
Abstract
Collaborative care for mental health is a strategy that restructures the roles of health care providers, and sectors outside of health care provision, to encourage a team-based approach in dealing with mental illness. Previous research proposed a collaborative care strategy to make mental health care more accessible and culturally appropriate. This study systematically reviewed the available literature to produce a summary of collaborative care in the context of mental health care in South Africa. More specifically, the aims were to document existing efforts towards collaboration and highlight barriers and challenges associated with collaborative care in mental health care in South Africa. This review was conducted in accordance with PRISMA guidelines. South African studies published in English between 2002 and October 2021 were considered for inclusion. Twenty-five studies with heterogeneous study designs were included in this review and analysed using a thematic synthesis approach. Collaborative care models hold promise for closing the mental health treatment gap and providing culturally appropriate mental health care in South Africa. However, despite progress made, several challenges remain in the implementation of collaborative policies. Four main strategies were identified to improve the implementation of collaborative care models in South Africa. These included (1) redirecting resources and improving infrastructure, (2) formalising roles and relationships and improving leadership, (3) improving communication and supervisory structures, and (4) improving training and education. This review offers valuable recommendations for South African mental health care policy that might also be useful for other resource-constrained countries.
Keywords
Accompanying the end of Apartheid in 1994, South Africa’s health system faced major challenges resulting from inequities in the old dispensation’s allocation of resources, many of which continue to exist. One particular challenge is the lack of access to mental health care (MHC) services in previously disadvantaged and marginalised populations (Janse van Rensburg, 2009; Petersen, 2000), especially in rural areas (Jack et al., 2014; Lund et al., 2015). It is estimated that between 70% and 75% of South Africans with mental illness do not receive treatment (South African College of Applied Psychology [SACAP], 2018). Considering the South African psychologist to population ratio of about 1.4:100,000, mental health specialists alone will most likely not be able to close this treatment gap (Psychological Society of South Africa [PsySSA], 2017).
A second challenge for MHC delivery in post-apartheid South Africa is the shift away from imposed systems of Western psychology to culturally-appropriate and culturally-meaningful care for diverse populations of individuals (Bartholomew, 2016; Campbell-Hall et al., 2010). Adopting a universalistic perspective in mental health fails to explain culturally driven presentations of psychological distress (Laher, 2014) and could be a reason for the high levels of non-adherence to Western treatment regimes in South Africa (Bhagwanjee et al., 2008).
In response to these challenges, various researchers and policy-makers have proposed a collaborative care (CC) model for mental health service delivery in South Africa (Brooke-Sumner et al., 2016; Campbell-Hall et al., 2010; Jack et al., 2014; Shidhaye et al., 2015). A CC model refers to a strategy which ‘restructures the roles of health care providers and sectors outside of health care provision and introduces a team-based approach to the management of chronic conditions’ (Ngo et al., 2013, p. 2). For the purpose of this study, the different levels of collaboration were defined as (1) inter-professional collaboration, (2) community-level collaboration, (3) intersectoral collaboration, and (4) collaboration between healing paradigms.
Inter-professional collaboration
At the facility level, primary health care (PHC) workers can collaborate with specialist health care workers to integrate MHC services at a PHC level (Petersen, 2000). PHC workers can be trained and supervised by mental health specialists (psychologists or psychiatrists) to identify common mental illnesses in patients with chronic health conditions who are at risk for mental illness, manage these, and refer where appropriate (Jack et al., 2014).
Community-level collaboration
At the community level, collaboration refers to the training and involvement of community members, such as lay people, to assist in screening, the promotion of mental health, and the facilitation of self-help groups in a PHC setting (Shidhaye et al., 2015). This type of collaboration is often called task-sharing, or task-shifting, where MHC is provided by non-specialists to improve access in resource-scarce areas (Mendenhall et al., 2014), to lighten the workload of PHC workers (Ngo et al., 2013), to enable community participation and empowerment (Hanlon et al., 2014), and to promote culturally congruent care by striving to overcome class, language, and racial barriers (Petersen & Lund, 2011).
Intersectoral collaboration
At an intersectoral level, collaboration refers to ‘a relationship between the health sector and other sectors which is necessary to improve health outcomes more effectively, efficiently, or sustainably, than would be achieved by the sole action of the health sector’ (Brooke-Sumner et al., 2016, p. 1). Sectors outside of the health sector may include Departments of Education and Social Development, and non-governmental organisations (NGOs). Together, these sectors could address the distal determinants of mental illness including poor social development, poverty, and unemployment through an exchange of resources, including staff, information, grants, equipment, skills, and expertise (Skeen et al., 2010).
Collaboration between healing paradigms
Numerous researchers have advocated for syntheses between Western care providers (WPs), including psychologists and psychiatrists, and complementary and alternative care providers (CAPs) in looking after the mental health of South Africans (Gureje et al., 2017; Janse van Rensburg, 2009; Laher, 2014; van der Watt et al., 2017). CAPs include traditional healers (e.g., ‘diviners’ [amagqira], ‘herbalists’ [ixhwele], and ‘faith healers’ [umthandazeli] in the Xhosa culture) and other faith healers such as Muslim or Christian healers (Moshabela et al., 2016). Models for collaboration between care paradigms include the establishment of referral systems between WPs and CAPs, including CAPs as part of a multidisciplinary team, or CAPs visiting hospitals as consultants (F̀reeman & Motsei, 1992).
Since there seems to be more CAPs than WPs in rural areas in South Africa, such collaborative models could help to narrow the mental health treatment gap (Meissner, 2004). Simultaneously, these models can provide more culturally appropriate care where patients can experience a validation of their cultural beliefs and, in turn, a greater sense of control over their mental health difficulties (Laher, 2014). Conversely, some researchers cautioned against the inclusion of CAPs in treating mental illness. Documented concerns include CAPs’ questionable ability to effectively deal with more severe mental illness such as psychotic disorders and CAPs tendency to engage in harmful practice, which could violate human rights (Gureje et al., 2017).
Despite the strong recognition for the need for a CC model in MHC services and policies, evidence on the uptake of a CC strategy for mental health is scarce (Gureje et al., 2017; Lund et al., 2015). Although some research has shown that CC is positively received by patients, rewarding for community members to deliver, and can be sustained at a low cost, other researchers are critical of this stance (Janse van Rensburg, 2009; Thornicroft et al., 2016). Furthermore, most of the research on CC models has been conducted in high-income countries, and less evidence is available from low- and middle-income countries. South African research regarding collaborative efforts has focussed mostly on the prevention and treatment of HIV/AIDS and MHC has received little attention (van der Watt et al., 2017). Seeming failures in understanding and poor implementation of national policies advocating for more collaborative and community-based MHC have resulted in disaster. One example is the Life Esidimeni tragedy, where more than 118 patients died after being ‘wrongly’ deinstitutionalised in May/June 2016. This highlighted the urgent need to generate more evidence about this approach and improve collaboration (Mutsago et al., 2017).
The aim of this study was, therefore, to systematically review the available literature to produce a summary of CC in the context of MHC in South Africa. More specifically, the study aimed to document existing efforts towards collaboration, highlight barriers and challenges, and identify guidelines to facilitate the utilisation of CC models in the future.
Method
Review procedures
The systematic review for this study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Liberati et al., 2009). Figure 1 depicts a flow diagram as a visual representation of the results of the review process (adapted from PRISMA flowchart; Liberati et al., 2009).
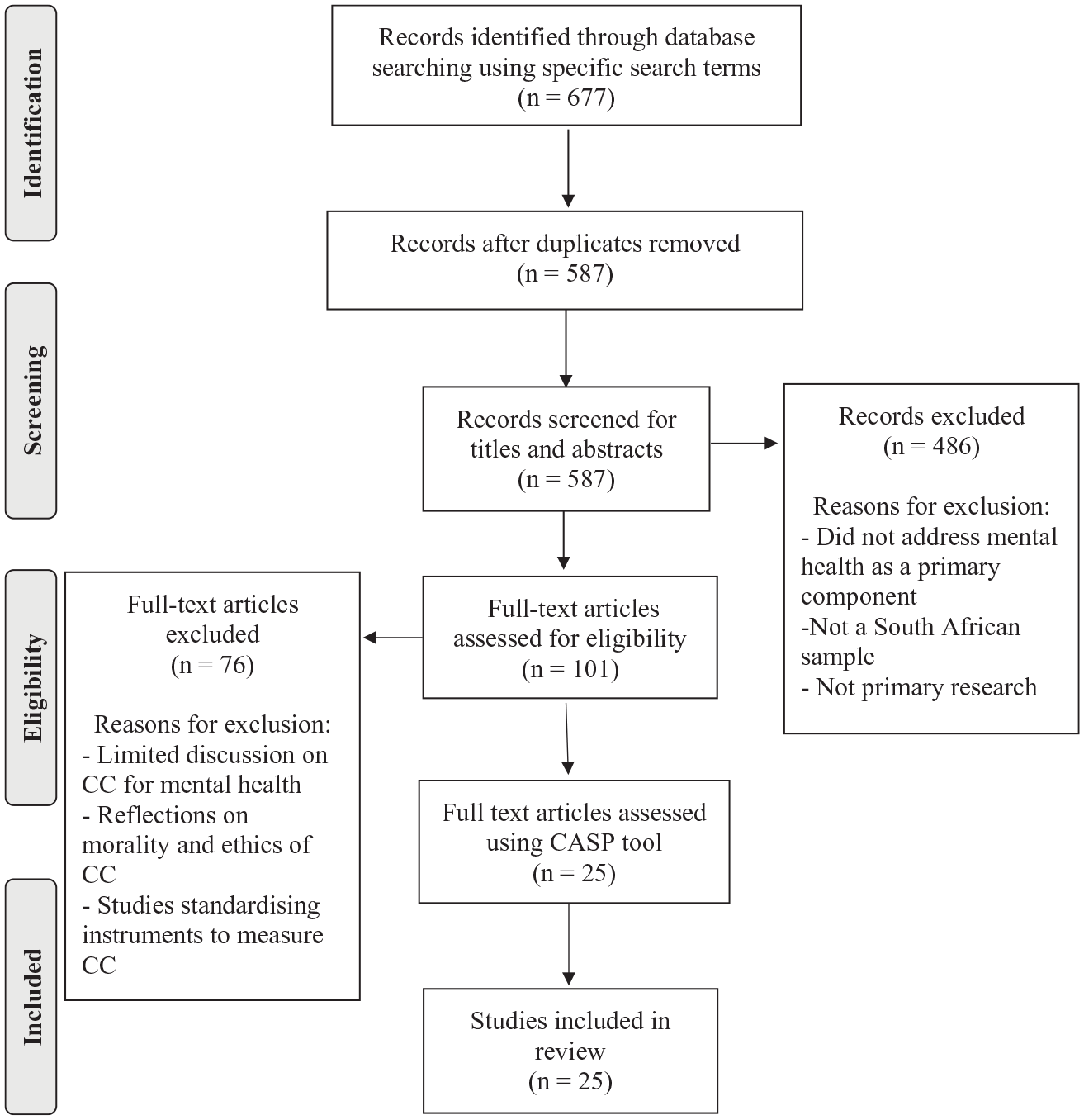
Flow diagram of review process results.
Search strategy and study selection
Sources of evidence
Research was accessed using six electronic databases namely PsycInfo, PubMed, EBSCO, Science Direct, Africa-Wide, and Sabinet. Reference mining was used to identify potentially relevant studies that were not identified through the database search (Boland et al., 2017). Articles identified for possible inclusion based on the abstract screening were mined for references and potentially relevant studies screened accordingly.
Search terms and search strategy
The following search terms were used: ‘Collaboration’, ‘care’, ‘mental health’, ‘psychology’, ‘psychiatry’, and ‘South Africa’. A Boolean phrase was used to optimise the search strategy: Collaborat* care AND (mental OR psych*) AND ‘South Africa’. Titles, abstracts, and full texts of all articles were searched for the presence of these key words in published studies with abstracts and full texts in English.
Inclusion and exclusion criteria
To be eligible for inclusion in the review, the studies must have satisfied all the following criteria: (1) studies explored collaboration at either an inter-professional, community, intersectoral, or paradigm level, (2) studies were conducted in the context of MHC in South Africa, (3) studies contained primary research, and (4) studies were published from 2002 onwards. The time criterion is based on the Mental Healthcare Act that was promulgated in 2002. This act addressed the need for more collaborative and community-based care in South Africa. All study designs, including quantitative and qualitative designs, were considered for inclusion in this review.
Studies that met one or more of the following criteria were excluded: (1) review articles, policy documents, or commentaries on policy documents, (2) only studied collaboration between the patient and professional(s) in the form of case studies or reflections, to improve the quality of MHC, (3) studied collaboration in the context of general health care in South Africa, and (4) were published in a language other than English. Due to time and resource constraints, grey literature (i.e., unpublished literature) were also excluded.
Quality assessment
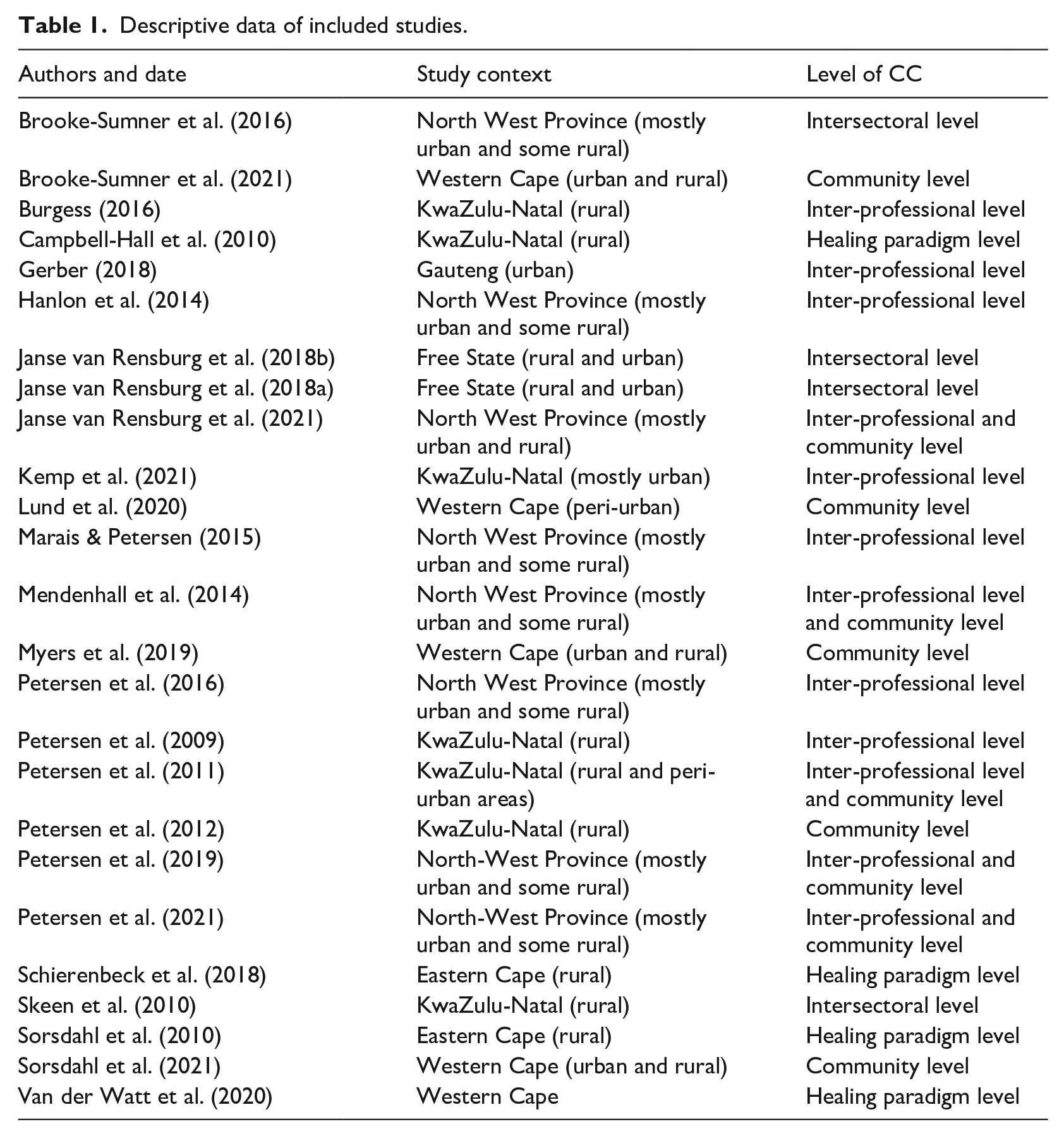
Eligible qualitative studies were assessed for risk of bias using the Critical Appraisal Skills Programme (CASP) Qualitative Checklist Tool (Critical Appraisal Skills Programme, 2017). An adapted version of the CASP Qualitative Tool was used to assess eligible quantitative studies. Available quantitative quality assessment tools, such as the Cochrane Risk of Bias Tool, were designed specifically for randomised control trials whereas the CASP Tool is user friendly and could easily be adapted to assess a variety of quantitative study designs (see Hassem & Laher, 2019). Included studies were given a score on a range of 0–10 and classified as either ‘low risk’, ‘high risk’, or ‘unclear risk’. All 25 studies achieved scores equal to or higher than 7/10. Thus, all 25 studies were assessed to be of a high quality and classified as low risk and were therefore included in the review. Table 1 provides a brief descriptive overview of the included articles.
Descriptive data of included studies.
Data extraction
Relevant data were extracted from the included studies and recorded in self-constructed data extraction tables. These tables contained a general description (including a description of study context and how the study defined CC), a methodological appraisal and a summary of results, recommendations, and limitations of each included study. The purpose of the data extraction step was to provide an overview on the study characteristics and the extracted texts were then analysed (Boland et al., 2017).
Data analysis and synthesis
Data were analysed using a thematic synthesis. Thomas and Harden (2008) proposed three steps for the thematic synthesis: (1) Line-by-line coding of the text, (2) the development of descriptive themes, and (3) creation of analytical themes (Thomas & Harden, 2008). Descriptive themes summarise and describe the original findings of the included studies while analytical themes go beyond the original content to generate additional concepts, understandings, or hypotheses. The process of analysis involved a cyclical route by constantly reviewing and refining the themes.
Results
The context of CC in South Africa
The four-level definition of CC described in the introduction of this review was applied as a framework to provide a simple overview of the current state of different levels of CC in South Africa.
Studies provided evidence of CC occurring on an inter-professional level to integrate MHC as part of the basic PHC care package in the North West Province (Dr KK district), rural northern KwaZulu-Natal (Umkhanyakude district), and in Gauteng (West Rand). While mental health services at primary level previously focussed on the emergency management of psychiatric patients and ongoing psychopharmacological care, evidence on improving access for common mental illnesses at PHC level is growing. For example, PHC nurses are now being trained to use a screening tool to assess for depression and to subsequently offer brief psychoeducation to patients. However, leading research initiatives, including PRIME (PRogramme for Improving MHC) and MhAPP (The Mental Health and Poverty Project) remain largely at the testing phase and their feasibility and effectiveness has not been adequately assessed in the South African context.
Community-level CC efforts are occurring in the North West province (Dr KK district), northern KwaZulu-Natal, and in various PHC clinics across the Western Cape. The leading research initiative in this field seems to be ‘Project MIND’ where lay counsellors are provided with ongoing training and supervision to provide brief counselling for unhealthy alcohol use and depression among patients receiving care for HIV and diabetes at PHC level. Other studies demonstrated how CHWs formed and led community-based self-help groups that focussed on providing supportive counselling and initiating income generating projects to address unemployment as a social determinant of poor mental health. In such cases, researchers found that collaborating with CHWs constitutes a promising strategy to increase access to culturally appropriate MHC and to promote social inclusion and address stigma at the community level.
Intersectoral collaborative efforts for mental health occurred in the North West Province (Dr KK district), the Free State (Mangaung Metropolitan District) and rural northern KwaZulu-Natal (district Umkhanyakude district). Researchers, however, concurred that existing levels of intersectoral collaboration are inadequate at provincial level and apparently non-existent at district level.
Despite several calls for greater collaboration between healing paradigms, there has been little progress in this regard. Studies indicated that some referrals happen from CAPs to WPs and from traditional healers to health care clinics while the establishment of a multisectoral community collaborative forum facilitated meetings between Western and traditional practitioners. Other studies noted a complete absence of collaboration between traditional or religious healers and PHC services. All these studies agreed that this absence of formal collaborative arrangements between CAPs and WPs is a particular concern.
Barriers to the implementation of CC models
Resources shortage and poor infrastructure
Studies identified a lack of human resources, especially specialist MHC workers. Due to this, available PHC workers and CHWs could not engage with specialists for guidance and supervision and felt unable to provide MHC as they already felt overburdened and barely managed to cope with the current burden of physical illness. Furthermore, studies reported a lack of finances and poor infrastructure in terms of inadequate spaces to provide psychosocial care, and an unreliable supply of psychotropic medication.
Perceptions of a lack of support and trust
Perceptions of a lack of support from other sectors or stakeholders to work collaboratively towards a mutual goal and a sense of mistrust in other stakeholders’ competencies to do their part hampered efforts towards collaboration. This occurred at an intersectoral level, among participants from the Department of Health (DOH), Department of Social Development (DOSD) and NGOs. In a similar line, there was a general sense of mistrust among PHC workers, CHWs, and mental health specialists in government stewardship to provide quality mental health services.
PHC workers had poor trust in community lay counsellors’ competency to counsel patients effectively and to follow-up on referrals while lay counsellors had poor trust and confidence in their own abilities. Lower tiered staff did not feel adequately supported by higher tiered staff and PHC workers complained about a lack of support and supervision from mental health specialists. PHC staff also reported a lack of support from general doctors, due to stigmatising attitudes, to support provision of MHC at primary level and indicated that general doctors were often absent at meetings scheduled to address collaboration.
Some traditional healers were reluctant to collaborate with WPs as they feared that their methods and indigenous knowledge would be exploited. CAPs tended to view WPs as harbouring feelings of mistrust towards them, not respecting their profession, believing that their practices are harmful or ineffective, and that WPs were therefore reluctant to collaborate with CAPs.
Poor information and referral systems
Overall, formal agreements for partnerships and collaboration were lacking and referrals between services and professionals occurred in an informal fashion. As a result, onward referrals occurred more often than back-referrals. This lack of established referral pathways between different systems and levels of care negatively affected already overburdened hospitals and specialist care settings. In turn, PHC nurses, CHWs, lay counsellors, and traditional healers complained about not getting feedback from hospitals or clinics to assist them in the management of patients in PHC settings. Referrals and communication between health professionals were further complicated by the absence of a unified mental health information system.
Inadequate education and training
Poor understanding and awareness of existing mental health policies, sporadic training for PHC workers in how to care for mental health, and a general lack of knowledge regarding mental illness were barriers to implementing CC models at all levels. Studies demonstrated that policy information was poorly communicated from national down to provincial and district levels. Inadequate training further left PHC nurses and lay counsellors feeling incompetent to care for the mentally ill. Poor knowledge of mental illness among traditional healers did, in fact, result in healers failing to detect common mental disorders in patients and to accordingly refer them to relevant biomedical services to obtain necessary psychiatric medication.
Low prioritisation and stigmatisation of mental illness
Health workers’ stigmatising attitudes towards mental health contributed to non-participation in collaborative efforts and deferral of responsibilities when dealing with the mentally ill. For example, some NGO workers refused to see mental health patients based on stigmatised beliefs that they were ‘insane’ and aggressive. In addition to stigma, viewing mental health separately from general health, added to the low priority status of mental health and negatively impacted attitudes among health workers towards collaboration. For example, general doctors displayed a lack of respect for the mental health discipline and HIV, tuberculosis (TB), and physical disability were considered more acute than mental disability. Subsequently, nurses, medical doctors and CHWs expressed a reluctance towards collaboration at primary care level and voiced their preference to keep MHC separate from PHC.
Power dynamics
NGO members, nurses, CHWs, and traditional healers felt like they had limited power in comparison to psychiatric services and medical doctors to shape MHC. This hierarchical structure of MHC, and lower tiered members feeling frustrated with and disrespected by members working in higher levels of care, impeded collaborative efforts. Moreover, limited resources and a focus on personal objectives resulted in different sectors competing for recourses and a preference to work in silos rather than collaborating.
Problems delineating roles
An unsystematic approach to intersectoral collaboration resulted in a difficulty to delineate the roles and responsibilities of different sectors in the provision of MHC. Stakeholders at different levels of health care expressed varying understandings of CC and complained of a lack of clear strategy that outlines their role in terms of collaborating with other stakeholders.
Proposed strategies to improve the implementation of CC models
Studies proposed different strategies to address the aforementioned barriers and to improve the implementation of CC models. Figure 2 summarises the four main strategies identified across the studies.
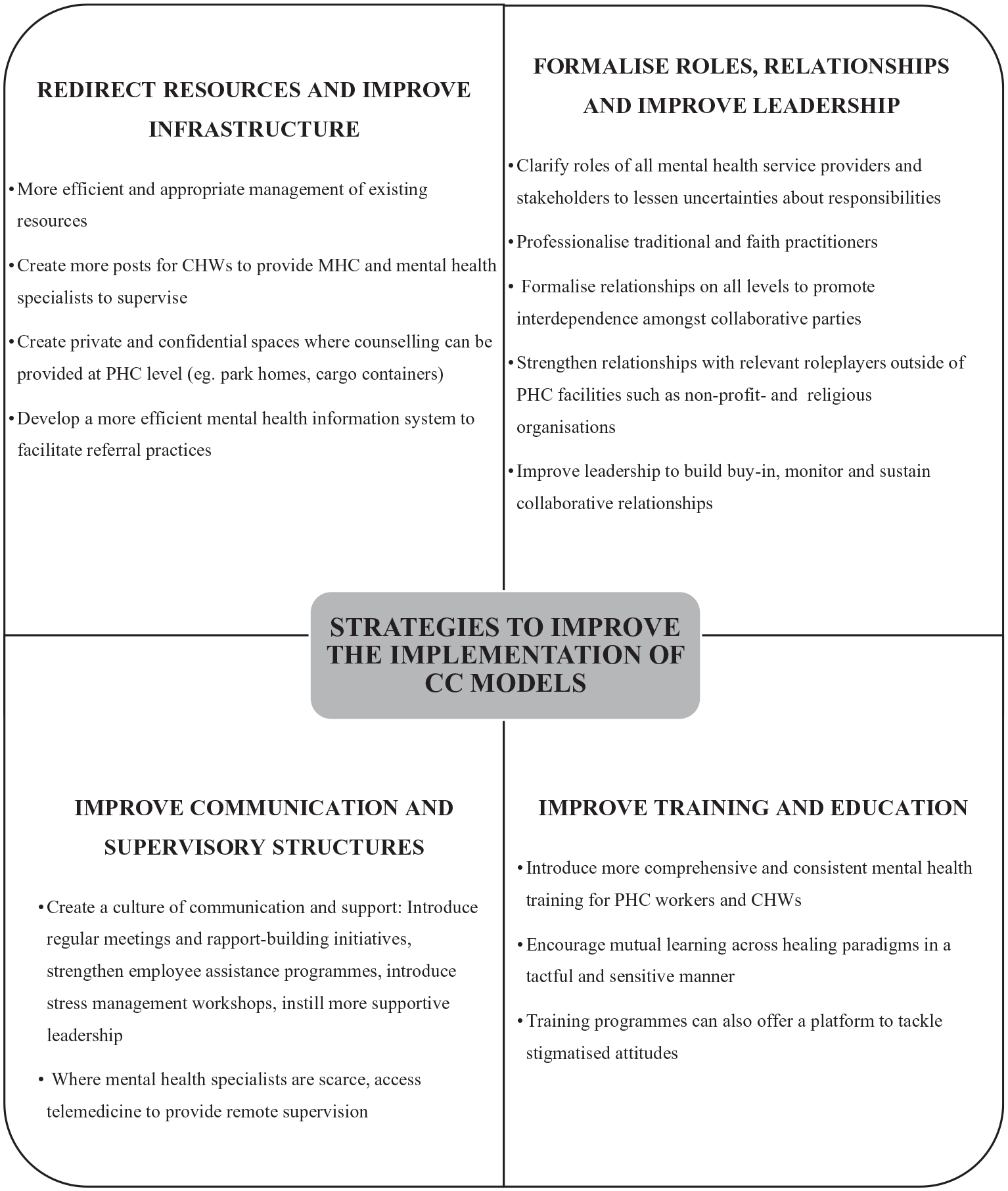
Strategies to improve the implementation of CC models.
Discussion
CC for mental health seems to be a relatively novel term and a topic that has more recently moved into the spotlight, as indicated by most studies being published between 2018 and 2021. Specifically, collaboration at inter-professional and community levels have received substantially more attention compared with collaboration at other levels. Several research protocols discuss existing collaborative efforts to integrate MHC at PHC level – showing that this research field is growing rapidly both locally and internationally (e.g., Myers et al., 2018). Although this review instils some hope regarding the potential effectiveness of CC models at a PHC level in South Africa, the existing evidence on its feasibility is inconclusive.
Despite the urgent need to generate research on intersectoral collaboration brought on by the Life Esidimeni tragedy, South African evidence on intersectoral collaboration appears to be lacking. The current stance of CC in South Africa can, therefore, be criticised for relying mostly on existing PHC resources and community participation to upscale MHC and not adequately addressing the socio-economic drivers of poor mental health. This raises concerns about the sustainability and contextual appropriateness of CC in South Africa.
Included studies were preoccupied with the barriers to implement CC models and, as such, failed to adequately investigate the actual process of collaborating. The literature reviewed in this study further lacked a clear agreed-upon definition and critical stance of the concept of CC. Thus, there is a need for a more in-depth exploration of how South African stakeholders can form interdependent partnerships and take collective ownership of goals.
South Africa can learn from existing international CC models for MHC. Leading and recent evidence from other lower-middle-income countries describing successful CC at a community level comes from India (Sangath, n.d.) while Nigeria and Ghana seem to be at the forefront regarding collaboration between healing paradigms (Gureje et al., 2020). Strategies identified to improve sustainable and effective multi-level CC models in high-income countries, including the United States and Australia, align strongly with local strategies highlighted in this review (Coates et al., 2021; Rosenberg, 2017). However, peer reviewed evidence on the real-world application of such strategies, especially for intersectoral collaboration, is lacking even in high-income countries. It might be useful to investigate whether a Norwegian evidence-based strategy to improve leadership in a health care setting (Skar et al., 2021) and a mental health stigma-reducing intervention from Nepal (Kohrt et al., 2020) could be applied to the South African context to improve organisational readiness for CC models. In addition, future research could explore whether established CC models focussed on the prevention and treatment of HIV/AIDS and TB can be transferred to CC for MHC.
This review has limitations. Given that the concept of CC is still poorly defined in the South African literature, including search words such as ‘integrative care’, ‘CHW delivered psychological interventions’, and ‘task-shifting’ would have widened the literature search and could have possibly provided access to more relevant studies.
Conclusion
This systematic review provided a mapping of available research on CC for mental health in South Africa, described the current status of this research field, and offers a metacommentary that can inform policy. From this review, it is evident that CC models hold promise for closing the mental health treatment gap and providing culturally appropriate MHC. However, despite the progress made, several challenges remain to implement collaborative strategies. The risk is that the failed implementation of CC initiatives could contribute to the revolving-door phenomena or a second Life Esidimeni tragedy. Importantly, this review emphasised the use of pre-intervention research to assess whether requirements for CC are present before CC models can be implemented in a specific context. Based on the review, four core areas were identified to facilitate CC in South Africa. Not only are these recommendations useful for the South African MHC policy, but they might also be useful for other resource-constrained countries.
Footnotes
Acknowledgements
I would like to thank my supervisor, Prof. Sumaya Laher, for her consistent support and guidance throughout this research project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.