
Abstract
Youth in low socioeconomic status communities experience multiple risks which disrupts their emotional, cognitive, and psychological development. In South Africa, there is a tacit acceptance of risk constructs as researched globally. This study examines risk occurrence with the aim of identifying and examining the uniqueness of risks in a community sample of youth. Data were collected from youth and their maternal caregivers through interviews and standardized instruments. Youth from grade 7 and grade 10, 9 to 18 years (M = 13.11; SD = 1.54) were recruited. Sixty-five percent were female. Thirty-five frequent risk factors were identified using a z-test for proportion of means. Five risk factors, namely, low household income, race, English not being the primary home language of the parent, low maternal self-esteem, and low dyadic satisfaction, emerged as significant risks. Other risk factors (e.g., single-parent household), which feature prominently in international studies, did not emerge as significantly present. While risk occurrence in our sample shares commonalities with international trends, our study further highlights how risk is underscored and shaped by South Africa’s socioeconomic and political history. We argue that traditional concepts, like family, race, and language require conceptual review when undertaking research and developing policies and interventions that are relevant to South African communities.
Youth is characterized by psycho-emotional and physical changes involving normative but stressful stages. These include a search for identity and autonomy, complex peer relations, and higher scholastic demands, which facilitates behaviours, values, and cognitions necessary for the development of higher-order capacities (Santiago et al., 2016). According to Suryoputri et al. (2022), youth in low socioeconomic status (SES) environments experience additional adversities, like low household income, and increased exposure to violence which studies show, contribute to health disparities and adjustment challenges (Brody et al., 2013; Ciairano et al., 2009; Quon & McGrath, 2014). Davis-Kean et al. (2021), for example, found that parental education is indirectly related to children’s academic outcomes by achievement, while another study by Noble et al. (2015) found that parental education and family income were associated with children’s brain development.
Risk construct
In this context, risks are factors that pose significant threats to youth’s optimal development. While many risks occur at the individual and family levels, others are embedded within the socioeconomic environment. Poverty, for example, is frequently associated with multiple adverse outcomes and often co-occurs with other risks, such as maternal depression and overcrowding (Roy & Raver, 2014). While Rutter (1981) and others focussed on multiple risks, Ackerman et al. (1999) seminally focussed on the assessment of individual risk. They argued that risks are not the same and challenged the assumption that all risks may be equally weighted, especially in the additive risk model. Salience theory (Susser et al., 2006), for example, posits simultaneous investigation and causal identification, without focussing only on levels of putative explanations. In a landmark study in a poor urban neighbourhood in Brazil, Verner and Alda (2004) found that 93% of youth grew up without biological fathers, and low parental education was a high-risk with 71% and 76% of fathers and mothers. Cognizant of these multiple levels of risk, our study builds on single-risk research by focussing on four domains of risks–sociodemographic, psychosocial, psycho-emotional, and biomedical (Evans et al., 2013).
Risks in South Africa
South African research has established significant linkages between mental health and socioeconomic adversities, focussing on protective and promotive factors (Jefferis & Theron, 2017; Meinck et al., 2015; Schwartz et al., 2017; Theron & Theron, 2014). While risk profiles are generally deemed similar to global trends (van Breda & Theron, 2018), racial and gender issues are often overlooked (Modiri, 2012). One damaging effect of apartheid is that the majority of South Africans grew up in a society characterized by violence, mostly influenced along racial and economic lines (Makiwane & Kwizera, 2009). This experience of violence continues to permeate society where, for example, the recent civil unrest, violence and looting in the provinces of KwaZulu Natal and Gauteng in July 2021 (Singh et al., 2021) was seen as being fuelled by ongoing risks like poverty and unemployment (Friedman, 2021).
Much of the previous work on risk is derived from Bronfenbrenner’s (1977) bio-ecological theory of human development which focuses on dynamic interactions between individuals, their families, and their environments (Bronfenbrenner & Evans, 2000). In our study, risk is therefore conceptualized within specific domains based on how and where they occur. We use Bronfenbrenner’s framework to investigate single risks within four domains, viz. the sociodemographic, psychosocial, psycho-emotional, and biomedical domains. The aim of this study goes beyond the reiterative investigation of developmental outcomes of risks and accepts prior studies which have associated a wide range of negative developmental outcomes ranging from economic, social, behavioural, mental, cognitive, and academic outcomes. Our study entails a novel application of Bronfenbrenner’s framework in investigating the occurrence of risks in a low SES sample in South Africa. The investigation of risk occurrence in vulnerable youth offers critical value to inform interventions and further research.
Method
This study is part of a larger collaborative project on risk and resilience among youth in low SES communities in Durban, South Africa.
Participants
The participants were youth (N = 324) in grades 7 (n = 256) and 10 (n = 68) and stayed with their maternal caregivers (N = 324). Participants were recruited from schools in low-SES communities within Durban, South Africa. Maternal caregivers comprised both biological mothers and non-biological maternal caregivers. The communities in Durban are a rich array of racial, ethnic, and socioeconomic backgrounds and arguably constitute an approximate representation of South African society (Britannica, 2022). The communities studied were identified by government census statistics based on income, education, and crime. These communities afforded easy and safe access for research teams. Youth ages ranged from 9 to 18 years (M = 13.11, SD = 1.54). Approximately 65% of the sample was female (n = 210). The youth sample, while diverse, with 55.60% Black African, 23.10% Indian, 14.69% Coloured and 6.88% White, is notably not a close representation of South Africa’s demographics. Maternal caregivers were included in the study to obtain relevant sociodemographic data and to investigate risk profiles specific to maternal caregivers, such as maternal depression and maternal self-esteem.
Instruments
Caregiver interview questionnaires:
The Demographics and Questions about Child’s Health schedule, developed by the Project Care research team, were used to collect data on demographics, family and parental information, and parental assessment of a child’s health.
The Family History of Risk, a 22-item questionnaire used to assess the presence or absence of a variety of events that could be considered as elevating the risk for maladjustment was originally developed by the Programme for Prevention Research in 1992 (Johnson & Kliewer, 1999). The risk constructs included maternal caregiver mental health problems (the maternal caregivers received professional psychological, psychiatric, or social work care for emotional problems); maternal caregiver suicidal ideation and attempts; the child’s mother or father spending more than a week in jail; parental separation or death; foster care; child abuse or neglect resulting in government intervention; financial strain, and the child’s exposure to intimate partner violence. Several studies, for example, the study by Johnson and Kliewer (1999) on predictors of depression in youth in risky neighbourhoods, found that these indicators, including history of abuse, low maternal education, history of domestic abuse, and so on, contributed significantly to children’s depressive symptoms beyond the contribution of demographic and other family factors.
The Dyadic Adjustment Scale (DAS), a 32-item measure, developed by Spanier (1976) assesses relationship quality between married or co-habiting couples. The caregiver responded to a 7-item short form of the DAS, which included abbreviated versions of the Consensus and Cohesion subscales and one item from the Satisfaction subscale. The subscales have a moderate to excellent internal consistency: Satisfaction α = 0.94, Cohesion α = 0.81, and Consensus α = 0.90 (Sharpley & Rogers, 1984).
The Rosenberg Self-Esteem Scale (RCE) (Rosenberg et al., 1995), a self-report measure of global self-esteem, was used to measure caregivers’ self-esteem. It consists of 10 statements related to overall feelings of self-worth or self-acceptance. Reported internal consistency reliability range from α = 0.85 to α = 0.88 for college samples and alpha coefficients greater than 0.7 being reported with African American women (Wesley, 2003).
The Brief Symptoms Inventory (BSI), developed by Derogatis and Cleary (1977), is a 53-item self-report inventory evaluating symptoms orientated towards psychiatric diagnosis. Four of the nine dimensions of the BSI were used, viz., somatization, depression, anxiety, and hostility. Internal consistency was reported with alpha coefficients ranging from 0.71 to 0.85 and retest reliabilities ranging from 0.68 to 0.91 (Borre & Kliewer, 2014).
The Child Behaviour Checklist (CBCL) (Achenbach, 1991) is a parent-report questionnaire. It contains a series of 113 items that help assess a child’s behavioural and emotional problems over the three months preceding the administration of the questionnaire. It assesses internalizing (i.e., anxious, depressive, and overcontrolled) and externalizing (i.e., aggressive, hyperactive, noncompliant, and under-controlled) problems with adequate reliability indices (Achenbach, 1991). In this study, the reliability for the anxiety-depression subscale was 0.81 and 0.77 for the somatization subscale.
The Emotion Regulation Checklist (ERC) designed by Shields and Cicchetti (1997) is a 24-item parent questionnaire measuring emotional patterns of school children. It consists of negatively and positively weighted items to capture emotionality and regulation and comprises two subscales. Studies report good reliability with a Cronbach’s alpha as follows: emotion regulation α = 0.73 and lability/negativity α = 0.92.
Youth interview questionnaires:
The Social Experiences Questionnaire (SEQ-S) is a self-report measure of children’s experience of relational victimization, overt victimization, and cyber-victimization derived from the Problem Behaviour Frequency Scales by Crick and Grotpeter (1996). The instrument’s internal consistency ranges from 0.77 to 0.80.
The Survey of Children’s Exposure to Violence, 40-item survey developed by Richters and Saltzman (1990), measures children’s exposure to community violence. It assesses the frequency of victimization by witnessing or hearing about 20 different forms of violence and violence-related activities. Satisfactory reliability (test–retest, r = 0.90; internal consistency, α = 0.85) has been reported (DuRant et al., 1994).
The Peer Deviance Scale (PDS), developed by Loeber et al. (1998), by expanding a scale from the Denver High Risk Delinquency Survey, is a 15-item scale that assesses youth’s reports of a friend’s involvement in deviant activities. The targeted behaviours include aggression or violence, substance use, and delinquency. Reliability for the PDS has been reported at 0.86 and the Cronbach’s Alpha was α = 0.86
Kovacs (1992) developed the Children’s Depression Inventory (CDI) as a 27-item self-report measure of cognitive, affective, and behavioural symptoms of depression in children. It has established reliability and validity for describing depressive symptoms, has good correlation with other scales, diction validity for suicidal ideas, and high predictive validity for suicidal ideas (Bang et al., 2015). The CDI has good sensitivity and specificity as well as a relatively high test re-test reliability and internal consistency with coefficients ranging from 0.71 to 0.89 (Kovacs, 1992).
The Children’s Somatization Inventory -Short Form (CSI), first used in a paediatric sample, contains 18 items reflecting somatic symptoms on a 5-point scale with higher scores indicating a higher intensity of symptoms (Walker et al.,1991). Studies have reported good internal consistency with a Cronbach’s alpha of 0.88 for the total score.
The 37-item self-report inventory, namely, the Revised Children’s Manifest Anxiety Scales (RCMAS) by Reynolds (1980) assesses emotional and physical symptoms of anxiety. It includes the physiological anxiety subscale, worry and oversensitivity subscales, and the social concern (fears) and concentration subscales, with a reported coefficient alpha, α = 0.80, for the total anxiety scales (Reynolds & Richmond, 1978). Studies also supported the construct validity of the RCMAS as a measure of chronic manifest anxiety.
The Experiences in Close Relationships (ECR), developed by Brennan et al. (1998), is a 36-item youth self-report measure of attachment style, using avoidance and anxiety subscales as continuous variables. It has good reliability and internal consistency with anxiety α = 0.90 and avoidance α = 0.91 (Cohen et al., 2011).
The Children’s Emotion Management Scales (CEMS) by Zeman et al. (2002) measures a child’s ability to manage emotional arousal of anger and sadness within three subscales, viz., inhibition, dysregulated expression and emotion regulation coping. These subscales have good reliability with a coefficient alpha range of α = 0.62 to α = 0.77 and a test re-test reliability range of α = 0.61 to α = 0.80.
Data from the interviews and the instruments, informed by the seminal works of Evans et al. (2013) were used to identify 35 risk factors.
Procedure
Public schools in low-SES areas in Durban, South Africa, were identified. School principals were contacted, and meetings were held with the principals to explain the purpose of the project, study objectives, the school’s involvement, and benefits to the school. Youth were briefed on the study using a standardized script and were invited to voluntarily participate in the study. An information pack comprising an introduction letter addressed to the maternal caregiver, a permission letter from the principal, a caregiver reply slip, and consent and assent forms, was given to the youth. Youth and caregivers who agreed to participate provided written consent and assent forms and were subsequently contacted for home-based interviews. Interviews were conducted at caregivers’ homes by trained research assistants.
Ethical consideration
Study approval was obtained from the University of KwaZulu Natal’s Biomedical Research Ethics Committee of the University of KwaZulu-Natal (BE052/11), the KwaZulu Natal Department of Education and the principals of participating schools. As a gesture of appreciation for time and effort, each participant was awarded a shopping voucher.
Data analysis
Data analysis was performed using SPSS version 27. Continuous variables were summarized as mean ± standard deviation (SD) and compared using the youth’s t-test while categorical variables were summarized as proportions. Thirty-five of the most frequently identified risks in the literature were recorded on an ordinal scale and for the purposes of classification, each variable was split into two, based on whether the values were below the mean (coded 0) or above the mean (coded + 1). For each study participant, we determined the frequency of 0 and 1 with respect to each variable. A z-test for proportions of means was used to determine if the numbers of 0 and 1 for each variable differed significantly.
Results
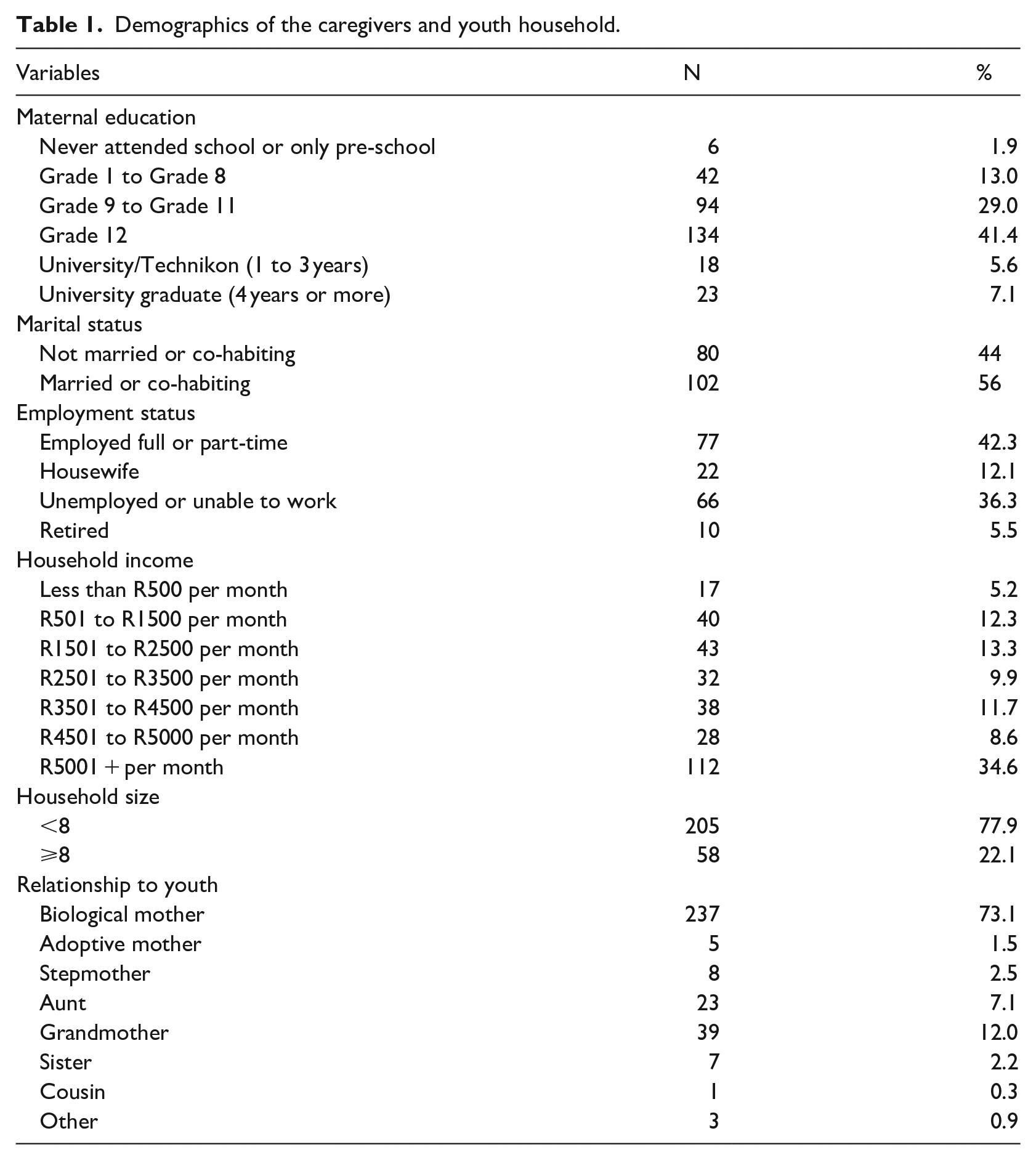
Demographic details of the caregivers are found in Table 1. Maternal caregivers’ ages ranged from 21 to 75 years (M = 41.57, SD = 9.86), with most being biological mothers (73.1%). Other maternal caregivers were adoptive mothers, stepmothers, aunts, grandmothers and sisters, cousins, and others. Most caregivers had a high school education, and a third were unemployed or unable to work. Household incomes were diverse, with 142 (43.8%) reporting unstable income.
Demographics of the caregivers and youth household.
Thirty-five risk factors were examined using a z-test to compare the means of risks reported ‘present’ to means of risks ‘not being present’. Based on Bronfenbrenner’s (1977) theory and the seminal work of Evans et al. (2013), risks were categorized into four main domains, namely, the sociodemographic, psychosocial, psycho-emotional, and biomedical domains. Table 2 shows that of the 35 risks examined, five risks, namely, ‘low household income’ (61.4%), ‘race’ (93.2%), ‘English not being the primary home language of the parent’ (63.6%), ‘low maternal self-esteem’ (80.2%), and ‘low dyadic satisfaction’ (78.5%) were significantly present, while many risks emerged as not being significantly present. While there was no significant difference in proportions reporting single-parent households and not reporting as single-parent households, (z = −1.65, p > .09), there was nonetheless a high percentage of single-parent families in our sample (45.4%). Similarly, there were not significant differences in low maternal education (z = −1.44, p > .15), with the percentage of those at risk at 46.0%.
Exploratory analysis of study variables.
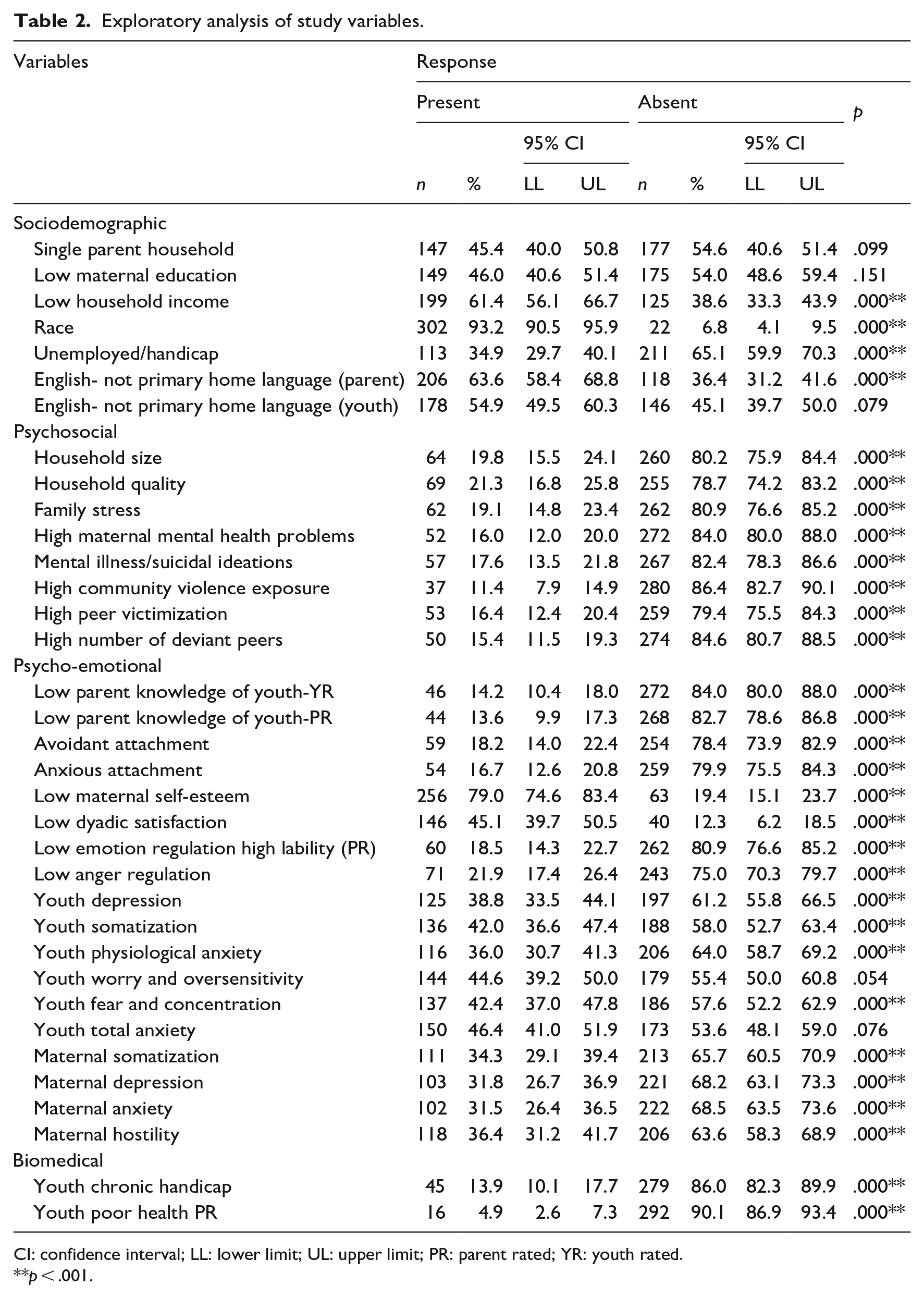
CI: confidence interval; LL: lower limit; UL: upper limit; PR: parent rated; YR: youth rated.
p < .001.
Interestingly, in international studies, single-parent households and low maternal education often emerged as significantly high risks (Amato et al., 2015; Arroyo-Borrell et al., 2017). English not being the primary home language of the youth (z = 1.76, p = .08), youth worry and oversensitivity (z = −1.93, p = .54), and youth anxiety (z = −1.29, p = .20), are other notable risks that are not in keeping with international findings (Figure 1).
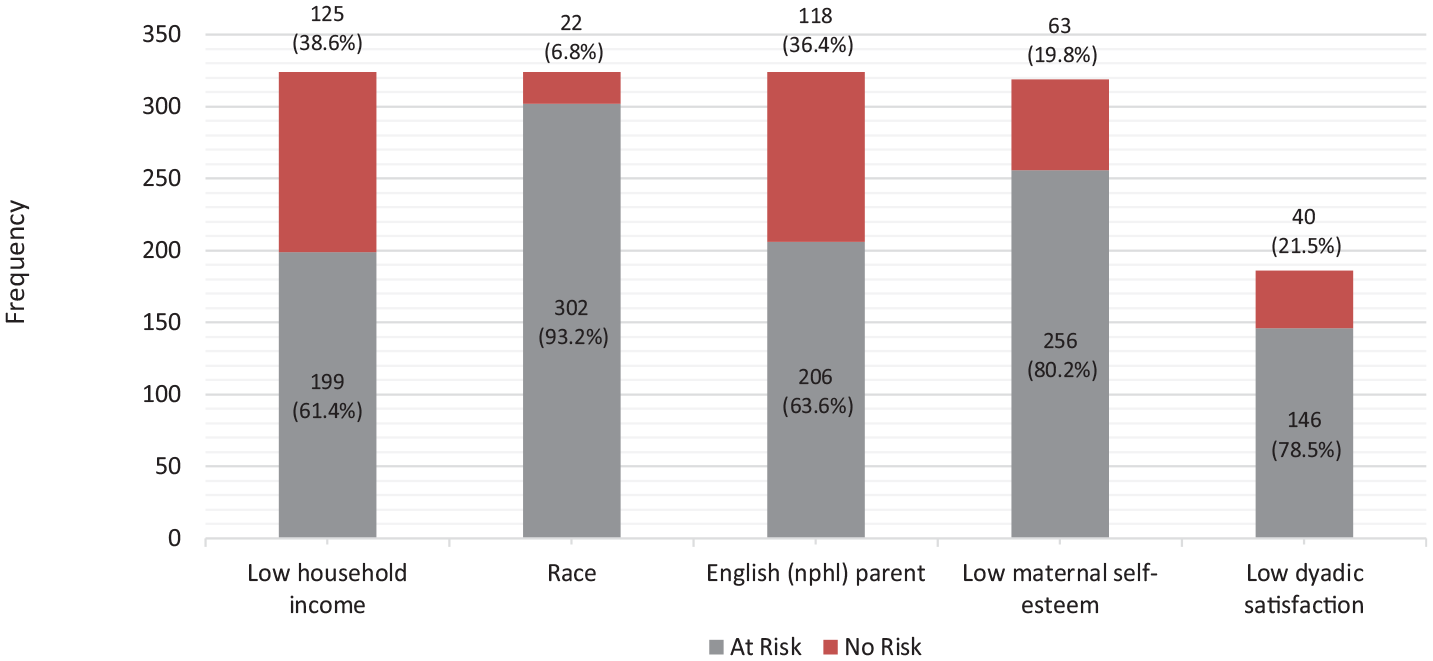
Five risk factors with a statistically significant difference in the proportion of presence vs. absence.
Biomedical markers did not emerge as significantly present, which could be due to youth having developed biomedical resilience or desensitization to the chronicity of risks.
Discussion
This study identified risks across the sociodemographic, psychosocial, psycho-emotional, and biomedical domains. In South African research, risk is mostly seen to occur in much the same way as it does globally (Jefferis & Theron, 2017) and while there is an inclination to accept global trends, South Africa’s unique socio-political history necessitates a re-examination of this tendency. The apartheid system not only classified and segregated races but also governed with differential and discriminatory racial policies. The trajectory of youth risk exposure and multi-generational risks is steeped in this history. Our study therefore includes diverse race groups to illustrate this unique burden of risks.
Five risks emerged as significantly present in our sample, viz. “low household income,” “race,” “English not being the primary home language of the parent,” “low maternal self-esteem” and “low dyadic satisfaction” (referring to the low communication and low quality of relationship between parents in the family). Low income is not only a main contributor to poverty, but also contributes to a higher allostatic load with wear and tear on physical health (Khullar, 2018). Low income contributes to poor health which in turn contributes to low income by limiting one’s educational attainments, ability to work, and economic opportunities, leading to a negative feedback loop. According to Vogel (2019), poverty is the single most important determinant of ill health, contributing to one in five youth experiencing mental health problems. Our study indicates that while there was no statistically significant difference in occurrence between youth that reported mental illness or suicidal ideations and those that did not, the reported occurrence of youth depression (38.8%) and youth total anxiety (46.4%) on the contrary, remains high. Low income is also linked to children’s neurocognitive functioning, including language development, memory, self-regulation, and socioemotional processing (Hackman et al., 2010). Blair and Raver (2016) add that poverty affects children’s health through the toxic effects of stress on the brain. Duval et al. (2017) found that those at higher-income levels showed higher hippocampal activation and recognition accuracy than those at lower-income levels, suggesting that income is more strongly associated to brain development in youth than may have been previously thought.
By 2018, more than half of South Africans (55.5%) were considered poor (Maluleke, 2018). The redress of past socioeconomic disparities has been extremely slow (Segalo, 2015) and the previously disadvantaged continue to suffer socioeconomic inequities. The reality of post-apartheid South Africa is that communities and public schools continue to be segregated along racial and ethnic lines, inadvertently re-enforcing racial self-identity (Modiri, 2012). Lee et al. (2020) found that African Americans transitioning to adulthood demonstrated varying levels of perceived racial discrimination (PRD), suggesting that if race is salient to one’s image, then an individual is more likely to make continuous negative attributions to self-identity. Like income-based health disparities, the literature suggests that race-based health disparities still define much of the South African landscape (Lee et al., 2020; Sanders-Phillips & Kliewer, 2019). The deconstruction of negative attributions in racial identity, therefore, ought to be central in policies and programmes aimed at empowering youth, especially in educational and employment challenges and in redressing historical inequities of resources.
Language, as an extension of racial and ethnic identity, defines one’s ethnic group, social identity, and status. Krugel and Fourie (2017) posit further that language and communication is fundamental to development and learning. South Africa has 11 official languages with a multilingual population fluent in at least two languages. English not the primary home language of the parent (and of the youth) presents as a unique enquiry of this study. Parents whose primary home language is not English often view English as the language that enables access to knowledge and is a pathway to success and scholastic achievement. Parents may likely experience a sense of powerlessness in supporting English usage, and the related sense of social standing (Saneka & de Witt, 2019). English not being the primary home language of the youth did not emerge as a significantly present risk, notwithstanding the high occurrence (54.9%). Low maternal self-esteem and parents’ dyadic relationship also emerged as significant. A three phased web-based study by Zemp et al. (2016), for example, found that children exhibited internalizing and externalizing problems with parents who reported relationship difficulties. Youth may also externalize distress in the form of aggression, bullying, antisocial behaviour, delinquency, and vandalism. In addition, youth from high-conflict homes are more likely to exhibit poor interpersonal skills, low problem-solving abilities, low social competence, and to experience physiological reactions related to stress. Our study, in uncovering the occurrence of these psycho-emotional risks, compels more research on maternal mental health and parental relationships and on parent-focussed interventions as a buffer against externalizing and internalizing problems.
Whereas international studies show that single-parent households present significantly in low SES communities (Evans et al., 2013), in our study, it was not significantly more present. Under apartheid, Black African men, especially, were forced to leave their homes and relocate in search of employment in urban areas, resulting in a preponderance of single-parent families. Factors such as death due to HIV/Aids and violence have further shaped family structures, ranging from traditional two-parent families to grandmother as primary parent, to child-headed families. The concept of family, therefore, needs be revisited, given that the family unit is a dynamic agent for upliftment and empowerment of at-risk youth (Scharte et al., 2013).
An additional maternal risk, which was high in occurrence but not significantly present was low maternal education. This may be explained by the historical ‘community awareness’ of the value of education in overcoming poverty, challenging inequities, and improving one’s circumstances. It was not uncommon for low SES communities to ‘self-fund’ state-aided schools and educational infrastructure (South African History Online, 2016, 2019). Research suggests that more highly educated mothers provide more stimulating activities and engage in higher-quality interactions with their children (Jeong et al., 2017). While Prickett and Augustine (2016) report a variety of linkages between low maternal education and parents with lower knowledge of childhood development, there are numerous examples across racial and ethnic groups which demonstrate that even under adverse psychosocial and economic conditions, people are known to achieve various levels of academic, professional, and business success (Vivier, 2020). This suggests that despite parents having low education, other factors like significant relationship between the families’ adaptation and intrafamilial support, family hardiness, a positive approach to problems, and religion are some of the key factors that motivate and inspire success and resilience (Greeff & Fillis, 2018).
Risks do not occur in isolation (Evans et al., 2013), instead risks from different domains are likely to interact. For example, low household income is more prevalent in families who identified as Black African, Indian, and Coloured, and racial identity in turn is linked to language challenges. This implies that policy development and interventions must include these linkages into a central organizing theme.
A limitation of this study was the cross-sectional design which does not yield longitudinal data to track changes in risks and occurrences over time. Self-report inventories may involve degrees of subjectivity, misconception of constructs, and recall difficulties. While the study reflects the overall demographics of the race groups in South Africa, perhaps proportions of participants that more accurately reflect the representation of the different race groups in the broader population would increase validity. Despite these limitations, this study adds substantive insights into the uniqueness of risks in South Africa and its commonality with global trends.
Conclusions
Risk research has gained increasing traction in the past decade due to wider calls for informed and relevant programmes to address childhood developmental challenges, especially in low socioeconomic communities. This study focussed on the occurrence of risk factors within a South African community sample, with reference to its unique socioeconomic and political history. The underlying thrust is that inclusive studies are more likely to elucidate the unique occurrence and burden of risks linked to youths’ behavioural, emotional, neurocognitive, and scholastic functioning.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.