
Abstract
Aggressogenic parenting styles are associated with increased rates of callous and unemotional traits, and in turn, with antisocial behaviours. Traumatic brain injury is also associated with antisocial behaviour, but not callous and unemotional traits specifically. No study has previously investigated these three variables, aggressogenic parenting, traumatic brain injury, and callous and unemotional traits, in a single study. The study setting was Cape Town, South Africa. The sample included high school boys (N = 54), aged 13–21 years in an observational, descriptive study. We hypothesised that boys who reported that they had sustained a traumatic brain injury and who had been exposed to aggressogenic parenting would display increased levels of callous and unemotional traits, and that those with traumatic brain injury but had experienced positive parenting would display lower levels of such traits. The main measures included the Comprehensive Health Assessment Tool, the Inventory of Callous/Unemotional traits, and the Alabama Parenting Questionnaire. Results show that almost 41% (22/54) of participants reported sustaining a traumatic brain injury. Aggressogenic parenting significantly moderated callous and unemotional traits only in participants with traumatic brain injury, F(1.46) = 4.76, p = .03, while positive parenting and substance use did not. In conclusion, traumatic brain injury in the presence of aggressogenic parenting is associated with greater callous and unemotional traits in this sample of adolescent boys.
Crime rates in South Africa are high and increased from 2016/2017 to 2017/2018 (Statistics South Africa, 2018), with highest rates found in lower socio-economic status (SES) communities (Gardner et al., 2015). Many South African youths find themselves within such low-SES settings, where males aged 12–22 years especially face high exposure to crime and violence alongside poverty, relative to the general population (Bhorat et al., 2017; De Lannoy et al., 2015; Gardner et al., 2015). However, youth are not only witness to and victims of crime but are also among the leading perpetrators thereof (du Plessis et al., 2015; Statistics South Africa, 2018). A well-established predictive factor of criminal involvement in individuals is the presence of antisocial behaviours (Gardner et al., 2015). Callous and unemotional (CU) traits, characterised by a lack of empathy and low affect, in turn predict antisocial behaviour (Mann et al., 2015; Viding et al., 2012) and this tends to occur at higher rates in males than females (Larsson et al., 2008) and within lower SES settings (Piotrowska et al., 2015).
Style and methods of parenting have been found to have important and long-lasting effects on children’s behaviour that continue into adolescent and young adult years (Ward et al., 2015). Early work on types of parenting styles revealed three clusters that are still influential in parenting research today – authoritative, authoritarian, and permissive parenting styles (Baumrind, 1966, 1971). Maccoby and Martin (1983) expanded on this seminal work and conceptualised that support and control made up a framework operating on two dimensions: responsiveness and demandingness. In light of this framework, they defined four styles of parenting: authoritarian (low support, high control; discipline with demands and low child autonomy), authoritative (high support and control), permissive (high support and low control; a lack of monitoring, control, and discipline, yet it is warm and nurturing), and neglecting (low support and control). Their research indicated that any style that is not authoritative may lead to increased risk of associated negative outcomes. In particular, authoritarian and permissive styles have been found to be linked to negative psychosocial developmental outcomes and behavioural problems over time (Fernandez, 2009; Flouri & Midouhas, 2017).
Research investigating the relevance and prominence of the four styles has shown that at least in Western culture, there is a strong evidence base for the existence and pertinence of these styles (Power, 2013). Although sometimes clusters may differ between three or four parenting clusters, little to no evidence has indicated more types of parenting styles than those described by Baumrind, and Maccoby and Martin (Roman et al., 2016). Indeed, parenting research in South Africa has used these three/four styles successfully and found them relevant and useful for study in this context (Kritzas & Grobler, 2005; Latouf, 2008; Makwakwa, 2011; Roman et al., 2016).
For the purposes of this study, aggressogenic parenting was taken to include dimensions: inconsistent discipline, and corporal punishment, and monitoring and supervision from the Alabama Parenting Questionnaire (APQ; Frick, 1991), as informed by characteristics that fall under parenting styles associated with negative outcomes, namely, the high control, discipline with demands and low child autonomy under authoritarian parenting; the lack of monitoring, control, and discipline under permissive styles; and low support and control that characterise neglecting parenting styles.
There is a large pool of research establishing links between antisocial behaviour and CU traits, and aggressogenic parenting styles (Viding et al., 2012; Waller et al., 2018). As noted, aggressogenic parenting styles include harsh or coercive parenting, parenting that is low in warmth, and poor supervision (Waller et al., 2013). Harsh discipline has been reported as a strong predictor of antisocial behaviours (e.g., high levels of aggression) in children as young as 5 years old (Leibbrandt et al., 2012). Furthermore, parenting styles involving violence from parents towards children are also associated with higher levels of antisocial behaviours in children (Ward et al., 2015). While there are few national studies of parenting in South Africa, rates of corporal punishment by caregivers – a form of harsh, coercive parenting – range from 18% upwards (Ward et al., 2018). Studies on CU traits and aggressogenic parenting styles in this context are however lacking.
In addition, there is an association between traumatic brain injury (TBI) and antisocial behaviour (Andrews et al., 1998; Tomaszewski et al., 2014; Williams et al., 2018), which may be moderated by parenting style (Chavez Arana et al., 2020). Parenting style has been found to moderate functional impairments in children with TBI across cognitive and social domains, where children parented with a permissive (negative) style of parenting are significantly more likely to display these impairments over time, in comparison with those who experience more positive parenting (Wade et al., 2016). These differences in cognitive and social behavioural outcomes between children with TBI and controls become consistently more pronounced under extreme authoritarian and permissive parenting styles (Yeates et al., 2010).
However, as yet, there is a dearth of research on TBI and CU traits, despite the link of both to antisocial behaviour (Andrews et al., 1998; Tomaszewski et al., 2014; Williams et al., 2010). Developing countries like South Africa are postulated to have higher rates of TBI than developed world countries (Dewan et al., 2018), making South Africa an ideal location to explore such research.
In sum, aggressogenic parenting styles are associated with increased rates of CU traits, and both TBI and CU traits are associated with antisocial behaviour, but no previous study has investigated these three variables together.
Aim and hypotheses
The aim of this study was to investigate whether parenting styles towards youth who report having sustained a TBI moderate the presence of CU traits. Specifically, we investigated whether adolescents who report having sustained a TBI, and who have been exposed to more positive parenting styles, as measured by the APQ, would report lower rates of CU traits than those with TBI who had been exposed to aggressogenic parenting behaviours.
We hypothesised that (1) youth who report having sustained a TBI, who had been exposed to a positive parenting style, would report lower levels of CU traits; and (2) youth who report having sustained a TBI, who had been exposed to an aggressogenic parenting style, would report higher levels of CU traits.
Method
The study was cross-sectional and quantitative. The independent variables in this study were (self-reported) TBI (yes/no) and style of parenting to which participants had reportedly been exposed (positive/aggressogenic). The dependent variable was the CU trait score.
Participants
Participants were recruited through purposive sampling from two high schools in low- to middle-SES areas within Cape Town. Specific schools were selected based on their proximity to the university, and a previous research association with one of the schools. Participants were English- or Afrikaans-speaking males, aged 13–21 years.
Instruments
Alcohol, Smoking, and Substance Involvement Screening Test
The Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST) is a self-report questionnaire with eight items designed to assess levels of substance use in the 3 months preceding the test. The measure screens for a range of substances, including, but not limited to, alcohol, tobacco, and cannabis. The World Health Organization (WHO) ASSIST Working Group (2002) designed the ASSIST in 2010, with the goal of creating a standardised measure with which to assess levels of substance abuse worldwide. It has high levels of reliability and validity (a = .83, Kaiser–Meyer–Olkin [KMO] = .77; Simelane-Mnisi & Mji, 2017). Seeing as the measure was created with a global population in mind, and has been tested in an African population, it is suited to the South African context (Humeniuk et al., 2010; Simelane-Mnisi & Mji, 2017).
Alcohol Use Disorders Identification Test
The Alcohol Use Disorders Identification Test (AUDIT) is a 10-item questionnaire that was developed by the WHO to measure alcohol consumption, dependence, and associated complications (Babor et al., 1992). It is particularly aimed at health care practitioners, but it can and has been successfully self-administered or administered by non-health care professionals. The AUDIT has high internal consistency and reliability (Cronbach’s alpha = .80), and these properties have been tested and found to be retained in South African samples (Meneses-Gaya et al., 2010; Peltzer et al., 2011).
Beck Depression Inventory
The Beck Depression Inventory (BDI) is a widely utilised tool used to assess levels of depression. Both psychological and physical symptoms of depression are assessed. It is a self-report measure with 21 items using a 4-point Likert scale. Standard cutoff scores are as follows: scores between 0 and 9 indicate normal functioning, 10–19 indicate mild to moderate depression, and 20 and above indicate severe depression (Beck et al., 1996). The test has good psychometric properties, including high validity (Cronbach’s alpha = .96) and test–retest reliability scores (Cronbach’s alpha = .73–.96; Beck et al., 1996; Wang & Gorenstein, 2013). In addition, the BDI has been used successfully and widely in South Africa and was thus suited to the context (Khumalo & Plattner, 2019; Stellenberg & Abrahams, 2015).
TBI measure
Comprehensive Health Assessment Tool
The Comprehensive Health Assessment Tool (CHAT) is a standardised measure used to screen for health complications. It was originally designed with a young offender population in mind. It includes four sections: physical health, mental health, substance misuse, and neurodisability (Chitsabesan et al., 2014). We used the CHAT to distinguish between adolescents who have sustained a TBI and those who have not. An advantage of this tool is that it measures frequency and severity of each TBI (if there has been more than one). The CHAT has good psychometric properties when compared to other health assessment tools, and high reliability and validity when assessing presence of TBI (Chitsabesan et al., 2015). This measure has previously been used in South Africa (Nkoana et al., 2020).
Demographic questionnaire
This short questionnaire was used to assess the individual participants’ socioeconomic environment. Questions pertaining to the participants’ age, residential area, number of individuals residing within the household, number of rooms within the household, and the type of materials out of which the house was made were used to determine the SES of participants
Parenting measure
APQ
The APQ is a two-part self-report questionnaire whereby the participant in question is asked to rank his responses to 42 items on a 5-point Likert scale. There are two separate questionnaires for youth and their parents. For the purposes of this study, only the high school boys were asked to complete this questionnaire, due to difficulty obtaining responses from parents. The questionnaire is used to assess parenting styles in five subcategories: involvement, positive parenting, monitoring/supervision, inconsistent discipline, and corporal punishment (Frick, 1991). High factorial validity has been found between these categories (Maguin et al., 2016). Internal consistency is adequate and test–retest reliability is good (r = .84–.90; Dadds et al., 2003). The APQ is a commonly used measure, with multiple translated versions in use. This measure has been successfully used to assess parenting in South African studies (Lachman et al., 2013). For the purposes of this study, the five categories were grouped into two larger categories of positive and aggressogenic parenting for better operationalisation. Positive parenting and involvement were grouped as positive parenting, while monitoring/supervision, inconsistent discipline, and corporal punishment were grouped under aggressogenic parenting, allowing for two parenting scores.
Antisocial behaviour measure
Inventory of Callous and Unemotional Traits
The Inventory of Callous and Unemotional Traits (ICU) is made up of 24 items that measure levels of aggression and antisocial behaviour across three subsections, including callousness, unemotionality, and uncaring tendencies (Frick, 2004). Each item is rated on a 4-point Likert scale and the participants are required to rank their responses to statements as such. Some items require reverse scoring. The ICU has been found to have good psychometric properties (e.g., reliability) even in cross-cultural settings (Cronbach’s alpha = .77) and reliable in detecting antisocial tendencies in adolescents (Kimonis et al., 2014; Mooney, 2010). Although this measure has only been used in an unpublished South African study, a study investigating cross-cultural properties of the ICU found it to retain its psychometric properties in varied cultural settings, and we therefore consider it appropriate for our context and purposes (Feilhauer et al., 2012; Ockhuizen, 2014).
The total score for the ICU is 72, with the optimal cutoff score of 28 reported for youth self-report form. However, we did not apply a stringent cutoff score, but considered scores comparatively (Docherty et al., 2017).
Procedure
All boys who met the inclusion criteria were invited to participate in the study. Parental consent was sought for those who were below age 18. Informed consent (for those aged 18 or above) and assent (for those below age 18) was obtained prior to interviewing participants. All measures were administered in an interview style with each participant. Each participant was interviewed individually in an empty classroom where there was no risk of disruption or violation of confidentiality. At the end of the interview, the researchers provided each participant with a R50 food shopping voucher.
Ethical considerations
Ethical approval was obtained from the Research Ethics Committee of the Psychology Department at the University of Cape Town, and permission to test in schools from the Western Cape Department of Education.
Data analysis
We analysed the study data using the Statistical Package for the Social Sciences Version 25.
We first ran descriptive statistics for the correlations between, age, the control variables (BDI, AUDIT, ASSIST, age), the predictor variables (TBI and parenting style), and the outcome variable (CU traits). We then ran two hierarchical moderation analyses to determine whether boys with TBI (yes/no) who had been exposed to more positive/aggressogenic parenting styles (both through self-report) reported fewer/more CU traits, respectively. To allow aggressogenic and positive parenting to be on the same scale when running our analyses for better operationalisation and comparison, we represented aggressogenic and positive parenting as percentages of the total possible score. Thus, each participant’s aggressogenic score was divided by 95, which represents the total possible score for aggressogenic parenting and each positive parenting score by 130, which represents the total possible score for positive parenting. We controlled for depression, substance use, and age in these analyses.
For both moderation analyses, all control variables and age were entered as a block, followed by TBI, and then by either positive or aggressogenic parenting style, with the interaction term entered as the final block. Some studies have shown that substance use and depressive symptoms in adolescents may increase the likelihood of displaying antisocial behaviours (Hemphill et al., 2015; Park et al., 2010). In addition, age has a significant impact on antisocial behaviours in that the period of adolescence is associated with a significantly higher degree of antisocial behaviours compared to other phases in an individual’s lifespan (Eme, 2016; Henry et al., 1993). Although all our participants were adolescents, the age range was quite large (13–21), and thus it was necessary to control for age. It was, therefore, necessary to consider these potential confounding variables in the study.
Results
Sample characteristics
The sample size was N = 54 and included high school boys in Grades 8 to 12, aged 13–21 at the time of testing. About 40% of the sample (n = 22) reported having sustained a TBI at some point in their lifetime, of which 54.5% had experienced a loss of consciousness, 4.5% of those for less than 5 min, 27% between 5 and 30 min, 9% between 30 min to 1 hr, and 9% between 1 hr and 24 hr, and 4.5% for longer than twenty-four hours. In all, 77.2% experienced feeling dazed and confused after the injury. Participants resided in predominantly low-SES areas, with 63% of participants residing in high-density informal settlements.
Comparing TBI and no-TBI groups
There were no significant differences between the no-TBI and TBI groups in terms of substance use, where 66% and 91% of participants in each group reported substance use, respectively (ASSIST; χ2 = 1.571; p = .216). The results of comparisons for alcohol consumption, CU traits, depression, and parenting styles for the TBI and no-TBI groups are presented in Table 1. There were also no significant between-group differences for these variables. Depression scores for both groups were in the mild depression range of 14–19 on the BDI-II (Beck et al., 1996) and scores for the ICU for both groups were below the cutoff score of 28 (higher scores present greater likelihood of offender-like behaviour, including antisocial, aggressive, and violent behaviour; Docherty et al., 2017).
Descriptive statistics and between-groups analysis for TBI versus non-TBI groups.
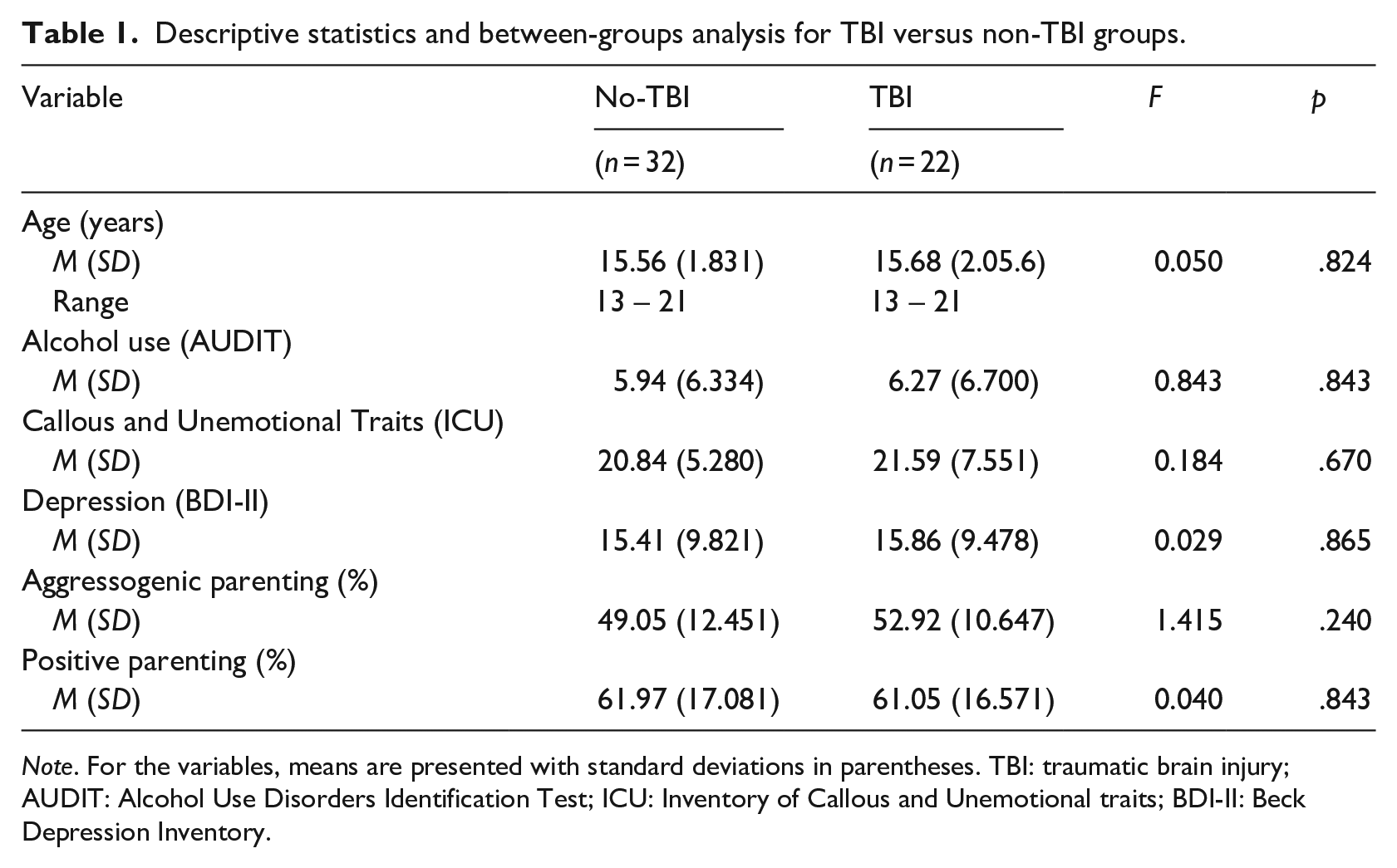
Note. For the variables, means are presented with standard deviations in parentheses. TBI: traumatic brain injury; AUDIT: Alcohol Use Disorders Identification Test; ICU: Inventory of Callous and Unemotional traits; BDI-II: Beck Depression Inventory.
Correlations
TBI was positively and weakly correlated to aggressogenic parenting (r = .16, p = .12) and negatively and weakly correlated to positive parenting (r = −.028, p = 42). Positive parenting was significantly negatively correlated with CU scores (r = −.26, p = .02). The associations between aggressogenic parenting and CU traits (r = −.02, p = .41), and TBI and CU traits (r =-.2, p = .33), were not significant. These correlations are presented in Table 2.
Bivariate correlations for the study measures for the total sample (N = 54).
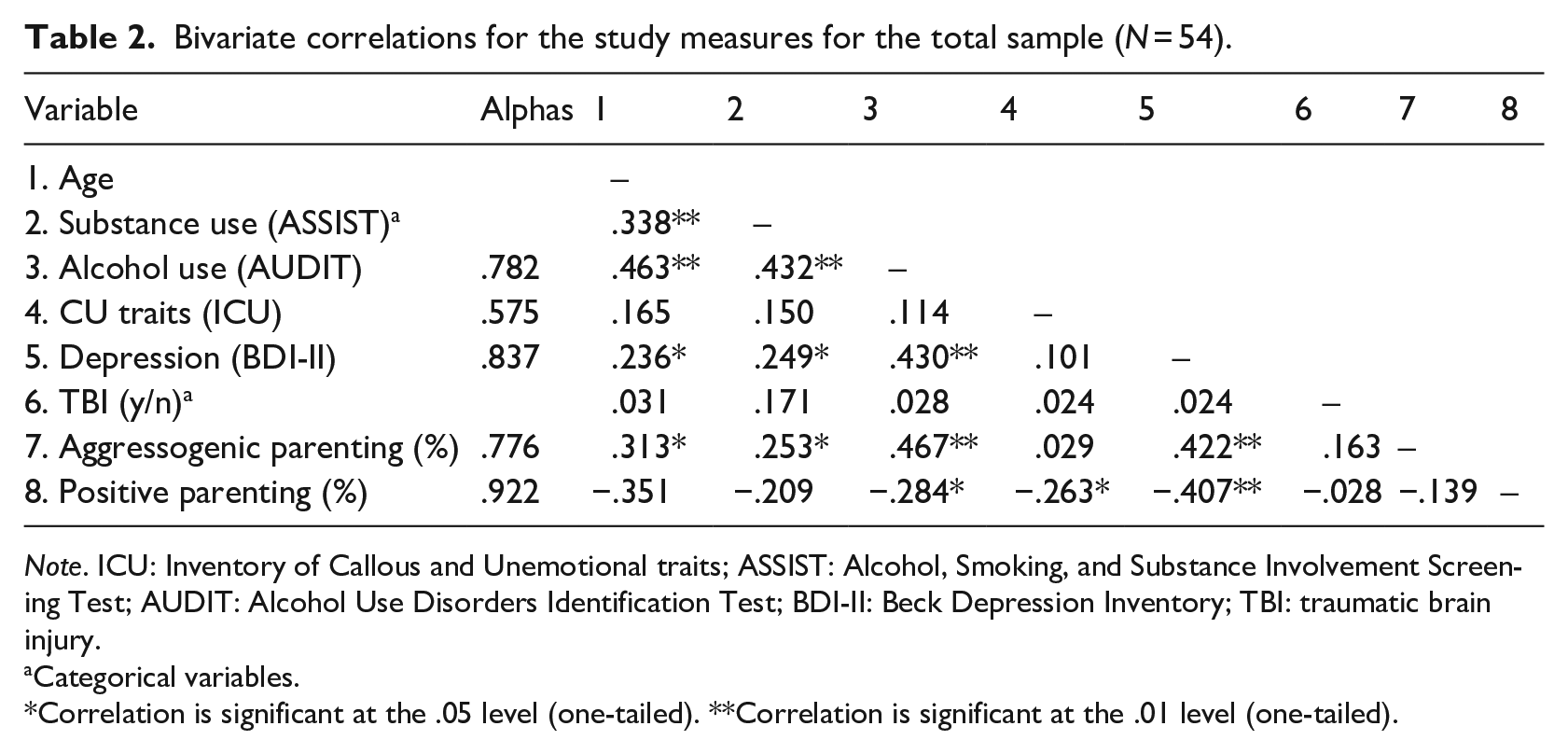
Note. ICU: Inventory of Callous and Unemotional traits; ASSIST: Alcohol, Smoking, and Substance Involvement Screening Test; AUDIT: Alcohol Use Disorders Identification Test; BDI-II: Beck Depression Inventory; TBI: traumatic brain injury.
Categorical variables.
Correlation is significant at the .05 level (one-tailed). **Correlation is significant at the .01 level (one-tailed).
Cronbach’s alphas for measures of alcohol use, depression, and positive and aggressogenic parenting ranged from .776 to .922, as shown in Table 2, which are in the generally acceptable range (Tavakol & Dennick, 2011). However, the alpha for the measure of CU traits was lower than the acceptable level. Even though these results are not consistent with psychometric properties reported in previous studies (e.g., Kimonis et al., 2014; Mooney, 2010), the ICU is the only measure specifically designed to measure CU traits. Furthermore, a recent meta-analytic review of the ICU notes that internal consistency of the measure might be undermined by the unemotional subscale specifically, rather than all three subscales (Cardinale & Marsh, 2020).
Moderation analyses
For both moderation analyses, all control variables and age were entered as a block, followed by TBI, and then by either positive or aggressogenic parenting style, with the interaction term entered as the final block.
We ran two separate hierarchical regression moderation analyses where for both analyses, depression, substance use, and age were controlled for in the first block; TBI was added in the second; positive or aggressogenic parenting in the third; and the interaction term of variables positive or aggressogenic parenting and TBI was entered in the final block, respectively. The outcome variable was CU traits for both moderation analyses (see Tables 3 and 4).
Hierarchical moderation analysis: Positive parenting and TBI as predictors and CU traits (ICU) as outcome variable (N = 54).
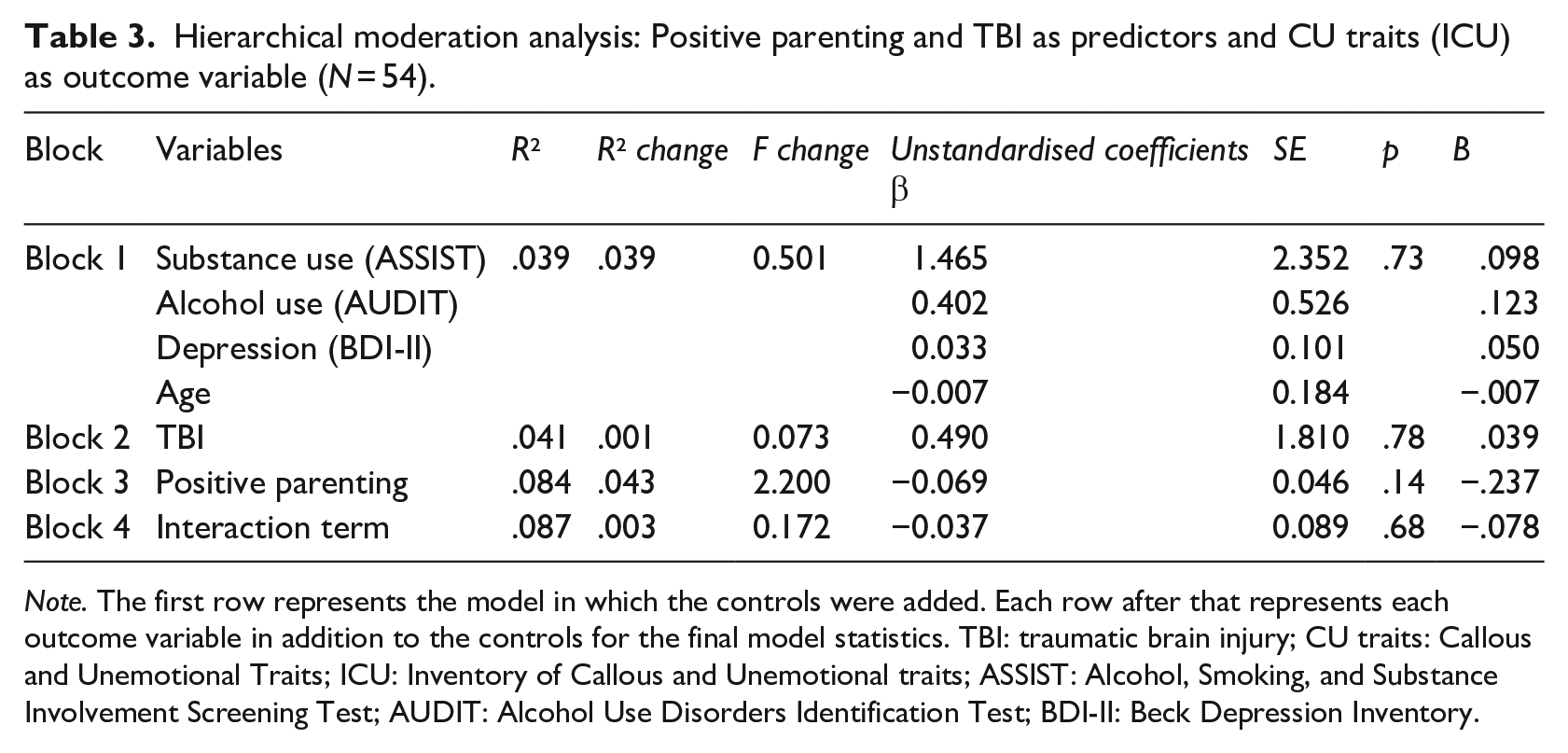
Note. The first row represents the model in which the controls were added. Each row after that represents each outcome variable in addition to the controls for the final model statistics. TBI: traumatic brain injury; CU traits: Callous and Unemotional Traits; ICU: Inventory of Callous and Unemotional traits; ASSIST: Alcohol, Smoking, and Substance Involvement Screening Test; AUDIT: Alcohol Use Disorders Identification Test; BDI-II: Beck Depression Inventory.
Hierarchical moderation analysis: Aggressogenic parenting and TBI as predictors and CU traits (ICU) as outcome variable (N = 54).
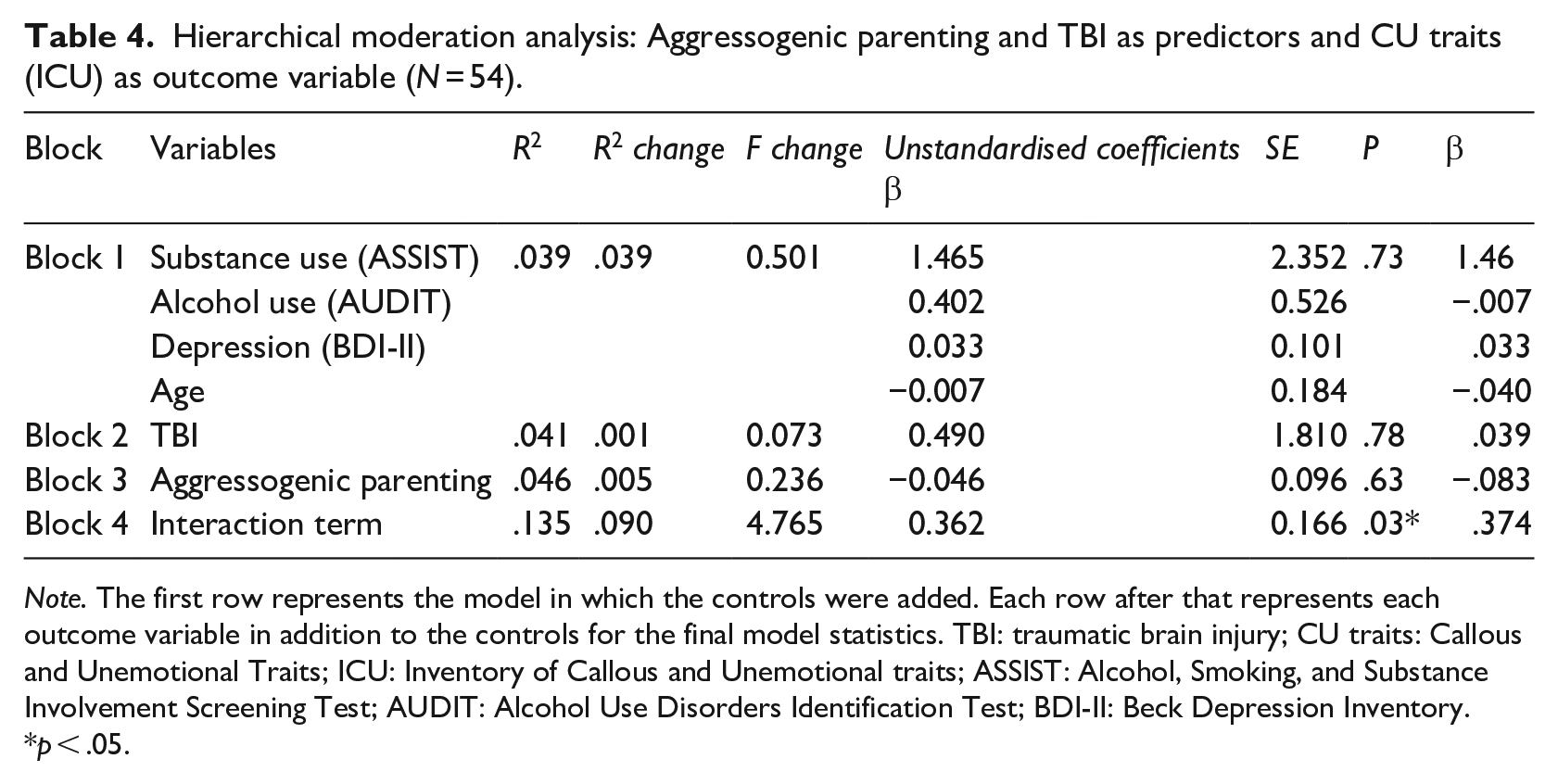
Note. The first row represents the model in which the controls were added. Each row after that represents each outcome variable in addition to the controls for the final model statistics. TBI: traumatic brain injury; CU traits: Callous and Unemotional Traits; ICU: Inventory of Callous and Unemotional traits; ASSIST: Alcohol, Smoking, and Substance Involvement Screening Test; AUDIT: Alcohol Use Disorders Identification Test; BDI-II: Beck Depression Inventory.
p < .05.
Positive parenting and TBI
Overall, the positive parenting model was not statistically significant, F(7, 46) = .62, p = .73. Furthermore, there was no moderation effect present and thus positive parenting did not moderate CU traits in children with or without TBI, all as reported by participants.
Aggressogenic parenting and TBI
Similarly, the aggressogenic parenting model was not significant overall, F(7, 46) = .1.02, p = .42, and explained 13.5% of the variance. As shown in Table 2, none of the variables significantly predicted CU scores by themselves – however, there was a moderation effect present as the interaction term significantly predicted CU scores. The interaction term explained 9% of the variance, F(1, 46) = 4.76, p = .03. Therefore, there was a moderating effect present and thus reported aggressogenic parenting moderated CU traits in children with reported TBI (see Figure 1).
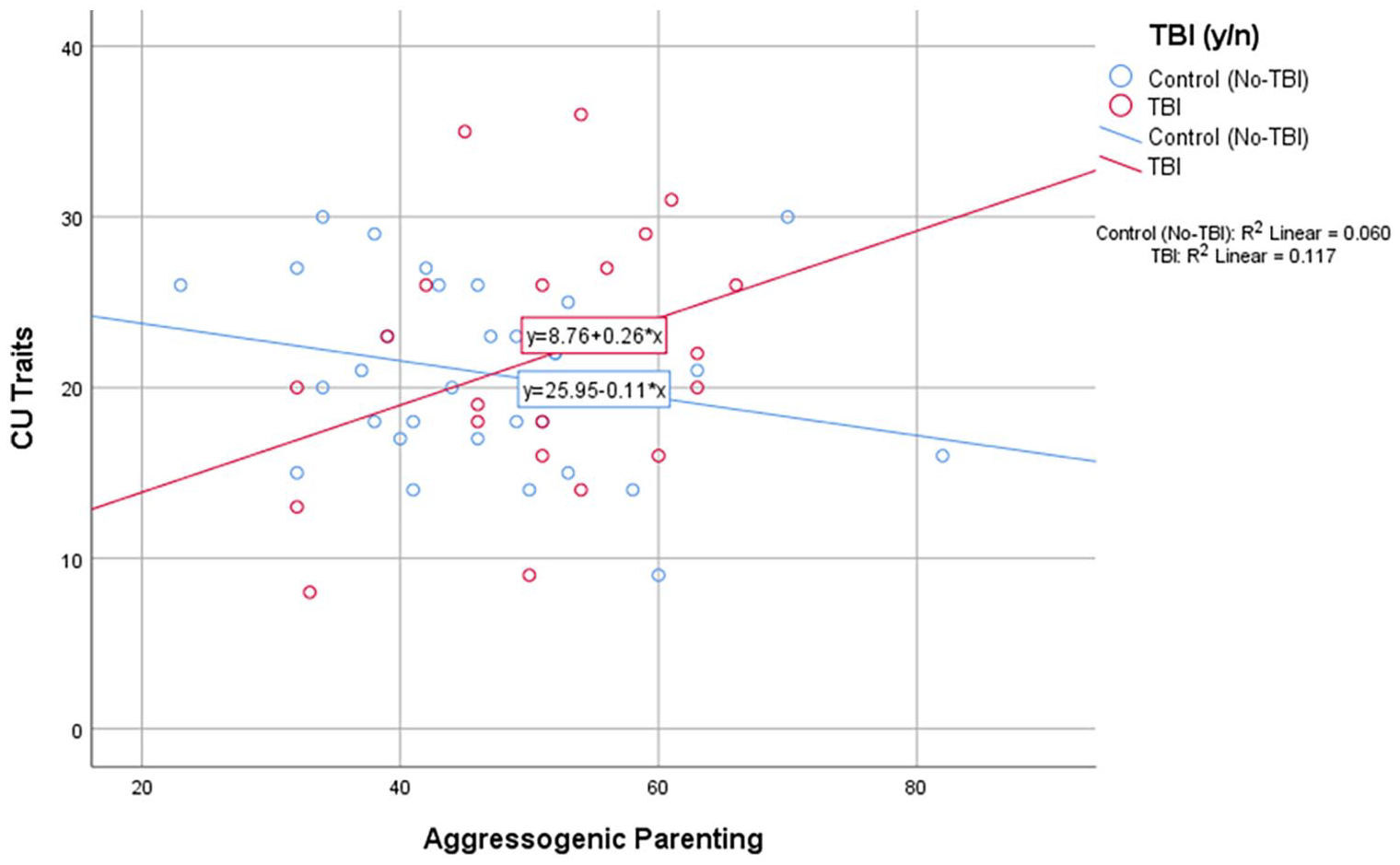
Scatter plot showing the interaction between aggressogenic parenting and CU traits for youth who had sustained TBIs and controls.
The moderation analysis indicated that only in the presence of aggressogenic parenting did participants with TBI exhibit more CU traits than those without TBI. Figure 1 is a visual attempt at understanding the interaction, with the test of moderation acting as the interaction term in the model. The analysis tells us that the difference between no TBI and TBI is significant based on the test of the interaction. From a simple slopes analysis, the trend for the TBI group is 0.26, with a 95% confidence interval of −0.01 to 0.52 (p = .119). There appears to be marginal evidence that the slope for TBI children is positive, and that for no-TBI group (−0.11), the slope is likely flat (95% confidence interval [CI] = −0.3 to 0.08, p = .176). However, each group slope is not significantly different from 0.
Discussion
Crime levels in South Africa, and especially within low-SES communities, are exceedingly high (Statistics South Africa, 2018). Youth and particularly adolescent males within these communities are among the leading victims and perpetrators of criminal activity (du Plessis et al., 2015; Statistics South Africa, 2018). The presence of antisocial behaviours is associated with an increased likelihood of criminal activity (Moffitt, 2018). Two established predisposing factors towards antisocial behaviours associated with criminal activity are (1) presence of a TBI, due to its associated neurological and subsequent behavioural pathologies (Ilie et al., 2014); and (2) harsh discipline and other techniques associated with poor parenting style (Ward et al., 2015). Considering the high levels of TBI among South African youth residing in low-SES communities, and the context of extreme crime levels in the country, it is important to establish whether certain parenting styles further predispose children with TBI to involvement in criminal activities (Naidoo, 2013; Statistics South Africa, 2018).
A worryingly high 41% of the sample reported having sustained a TBI. These figures are consistent with other research on prevalence of TBIs in South Africa and other developing world countries and reflect the high frequencies of common mechanisms of TBI in the country (Dewan et al., 2018; Naidoo, 2013; Statistics South Africa, 2018). The number of complicated mild TBIs are, however, very high relative to other samples in high-income countries (Williams et al., 2018).
There were no significant differences between the TBI and non-TBI groups regarding CU traits, nor differences in styles of parenting. There was a weak negative correlation between positive parenting and ICU scores; however, the regression analysis indicated that positive parenting did not significantly predict CU traits. The moderation analysis indicated that while positive parenting did not moderate CU traits in children with TBI, aggressogenic parenting significantly moderated ICU scores in children with TBI and explained 9% of the variance in the model.
Regarding the first finding, it is possible that cultural differences affected the measures; also, since parents may use both aggressogenic and positive parenting approaches with the same child, it is possible that the aggressogenic effects outweigh the positive effects.
The second finding, however, suggests that parenting may be an important intervention point for children with TBI. These findings are consistent with the literature reviewed, indicating that poor parenting exacerbates the negative social effects of TBI and increases levels of antisocial behaviours. This outcome is in contrast to the non-significant findings regarding the impact of good parenting on children with TBIs in terms of antisocial outcomes. This could suggest that South African children with TBIs are more susceptible to the effects of poor parenting including discipline, monitoring and supervision, and corporal punishment, typically delivered by parents, but not as susceptible to the effects of good parenting. This could potentially be due to wide networks of social support and thus less reliance on parents for positive social support than children in other settings. However, South African children with TBIs are still vulnerable to the effects of poor parenting.
Parenting support and training may prevent the development of antisocial behaviour (Cluver et al., 2018) and/or CU traits, which would both improve the life chances of the individual children, and potentially – given how widespread TBI is – even reduce the national crime rate. The implications of these tentative findings could be that we need to target parents of children with TBI, with the intention of reducing the prevalence of behaviours associated with poor parenting, as these appear to increase the risk of children with TBI engaging in antisocial behaviours. Hospitals, where TBIs are often diagnosed and reported, could be a hotspot for identifying parents of children who have sustained TBIs and encouraging them to enrol in parenting workshops specific to their needs and situation. Furthermore, parents of children who have sustained TBIs could have their parenting style assessed and be provided with support and education regarding the parenting of children who have sustained TBIs.
However, it must also be recognised that reverse causality is a possibility: those with TBI may well be more ‘difficult’ children to parent (more likely to take risks, etc.) who elicit aggressogenic parenting. Longitudinal studies are needed to investigate such effects.
We acknowledge the recognised limitations associated with self-report measures (social desirability bias and lack of insight [the latter could be a consideration where there is a history of TBI]), as well as our limited sample size and representation, which impacts on the statistical power in our analyses and the generalisability of our findings, respectively. We also acknowledge the lower than acceptable alpha found for the ICU for this study sample. We did not have access to medical records of the children and thus had to rely on their recollection of having sustained a TBI. To this end, the severity of TBI was also not objectively assessed. Furthermore, we were not able to administer the parent component of the APQ and thus only had responses of the high school participants, where both would have provided a more reliable score, and the perception of the child may therefore drive our findings.
Conclusion
This study found that children with a TBI are more susceptible to the effects of aggressogenic parenting, in terms of displaying more CU traits, but not to the effects of parental involvement and positive parenting. Further research is needed to establish the lack of effect positive parenting had on those with TBI and to match self-report measures with medical records. The effects of aggressogenic parenting may affect future criminal behaviour and thus it is crucial that interventions be put in place for children with TBIs who are exposed to aggressogenic parenting.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation (NRF) Thuthuka Grant (TTK170418227316) and the MRC Confidence in Global Mental Health: Trauma and Adverse Childhood Experiences Springboard (TrACES) grant (MC_PC_MR/R019991/1).