
Abstract
After World War II, infant mortality rates started dropping steeply. We show how this was accomplished in socialist countries in East-Central Europe. Focusing on the two postwar decades, we explore comparatively how medical experts in Poland, Hungary, Czechoslovakia, and East Germany saved fragile newborns. Based on an analysis of medical journals, we argue that the Soviet Union and its medical practices had only a marginal influence; the four countries followed the recommendations of the World Health Organization instead, despite not being members. Importantly, we analyze the expert clashes over definitions of livebirth, which impact infant mortality statistics. We analyze the divergent practices and negotiations between countries: since the infant mortality rate came to represent the level of socioeconomic advancement, its political significance was paramount. Analyzing the struggle to reduce infant mortality thus helps us understand how socialist countries positioned themselves within the transnational framework while being members of the “socialist bloc.”
On Health Day 1965, the East German health minister gave a speech summarizing the progress achieved in his field. He underscored the “unity of socialism and humanism” as the driving force behind breakthroughs, and he proclaimed that medical professionals could “proudly look back on the good and beautiful successes of their work.” Among the accomplishments, he highlighted the infant mortality rate, which had “declined to 2.42 percent.” 1 His speech came in the wake of a series of international symposia where experts from the Eastern bloc gathered to compare their views on how to count infant mortality and exchange experiences on how to combat it.
Infant mortality rate (IMR) is an important indicator of socioeconomic advancement for two main reasons. First, it provides information about a child’s chances of surviving the first days and months after birth. Historical demographers showed that a vast decrease in infant and child mortality rates occurred across Europe around the end of the nineteenth century and continued throughout the twentieth century. 2 Second, shortly after the end of World War II, IMR became “regarded as a relatively more sensitive measure of health conditions than is the crude death rate.” 3 As such, the measure became a politically sensitive topic that could serve as a point of pride and sign of achievement if the numbers were low and kept dropping. In 1946, more than 100 out of every 1,000 babies died within the first year of their lives in East-Central Europe; two decades later it was only 25–40, depending on the country. 4 Infant mortality rates plummeted by two-thirds in Poland and Hungary and by three-quarters in Czechoslovakia and East Germany over the course of the two postwar decades.
How was the postwar decrease in infant mortality in East-Central European socialist countries accomplished? What role did scientists and experts play and how did their clashes and collaborations affect the decrease in infant mortality? We comparatively explore Poland, Hungary, Czechoslovakia, and East Germany during the critical period between 1945 and 1965, analyzing health services as these were understood and provided by medical doctors, specifically gynecologists, obstetricians, and pediatricians, together with midwives and obstetrical nurses. We focus on the perinatal period, that is, the time immediately preceding and following delivery, thus excluding the later weeks and months of the child’s life. 5 Our reason is twofold. First, experts concentrated the most effort on this perinatal period since improved care at that time increased the chances of saving vulnerable children, namely those born prematurely, which resulted in lowering infant mortality. Also, many measures were newly implemented between 1945 and 1965, especially in the 1950s. Second, we analyze the definitions crucial for measuring IMR, especially what it meant to be liveborn and stillborn, and how these terms were defined on the national levels of our four countries and contested internationally. In both aspects – measures implemented (saving newborns) and crucial definitions (defining livebirth) – we identified a decisive influence of the World Health Organization (WHO) and its guidelines and pronouncements. That influence is all the more interesting as it shaped the expert approaches in our region at a time when the Cold War Eastern countries had suspended their membership in the WHO.
In the aftermath of the war, state efforts concentrated on expanding and universalizing healthcare for women and children as part of the pronatalist policies aiming to compensate war losses and of the policy of expanding healthcare. 6 While infant mortality and the struggle against it remained an important issue for the societies and governments of East-Central Europe in the postwar period, it has so far attracted little scholarly attention among historians. 7 In Poland, historical demography has widely addressed infant mortality, but only until the outbreak of World War II. 8 Sylwia Kuźma-Markowska showed that the postwar medicalization of pregnancy and the fight against rural midwives in mid-1950s Poland had to do with the state’s concern with high IMRs. 9 Historical demographers in Hungary analyzed the topic in the longue durée of the eighteenth to the twentieth century, ending with World War I. 10 Éva Orosz provided a general overview of infant mortality in the context of public health during socialism. 11 Czech historians linked the decline in infant mortality to improvements in prenatal care and the introduction of antibiotics, without reflecting the high impact of how livebirth was defined and noting its changes. 12 Demographers more attuned to definitions pointed out that even after adopting a stricter approach in 1965 and recalculating the previous mortality rates, Czechoslovakia still performed better than some Western countries such as France. 13 In East Germany, as Donna Harsch has argued, infant mortality ranked as a major concern of the healthcare system. 14 Legislation and an ample set of measures proved successful in the rapid reduction of infant deaths, outdoing even West Germany. 15
Researchers have argued that health outcomes, including or even exemplified by infant mortality, have been determined by overarching political systems, such as capitalism vs. socialism, or social welfare regimes, such as social or liberal democratic. 16 There seems to be an agreement that the economic conditions provided by “left and egalitarian political traditions on population health are the most salutary, consistent, and substantial.” 17 Simultaneously, others have argued for the crucial role of cultural factors, defined as “the care shown towards infants and children at the family and society level; breastfeeding and infant feeding practices, the use of health services, etc. 18
A socioeconomic emphasis motivated the WHO’s efforts: in the preamble to its Constitution, diseases were presented as triggered and perpetuated socially and economically, and thus the appropriate response included addressing the socioeconomic settings. Yet, especially during the first decades of the WHO’s existence, clashes occurred with the proponents of technocratic approaches who aimed at controlling disease without addressing the broader social contexts. 19 Recent scholarship, aiming to address the forgotten contributions of East-Central European countries to global health since 1919, has pointed to them being particularly vocal in stressing social approaches to health issues, an attitude reinforced in the postwar era by an anticolonial stance; in this scholarship, our countries appear as a rather unified block. 20 Dóra Vargha showed how tensions between the United States and socialist countries were especially pronounced before the Soviet Union left the WHO and our countries followed suit in 1950. At the time, Eastern European states were dissatisfied with receiving mostly expertise when they urgently required material aid, such as access to antibiotics. Instead, as Czechoslovakia complained, they were given “duplicate technical assistance from the WHO and the International Children’s Emergency Fund of the UN for maternal and child health” that they did not need. 21
At the time discussed here, counting infant mortality was becoming standardized. For a certain process to become standardized, a level of uniformity is constructed “across time and space, through the generation of agreed-upon rules.” 22 The closer we get to life-or-death-issues, the more these rules tend to reflect the existing norms and values. Standardization is an offspring of the Foucauldian processes of discipline and normalization that define modern forms of governance. While words such as “standard” and “uniformity” might suggest one-size-fits-all models imposed and enforced without distinction, we understand the processes in line with Stefan Timmermans and Steven Epstein, who “emphasize the local and the contingent and treat ‘universals’ as a complex construct” and caution against “a tendency [. . .] to emphasize the link between standardization and the homogenization or flattening of social life in modernity.” 23 In this paper, we highlight the layered processes involved in standardizing the care for newborns and defining livebirth.
At least since the interwar period, the rise of medical statistics has contributed to more precise forms of measuring and counting infant mortality; some efforts to standardize medical and statistical practices nonetheless resulted in only uneven implementation. Consequentially, experts complained about the lack of comparability of infant mortality rates: statistical ways of counting differed, and the registration and definition of live birth varied from one country to another. 24 While the definition of infant mortality appears fairly straightforward – indicating a ratio of children dying before reaching their first birthday – how it is counted is another matter completely. In this paper, we detail how crucial it is to define what birth is, specifically what livebirth is – because only who was first alive can later die. As a result, only a child who was counted as liveborn and then died enters the infant mortality statistics. The definition is a “social construction” that has raised discussions reflecting a diversity of scientific practices, religions, and political cultures. 25 Durbach noted that in England and Wales during the interwar period, “the definition of life is under permanent negotiation not only because of medical advances but also because the need to distinguish between life and death emerges out of particular cultural contexts.” 26
After World War II, the newly created WHO aimed to spread unified medical practices more consciously, which included standardization of statistical medical practices and the definition of live birth. The WHO’s hopes for achieving worldwide implementation of their statistical standards were hindered in practice by Cold War dynamics; as East–West tensions escalated, some socialist states perceived the WHO as an ideological menace and were reluctant to apply some of its guidelines. 27
This negotiation continued in the second half of the twentieth century and up to the present day. As Walter Krämer and Klaus Leciejewski have recently argued, state socialist countries diverged in how they counted infant mortality. 28 Nadezhda Aleshina and Gerry Redmond documented definition divergences between East-Central Europe and the successor states of the former Soviet Union; other studies showed similar major differences within the European Union. 29 Charles Woods et al. even proved definition disparities between hospitals in the same U.S. state. 30 All these case studies show that the definitions influence the outcomes; indeed, as Godelieve Masuy-Stroobant put it, the lower that infant mortality is, the more important the definition of livebirth becomes, since once late infant mortality is reduced, most infant deaths tend to occur in the very early hours or days. 31 The statistical reporting of infant mortality is equally important. Socialist countries strove for more accurate and reliable statistics over time. 32 However, after the counting methods improved in the Soviet Union in the mid-1960s, statistics reported an increase in the IMR and, as Jessica Lovett argued, the authorities decided to censor the statistics. 33
We based our analysis on medical and demographic expertise published in professional journals, books, and conference proceedings. For Poland, we relied on Pediatria Polska (Polish Pediatrics), Zdrowie Publiczne (Public Health), Studia Demograficzne (Demographic Studies), book publications, and published regulations. For Czechoslovakia, we analyzed articles published in Pediatrické listy (Pediatric Letters), renamed Československá pediatrie (Czechoslovak Pediatrics) in 1955, Československé zdravotnictví (Czechoslovak Health Care), Československá gynekologie (Czechoslovak Gynecology), and Demografie (Demography). For East Germany, we identified Zentralblatt für Gynäkologie (Central Gazette for Gynecology), Das deutsche Gesundheitswesen (The German Healthcare System), and Zeitschrift für ärztliche Fortbildung (Journal of Continuing Medical Education). The Hungarian analysis is based on articles published in Magyar Nőorvosok Lapja (Hungarian Journal of Gynecology), Gyermekgyógyászat (Pediatrics), Orvosi Hetilap (Medical Journal), Egészségügyi Dolgozó (Health Worker), Népegészségügy (Public Health), and Demográfia (Demography). Somewhat surprisingly, demographers intervened rather little in debates over the crucial category for infant mortality: livebirth. This relative absence of demographers makes sense if we consider their “jurisdiction”: while demographers focused on how to construct mortality statistics, it was medical doctors who were present at childbirth and who were responsible for saving the vulnerable newborns while pronouncing in each individual case who was alive and who had died. Thus, in these debates over the definition of livebirth, medical doctors spoke more often and with more prominence. The transnational perspective is captured mainly through WHO deliberations and recommendations, as published in proceedings from expert group meetings and health assemblies. Importantly, we pay attention to conferences within the socialist bloc to understand knowledge flows and mutual influences.
In order to reconstruct the events that resulted in decreasing rates of infant mortality, we employed methods of documentary analysis that encourage researchers to analyze both the content and the flow of documents. In other words, we approached our documents as “topics,” trying to understand “how documents function in, and impact on, schemes of social interaction and social organization.” 34
We show that the measures taken were in line with WHO recommendations despite the fact that our countries were not active WHO members between 1949 and 1957. We discuss what differed among our countries and what differed from the WHO in the definition of livebirth. This point cannot be stressed enough: defining and counting have immense consequences because there is not always a clear line between being born dead or alive. Some babies, especially those born prematurely, might not be breathing or showing other signs that doctors consider proof of life. Yet some of them survive, while others die very soon after birth. How this liminal life-or-death moment is classified makes a difference. We analyze international debates about how livebirth should be counted, as the countries’ representatives recognized that this definition affected each country’s IMRs: stillborn babies did not figure into infant mortality; only a baby who was alive and then died was included in the mortality count. As a result, how livebirth was defined directly impacted the statistics and thus had potential to make a country look good or bad in international comparisons. We trace the transnational knowledge-flow to account for Soviet and WHO influences on the livebirth definition in East-Central Europe. We show the rather limited grip that Soviets had on definitional practice in their “satellites” and argue that in these countries a WHO-oriented outlook prevailed even during the 1950s. Importantly, we analyze the disputes that arose among East-Central European countries about how to define livebirth and how to then properly count infant mortality.
Measures recommended and taken to decrease infant mortality
With infant mortality rife in postwar Europe and beyond, the WHO raised the issue as one of the most pressing concerns at its First World Health Assembly in July 1948. An expert from Hungary connected infant mortality with the economic system of a country and its geopolitical standing, stating: Hungary in past years was known as the land of plenty; in spite of this, it was the sad privilege of Hungary to lead in the field of infant mortality and tuberculosis mortality in international statistics. In 1938 the infant mortality rate in Hungary was 13.4 percent, the tuberculosis mortality 14 per 10,000. This was due, in part, to the semi-colonial position of the country, and in part to the feudal system within the country itself.
35
This expert linked the IMR explicitly with the sociopolitical system of a country; it was precisely the sociopolitical systems adopted in East-Central Europe after the war that necessitated the withdrawal of its countries from the WHO by 1950. While Poland, Hungary, and Czechoslovakia had been among the founding members of the WHO, the Soviet Union’s departure from the WHO prompted its satellites to follow. Once the USSR announced it would rejoin in 1955, the satellite countries returned to their active membership. 36 This means that during the critical period in the 1950s when the rates of infant mortality dropped the fastest, our countries were not active WHO members. In the following section, we first present the measures recommended by the WHO and then discuss how the countries aligned with and differed from these guidelines.
Since much of infant mortality, especially shortly after birth, happened as a result of premature birth, experts focused on proper care for newborns, particularly those born preterm. The WHO concentrated mostly on the organization of delivery services and the training of professional personnel, both doctors and nurses. The WHO also highlighted the importance of prenatal care and good obstetrics. Once a child was born, it was vital to avoid mistakes in feeding; any shortage of maternal milk was to be solved through establishing milk banks.
A specialized WHO “Expert Group on Prematurity” gathered for the first time in 1950 and recommended “a well-organized delivery service, hospital or home.”
37
Importantly, the expert group did not push for the institutionalization of birth at any cost, recognizing that home birth is safe as long as the personnel are well-trained, including a public nurse to assess the suitability of the home and assist in a parent-teaching program, and transportation is available should the newborn require hospitalization. The experts put a premium on personnel training, underscoring collaboration: In order to promote team spirit, it is suggested that courses be organized for the joint participation of both medical and nursing personnel for at least some of the period. It is further suggested that there is a great advantage if a team of a doctor and one or more nurses working in the same centre takes the course together.
38
The Expert Committee on Maternity Care, which also met in 1950, also highlighted the importance of expenditures on personnel over anything else.
Even during the decade of suspended membership of our countries, personnel training occurred through UNICEF “with the technical approval of WHO.” For example, in 1951, the Institute of Mother and Child in Warsaw benefited from the “train[ing of] large numbers of special maternal and child health personnel, who later took up work in the general program of child care” in addition to providing supplies. 39 In Czechoslovakia, “WHO continued to advise on UNICEF supply programs with the assistance of the liaison officer attached to the European headquarters of UNICEF” who visited the country at the end of 1950. The “Progress Report on Medical Supply Assistance in Europe” from 1950 details spending over four million dollars on medical supplies for maternal and child health, the type of which “depended upon the stage of development of the public health services of the country.” Thus, Poland was provided with “transportation for physicians, nurses, and midwives,” making it possible for them to travel in rural areas. In Czechoslovakia, which – as the UNICEF experts noted – had a significantly lower infant mortality rate, “UNICEF is supplying incubators and other equipment to increase the network of centers for the care of the premature infant,” building on the country’s longstanding expertise at the “Prague center” (likely the Institute for the Care of the Mother and Child). 40 For 1951, the Progress Report included equipment for dried milk factories and a baby food processing plant in Czechoslovakia, and delivery of incubators in Poland. 41 A further visit was planned for 1952, although the government had not requested any of these services. 42
In countries with active membership, the WHO continued to train personnel, develop local facilities into which a vulnerable newborn could be transported in a portable incubator, and conduct research into the effect of social and economic conditions on stillbirths and prematurity.
43
By the mid-1950s, the WHO observed that the “steep fall in infant mortality in Europe has brought forward problems that were formerly of less relative importance” and the expert focus broadened to, for example, preventing childhood accidents.
44
The struggle was not over, as WHO experts acknowledged in 1958 when they looked back at the first decade of the WHO’s existence: The reduction in infant deaths was not evenly spread over the entire first year of life, but was greater in the latter part of the year and showed very little or no decrease in the first weeks. In not a few countries almost as many children were dying in the first week as in the whole of the remainder of the first year.
45
Indeed, similar patterns of infant mortality were recorded in East-Central European countries.
Measures taken by East-Central European countries
The measures implemented by our countries were similar to WHO guidelines. However, a significant difference lay in the emphasis on institutional birth. While the WHO was open to both home and institutionalized birth, most countries in our region moved childbirth to institutions. As a result, most Czechoslovak women gave birth in hospitals, as did their Polish and Hungarian counterparts who lived in cities; rural dwellers in these two countries frequented birthing homes run by midwives. East Germany, on the other hand, more closely embodied WHO guidelines as institutionalized birth was neither advised nor performed en masse there during the two postwar decades. Another difference was in the expert recommendation of breastfeeding. While the WHO did not issue any guidelines at the time, most of our countries’ physicians endorsed breastfeeding as the best nutrition. Czechoslovakia was an outlier, as doctors there approved of milk substitutes for premature babies until the 1960s, when they also switched to fully supporting lactation.
While late infant mortality improved rather quickly in all countries except for Poland (see Table 1), many children still died shortly after birth. What measures did experts implement?
Infant mortality by country and age groups (per mille) in 1953 and 1963.
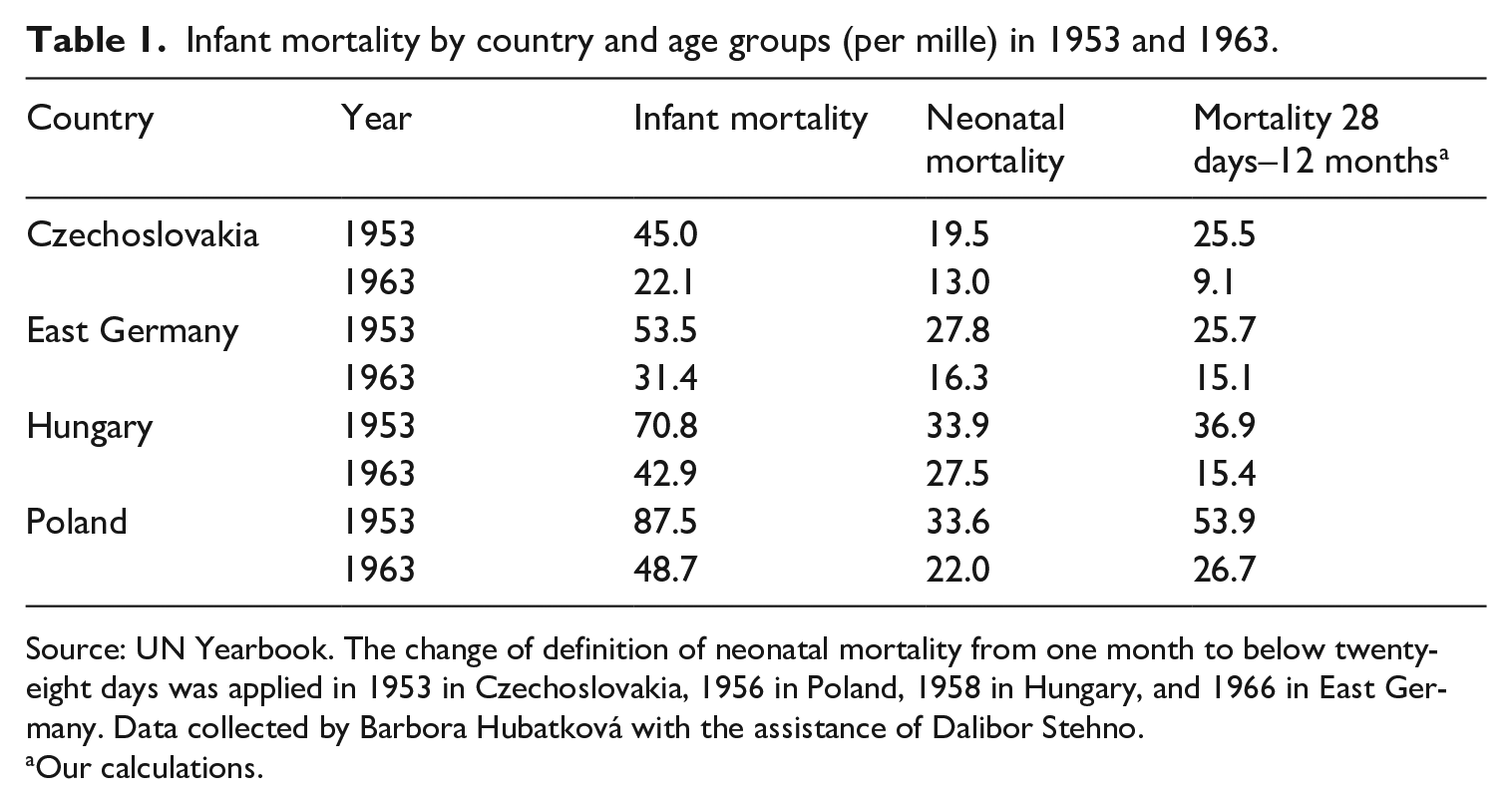
Source: UN Yearbook. The change of definition of neonatal mortality from one month to below twenty-eight days was applied in 1953 in Czechoslovakia, 1956 in Poland, 1958 in Hungary, and 1966 in East Germany. Data collected by Barbora Hubatková with the assistance of Dalibor Stehno.
Our calculations.
Our source material shows that medical doctors from our countries were familiar with these statistics. Gynecologists emphasized prenatal care, which could identify problematic pregnancies in time. In East Germany, the idea of pregnancy counseling was developed during the war and put into practice in the 1950s. However, it was not easy to persuade East German women to attend; only financial incentives accomplished that. A system of payments was put in place, and the woman got more money the more often she attended prenatal check-up visits. 46 In Czechoslovakia, it was not necessary to motivate women financially, yet in the late 1940s the country initially struggled with a lack of special institutions and trained staff who could advise on proper infant care that would prevent dangerous diseases or even loss of life. By the end of the decade, pregnancy courses opened in Brno and Prague, and social workers played an important role.
Polish doctors firmly believed that “advancements in the healthcare system play a more important role than improvements of economic conditions” in the struggle against infant mortality. 47 The Polish state healthcare system developed outpatient clinics for pregnant women shortly after the war, when their number increased from 127 in 1945 to 779 in 1947 (tending to over 106,000 women in 1947). More than 880 infant clinics tended to 600,000 babies in 1947. 48 From 1950, this network comprised the so-called K clinics (K for kobieta, woman) and D clinics (D for dzieci, children), both sick and healthy. 49 As in Czechoslovakia, experts embarked on an educational mission through visiting nurses and publications. 50 In Hungary, 1949 legislation gave rise to a system of registering pregnant women with the health system by a midwife who offered maternal health advice. The system was not fully state-controlled, as state and private midwives offered their services. Gynecological counseling was accompanied by midwife check-ups and a visiting nurse making house calls, ensuring the responsible implementation of medical advice for the mother-to-be. In 1953, midwives received a 50% pay increase for taking over prenatal care that then became compulsory for pregnant women to attend. Women did not always take advantage of this service and experts bemoaned the still high numbers of risky pregnancies going undetected and resulting in complicated births of vulnerable newborns or even perinatal deaths. This was despite the material incentive of a state-sponsored baby kit that was handed over during pregnancy care sessions. Based on a study conducted in the Debrecen Women’s Clinic over five years and published in 1959, doctors concluded that “the greatest task in combating perinatal mortality is preventive care, that the question of further increasing the surgical frequency is of secondary importance and that treatment and care of the newborn plays a third role.” 51 Preventative care was thus identified as vital. To motivate women, attendance became tied to maternity allowance in 1964: if a woman accessed pregnancy care only partially or not at all, her allowance was reduced accordingly.
What changed for a pregnant woman over time across our region was her option to give birth either at home or in an institution, be it a clinic or a hospital. The most dramatic changes occurred in Poland, where experts strongly advised clinics and professionally assisted birth from the early postwar period. In the early 1950s, almost four out of ten women delivered their babies at home with the help of a midwife (36% in 1951); less than two decades later, only two women in 100 had the same experience (2.3% in 1968). Hospital birth grew over the same period, from less than a third (30.1% in 1951) to almost eight in ten (79.5% in 1968), with birth under professional care reaching virtually every woman (99.3% in 1968). 52 Czechoslovak women also experienced an increase in institutional birth, albeit a bit earlier: immediately after the war, about half of women gave birth in a hospital (48.9% in 1948); five years later, it was eight in ten (81.5% in 1953) and more than nine in ten a decade later (96.2% in 1962). 53 In East Germany, in spite of the initial reluctance toward institutionalized birth, the numbers grew rapidly. 54 In 1946, the rate was 27%; in 1950, it rose to 38%. By 1956, 70% of deliveries occurred in a clinic and the number had grown to 98% by 1965. 55 In Hungary, women could give birth in various institutions: hospitals, clinics, birth institutes, and birth homes. They used them in increasing numbers. For example, in the city of Szeged in southern Hungary, up to half of births before 1945 took place at home; by 1953, home births were barely over 10%. 56
All four countries developed specialized care for prematurely born babies, whose high mortality greatly affected general infant mortality statistics. At a pediatric congress held in Leipzig in 1953, East German experts reported “the problem of prematurity as closely linked to perinatal mortality,” and strove to provide accurate care to prevent the immediate death of the babies. 57 To achieve that, they established special care wards next to the maternity facilities to avoid transporting the baby, as many did not survive that, and to provide a space where “obstetricians and pediatricians can work together under exemplary conditions.” 58 This approach to developing infrastructure for premature babies was shared by the other countries, although the networks of specialized wards expanded unevenly: in Czechoslovakia, where the first ward had opened in 1936, it was much more developed than in Poland. 59 Hungarian experts estimated that the central prematurity ward in Budapest could accept only 27% of those in need of intensive care in the early 1950s. 60
Further, experts tackled intractable conditions in rural areas. East Germany initiated an outpatient service providing “intensive home visits by midwives, community nurses and caregivers in the first months of life [that] can support and teach inexperienced mothers how to care for their babies. These home visits were particularly necessary in the winter months in rural communities.” 61 In Poland, as ministerial expert Eugenia Pomerska argued during a Polish–Czechoslovak demographic symposium on infant mortality in 1962, “high infant mortality is caused by the relatively slow development of culture and hygiene of the countryside.” 62 In 1950, the IMR was 101 per 1,000 in cities and 113.9 in the countryside; the difference became even more significant over the years: in 1960, the rates were 49.9 and 58.7, respectively. 63 Besides poor hygienic conditions, rural children had much worse access to healthcare. In the late 1940s, they “practically lack[ed] health care.” 64 For individual farmers, hospital care was free of charge only for birth and in the case of contagious diseases; it became fully accessible for children only in 1959. 65 In Poland – unlike the other countries in our region – in the late 1950s over 50% of child deaths occurred outside hospitals, and these proportions were even worse outside big cities. 66 At the Polish–Czechoslovak symposium, Polish experts concluded that the worse rates in their country resulted from its lower levels of urbanization and its less developed healthcare system. 67 The Hungarian countryside also suffered from underdeveloped infrastructure. To enhance birth conditions, health officials worked on connecting every village to the telecommunication system as well as improving the ambulance network. 68 The gradual establishment of rural birth homes was supposed to provide a safer environment for women giving birth far away from the nearest maternity hospital. 69
In any case, personnel training, growing professionalization, and the standardization of measures were occurring at a relatively high speed across our region. Importantly, all countries of our region strove to subsume the medical care surrounding pregnancy and childbirth under state control, integrated with state-enforceable quality controls. In Poland, the 1950s was a decade of new standardizing legislation on the working of healthcare institutions, medical procedures, registration, and reporting. For instance, in 1950 it regulated the outpatient clinics and milk banks; in 1958, newborn wards. In 1959, health booklets for children were introduced. Around the same time, the quarterly and annual regional reports on infant mortality were made obligatory; this was followed by the introduction of joint pediatrician–obstetrician elaboration of the analyses. Each case of death required an in-depth analysis. 70 Experts stressed the need for intensive training of midwives and doctors and for a rapid increase in the number of professionals, which had been extremely low in the aftermath of the war. 71 In East Germany, likewise, there were early regulations aiming to unify the healthcare system. During the war, Gustav Döderlein had devised a joint program whereby doctors, nurses, and midwives had to work in direct cooperation, as “there can be no question of doctors wanting to eliminate midwives, just as I can hardly believe that sensible midwives would have imagined providing health care without doctors.” 72
However, professionalization also meant clashes between various kinds of experts. In East Germany, midwives resisted the unification devised by the doctors. Midwives had different criteria on themes as important as where to give birth: midwives, as part of their traditional work, opted for home instead of clinic birth. In addition, they were poorly paid. This situation led to some midwives’ protests, which the East German state solved by raising their salaries and giving them better conditions. 73 However, clinic births continued to rise, and by the end of the 1950s, a clinic birth was an undisputed preference. By then, the unified system was fully implemented, along with further measures legislating counseling centers, milk banks, and the functioning of outpatient clinics. 74 In Hungary, where both state and private midwives became tied to the state reporting system in 1953, midwives were central to obstetrical care, especially in rural areas. Thus, the expertise and professional manner of midwives were decisive for positive birth outcomes, even more so in areas where a doctor’s assistance was not immediately accessible. Jenő Raics, founder of a state education system for midwifery in Debrecen, expressed criticism of irresponsible conduct during the birth process, sparking a debate between him and midwives. Midwives responded by acknowledging the unfortunate occurrence of mistakes but pointed to the need for improved availability of specialized doctors as well as ambulances. While the plea for improved infrastructure was especially urgent in rural areas, midwives also called for regular further education – ensuring state of the art knowledge. 75
In postwar Czechoslovakia, physicians agreed that an important link in the successful fight against high mortality was the cooperation of all experts involved in childcare, especially gynecologists and pediatricians. Since the highest number of deaths occurred shortly after birth, saving newborns was mainly a gynecological task. The pediatricians claimed that their care was of a high standard, which certainly could not be said of obstetric care, which needed to be improved.
76
Two prominent Czechoslovak pediatricians, Karel Poláček and Gustav Syrovátka, claimed that: A significant fact is that half of neonatal deaths are the result of birth trauma or anoxia, conditions that are directly causally related to delivery. These deaths almost invariably occur in the first days after birth, and it is clear that the best pediatric care has little application here and that the fate of this large group of children lies in the hands of obstetricians.
77
Similar tensions occurred in Poland, where pediatricians argued that early mortality (up to forty-eight hours) is usually the result of poor obstetric care. 78
In postnatal care, feeding was a hugely discussed topic. In East Germany, from an early stage, breastfeeding was considered superior to any type of artificial milk. 79 Experts and the health ministry called for campaigns of “breastfeeding propaganda” in the early 1950s. 80 Milk banks (FMS [Frauenmilchsammelstellen]) were launched as a more effective way to spread the use of human milk for those women who could not produce milk themselves, whether due to disease or poor nutrition. The health ministry planned to have, by 1954, seventy-five such milk banks to cover the whole territory. 81 In Hungary, experts recognized the feeding of (donated) breastmilk as crucial for combating infant mortality and superior to any other form of nutrition, specifically formula milk. As a result, milk banks were established across the country and also in prematurity wards in Budapest to improve the survival rates of preterm infants. 82 However, experts also recommended adding cow milk powder and honey to ensure extra nutrition and rapid weight gain. 83 In Poland, pediatricians strongly advised breastfeeding as they believed it was effective in reducing infant mortality, and campaigns encouraged women to breastfeed since the rates were unsatisfactory. The feeding of older infants, many of whom were dying as a consequence of diarrhea, was also under scrutiny, and feeding schemes were meant to improve the situation. 84 In Czechoslovakia, the first milk bank opened in 1949 in Prague. However, during the 1950s, some experts held that artificial milk, which was regularly advertised in the journal Časopis lékařů českých, was more beneficial for vulnerable premature babies. 85 The advertisements featured a drawing of a chubby baby reaching longingly for a can of Eviko artificial milk. 86 Although the range of artificial milk expanded in the following years, experts changed their view in the 1960s and came to consider breast milk as the best nutrition for newborns. 87
Unlike in other branches of medicine, the fight against infant mortality was not marked by Pavlovian approaches. While Pavlov was invoked in obstetrics, it was solely for the benefit of the mother, “creating a friendly and loving atmosphere that persuades women to face their pregnancy and childbirth with confidence and without fear.” 88 The “psychoprophylaxis for painless childbirth” was to ensure comfort for the woman; no benefit of a “healthy birth” for the child was invoked in Poland and Czechoslovakia, and only a few benefits were mentioned in Hungary and East Germany. This method, which according to Soviets ensured painless childbirth for up to 96% of women, arrived directly from the USSR at the very beginning of the 1950s to all our countries. However, the method did not bring the expected results and was abandoned by the end of the 1950s. 89
Similarities in the measures applied to combat early infant mortality were further strengthened by international exchanges between experts from state socialist countries in the early 1960s. At a 1962 symposium on combating perinatal death, medical doctors issued recommendations to be implemented in each country. These measures included broadening the scope of prenatal examination, focusing more on the risk of preterm birth, and introducing mandatory hospitalization and supervision of high-risk pregnancies. 90 As we show in the next section, the international experts’ agreement on measures contrasted with increasing tensions around the definition of livebirth.
Clashes over the definition of livebirth
In 1927, the League of Nations centered its definition of livebirth around drawing a breath: “A dead-birth is the birth of a foetus, after at least twenty-eight weeks’ pregnancy, in which pulmonary respiration does not occur; such a foetus may die either (a) before, (b) during or (c) after birth, but before it has breathed.” 91 However, as WHO experts acknowledged, this definition was not precise enough for defining livebirth vs. stillbirth. Decades later, there still was not a unified system of defining or, as a consequence, counting mortality rates. For example, in Spain a child had to survive twenty-four hours to be registered as a live birth; in France, a child born alive who died before registration was counted as a stillbirth. “Such differences in classification might, in some cases, mean a reduction in the general death-rate of the order of 1.2%,” noted the WHO experts. 92
Thus, in 1948, the WHO called for the preparation of a “list adapted to the problems of foeto-infantile morbidity and mortality” as part of the List of Diseases and Causes of Death, in which mortality was to be counted under one year, then by single years from one to four, subsequently in five-year increments until the age of eighty-four and then above eighty-five.
93
Two years later, the WHO Subcommittee on the Definition of Stillbirth and Abortion
94
provided the following definitions, approved by the Expert Committee on Health Statistics and Third World Assembly of WHO: Live birth is the complete expulsion or extraction from its mother of a product of conception, irrespective of the duration of pregnancy, which, after such separation, breathes or shows any other evidence of life, such as beating of the heart, pulsation of the umbilical cord, or definite movement of voluntary muscles, whether or not the umbilical cord has been cut or the placenta is attached; each product of such a birth is considered live born. Foetal death is death prior to the complete expulsion or extraction from its mother of a product of conception, irrespective of the duration of pregnancy; the death is indicated by the fact that after such separation the foetus does not breathe or show any other evidence of life, such as beating of the heart, pulsation of the umbilical cord, or definite movement of voluntary muscles.
Further, the experts imperatively added: “All live-born infants should be registered and counted as such, irrespective of the period of gestation, and if they die at any time following birth, they should also be registered and counted as deaths.” To underscore the point of “any sign of life means liveborn,” the Expert Group on Prematurity in 1950 refused to define a weight limit below which an expulsed or extracted fetus should be considered an “abortion.” In 1961, the Expert Committee on Maternal and Child Health suggested fine-tuning the counting of mortality rates – first twenty-four hours, then forty-eight hours, seven days, twenty-eight days, and one year. The WHO experts were thus very clear from the start about an all-encompassing definition of what counts as alive, and they stayed the course.
The introduction of the international definition was still a rather inconsistent process, as many countries had their own criteria for assessing what liveborn or stillborn meant. According to Soviet experts, the only sign of life was breath. Yet even babies who took a breath could have been discounted because those “who are born before 28 weeks [. . .], or who weigh less than 1000 grams, or who are less than 35 centimeters in length, are not supposed to be counted either as live births or infant deaths if they die within the first seven days (168 hours) after delivery, whether or not they even took a breath.” 95 Such babies were counted as miscarriages. 96 This strict definition was reflected in our region. Czechoslovakia adopted almost identical criteria in 1953 and other countries discussed this approach when evaluating their own mortality rates.
Before Czechoslovakia adopted the Soviet approach, all fetuses over 400 g emerging from the womb and dying after were included in perinatal mortality. 97 This translated into high IMRs. The definition was changed by a decree of the Ministry of Health in 1952 that came into force in 1953. According to the decree, Czechoslovakia used the same criteria for gestation length, weight, and length of the fetus as the USSR to define a liveborn child, but with two main differences. In the USSR, the child had to survive seven days to be counted; in Czechoslovakia, the liminal period for severely premature children was twenty-four hours. 98 Moreover, unlike Soviets, who considered only spontaneous breathing, Czechoslovak experts considered a child who “breathed spontaneously or after resuscitation” to be born alive. Babies who did not meet the conditions of gestation, length, and weight in the Soviet definition were classified as miscarriages and were thus not entered into IMR. 99 As a result, the numbers looked immediately much better and catapulted Czechoslovakia among the countries with the best IMRs, making it a champion in our region.
The Czechoslovak definition made other countries look bad in comparison. The Hungarian health minister and trained medical doctor Frigyes Doleschall celebrated the IMR of 6% that Hungary reached in the late 1950s as “a huge achievement when compared with older infant mortality rates of 10 and even almost 20 percent.” 100 Although noticeable improvements had indeed been made, Hungary was still lagging behind, not only across the Cold War divide but also within the socialist camp. The achievements were “not satisfactory when compared with the three percent infant mortality in the Soviet Union and Czechoslovakia,” despite major efforts in pre- and postnatal care. 101
While data collection did not follow unified criteria as proposed by the WHO, Hungarian demographers were quick to point out how different definitions of livebirth and stillbirth made a noticeable impact on infant mortality rates. As the “concept of stillbirth, and consequently the practice of birth registration and vital statistics, is not uniform even in developed countries,” registration policies made lower infant mortality rates possible, but not under the Hungarian rigid notification system.102,103 Any infant that gave at least one sign of life was considered liveborn, no matter how long it stayed alive. It is therefore hardly surprising that Hungary suffered especially from high first-day infant mortality rates. 104 Among the countries enjoying the lowest levels in this category, that is below 7%, demographers pointed out that “Czechoslovakia and France are undoubtedly not comparable with the others,” referring to data collection practices as described in the UN Demographic Yearbook. 105 Despite that, Hungarian experts stuck to the inclusive definition of livebirth.
In Poland, the experts took a different path. While dismal mortality rates in older groups (5–12 months) remained a concern, ministerial experts also discussed the problem of high mortality rates during the first day of life. In the early 1960s, they pointed to Czechoslovakia and France, where numbers were low because they did not register babies who were “unable to survive,” which resulted in Czechoslovakia recording 2.5 times lower rates than East Germany. 106 In Poland, all newborns showing any “sign of life” counted as born alive. Switching to “the Czechoslovak definition,” experts noted, would reduce the numbers by about five points, from 71 to 66. 107 Ministerial instruction on birth registration issued in 1962 in Poland thus changed the definition. Similar to the Czechoslovak definition, babies below 1,000 grams but with (whatever kind of) signs of life had to survive twenty-four hours in order to be counted as liveborn. The difference lay in classifying births that did not meet the criteria of survival, because in Poland they would be called stillborn, and “unviable” if below 601 grams, but these differences did not change the fact that the statistics of liveborn children were constructed in almost the same way. Ministerial experts argued that the change of the definition of livebirth affected the IMR to a limited degree: it dropped by 2.1–2.3 points. However, in cities and regions with low infant mortality, the difference was over 6 points – logically, these were places where early infant mortality was more significant than late infant mortality. Ministerial experts also claimed Polish numbers had become internationally comparable. 108 Other experts criticized the change, arguing that before 1962, the Polish definition had been “close to the international one” (meaning the WHO) and that the change “artificially lowered the number of live and stillborn, as well as infant mortality rates,” and made infant mortality, and perinatal mortality in particular, difficult to compare with other countries. 109 In spite of these critical voices, the new definitions persisted until the 1990s.
Around the same time that the Polish discussions on the definition took place, Poland attempted to unify the definitions in the whole socialist bloc, within a broader quest to agree on how medical statistics were to be constructed. In 1961, the Polish Ministry of Health and Social Care planned to issue a “call to the other state socialist countries to standardize criteria, to achieve comparable statistics” during an annual meeting of the health ministers, but the meeting did not take place that year. 110 Poland sent an inquiry to all the other countries in order to gather the necessary information to elaborate on joint criteria. In October 1962, at the International Symposium of Demographers in Moscow, Zygmunt Branowitzer, who headed the Department of Medical Statistics in the Ministry of Health, called for establishing common definitions in medical statistics, arguing that it had “an importance also from the ideological and political perspectives,” because when reporting to the WHO, state socialist countries seemed to have worse rates due to different criteria. 111 However, a unified socialist definition never materialized.
In East Germany until the early 1960s, the criteria relied exclusively on the presence of one of the signs of life: a heartbeat, lung respiration, or movement of voluntary muscles was sufficient to declare a baby liveborn. However, in 1961, experts raised the bar on what constituted livebirth from one to at least two signs of life. In West Germany, the one-sign-of-life rule continued to apply. The East German IMR dropped and was questioned in turn by West Germans as being a result of legal intervention, rather than an improvement in the healthcare system. The East German definition change was encouraged by Erwin Marcusson, a medical doctor and former deputy health minister. After the criticism arising from the West, Marcusson argued in 1963 that East German IMRs were already sharply decreasing in the years before adopting the new definition. In addition, in 1962, right after the new definition came into force, the differences from previous IMRs were far from striking. 112
The tensions within the socialist camp came to a head in 1963 at a symposium on “Infant mortality: A guide to combating it from an international perspective” hosted in East Berlin and attended by leading experts from East-Central Europe. The event opened with optimistic words from the organizers: “Thirty years ago, no one would have predicted that [an] infant mortality rate of 15 per mille could be sustained for years in entire countries.” 113 East German doctors brought up the issue of the livebirth definition in the opening lecture of the symposium. They declared the definition “of an influence that should not be underestimated” as it might have “a disturbing effect on temporal or territorial comparisons and can falsify the results.” The East Germans outlined the state socialist definitions and asserted that “while the definitions of Hungary, Romania and the GDR” could “be compared without restriction [. . .] those of the Soviet Union and Czechoslovakia, and recently also Poland, differ.” The experts concluded that “the definitions used in the Soviet Union, Czechoslovakia and Poland restrict the numbers of dead infants [. . .] so when calculating the IMR, a certain difference arises, not with regard to the calculation method, but according to the definition.” 114 The East Germans were closer to the countries following the WHO definition more strictly and claimed that using their definition in countries such as Czechoslovakia meant that “the crude infant mortality rate would be somewhat higher than is currently reported.” Indeed, “applying the Czechoslovak definition to the conditions in the GDR would result in an infant mortality rate of 20.5 instead of 31.7 for 1962.” The East Germans considered the WHO definition, which they and the Hungarians followed, as strictly superior to the Czechoslovak, Polish, and Soviet model. As they concluded: “In the discussion, it was pointed out very forcefully that, in the interest of truth and humanism, every child who showed signs of life after birth should be counted as a liveborn child, irrespective of other criteria such as length, weight, or survival time.” 115
Indeed, Hungarian experts took data reporting according to WHO standards seriously long before rejoining the WHO in 1963. The experts were eager to point out that Hungary’s compliance with WHO standards resulted in internationally comparable data, knowing that such comparability had not been reached within the socialist bloc nor on an international level. After Hungary’s admission to the WHO in 1963, the experts provided data surpassing the WHO norm, delivering answers on the age and maturity of all infants who died in more detail than requested. 116
Czechoslovak experts often mentioned that their foreign colleagues criticized the definition they used and the results it produced. They themselves admitted that the definition led to better numbers, as they stated that “the requirement of three conditions if the termination of pregnancy is to be considered a birth hides a certain tendency to shift fetuses with little chance of survival into miscarriages, resulting in some decrease in perinatal and infant mortality.” 117 They argued that the pre-1953 definition was highly disadvantageous for Czechoslovakia and were convinced that the lowered rates were also the result of advanced care, not only the “new definition” and the effects it brought: “It is also certain that in the previous period from 1949 to 1952 [the definition was based on] very extreme criteria, namely a weight of 400 g. It is also true that it was in 1953 that the fight against perinatal mortality was proclaimed and fully mobilized in collaboration with pediatricians and also with pathologists.” 118 To defend themselves even more strongly, Czechoslovaks indicated other countries that used the same definition, saying that “the USSR recommends criteria identical to our decree, with the difference that severely premature fetuses are registered only if they survive 7 days.” 119
Despite these justifications, Czechoslovakia adopted the international definition of liveborn and stillborn in 1965. Livebirth was newly defined as a baby who was born (regardless of the length of gestation) and was breathing or showing another sign of life (heartbeat, umbilical cord pulsation, or active muscle movement). Stillbirth was defined as a baby who died before birth and showed no sign of life. For the purposes of demographic statistics, stillborn babies were divided into further groups according to the length of gestation. The perinatal period was shortened from ten days to seven days.
120
Stillbirth before the twenty-eighth week of pregnancy was considered a miscarriage, and after twenty-eight weeks was classified as perinatal mortality.
121
The change in definition was immediately reflected in increased IMRs. Czechoslovak experts were, unsurprisingly, dissatisfied with this increase as they compared the current IMRs with those according to the old definition to show that the numbers were in fact not as bad as they might have seemed: The infant mortality rate in the Czechoslovak Socialist Republic rose to 25.3‰ in 1965 from 21.4‰ in 1964 [. . .] The overall increase of 3.9‰ is in 2.7‰ cases caused by the change in definition, since 647 individuals who would have been considered miscarriages under the old definition were included among the infant deaths. The actual increase in infant mortality is 1.2‰.
122
On the other hand, even before the new definition was introduced, experts said they would welcome an international definition because it would allow for better comparison with mortality rates in other countries, and the Czechoslovak numbers would not be labeled as unreliable. They again argued in support of good prenatal care, stressing mainly the high percentage of hospital births, the wide range of specialized institutions, and the good cooperation of all experts, as 80% of all perinatal deaths were autopsied. 123
In Hungary, the definition of livebirth vs. stillbirth remained constant while the country eagerly followed recommendations on the WHO level. Unfortunately, the IMRs had not improved by the mid-1960s through medical measures as anticipated. Instead, experts were left to celebrate a specific achievement in contrast to capitalist countries, priding themselves on overcoming class differences, stating that “under the capitalist system considerable differences in infant mortality between the various social strata remain almost unchanged or even increased [. . .], while socialist development has resulted in a sharp narrowing of these differences.” 124 Thus, Hungarian experts linked their fight against infant mortality to egalitarian premises of socialism while they continued their efforts on the ground for many years, as did their East-Central European neighbors.
In East Germany, the two-signs-of-life criteria were applied until the late 1970s. However, some critical voices arose from the medical profession, advocating for “adhering strictly to the WHO definition” instead of the newly passed legislation. 125 Indeed, historians argued that in practice many East German doctors reported babies as “liveborn” who had at least one sign of life. 126 The IMR decreased over time and East Germany became one of the best of the socialist camp and only slightly inferior to the leading Western countries. Despite the initial dissatisfaction of Czechoslovak experts with higher IMRs after adopting the 1965 definition, it remained unchanged until 1988. Poland, where IMR fell significantly in the 1970s and 1980s, kept the narrow definition of livebirth until the early 1990s.
Conclusion
The story of the standardization of infant mortality counting and measures to save newborns’ lives in the second half of the twentieth century, as we present it here, is one of establishing a global standard (on the WHO level) and its uneven local application (on the levels of East-Central European nation states). It is a story of challenges and contestations among the nation states where the global definition was invoked by some as the gold standard because nothing less than what “we” consider life was at stake, and of the pragmatic motivations to make a given state look better in international comparisons. In response, others grudgingly modified their counting methods, but even that did not bring about uniformity, not even across East-Central Europe. Despite the “global” and “uniform” outlook, we are reminded that “standardization is a recursive practice” and that “standards are intensely local.” 127 While standardization strives to achieve homogeneity, this aim is hardly ever fully accomplished. Yet, the expert discussions we analyze here show that incrementally, standardization moves along.
We have shown that in the medically and politically sensitive matter of infant mortality, experts in East-Central European countries acted independently of the geopolitical pressures of the era, yet with good knowledge of international developments. Despite not being active members of the WHO for most of the 1950s (for some countries even longer), experts implemented measures closely resembling those recommended by the WHO; in Poland and Czechoslovakia, UNICEF provided some support in lieu of the WHO. Across our region, personnel were trained in assisting childbirth and infrastructure was significantly extended for expectant mothers to receive counseling during pregnancy and care during labor and beyond. While expert groups negotiated responsibilities – such as pediatricians and obstetricians in Czechoslovakia and midwives and physicians in Hungary – by the end of the 1950s, measures taken to ensure healthy childbirth had been largely standardized. The only point of slight divergence from WHO recommendations was Czechoslovak insistence on exclusively hospital delivery. Other countries initially made arrangements for improved home delivery, as advised by the WHO; Czechoslovakia was quick to normalize hospital birth. However, in the 1960s, the overwhelming majority of children were born outside of the home in all our countries. Overall, rapid changes in the organization of healthcare drove down the numbers of babies dying in the perinatal period.
Curiously, the Soviet influence on saving children at birth was rather fleeting. While Pavlovian methods of preparing women for birth, allegedly doing away with pain during labor, made an impression across East-Central Europe, the interest was short-lived as the methods did not bring the expected results. Only in Hungary did medical doctors point out a potential benefit to the child; even that did not prove useful in practice.
The Soviet influence on definitions of livebirth was similarly limited. How livebirth is defined is consequential for IMRs: only those who are first counted as liveborn and who then die enter IMR statistics. Only one East-Central European country implemented a definition approximating the Soviet one: in 1953, Czechoslovakia introduced an identical definition of the newborns’ minimal measurements to be declared alive and also only counted breathing as a sign of life; yet it importantly differed in waiting twenty-four hours (where Soviets took seven days), after which period the surviving child was ultimately declared liveborn. While this Soviet-like definition was established at the height of Stalinization, nothing in our sources suggests an imposition, let alone pressure from Moscow. In fact, the rhetoric used by Czechoslovak experts indicates convenience: employing this definition significantly improved their IMR numbers. In a ripple effect, Poland, whose IMR lagged behind that of its neighbors, suggested following the Czechoslovak example and unifying the definition across the socialist camp. However, no unification was achieved; only Poland changed their own definition so that it resembled the Czechoslovak one.
While Czechoslovakia and Poland exhibited a certain expediency when it came to definitions, Hungary and East Germany were rather staunch proponents of an all-encompassing definition of livebirth, a stance very much in line with the inclusive definition promoted by the WHO. This transnational organization never imposed any minimal measurements for a newborn to be counted alive and insisted on a wide array of signs, any of which constituted livebirth. East Germany embraced this approach and yielded only slightly when, in 1961, in a competition with its western neighbor, it raised the required evidence of life from one to at least two signs. Hungary, on the other hand, never wavered in applying the rigorous WHO definition of livebirth, despite the negative effect on IMR statistics.
In 1963, a symposium held in East Berlin laid bare the dissatisfaction of those adhering to definitions closer to the WHO with the countries employing pragmatic ways of counting. East German experts invoked socialism and humanism, to compel everyone to count all life as life. Czechoslovak experts, as the main culprits, attempted to shield themselves behind the Soviet definition, but they quickly yielded to pressure and adopted the WHO definition in 1965. In the end, Poland’s definition rendered its infant mortality statistics unusable for international comparison.
In the transnational knowledge exchange that surrounded the definition of livebirth, as well as the measures to combat infant mortality, we have documented a rather high level of independence of East-Central European countries from the developments in the Soviet Union. We have shown that, in both the measures and the definitions, our countries tended to implement what was recommended by the WHO. Nevertheless, as we have shown, clashes over the definition of livebirth occurred between state socialist countries, and this case reveals that the Soviet bloc was by no means unified in the approach to such an important issue as the counting of infant mortality. These findings give further nuance to the historical narrative on state socialism, public health, and international exchange, including the global process of standardizing medical practices.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Czech Science Foundation, EXPRO grant agreement GX21-28766X.
1.
Max Sefrin, “Einheit von Sozialismus und Humanismus,” Neue Zeit, November 12, 1965.
2.
Carlo A. Corsini and Pier Paolo Viazzo (eds.), The Decline of Infant and Child Mortality: The European Experience: 1750–1990 (The Hague: Brill Nijhoff, 1997).
3.
4.
The exact numbers for 1946 are: 119.8 per mille in Poland; 116.5 in Hungary; 108 in Czechoslovakia; and 130 in East Germany (Soviet Occupation Zone). For 1965: 41.7 per mille in Poland; 38.8 in Hungary; 25.5 in Czechoslovakia; and 24.8 in East Germany (source: UN Demographic Yearbook).
5.
We use perinatal in its dictionary definition, as “a period around childbirth.” It is pertinent to our argument that definitions change in time and place. Indeed, to this day, there is no universal definition of perinatal: it is usually defined as beginning at a point of fetal viability and lasting until seven days or one month after delivery. After one month up to one year, a child can succumb to late infant mortality. This period, however, calls for different measures to be implemented, e.g., vaccines, vitamins, and antibiotics have grown in prominence. Also, importantly for the focus of this paper, the measure of IMR is no longer affected by the definition of livebirth.
6.
Barbara Klich-Kluczewska, “Making Up for the Losses of War: Reproduction Politics in Postwar Poland,” in Maren Röger, Ruth Leiserowitz (ed.) Women and Men at War: A Gender Perspective on World War II and Its Aftermath in Central and Eastern Europe (Osnabrück: DHI Fibre Verlag, 2012), pp.307–28; Ewelina Szpak, “Chory człowiek jest wtedy jak go coś boli”: społeczno-kulturowa historia zdrowia i choroby na wsi w Polsce Ludowej. (Warszawa: IH PAN, 2018); Lenka Kalinová, Společenské proměny v čase socialistického experimentu: k sociálním dějinám v letech 1945-1969 (Praha: Academia, 2007), pp.88–91, 134–9; Petr Svobodný and Ludmila Hlaváčková, Dějiny lékařství v českých zemích (Praha: Triton, 2004), pp.217–21; Eszter Varsa, “Sex Advice East and West: Sex Education and Family Planning in Cold War Austria and Hungary,” The History of the Family 25, no. 4 (2020): 649–70; Julianna Novák, “Normális szülés Magyarországon a 20. század elejétől napjainkig,” in Barbara Kisdi (ed.), Létkérdések a születés körül (Budapest: L’Harmattan, 2015), pp.149–84; Dóra Vargha, Polio across the Iron Curtain: Hungary’s Cold War with an Epidemic, 1st ed. (Cambridge: Cambridge University Press, 2018), especially pp.42–45; Anna-Sabine Ernst, “Die beste Prophylaxe ist der Sozialismus”: Ärzte und medizinische Hochschullehrer in der SBZ/DDR 1945 – 1961 (Münster: Waxmann, 1997); Jutta Braun, “Politische Medizin. Ideologie und Gesundheitsökonomie im SED-Staat der 1950er- und 1960er-Jahre” (Göttingen: Wallstein, 2020).
7.
We analyze the changing expert understanding of pregnancy and childbirth in socialist East-Central Europe in our forthcoming paper “Work, Marriage, and Premature Birth: The Socio-Medicalisation of Pregnancy in State Socialist East-Central Europe” in the journal Medical History, doi:10.1017/mdh.2023.28.
8.
Dawid Dziuba, “The Issue of Infant Mortality in Polish Historical Research,” Przeszłość Demograficzna Polski 42 (2020): 9–35.
9.
Sylwia Kuźma-Markowska, “Walka z ‘babkami’ o zdrowie kobiet: medykalizacja przerywania ciąży w Polsce w latach pięćdziesiątych i sześćdziesiątych XX wieku,” Polska 1944/45-1989. Studia i Materiały 15 (2018): 189–215.
10.
Tamás Faragó, “Csecsemőhalandóság Magyarországon a 18–20. században,” in Zsolt Horváth, András Lugosi, and Ferenc Sohajda (eds.), Léptékváltó társadalomtörténet: tanulmányok a 60 éves Benda Gyula tiszteletére (Budapest: Hermész Kör-Osiris, 2003), pp.46–74.
11.
Éva Orosz, “Health and Development under State Socialism: The Hungarian Experience,” in David Phillips and Yola Verhasselt (eds.), Health and Development (London: Routledge, 1994), pp.276–88.
12.
Svobodný and Hlaváčková, Dějiny lékařství v českých zemích (note 6); Milena Lenderová et al., Velké dějiny zemí Koruny české. Tematická řada, Dětství., Vydání první, Velké dějiny zemí Koruny české. Tematická řada 8 (Praha: Paseka, 2021).
13.
J. Rychtarikova, “Infant Mortality Trends in Countries of Central and Eastern Europe,” Demografie 37, no. 2 (1995): 113–25; Jacques Vallin, Jitka Rychtaříková, and France Meslé, “Comparative Study of Mortality Trends in France and Czech Republic since 1950,” Population 44, no. 1 (1989): 291–321.
14.
Donna Harsch, “The Fight against Infant Mortality in Cold War Germany: East/West Convergence on Liberal Governmentality,” The Journal of Modern History 93, no. 2 (2021): 401–32.
15.
Sabine Major, Zur Geschichte der außerklinischen Geburtshilfe in der Deutschen Demokratischen Republik (Berlin, Germany: Humboldt University, 2003); Jörg Vögele, Luisa Rittershaus, and Thorsten Halling, “‘Breast Is Best’—Infant-Feeding, Infant Mortality and Infant Welfare in Germany during the Late Nineteenth and Twentieth Centuries,” Health 5, no. 12 (2013): 2190–203; Stefan Mallik, “Lebendgeburt und Totgeburt in der DDR. Motive und Konsequenzen der Neudefinition von 1961,” Geschichte der Gynäkologie und Geburtshilfe 46 (2013): 858–64.
16.
Vicente Navarro, “Has Socialism Failed? An Analysis of Health Indicators under Capitalism and Socialism,” Science & Society 57, no. 1 (1993): 6–30; Carles Muntaner et al., “Politics, Welfare Regimes, and Population Health: Controversies and Evidence,” Sociology of Health & Illness 33, no. 6 (2011): 946–64.
17.
Ibid., 946.
18.
Corsini and Viazzo, The Decline of Infant and Child Mortality (note 2); Lucia Pozzi and Diego Ramiro Fariñas, “Infant and Child Mortality in the Past,” Annales de Démographie Historique 129, no. 1 (2015): 55–75, 66.
19.
Marcos Cueto, Theodore M. Brown, and Elizabeth Fee, The World Health Organization: A History. Global Health Histories (Cambridge, United Kingdom: Cambridge University Press, 2019).
20.
Bogdan C. Iacob, “Health,” in Bogdan C. Iacob (ed.), Socialism Goes Global (Oxford: Oxford University Press, 2022), pp. 255–89; Bogdan C. Iacob, “Malariology and Decolonization: Eastern European Experts from the League of Nations to the World Health Organization,” Journal of Global History 17, no. 2 (2022): 233–53.
21.
Dóra Vargha, “Technical Assistance and Socialist International Health: Hungary, the WHO and the Korean War,” History and Technology 36, nos. 3–4 (2020): 400–17, 403–6.
22.
Stefan Timmermans and Steven Epstein, “A World of Standards but Not a Standard World: Toward a Sociology of Standards and Standardization,” Annual Review of Sociology 36, no. 1 (2010): 69–89, 71.
23.
Ibid., 74.
24.
Gayle Davis, “Stillbirth Registration and Perceptions of Infant Death, 1900–60: The Scottish Case in National Context,” The Economic History Review 62, no. 3 (2009): 629–54.
25.
George Emery, Facts of Life: The Social Construction of Vital Statistics, Ontario, 1869-1952 (Montreal: McGill-Queen’s University Press, 1993). For further discussion see Martha Lampland and Susan Leigh Star (eds.), Standards and Their Stories: How Quantifying, Classifying, and Formalizing Practices Shape Everyday Life (Ithaca, NY: Cornell University Press, 2009).
26.
Nadja Durbach, “Dead or Alive? Stillbirth Registration, Premature Babies, and the Definition of Life in England and Wales, 1836–1960,” Bulletin of the History of Medicine 94, no. 1 (2020): 64–90, 66.
27.
Yi-Tang Lin, “Making Standards to Quantify All Health Matters: The World Health Organization’s Statistical Practices, 1946–1960,” Monde(s) 11, no. 1 (2017): 247–66.
28.
Walter Krämer and Klaus Leciejewski, “Statistik im Sozialismus,” AStA Wirtschafts- und Sozialstatistisches Archiv 15, no. 2 (2021): 73–91.
29.
Nadezhda Aleshina and Gerry Redmond, “How High Is Infant Mortality in Central and Eastern Europe and the Commonwealth of Independent States?” Population Studies 59, no. 1 (2005): 39–54; G. Gourbin and G. Masuy-Stroobant, “Registration of Vital Data: Are Live Births and Stillbirths Comparable All over Europe?” Bulletin of the World Health Organization 73, no. 4 (1995): 449–60.
30.
31.
Godelieve Masuy-Stroobant, “Infant Health and Infant Mortality in Europe,” in Carlo A. Corsini and Pier Paolo Viazzo (eds.), The Decline of Infant and Child Mortality: The European Experience, 1750–1990 (The Hague: Martinus Nijhoff, 1997), pp.1–34.
32.
Krämer and Leciejewski, “Statistik im Sozialismus” (note 28).
33.
34.
Lindsay Prior, “Repositioning Documents in Social Research,” Sociology 42, no. 5 (2008): 821–36, 825.
35.
36.
Poland rejoined in 1957, Czechoslovakia in 1958, and Hungary in 1963. East Germany only joined the UN in 1973, enabling it to become part of the WHO.
37.
World Health Organization (ed.), Expert Group on Prematurity: Final Report [on a Meeting Held in] Geneva, 17–21 April 1950. World Health Organization Technical Report Series, no. 27 (Geneva, Switzerland: World Health Organization, 1950), p.8.
38.
Ibid., p.12.
39.
40.
UNA Technical Assistance for Social Welfare – Cooperation and Liaison – Specialized Agencies – United Nations Children Fund (UNICEF) Western Europe; S-0441-1547-0004.
41.
UNA Technical Assistance for Social Welfare – Cooperation and Liaison – Expert Assistance to Governments – United Nations Children Fund (UNICEF); S-0441-1546-0001.
42.
World Health Organization and Chisholm, The Work of WHO 1951, p.110 (note 39).
43.
44.
45.
46.
J. Brey and J. Wienold, “Welchen Einfluss nimmt die Sozialgesetzgebung auf die Frühgeburtlichkeit?” Zeitschrift für ärztliche Fortbildung 2 (1962): 79–84.
47.
Irena Krysztofowicz, Zwalczanie umieralności niemowląt. Biblioteka Lekarza Praktyka. Seria 2; t. 64 (Warszawa: Państwowy Zakład Wydawnictw Lekarskich, 1971).
48.
Rajmund Barański, “Opieka nad matką, noworodkiem i niemowlęciem,” Pediatria Polska 4 (1948): 477–93.
49.
Krysztofowicz, Zwalczanie umieralności niemowląt (note 47).
50.
See, for example, advice books and the journal Mother and Child, published by the Institute of Mother and Child, the latter also including instructions for healthcare educators (przodownice zdrowia).
51.
Jenő Raics, “A perinatális mortalitás okainak elemzése klinikánk ötéves anyagában,” Magyar Nőorvosok Lapja 22, no. 4 (1959): 202–21, 219.
52.
Krysztofowicz, Zwalczanie umieralności niemowląt, p.53 (note 47). In the 1950s, clinic birth could be performed either in a hospital or a birth room (izba porodowa) attended by a midwife.
53.
Miroslav Vojta, Lubomír Jíra, and Augustin Syrovátka, “Úspěchy zdravotní péče o matku a dítě v Československu,” Demografie: Revue pro výzkum populačního vývoje 5, no. 3 (1963): 247.
54.
Gustav Döderlein, “Häusliche und klinische Geburtshilfe in heutiger Zeit – Tagung der medizinisch-wissenschaftlichen Gesellschaften für Geburtshilfe und Gynäkologie an den Universitäten Greifswald und Rostock 1949,” Zentralblatt für Gynäkologie 73, no. 11 (1951): 1061–2.
55.
Statistisches Jahrbuch der Deutschen Demokratischen Republik (1950 – 1989) (Berlin: Staatsverlag der Deutschen Demokratischen Republik, 1990). 556–57
56.
János Batizfalvy, “Alkotmányos anyavédelem,” Viharsarok, August 9, 1953: 5.
57.
L. Weingärtner, “Kinderärzte-Tagung der DDR in Leipzig vom 24. bis 26. April 1953,” Kinderärztliche Praxis 13 (1953): 487–500.
58.
Gerhard Opitz, Über die Ursachen der Frühgeburt (Berlin: Volk und Gesundheit, 1956), p.115.
59.
Izabela Bielicka and Janina Kochanowska-Sikorska, “Zachorowalność i śmiertelność wcześniaków,” Pediatria Polska 33, no. 7 (1958): 821–30. In 1957, there were twenty-two premature infant stations in the Czech lands and twelve in Slovakia. Olga Štolová and Helena Dufková, “Současný stav a další vývoj péče o nedonošené děti,” Československá pediatrie 23, no. 3 (1968): 193–7, 193.
60.
Rudolf Pomóthy, Kálmán Frank, and Lajos István, “Koraszülöttápolásunk,” Gyermekgyógyászat 2, no. 12 (1951): 353–62.
61.
Erwin Marcusson, “Maßnahmen zur weiteren Senkung der Säuglingssterblichkeit,” Zeitschrift für ärztliche Fortbildung 57, no. 23 (1954): 1269–77, 1271.
62.
M. Namysłowska, “Sprawozdanie z polsko-czechosłowackiego sympozjum demograficznego w Jabłonnie pod Warszawą w dniach 2-5 września 1962,” Studia Demograficzne 1 (1963): 95–111, 96.
63.
Władysław Kondrat, Umieralność niemowląt w latach 1950–1972 (Warszawa: Główny Urząd Statystyczny, 1974), p.26.
64.
Barański, “Opieka nad matką, noworodkiem i niemowlęciem” (note 48), p.485.
65.
Helena Słomczyńska, “Zadania ochrony zdrowia matki i dziecka w świetle dotychczasowych osiągnięć,” Pediatria Polska 28, no. 7 (1953): 663–70; Krysztofowicz, Zwalczanie umieralności niemowląt (note 47).
66.
Irena Krysztofowicz, “Problemy umieralności niemowląt w Polsce,” Pediatria Polska 34 (1959): 1027–36.
67.
Namysłowska, “Sprawozdanie z polsko-czechosłowackiego sympozjum demograficznego w Jabłonnie pod Warszawą w dniach 2-5 września 1962” (note 62). Czechoslovak demographers also reported on the symposium and its main topics, see Z. Pavlík, “Polsko-československé demografické symposium v Jabłonnie,” Demografie: Revue pro výzkum populačního vývoje 5 (1963): 181–2.
68.
István Kováts, “A szülészeti ellátás,” Orvosok Lapja 4, no. 26 (1948): 389–94.
69.
György Hatos, “Anyavédelmünk fejlődésének megnyilvánulásai és a fejlődés okai,” Népegészségügy 32, no. 4 (1951): 159–63.
70.
Krysztofowicz, Zwalczanie umieralności niemowląt, pp.56–7 (note 47).
71.
Słomczyńska, “Zadania ochrony zdrowia matki i dziecka w świetle dotychczasowych osiągnięć” (note 65).
72.
Gustav Döderlein, “Ärztliche Schwangerschaftsvorsorge und ihre gesetzliche Regelung,” in H. Fuchs and H. Naujoks (eds.), Verhandlungen der deutschen Gesellschaft für Gynäkologie 1941 (Heidelberg, Germany: Springer, 1942), pp.175–96, 181.
73.
Harsch, “The Fight against Infant Mortality in Cold War Germany” (note 13).
74.
Major, Zur Geschichte der außerklinischen Geburtshilfe in der Deutschen Demokratischen Republik, pp.33–6 (note 14).
75.
Jenő Raics, “A szülésznői munka jelentősége a szülészeti eredmények javulásában,” Egészségügyi munka 3, no. 3 (1956): 65–9.
76.
Karel Poláček, “Úmrtnost nedonošených dětí během prvního roku života,” Pediatrické listy : orgán Československé pediatrické společnosti (sekce Čs. lékařské společnosti J.E.Purkyně) 7, no. 4 (1952): 201–4, 201; Kamil Kubát, Karel Poláček, and Helena Trojanová, “Několik základních dat o nedonošených dětech narozených v Praze v letech 1947–1948,” Československá gynaekologie : časopis Gynekologické a porodnické společnosti 15, no. 3 (1950): 250–7, 255–6.
77.
Karel Poláček and Gustav Syrovátka, “Péče o nedonošené děti v Československu, její možnosti a úkoly,” Pediatrické listy: orgán Československé pediatrické společnosti (sekce Čs. lékařské společnosti J.E.Purkyně) 6, no. 5 (1951): 294–300, 295.
78.
K. Jerzykowska-Kuleszyna and I. Żywicka-Twarowska, Śmiertelność noworodków w 1951 r. opracowana na podstawie materiału oddziału noworodków kliniki położniczo-ginekologicznej AM w Poznaniu,” Pediatria Polska 27, no. 9 (1952): 1091–7.
79.
Karl-Heinz Mehlan, “Über die Notwendigkeit des Stillens,” Das deutsche Gesundheitswesen 8, no. 34 (1954): 1033–7.
80.
Johannes Schoedel, “Zwei Fehler heutiger Säuglingsernährung: Mangelnder Stillwille und vorzeitige Breinahrung,” Das deutsche Gesundheitswesen 8 (1949): 1136–42.
81.
Eva Schmidt-Kolmer, “Frauenmilchsammelstellen in ländlichen Bezirken,” Das deutsche Gesundheitswesen 9, no. 36 (1964): 1066–99.
82.
Tamás Fülöp, “Az orvos-egészségügyi dolgozók szakszervezetének III. kongresszusáról,” Orvosi Hetilap 101, no. 50 (1960): 1789–93.
83.
Kálmán Frank, Domján Jánosné, and Mangliár Károlyné, “Koraszülött-táplálásunk változása 10 év alatt és az ezzel elért eredmények értékelése,” Gyermekgyógyászat 18, no. 3 (1967): 359–66; István Szentkirályi and Obál Ferencné, “A méz hatása koraszülöttek súlygyarapodására,” Gyermekgyógyászat 5, no. 7 (1954): 203–9.
84.
Izabela Bielicka, Mikołaj Łącki, and Irena Sztachelska, Niektóre zagadnienia organizacji opieki otwartej nad najmłodszym dzieckiem w świetle wycinkowej analizy zachorowalności i umieralności niemowląt z powodu biegunki,” Pediatria Polska 31, no. 4 (1956): 449–58.
85.
Miroslav Mrázek, “Ošetřování předčasných novorozenců,” Československá gynaekologie: časopis Gynekologické a porodnické společnosti 15, no. 1 (1950): 151–7, 154.
86.
“[Eviko],” Časopis lékařů českých 92, no. 32 (1953): 886.
87.
Miroslav Toman and O. Fintajslová, “Význam mateřského mléka ve výživě nedonošence,” Československá pediatrie 16, no. 5 (1961): 392–5.
88.
Imre Hirschler, “A fájdalommentes szülés. A szülési fájdalom ,megszüntetése’” Természet és Társadalom 115, no. 4 (1956): 222–4, 224.
89.
Gustav Döderlein, “Häusliche und klinische Geburtshilfe – Tagung der medizinisch-wissenschaftlichen Gesellschaften für Geburtshilfe und Gynäkologie an der Universität Leipzig 1957,” Zentralblatt für Gynäkologie 79, no. 15 (1957): 590–2; Ema Hrešanová, “The Psychoprophylactic Method of Painless Childbirth in Socialist Czechoslovakia: From State Propaganda to Activism of Enthusiasts,” Medical History 60, no. 04 (2016): 534–56; Agnieszka Kościańska and Agata Ignaciuk, “Re-gendering Childbirth: Catholicism and Medical Activism Regarding Birth Preparation in Communist and Early Democratic Poland (1950s–1990s),” Journal of the History of Medicine and Allied Sciences, <![]() >; G. Silló-Seidel, “Kritik der Schwangerenprophylaxe im Rahmen der Statistik,” in G. Döderlein and H. Kirchhoff (eds.), Verhandlungen der deutschen Gesellschaft für Gynäkologie (Berlin: Springer, 1960), pp.403–5; Hirschler, “A fájdalommentes szülés.” (note 88).
>; G. Silló-Seidel, “Kritik der Schwangerenprophylaxe im Rahmen der Statistik,” in G. Döderlein and H. Kirchhoff (eds.), Verhandlungen der deutschen Gesellschaft für Gynäkologie (Berlin: Springer, 1960), pp.403–5; Hirschler, “A fájdalommentes szülés.” (note 88).
90.
Ireneusz Roszkowski, Zalecenia międzynarodowego sympozjum przedstawicieli krajów demokracji ludowej w zwalczaniu śmiertelności okołoporodowej,” Ginekologia Polska 34 (1963): 655–8.
91.
Harry Sutherland Gear, Yves Biraud, and Satya Swaroop, “International Work in Health Statistics, 1948–1958 / H. S. Gear, Y. Biraud, S. Swaroop,” 1961, p.17, <![]() > (May 17, 2022), citing from League of Nations (1927) “Report of the Committee [of] Expert Statisticians on the Definition of Stillbirth, Geneva” (Document C.H./Expert Stat./46).
> (May 17, 2022), citing from League of Nations (1927) “Report of the Committee [of] Expert Statisticians on the Definition of Stillbirth, Geneva” (Document C.H./Expert Stat./46).
92.
Ibid.
93.
94.
What is meant by abortion here is actually miscarriage. In medical literature, “abortion” was used to describe the spontaneous end of a pregnancy, years before the procedure now referred to as an “abortion” was legalized. To further complicate matters, in many languages of the countries we study, there is no linguistic distinction. For example, in Czech, “potrat” means both abortion and miscarriage. It is possible to add the adjective “spontánní” to indicate miscarriage, but this was not done in the medical literature of the time we analyze. We have chosen to continue using the original terminology of our sources.
95.
Barbara A. Anderson and Brian D. Silver, “Infant Mortality in the Soviet Union: Regional Differences and Measurement Issues,” Population and Development Review 12, no. 4 (1986): 705–38, 708.
96.
Ibid.
97.
Olga Štolová and Jan Jerie, “Perinatální úmrtnost v ČSSR v mezinárodním srovnání,” Československé zdravotnictví : časopis Společnosti sociálního lékařství 12, no. 9 (1964): 428–31, 428.
98.
Karel Poláček, “Základní statistické pojmy perinatálního období,” Československá pediatrie 19, no. 9 (1964): 775–7, 776.
99.
Ibid., 776–7.
100.
“Az 1959. évi egészségügyi költségvetésről, az egészségügy távlati tervének eddig kialakult elgondolásairól beszélt dr. Doleschall Frigyes egészségügyi miniszter szakszervezetünk továbbképző tanfolyamán,” Egészségügyi Dolgozó 3, no. 3 (1959): 3.
101.
Ibid., 3.
102.
Lajos Salamon, “A halvaszületésekről,” Demográfia 3, no. 1 (1960): 107–20, 107.
103.
Béla Pápai, “Az újszülöttkori halálozás egyes kérdései Budapesten és néhány Európai nagyvárosban,” Demográfia 3, no. 3–4 (1960): 447–60.
104.
KSH, “A 24 órán belüli csecsemőhalandóság. A KSH népesedésstatisztikai osztályának közleménye,” Demográfia 6, no. 2 (1963): 247–54.
105.
Ibid., 248.
106.
Zygmunt Branowitzer, “Umieralność dzieci do 1 roku życia (niemowląt) w Polsce w latach 1958-1961,” Zdrowie Publiczne 7 (1963): 295–301, I. Krysztofowicz, Ocena wyników walki z umieralnością niemowląt w 1959 roku,” Pediatria Polska 35 (1960): 1419–39.
107.
Branowitzer, “Umieralność dzieci do 1 roku życia (niemowląt) w Polsce w latach 1958-1961” (note 106).
108.
Alina Lenc-Krumholz, Współczynniki umieralności niemowląt a kryteria żywych urodzeń,” Zdrowie Publiczne 4 (1967): 501–4.
109.
Kondrat, Umieralność niemowląt w latach 1950–1972, pp.16–17 (note 63).
110.
Archiwum Akt Nowych, Ministerstwo Zdrowia i Opieki Społecznej, 1/8.
111.
Zygmunt Branowitzer, “Zagadnienie ujednolicenia pojęć i zasad rejestracji w badaniach statystycznych w zakresie statystyki medycznej,” Zdrowie Publiczne 11 (1963): 519–22, 522.
112.
Marcusson, “Maßnahmen zur weiteren Senkung der Säuglingssterblichkeit” (note 61).
113.
Kurt Winter, “Vorwort,” in Kurt Winter (ed.), Säuglingssterblichkeit. Eine Anleitung zu ihrer Bekämpfung aus internationaler Sicht (Leipzig: VEB Georg Thieme, 1964), p.VIII.
114.
Werner Hesselbarth, Reimer Schorr, and Kurt Winter, “Begriffe und Methoden zur Erfassung der Säuglingssterblichkeit,” in Kurt Winter (ed.), Säuglingssterblichkeit. Eine Anleitung zu ihrer Bekämpfung aus internationaler Sicht (Leipzig, VEB Georg Thieme, 1964), pp.1–9, 2.
115.
Ibid., 6.
116.
szn, “A csecsemőhalálozás alakulása 1964-ben. Egy tanulmány margójára,” Egészségügyi Dolgozó 9, no. 11 (1965): 2.
117.
Poláček, “Základní statistické pojmy perinatálního období,” 776 (note 98).
118.
Štolová and Jerie, “Perinatální úmrtnost v ČSSR v mezinárodním srovnání,” 429 (note 97).
119.
Poláček, “Základní statistické pojmy perinatálního období,” 776–7 (note 98).
120.
Jan Jaroš, “Kojenecká, novorozenecká a perinatální úmrtnost v ČSSR - od 1. ledna podle me-zinárodních definic,” Československé zdravotnictví: časopis Společnosti sociálního lékařství 13, no. 2 (1965): 93–4.
121.
“Vyhláška ministerstva zdravotnictví o povinném hlášení živě i mrtvě narozeného plodu, úmrtí dítěte do sedmi dnů po porodu a úmrtí matky: (24. 11. 1964),” Československá pediatrie 20, no. 1 (1965): 67–70, 69.
122.
Kamil Kubát, Olga Štolová, and Augustin Syrovátka, “Kojenecká úmrtnost v ČSSR po změně definice živě narozeného dítěte. Některé biologické a sociální faktory ovlivňující kojeneckou úmrtnost,” Československá pediatrie 21, no. 9 (1966): 832–40, 833.
123.
Štolová and Jerie, “Perinatální úmrtnost v ČSSR v mezinárodním srovnání,” 430 (note 97).
124.
Tamás Fülöp, “Szociális és kulturális faktor szerepe a csecsemőhalandóságban,” Orvosi Hetilap 107, no. 9 (1966): 1966: 385–9, 389.
125.
Hesselbarth et al., “Begriffe und Methoden zur Erfassung der Säuglingssterblichkeit,” 7 (note 114).
126.
Mallik, “Lebendgeburt und Totgeburt in der DDR. Motive und Konsequenzen der Neudefinition von 1961” (note 15).
127.
Lampland and Star, Standards and Their Stories, pp.14, 16 (note 25).