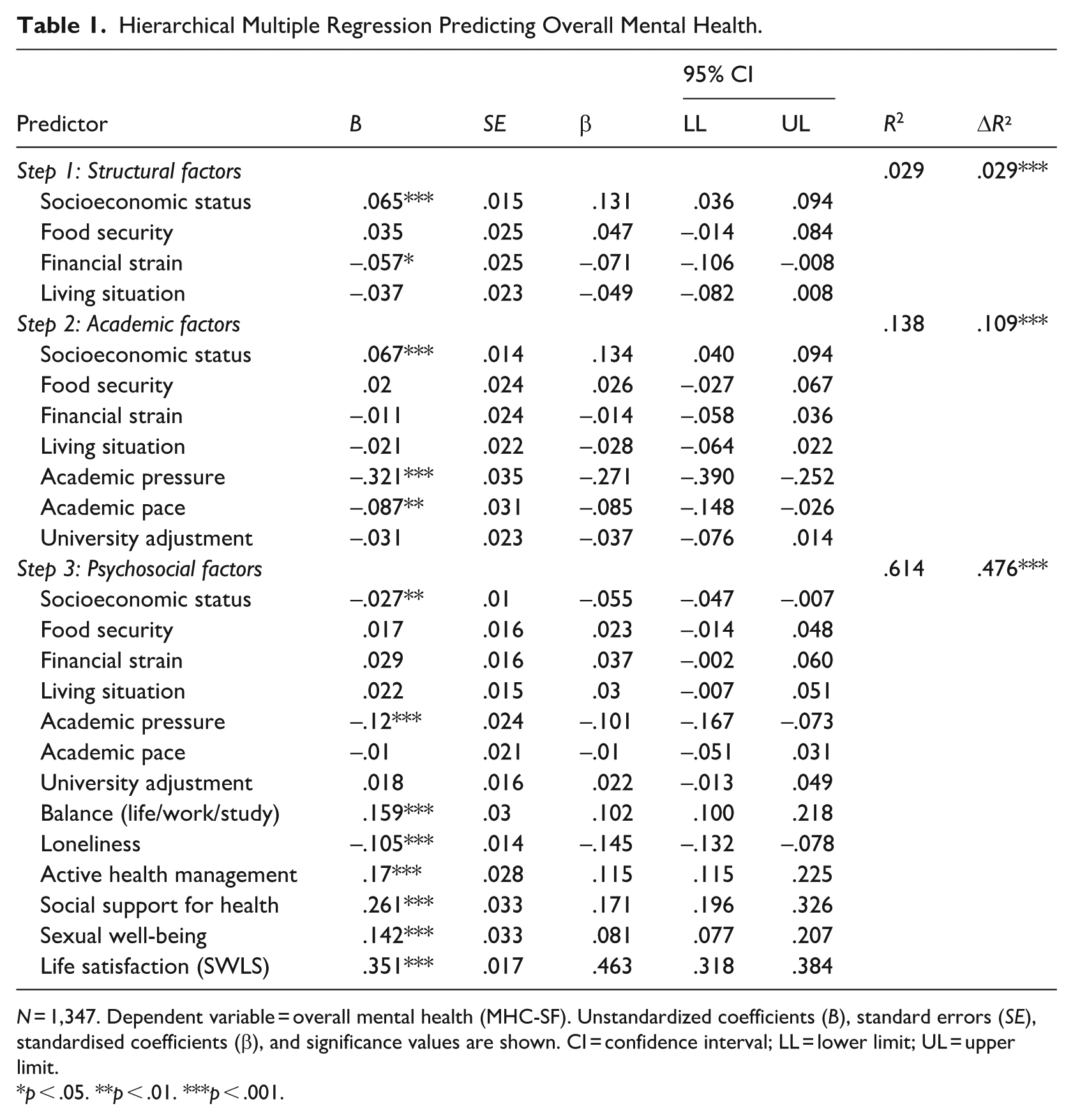
N = 1,347. Dependent variable = overall mental health (MHC-SF). Unstandardized coefficients (B), standard errors (SE), standardised coefficients (β), and significance values are shown. CI = confidence interval; LL = lower limit; UL = upper limit.
p < .05. **p < .01. ***p < .001.
In Step 1 (structural factors), SES, food security, financial strain, and living situation were entered. This model was statistically significant, F(4, 1342) = 10.16, p < .001, and accounted for 2.9% of the variance in mental health (R² = .029). Among these predictors, higher SES emerged as a significant positive predictor (β = .13, p < .001), whereas financial strain was a significant negative predictor (β = –.07, p = .026).
In Step 2 (academic factors), academic pressure, academic pace, and adjustment to university life were added. The inclusion of these variables significantly improved the model, ΔR² = .109, Fchange(3, 1339) = 56.24, p < .001, bringing the total explained variance to 13.8% (R² = .138). In this model, academic pressure (β = –.27, p < .001) and academic pace (β = –.09, p = .005) were significant negative predictors, while SES remained a positive predictor (β = .13, p < .001).
In Step 3 (psychosocial factors), six additional variables were entered: life satisfaction, loneliness, sexual well-being, AMH, SSH, and balancing life/work/study. This final model was highly significant, F(13, 1333) = 162.90, p < .001, and accounted for a substantial 61.4% of the variance in mental health (R² = .614, Adjusted R² = .610). In the final model, the strongest positive predictors were life satisfaction (β = .46, p < .001), SSH (β = .17, p < .001), AMH (β = .12, p < .001), managing life/work/study balance (β = .10, p < .001), and sexual well-being (β = .08, p < .001). Loneliness was the strongest negative predictor (β = –.15, p < .001). Structural and most academic variables were no longer significant once psychosocial factors were included, indicating that psychosocial factors were the primary drivers of students’ mental health outcomes (see Table 1).
A two-step cluster analysis was conducted using the same structural, academic, and psychosocial variables entered in the hierarchical regression. This procedure yielded a two-cluster solution, classifying 1,347 students into distinct subgroups of mental health profiles. Cluster sizes were well balanced, with 700 students in Cluster 1 and 647 students in Cluster 2.
The predictor importance output indicated that the most influential factors distinguishing the clusters were structural variables, including food security, living situation, financial strain, and SES. Psychosocial resources, particularly SSH and life satisfaction, also played a central role in differentiating the clusters. Other predictors such as loneliness, balance, AMH, and sexual well-being contributed to the solution but with less weight, while academic factors were least influential.
Descriptive statistics highlighted clear contrasts across clusters. Cluster 1 was characterised by poorer structural conditions (higher financial strain, lower food security, and less stable living situations), coupled with fewer psychosocial resources (lower social support, lower life satisfaction, and higher loneliness; see Table 2). Students in this cluster reported substantially lower overall mental health (M = 3.04, SD = 1.01). In contrast, Cluster 2 represented a more resourced profile, with greater food security, more stable housing, less financial strain, and higher levels of social support and life satisfaction. Students in this group reported significantly higher overall mental health (M = 3.77, SD = 0.97).
Cluster Differences in Structural, Academic, and Psychosocial Variables.
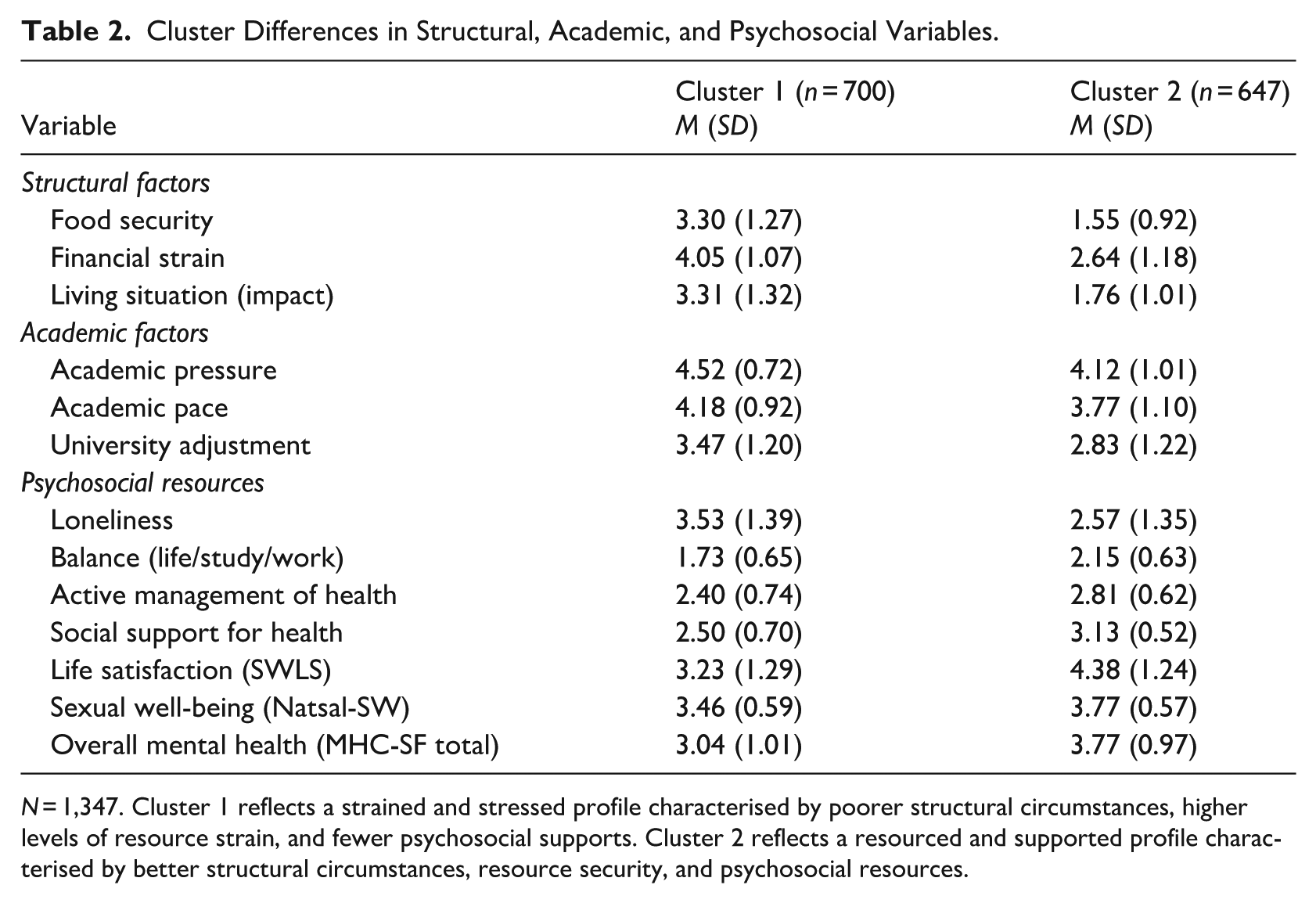
N = 1,347. Cluster 1 reflects a strained and stressed profile characterised by poorer structural circumstances, higher levels of resource strain, and fewer psychosocial supports. Cluster 2 reflects a resourced and supported profile characterised by better structural circumstances, resource security, and psychosocial resources.
An ANOVA confirmed that the difference in mental health scores between clusters was highly significant, F(1, 1345) = 185.52, p < .001, and represented a large effect (η² = .121). This indicates that cluster membership explained over 12% of the variance in students’ overall mental health. This result highlights that students’ placement in these profiles is a powerful predictor of mental health outcomes, more so than single demographic variables as reported earlier.
Taken together, the cluster analysis revealed two broad profiles of student well-being: a ‘Strained and Stressed’ cluster, defined by structural disadvantage and fewer psychosocial supports, and a ‘Resourced and Supported’ cluster, defined by greater resource security and psychosocial resources.
Discussion
This study examined the mental health and well-being of a large sample of university students. Key findings suggest that SA students experience moderate levels of overall mental health and life satisfaction, as well as relatively high sexual well-being and HL. In terms of the well-being domains outlined in the dual continuum model (Keyes, 2005), PWB was highest, followed by EWB and SWB. While structural and demographic factors may have some influence on student well-being, psychosocial resources such as life satisfaction, social support, and loneliness were the strongest predictors of mental health. Cluster analysis further distinguished between two student profiles: ‘Resourced and Supported’ students experiencing higher mental health, and ‘Strained and Stressed’ students experiencing lower mental health.
Key Descriptive Findings
The moderate levels of overall mental health and well-being in the sample are encouraging, particularly following the COVID-19 pandemic, which saw a decline in student mental health due to a lack of supportive social relationships and belonging (Graham & Eloff, 2022; Visser & Law-van Wyk, 2021). While this suggests a potential post-pandemic improvement, the lower scores on SWB, compared with other aspects of well-being, suggest that social support and connection remain challenging.
The relatively high levels of sexual well-being observed in this study represent a novel and important contribution to a literature that has historically overlooked this dimension of student health. Existing research on SA students in higher education has often adopted a risk-oriented lens, focusing on sexual risk behaviours, sexually transmitted infections, and experiences of sexual harassment or violence, both on- and off-campus (Mokgatle et al., 2021; Pillay et al., 2025). While such work is crucial, particularly given the exceptionally high prevalence of gender-based sexual violence directed towards women in South Africa (Merino & Afa, 2025), it has constrained our understanding of sex, sexual health, and sexuality as a potential source of well-being in this population. By highlighting the positive and protective role of sexual well-being in shaping mental health, the present study extends this discourse towards a more holistic and strength-based perspective.
The moderate levels of health literacy in the student sample identifies a potential area for institutional intervention. As HL is a determinant of overall health, predominantly among student populations (Alhussaini et al., 2025) and is associated with improved well-being (Zhang et al., 2021), universities are ideally positioned to address student HL. This is particularly relevant in resource-constrained environments, such as South Africa, where strengthening students’ ability to find and access diverse health information could improve their management of both physical and mental health. In addition, the social support component of HL highlights the value of having a supportive network for both physical and mental health needs.
The Importance of Psychosocial Resources
The results indicate that psychosocial factors explain most of the variance in mental health, while the influence of structural factors was attenuated in the regression model, suggesting an important mediating pathway. Once the psychosocial factors were accounted for, the influence of most structural and academic factors, measured as students’ perceived influence of these factors on their well-being, was decreased, suggesting that their negative perceived effects may be mediated through social connection and life satisfaction. The extent to which students believe factors like academic pressure matter for their well-being may thus be primarily channelled through psychosocial factors. Supportive psychosocial environments may thus buffer potential structural disadvantages. Consistent with theories of subjective well-being (e.g., Diener, 1984) and the buffering hypothesis of social support (Cohen & Wills, 1985), regression analysis indicated that life satisfaction, perceived social support, and active health management were the strongest predictors of mental health. This supports previous research linking social connection and life satisfaction to higher mental health (Kardas et al., 2019; Knoesen & Naudé, 2018) and suggests that while structural support remains important, interventions aimed at improving students’ social connections, life satisfaction, and health management skills may buffer the impact of structural challenges on mental health and well-being.
The Role of Structural and Demographic Factors
While differences by demographic factors were significant, effect sizes were small, suggesting that mental health challenges may be experienced similarly across demographic groups. However, the association between well-being and higher SES is consistent with prior literature (Alivernini et al., 2020; Rahal et al., 2023), suggesting access to resources may act as a buffer for poor mental health, while financial stress reduces well-being (Ryu & Fan, 2023). The relationship between socioeconomic disadvantage and mental health appears to be bi-directional and cyclical (Lund & Cois, 2018). This is especially relevant in the South African context, where many of the observed structural disparities may reflect experiences of marginalisation and discrimination (Bantjes et al., 2023). While prior studies indicated lower mental health for graduate students (Berry et al., 2023), PhD degree level was associated with higher mental health in the present study, potentially indicating greater life stability and autonomy. Higher qualifications may also offer higher career advancement, self-actualisation, self-confidence, social status, a sense of belonging, and positive emotions which contribute to students’ well-being (Graham et al., 2025). Lower well-being among sexual minority students is consistent with the literature (Bantjes et al., 2023) and has implications for developing inclusive campus support. In contrast, mental health scores did not differ significantly by gender identity or primary funding source in this sample, suggesting these areas may be less salient determinants of mental health than the psychosocial resources identified, and warrant further investigation.
Distinct Student Profiles
The cluster analysis identified two distinct student well-being profiles. The ‘Strained and Stressed’ cluster, characterised by structural disadvantages (food insecurity, financial strain) and psychosocial deficits (loneliness, low social support), indicates a high-priority group for support. The ‘Resourced and Supported’ cluster, characterised by greater resource security and psychosocial resources (secure living conditions, stronger psychosocial supports), demonstrated higher mental health. This supports prior findings that structural (e.g., economic) and psychosocial factors predict flourishing (du Plooy et al., 2019). In the South African context, Wissing et al. (2021) found that languishing citizens are often self-focused and motivated by their own needs whereas ‘flourishers’ are more other-focused. Unlike the ‘Resourced and Supported’ cluster, the ‘Strained and Stressed’ cluster may be constrained by meeting their basic needs, thus limiting their capacity to engage socially and live purposefully. The two profiles identified suggest that structural and psychosocial resources interact and concurrently influence well-being, highlighting a need for integrated interventions to improve overall student well-being, and illustrating how the confluence of structural and psychosocial factors identifies the students most at risk.
Implications
The findings of this study have practical implications for university policy and student support. It underscores the need for universities to adopt comprehensive health promotion strategies that include sexual well-being as a core component of student wellness and psychosocial support initiatives. Universities should prioritise psychosocial factors such as building social connections, teaching balance skills, and promoting life satisfaction. This may be done by strengthening peer and social support systems (e.g., through peer networks and student societies), developing initiatives to reduce loneliness (e.g., through community building), and promoting life satisfaction through workshops or well-being literacy. Structural constraints may be addressed through, for example, financial and food security initiatives, and support should be tailored to higher-risk groups such as undergraduate students, sexual minority students, and those from lower SES backgrounds. The moderate levels of health literacy, particularly the social support component, indicate a need for strategic health promotion through social networks where students can seek and share health-related information. Finally, student support services may consider screening for loneliness and low life satisfaction as indicators of potential risk.
Limitations and Future Research
This study has several limitations. First, the cross-sectional design limits causal interpretation and the self-report data are open to response bias. Longitudinal and qualitative studies are proposed. The single-institution sample limits generalisability to other South African institutions. Studies from additional institutions could provide broader insights and enhance generalisability. In addition, the study only focused on two subscales of HL, and future research should consider including a more comprehensive analysis of HL. Some demographic groups were small, thus limiting power. The sample predominately included cisgender women which limits the Generalisability of findings and may bias results towards gender-specific experiences. A larger and more representative sample is thus recommended. The use of single-item measures of institutional factors focused on students’ perceived influence of these domains on their well-being rather than the conditions themselves. Future research should use multi-item measures that distinguish between institutional factors and subjective appraisals to more precisely model their distinct contributions to mental health. Finally, while the use of a composite Natsal-SW score allowed for an overall assessment of sexual well-being, it constrained a more detailed understanding of how specific dimensions, such as sexual safety, comfort, or resilience, contribute to students’ sense of sexual well-being. Future studies should examine these dimensions separately to better understand the distinct ways they shape sexual and mental health outcomes.
Conclusion
SA students experience moderate levels of overall mental health which is strongly associated with life satisfaction, sexual well-being, and components of health literacy. While structural and demographic factors may influence student well-being, psychosocial resources were the strongest predictors of mental health. Consequently, two distinct student well-being profiles were identified: ‘Strained and Stressed’ experienced lower overall well-being, while ‘Resourced and Supported’ experienced higher overall well-being. In accordance with Keyes’s dual continuum model, universities should therefore adopt holistic well-being approaches that integrate structural support with psychosocial resource building, to promote student mental health.
Supplemental Material
sj-docx-1-sap-10.1177_00812463261453200 – Supplemental material for Predictors and Profiles of Mental Health and Well-Being Among South African University Students
Supplemental material, sj-docx-1-sap-10.1177_00812463261453200 for Predictors and Profiles of Mental Health and Well-Being Among South African University Students by Jacomien Muller, Jarred H. Martin, Sonja N. Mostert and Jolize Joubert van Appel in South African Journal of Psychology
Footnotes
Acknowledgements
The authors wish to thank the students who participated in this study.
Ethical Considerations
This study was approved by the University of Pretoria Research Ethics Committee (approval no. HUM043/0824) on December 13, 2024. All participants were required to give informed consent to access to the survey.
Consent for Publication
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.