
Abstract
Health professionals are key role players in the uptake of digital mental health tools; however, research on mental health e-Screening tools largely focuses on psychometrics and tool users’ views. There is currently only one online depression screening tool validated for the South African general public: the adapted online Center for Epidemiologic Studies Depression Scale – Revised. Because practitioners’ perceptions of the tool are lacking, this qualitative study explored health professionals’ perceptions of its properties and potential implementation. Seven participants, consisting of clinical psychologists, counselling psychologists, nurses, and medical doctors in public and private practice in the Gauteng, KwaZulu-Natal, and Western Cape provinces, were purposively recruited. Semi-structured online interviews were conducted, and the data were analysed using thematic analysis. The analysis yielded four themes: (Mis)fit for Purpose; Living in a (Virtue)al Reality?; Human Meets Machine; and A Targeted Approach. The findings demonstrate that the online screening tool has several positive properties and can be improved further with minor additions to contextualise some items and anticipate privacy risks. The tool can be integrated into practice to complement patient consultations in certain circumstances as deemed appropriate by practitioners. These findings provide initial insights into how the South African adapted online Center for Epidemiologic Studies Depression Scale – Revised can be usefully implemented and act as a guide for further tool refinement.
Keywords
The South African Declaration on the Prevention and Control of Non-Communicable Diseases (National Department of Health [NDOH], 2013) outlined 10 targets for 2020 to combat non-communicable diseases in the country, including a commitment to screen and treat 30% more people for mental disorders. South Africa is often lauded for this and other progressive mental health legislation and policies (Mental Health Care Act 17 of 2002; NDOH, 2023); however, the gap between those who need treatment for mental disorders and those who receive it is estimated to be 92% based on crude models of the uninsured South African population who accessed public inpatient and outpatient mental health care in the 2016/2017 financial year (Docrat et al., 2019). The reasons for this large disparity include patients’ and caregivers’ poor knowledge about depression and, consequently, poor help-seeking behaviour, and low detection rates of depression by practitioners due to high patient loads and low confidence in recognising depressive symptoms (Petersen et al., 2016). Online depression screening tools have addressed these factors by informing individuals’ decisions to seek help (Kim et al., 2011; Murphy et al., 2018); prompting further information seeking (Murphy et al., 2018); providing an opportunity for screening to individuals whose health care practitioners had not assessed them during visits (Bradley et al., 2019); and prioritising and streamlining further assessment for high-risk individuals (Sattler et al., 2024).
Screening for mental health problems is a non-diagnostic way to identify individuals who are potentially vulnerable to disorders and in need of further evaluation (American Psychological Association Services, 2014). Screening tools can be administered in several modalities, such as in hard copy, through interviewing, and, increasingly, electronically (Martin-Key et al., 2022). These tests can also be supervised or unsupervised to varying degrees (International Test Commission & Association of Test Publishers, 2022). Practitioners have identified several advantages and disadvantages of supervised electronic mental health screening (e-Screening). For example, in one study examining practitioners’ views of e-Screening using tablets in clinics in the United States, the practitioners found e-Screening useful for quickly and efficiently triaging patients’ mental health needs (Pittman et al., 2019). However, conducting supervised e-Screening in this way also disrupts the workflow within clinics and relies on patients arriving on time to appointments, which is not always the case (Pittman et al., 2019). Added administrative burdens associated with supervised e-Screening, such as handing out electronic devices to patients, have also been highlighted by practice staff in Australian primary care (Proudfoot et al., 2021). Consequently, even though e-Screening devices are available, there is inconsistent e-Screening implementation within and across health care settings (Pittman et al., 2019).
Less research has been conducted that looks at practitioners’ views of unsupervised mental health e-Screening. One Danish study described general practitioners’ views of a web-based version of the Major Depression Inventory (eMDI) (Krog et al., 2018). These practitioners believed the eMDI reduced their administrative workload and improved the quality of patient consultations once the initial challenge of change management was overcome (Krog et al., 2018). Instead, the focus of research on unsupervised mental health e-Screening has largely been confined to the tools’ psychometric properties (Martin-Key et al., 2022) and how individuals perceive self-screening using the tools (Kruzan et al., 2022; Mirea et al., 2021). Importantly, despite positive perceptions of mental health self-screening, few participants in a UK study subsequently discussed their e-Screening results with a mental health professional (Mirea et al., 2021). This suggests that more information is still needed to facilitate the integration of e-Screening tools into routine mental health care. Moreover, health care practitioners play an important role in facilitating the uptake of digital mental health tools (Whitton et al., 2021), which extends to the use of unsupervised e-Screening tools. Research also suggests that practitioners’ attitudes towards screening tools predict whether they use these tools in delivering mental health services (Bjaastad et al., 2019). As such, it is vital that more research is conducted to explore practitioners’ perceptions of mental health e-Screening tools that are presently available to better understand the contexts in which they are useful.
Currently, the only online depression screening tool that has been validated for the South African general population is a web-based version of the Center for Epidemiologic Studies Depression Scale – Revised (CESD-R). The full adaptation and validation processes are reported elsewhere (Hassem, 2021, 2022). The screening tool is a 19-item open-access resource, hosted on the Major Depressive Disorder South Africa website (www.mddsa.co.za) and can currently be accessed by anyone who visits the page. The website also provides additional information on depression to create greater awareness and on available resources. Members of the public who use the tool are given instant feedback classifying their presentation based on three levels of risk (low, medium, and high). Individuals who receive a medium- or high-risk outcome are prompted to request a call from a trained South African Depression and Anxiety Group (SADAG) lay counsellor by making a tick-box selection on the results page and providing their email address and/or phone number. The tool demonstrates good psychometric properties (reliability and validity) and an overall positive user experience (Hassem, 2021, 2022). However, although practitioners and other experts were consulted during the tool adaptation phase, their perceptions of the final tool are not adequately represented. As argued, it is key to have practitioners’ support to effectively utilise the online screening tool to its full potential. This will also contribute to validity arguments around screening tools, including e-Screening, which are a vital and ongoing concern in psychological assessment, particularly in multicultural contexts such as South Africa. Therefore, this study aimed to describe practitioners’ views on the South African adapted online CESD-R, including (1) its properties, such as the nature and presentation of the items and screening results; (2) how it can potentially be implemented, and (3) its applicable contexts.
Method
Design
The study followed a qualitative approach using a qualitative descriptive design (Sandelowski, 2000). This design remains close to the data to offer a comprehensive summary of a phenomenon. This was deemed appropriate, given that practitioners’ views of the South African adapted online CESD-R have yet to be described.
Participants
The study population comprised registered psychologists, nurses, and medical doctors practising in public or private health care in South Africa. These practitioners were selected because mental health problems are addressed in the mental health and general medical sectors in the country (Seedat et al., 2009). Retired health care professionals were excluded to ensure up-to-date views of the country’s current mental health landscape. The participants were recruited using non-probability, purposive snowball sampling (Moser & Korstjens, 2017). A digital information flyer with the study details was distributed via email or private messaging applications to eligible participants within the researchers’ personal and professional networks. Successfully recruited participants were asked to distribute the flyer to other eligible peers. Although every effort was made to recruit more participants, recruitment proved challenging as many individuals who were referred as potential participants either declined or did not respond to follow-ups after showing initial interest in the study. Seven health professionals, two men and five women, did agree to participate, including one clinical and two counselling psychologists, two nurses, one general practitioner, and one intern medical doctor. Five practised in Gauteng and one each practised in KwaZulu-Natal and the Western Cape. Two participants worked in the public sector and four worked in the private sector, with one working in both. The participants had, on average, 24 years of experience. Most participants commonly saw patients exhibiting depression symptoms. Only the intern medical doctor indicated that the number of patients with depression seen depended on the department in which they were completing a rotation. Five of the participants had no previous experience with online depression screening instruments, while two had been exposed to such tools in some capacity.
Procedure
Data were collected through online, semi-structured interviews from September 2022 to January 2023. Google Meet and Zoom were used based on the participant’s preference. The interviews lasted between 25 and 40 min, on a convenient date and time for the participants, and were conducted in English. The participants were sent the link to the South African adapted online CESD-R prior to the interview to peruse the questions, format, and results pages.
Instruments
The interviews were facilitated with an interview schedule with open-ended questions concerning the South African adapted online CESD-R, and demographic questions to describe the sample. Specific questions included, ‘What are your impressions of the online adapted CESD-R screening tool overall?’ and ‘How do you potentially see the tool being implemented in your work context?’
Ethical considerations
This study was approved by the Human Research Ethics School Committee (Non-Medical) of the University of the Witwatersrand (protocol number MASPR/22/03). All procedures were in accordance with institutional and national ethical standards. Participants were given an information sheet explaining that participation in the study was voluntary, and that withdrawal would be without consequences. The information sheet also indicated the option to request a summary of the findings and contained the details of a toll-free, South African mental health helpline in the event of such a need. Written informed consent was obtained from each participant. Privacy and confidentiality were maintained by conducting all interviews in a private room and removing identifying information from the transcripts and reports of results. All data and signed consent forms were stored on a password-protected computer.
Data analysis
Audio recordings of the interviews were transcribed using Microsoft Word transcription software and manually checked for quality. The data were analysed using thematic analysis (Braun & Clarke, 2006, 2019). Each transcript was read several times. Important aspects were highlighted, and initial remarks were noted. A list of codes was generated from an inductive, line-by-line analysis of the transcript as well as deductively based on the study aims and organised into categories. Themes were developed based on the codes and categories. These themes were reviewed and labelled to capture the essence of the theme. Finally, the themes were developed into an analytical account of the data. Rigour was ensured using the Trustworthiness model’s principles of credibility, transferability, dependability, confirmability, and authenticity (Guba & Lincoln, 1994; Lincoln & Guba, 1985). The first author devoted ample time to read the transcripts and the analytic process. This prolonged engagement ensured that the findings were data-driven. Thick descriptions were also used to discuss the sample characteristics, study procedure, and results, including several illustrative participant quotations to justify the findings. Moreover, a detailed audit trail and reflexivity journal documenting the study procedures and the first author’s experiences of data collection were kept and referred to during the analytic process to remain aware of the influence of personal assumptions and expectations on the findings.
Results and discussion
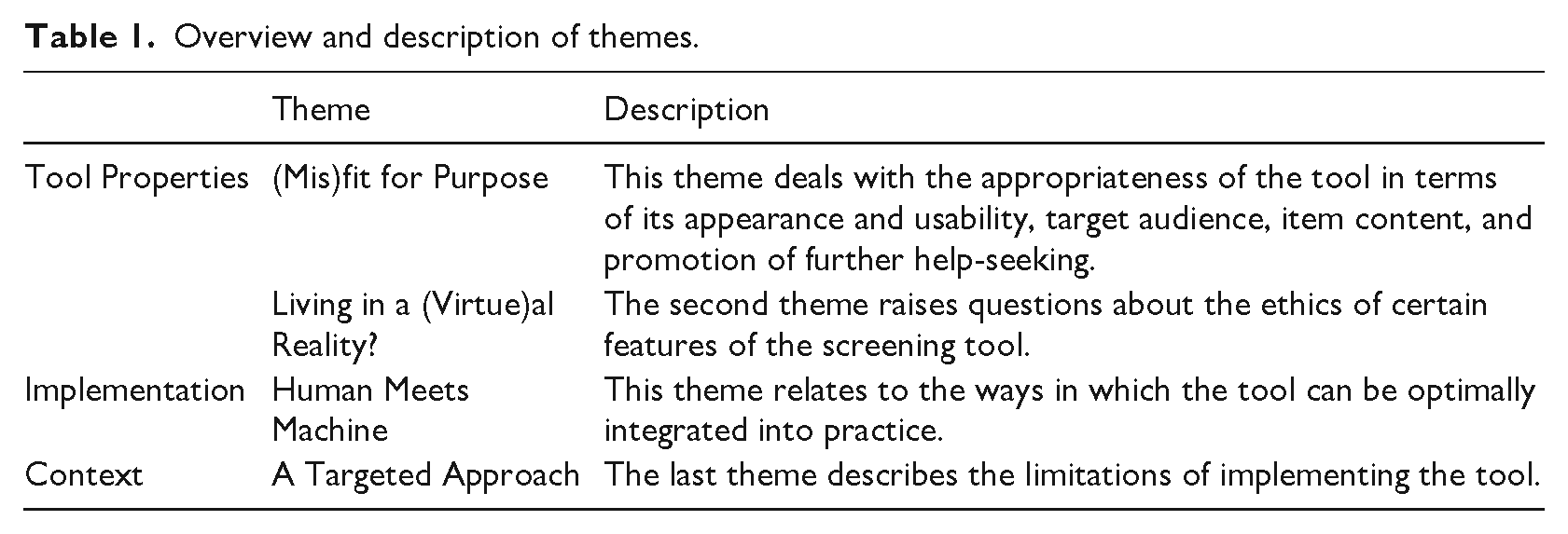
As shown in Table 1, the resulting themes are presented in three sections in accordance with the aims of the study.
Overview and description of themes.
Tool properties
(Mis)fit for purpose
Participants felt that the tool and feedback presentation were aesthetically pleasing and user-friendly, with the potential for the colour-coded risk result to promote urgent help-seeking: Just looking at it, it’s a nice clean format. It’s not, you know, too compact, and I like the results where it says low risk and high risk. Immediately, I suppose, if the person sees that they’re in a red category they would seriously think, ‘Well, I need to go to my . . .’ or, you know, ‘Next step is to see my doctor or go to the clinic’. (Participant 1, Nurse)
Importantly, one participant explained that the tool’s straightforward format is also sensitive to the experience of depressed individuals, who are the intended tool users: Someone that’s really depressed, the layout, you know, it’s kind of simple and straightforward. There’s not a lot of information, you know, it’s not overwhelming that someone that’s really depressed will feel overwhelmed. So, literally, how the questions [are asked], the actual layout of it was for me also positive and not threatening. So, I think that, for someone that is depressed, it’s one page, it’s questions I can just tick. (Participant 6, Clinical psychologist)
These tool features make the adapted online CESD-R accessible and promote its use among individuals who may be more severely depressed and most in need of further evaluation. This is similar to results obtained in a recent study in the United States showing that moderate to severely depressed people were more likely to complete a web-based depression screening as opposed to an in-clinic one (Sattler et al., 2024). The relationship between depression and help-seeking is notoriously complicated (Magaard et al., 2017). Poor knowledge about depression is an identified contributor to poor help-seeking and consequently the depression treatment gap in South Africa (Petersen et al., 2016). The screening feedback’s presentation provides a simple way of aiding individuals to recognise their symptoms as problematic as Participant 1 indicated, without necessarily relying on an established understanding of depression.
However, some participants were concerned about the discoverability of a web-based tool: The only thing that I haven’t put the link in my head to, is how will they find out about it, you know? Like how do you get the word out there that this thing exists for them to do it? (Participant 2, Intern medical doctor) I don’t think people would necessarily go look for a tool. They will go look for the information about depression . . . I don’t think people will necessarily think, ‘Okay, I need to go look for a tool to measure major depression’. I don’t think they will necessarily go for such an explicit search. (Participant 6, Clinical psychologist)
As Participant 6 suggested, many people use the internet to seek out mental health-related information (Jia et al., 2021). However, the participants’ main concern related to which search terms will retrieve the Major Depression Disorder South Africa website which hosts the screening tool, given that the general public is unlikely to use formal terminology or search specifically for screening tools. This also speaks to the poor knowledge about depression in South Africa (Petersen et al., 2016) and suggests that, in order for the adapted online CESD-R to be fit for purpose as an unsupervised e-Screening tool, the general public needs to be informed that the tool is available to them. Having informational posters containing links to the tool in doctor’s rooms and practitioners themselves advocating for the tool’s use during consultations are two avenues that could bring the screening tool to the general public’s attention. Thus, practitioners in medical centres, community health centres, and outreach organisations can consider displaying information leaflets and/or posters on the tool within these settings to facilitate its use.
In addition, certain items were perceived as ambiguous, and participants suggested that they should be contextualised for better understanding: For example, ‘I felt that I’ve been moving too slowly’. What do you mean by moving slowly? Is it physically or is it in my work, or is it I haven’t done things fast enough in my, you know, environment? (Participant 1, Nurse) ‘I could not focus on important things’. I didn’t feel that that was really a depression question, but I know where you’re coming from. But I think that won’t we all answer, ‘Yeah’ most or some of the time? We can’t focus because we are at this stage so overloaded with the lifestyles that we are leading. (Participant 5, Counselling psychologist)
The potential for misunderstanding certain tool items, as suggested by Participant 1, or unintentionally providing misrepresentative answers, as indicated by Participant 5, is a unique problem of unsupervised mental health e-Screening because tool users cannot ask a practitioner for clarification and practitioners cannot ask probing questions for context. This has important implications for the validity of the results which, in turn, may negate the screening feedback’s desired impact on help-seeking behaviour if tool users receive a false low-risk result. However, the screening tool’s very high sensitivity (Hassem, 2022) means that false negatives are unlikely. Nonetheless, the screening tool needs to balance the trade-off more carefully between a short, straightforward questionnaire and including enough information to ensure understanding. This can easily be achieved with the inclusion of a relevant practical example.
Living in a (virtue)al reality?
Some participants also had ethical concerns related to the environment in which an individual completes the screening tool and controlling access to the screening feedback: The problem with online is that sometimes you don’t have privacy if you’re in a house and you can’t go and close the door or it’s not quiet enough. So, it’s not always as private as we think it will be. . . . If somebody uses your laptop, and they see that you have got a medium risk or that you’ve accessed this site, . . . I just think that might put some people in a compromising situation. (Participant 5, Counselling psychologist) The person that has access to that data [from the screening feedback], you have power with that data. . . . Even when noting down your notes, you know, we’re [as practitioners] using clinical codes to actually document it in our notes. And, I mean, if a layperson has to get it [the screening feedback], what can they do with the data? I mean, you can blackmail people saying, ‘Well, I’m going to tell everyone you’re suffering from depression with this’. (Participant 3, Counselling psychologist)
The participants highlighted that, with the growing ease of access to the internet and digital technologies, there is also an increased risk that unintended parties can gain access to sensitive information. South Africans access the internet in their homes, workplaces, educational institutions, internet cafés, and public hotspots (Statistics South Africa, 2022). When it comes to online depression screening, device sharing and the use of public internet facilities mean that the same security offered by in-person consultations with practitioners is less attainable. As such, just as practitioners use clinical codes to document sensitive information, developing precautions for the screening tool, such as password protecting the downloadable screening feedback, may be necessary to better ensure tool users’ privacy.
Implementation
Human meets machine
When considering the implementation of the tool in practice, the participants all described a form of integration between the adapted online CESD-R and formal in-person consultations. This included using the screening feedback as part of client intake after the client completes the tool remotely, or recommending that existing clients, suspected of being depressed, complete the tool in their own time and bring the screening feedback to their next session: If the client could actually print it out and bring it with to say, ‘I completed this and this is my outcome’, and give it to me, then I could obviously see, alright, there’s been a change in sleeping patterns, there’s been a change in eating patterns, and use that as part of a structured interview for the intake. (Participant 5, Counselling psychologist) Let’s say there’s a first session and you talk about things, and I get the impression this person is depressed. I may not necessarily be able to have a discussion about that and what the symptoms are . . . there’s literally just not time. So, then I think this would be ideal. [I could say to clients], ‘Just do this screening, please bring the feedback back and then we can discuss it next time’. So, it would support me in that way . . . where I can maybe then, in a way, fast track the process and also they can come with questions. (Participant 6, Clinical psychologist)
This integrated approach to implementing the screening tool may assist practitioners who are considering incorporating the tool into their practice in several ways. As indicated by Participants 5 and 6, the screening tool can streamline the process of taking patient information by guiding or supplementing in-person consultations. This will give practitioners more time to explore the issues raised in the screening tool and move forward with treatment, if necessary. The tool is therefore useful for primary physicians as it assists them in coping with high patient loads in the South African health care system (Petersen et al., 2016), which puts pressure on practitioners to comprehensively assess their clients’ physical and mental health concerns within short time frames (Abrahams et al., 2023; Minty et al., 2021). Moreover, such an integrated approach may circumvent the participants’ concerns regarding item phrasing in the first theme, as tool users will have the opportunity to ask specific questions, as indicated by Participant 6.
In addition to clients completing the screening in their own time prior to a first or second consultation, one participant suggested that the tool can be completed on clients’ own devices in practice waiting rooms: The best way it will work is to actually have a barcode where you just scan it as you come in . . . While patients are waiting in the waiting room, it can be filled out . . . Some of them, it can be forwarded to them if they prefer, if they want it before then, but it can be done in the waiting room very simply. (Participant 7, General practitioner)
Two participants also suggested that the tool can even be completed during consultations: I think somebody, like a GP, general practice or maybe the clinic services running at Clicks and Dischem and places like that, they might see it as a more useful tool to say, ‘Would you like to actually run through this and let’s get an assessment done before we take next steps’. (Participant 4, Nurse) What could actually be useful is to have this questionnaire, have this website ready then just ask them to just pull out your phone, put it in front of them and then ask them to just do the questionnaire quickly, just take five minutes, maybe, while you’re, I don’t know, writing up notes or something . . . and then, if it says medium risk, or high risk, you can explain what that means. (Participant 2, Intern medical doctor)
These suggestions for the implementation of the tool closely resemble supervised mental health e-Screening. Even though practitioners hold mixed views regarding supervised e-Screening (Pittman et al., 2019; Proudfoot et al., 2021), the adapted online CESD-R has added benefits compared to traditional supervised e-Screening. The adapted online CESD-R, which people can access from their own devices, maintains the efficiency of supervised e-Screening, while disadvantages, such as distributing devices to patients on which to complete the screening, that can disrupt or add to practice staff’s existing duties, are eliminated. Moreover, this approach directly supports re-engineered primary health care and decentralised mental health services to address the country’s depression treatment gap (NDOH, 2023; Petersen et al., 2016). Specifically, the issue of practitioner confidence in recognising depression symptoms (Petersen et al., 2016) is addressed with the screening tool’s implementation as non-specialists can identify patients at risk, even with limited mental health training, which is a necessary but still evolving focus of intervention programmes (Liu et al., 2016).
Context
A targeted approach
Despite being open to integrating the tool into practice, the participants identified various barriers to the universal implementation of the tool, such as difficulties experienced by public health settings due to limited resources and individual differences in literacy, language, education, affluence, connectivity, and technological savviness: From a public health perspective, . . . they are so overwhelmed and overburdened and understaffed. To actually be running or using a tool like this, it would have to be a pretty sharp clinic. . . . It’s possible, but I think it would be quite a significant amount of work to actually get it functioning. (Participant 4, Nurse) I think it will work, but only for certain categories of people, depending on where they are and the language that they speak. This would be very good, for example, for a person who’s got a good command of English, but this questionnaire I feel might need to be translated into all 10 or 12 languages. (Participant 1, Nurse) It’s maybe more applicable to a younger generation. It’s something they’re familiar with, you know . . . For people that are a bit older, I would not necessarily use it. It would depend on each individual’s own comfort with using anything that is online. (Participant 6, Clinical psychologist)
Although the screening tool is targeted at the general public in South Africa (Hassem, 2021), it has certain restrictions. These results speak to the importance of and need for test adaptation and translation in multicultural contexts such as South Africa (Smith et al., 2022). Therefore, in its current form, practitioners wanting to incorporate the adapted online CESD-R into practice will need to use their discretion to decide whether the screening tool is suitable for their work context and, if so, for which of their clients.
Conclusion
This study explored how South African health professionals perceive the properties and potential implementation of the South African adapted online CESD-R. Practitioners viewed many of the tool’s properties positively, such as its ease of use and the presentation of the screening feedback. However, adjustments, including providing illustrative examples for certain items and increased measures to ensure privacy for tool users, will greatly improve the tool. Health care professionals are receptive to incorporating the tool into their practices but under various degrees of supervision. Displaying information on the tool within practices is the most effective way to ensure public awareness of the tool and its integration into health care provision. However, it is currently inadvisable to conduct universal depression screening using the adapted online CESD-R as it should rather be implemented on an individual needs basis. The strengths of the study include offering rich, qualitative insight into practitioners’ perceptions of the tool to supplement the results of earlier, primarily psychometric validation studies. It also provides practical suggestions for practitioners to make use of the tool. However, the study also has limitations. The results present the views of a select group of health professionals from three South African provinces and their relevance for practitioners elsewhere should be carefully evaluated. Input from other key practitioners, such as psychiatrists, community health care workers, and individuals practising in the remaining South African provinces, would provide a more comprehensive view of the tool and whether or how it can be usefully implemented in these contexts. Future research into the adapted online CESD-R could look at applying and evaluating the suggestions for implementing the tool made in this article to assess their feasibility and impact.
Footnotes
Author contributions
A.T.F. and T.H. jointly conceptualised the research topic and design. A.T.F. recruited the participants, conducted the interviews, and transcribed and analysed the data. A.T.F. drafted the article. A.T.F. and T.H. were responsible for critically revising and approving the final version of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.