
Abstract
The prevalence of Helicobacter pylori (Hp) in India is approximately 64%. However, substantial regional variations necessitate high-fidelity, locality-specific studies to characterise its population distribution in India. We conducted a cross-sectional study including 2998 dyspeptic patients at a tertiary care centre in Karnataka and investigated the relationship between Hp prevalence and the Multidimensional Poverty Index (MPI) by district. Helicobacter pylori prevalence in our population was 43.2% with a significant correlation between district-specific Hp prevalence and MPI. This data can be leveraged for evaluating local Hp infection control strategies, planning interventions for Hp hotspots in Karnataka and predicting a dyspeptic patient's risk of Hp infection.
Introduction
Helicobacter pylori (Hp) is of global relevance due to its widespread prevalence and strong association with upper gastrointestinal inflammation and gastric malignancy.1,2 The prevalence of Hp in India is substantial, but there are limited high-fidelity studies to help characterise it. 1 Analysis of these studies would improve understanding of epidemiological trends, the disparity in resource allocation, and the efficacy of current management patterns. We describe the geographical distribution of Hp in Karnataka and characterise our study population by Hp status. We further investigate the correlation between the prevalence of Hp and the India National Multidimensional Poverty Index (MPI).
Methods
We reviewed records at Kasturba Medical College, Manipal, a tertiary care centre located in the Udupi district of Karnataka, India, of patients 18 and older who underwent endoscopy for dyspepsia between 2016 and 2020, under the Department of General Surgery. Dyspepsia was defined as at least one of the following symptoms: epigastric pain, epigastric burning, early satiation or postprandial fullness. Data collected from electronic patient records included age, sex, district of residence, symptoms, endoscopic findings and histopathological results, including Hp status. The prevalence of Hp in Karnataka was calculated by district in those with at least 10 patients. The districts of Karnataka are divided among four administrative divisions, namely Bengaluru, Mysuru, Belagavi and Gulbarga. To include dyspeptic individuals from districts with <10 patients, prevalence was also calculated by division. Additionally, we calculated the Hp prevalence in patients from Kerala and out of state.
Multidimensional Poverty Index values were obtained from the ‘India National Multidimensional Poverty Index 2021: Baseline Report’, detailed by the policy commission of the Government of India, the National Institution for Transforming India (NITI Aayog). 3 Although available for Karnataka and individual districts, MPIs were unavailable for administrative divisions. These were calculated as a weighted average of the individual member districts’ MPIs in proportion to the magnitude of their individual populations, obtained from the 2011 Census of India. 4 In addition, they were calculated in accordance with the number of people in our study seeking care from the respective division, described as a sample weighted average MPI (swaMPI). Similarly, for patients from outside Karnataka, a swaMPI was calculated in accordance with the number of people seeking healthcare at our hospital from each distinct individual state. N.B. as Vijayanagara is a new district of Bellary, the district was considered to have the same MPI as Bellary for the purposes of this study.
The data were analysed using SPSS 27.0. Descriptive statistics were computed for continuous variables, including minimum and maximum values, means and standard deviations. Frequencies of categorical variables were computed with 95% confidence intervals. A linear regression was performed to delineate a correlation between MPI and Hp prevalence. No imputation was attempted for missing data. The study was approved by the Institutional Ethics Committee at Kasturba Hospital.
Results
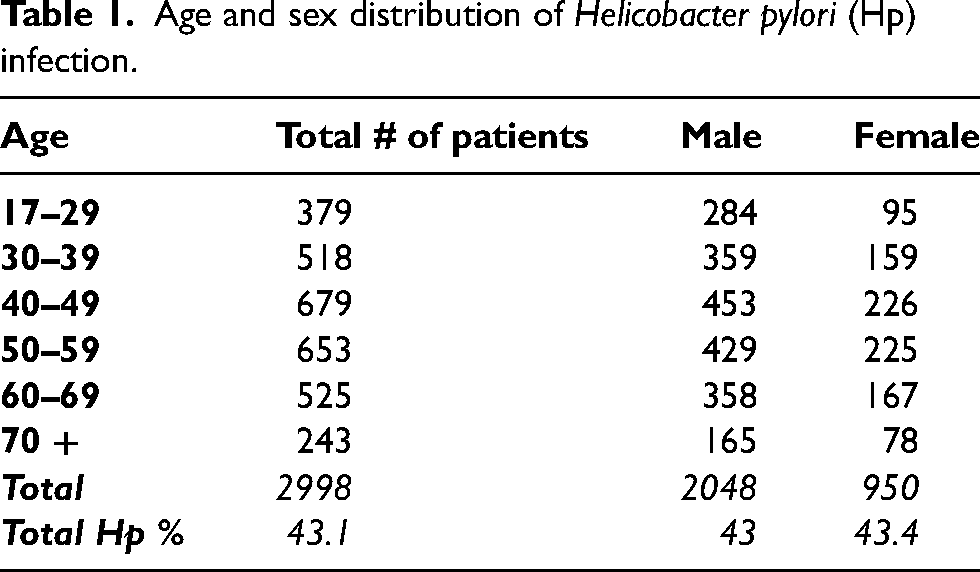
In total, 2998 patients underwent UGI endoscopy and a concomitant gastroduodenal biopsy. The age and sex distributions of patients, along with symptoms experienced, are represented in Tables 1 and 2. Among the dyspeptic patients, 94.7% had abnormal macroscopic endoscopy findings, and 43.2% were positive for Hp.
Age and sex distribution of Helicobacter pylori (Hp) infection.
Distribution of presenting symptoms and the corresponding Helicobacter pylori (Hp) prevalence.

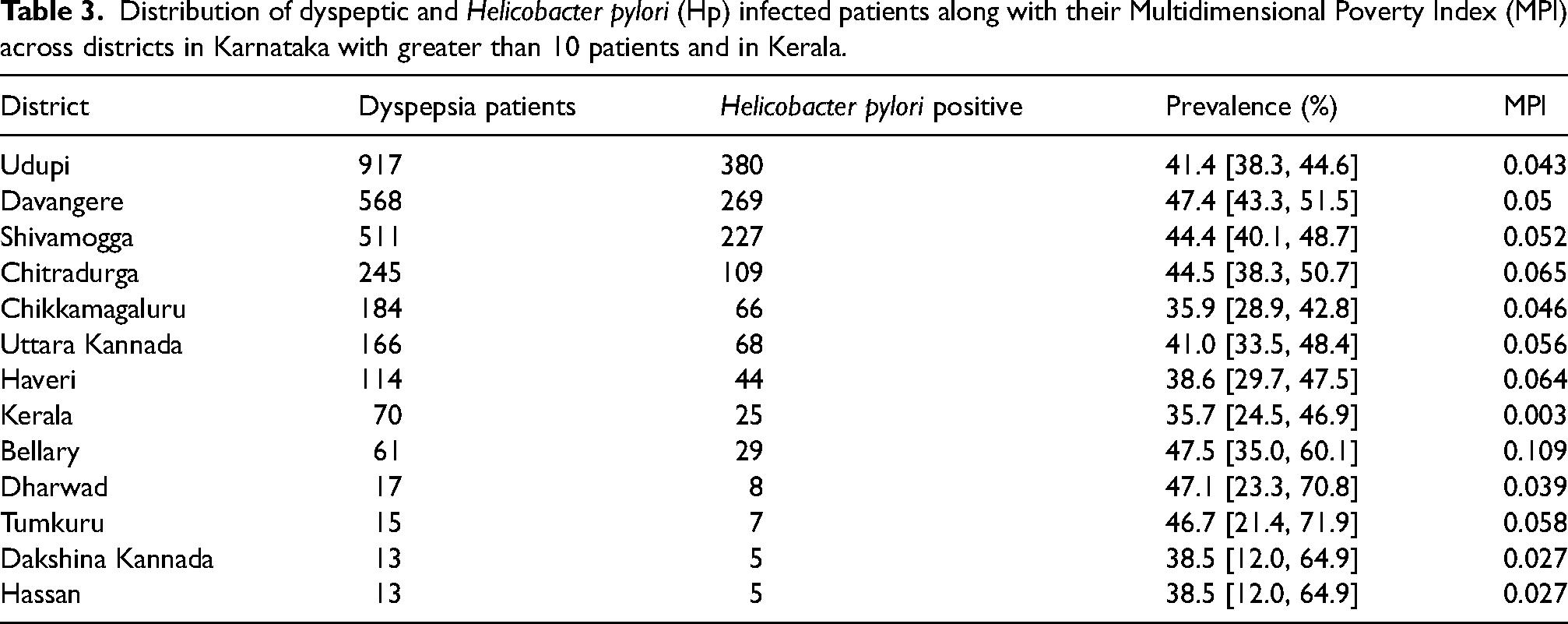
Patients from various districts of Karnataka were evaluated at KMC Manipal for dyspepsia. These districts are divided into four administrative divisions, namely Bengaluru, Mysuru, Belagavi and Gulbarga, in descending order of patient volume. The prevalence was calculated only for districts with at least 10 patients. In addition, to include dyspeptic individuals from districts with few patients, prevalence was calculated for each administrative division. The patient distribution and Hp positivity are detailed in Table 3 and pictorially exhibited in Figure 1. Helicobacter pylori prevalence and MPI have been schematically represented in Figure 2.
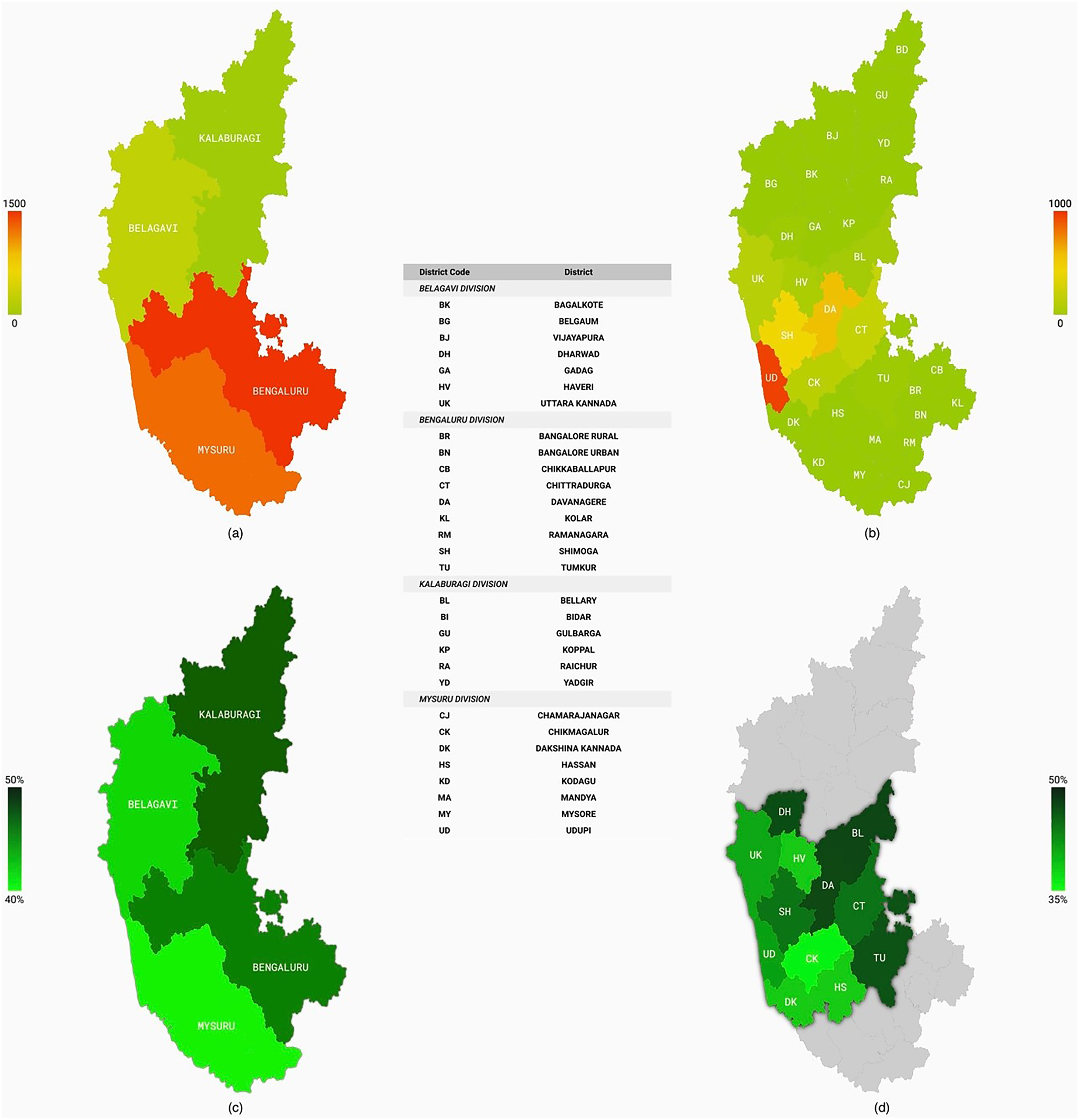
A schematic overview of prevalence of Helicobacter pylori among patients visiting Kasturba Hospital, Manipal, in the state of Karnataka, India. (a) Number of patients visiting from each administrative division of Karnataka. (b) Number of patients from each district in the state of Karnataka. (c) Prevalence of Helicobacter pylori amongst the administrative divisions of Karnataka. (d) Prevalence of H. pylori in individual districts of Karnataka with at least 10 patients seeking care in Kasturba Hospital, Manipal, for dyspepsia.
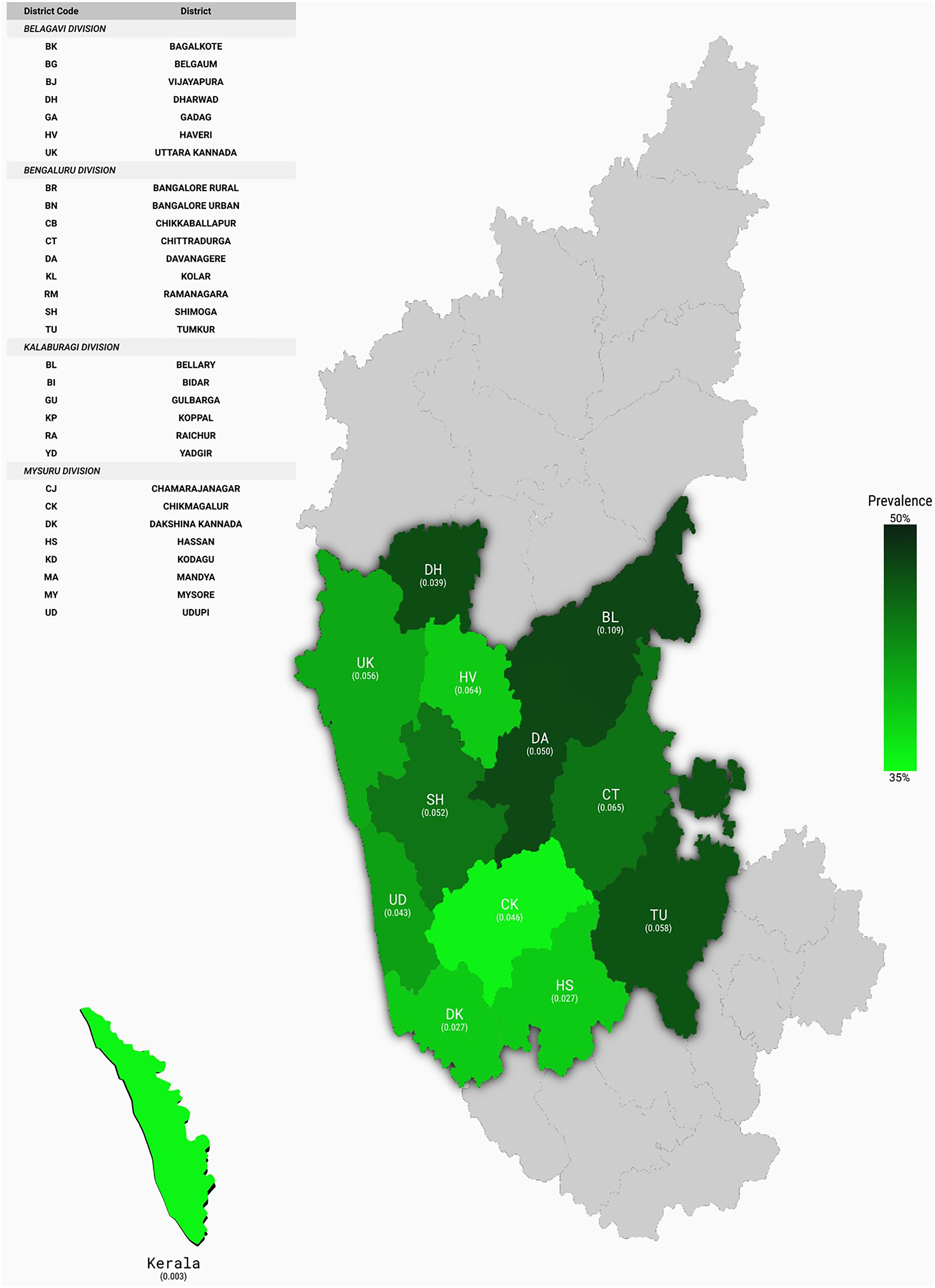
Schematic representation correlating Multidimensional Poverty Index (MPI) and Helicobacter pylori (Hp) prevalence in major districts in Karnataka and Kerala.
Distribution of dyspeptic and Helicobacter pylori (Hp) infected patients along with their Multidimensional Poverty Index (MPI) across districts in Karnataka with greater than 10 patients and in Kerala.
The 2021 NITI Aayog baseline report provided MPIs for all states and districts of India, including those of Karnataka. The calculated swaMPI for Karnataka was estimated to be 0.051 from our study and 0.056 according to the NITI Aayog report, as exhibited in Table 4. A linear regression model between the MPI and the prevalence of Hp in each district (and Kerala) with at least 10 patients was developed (R2 = 0.352, p < 0.05), as exhibited in Figure 3.
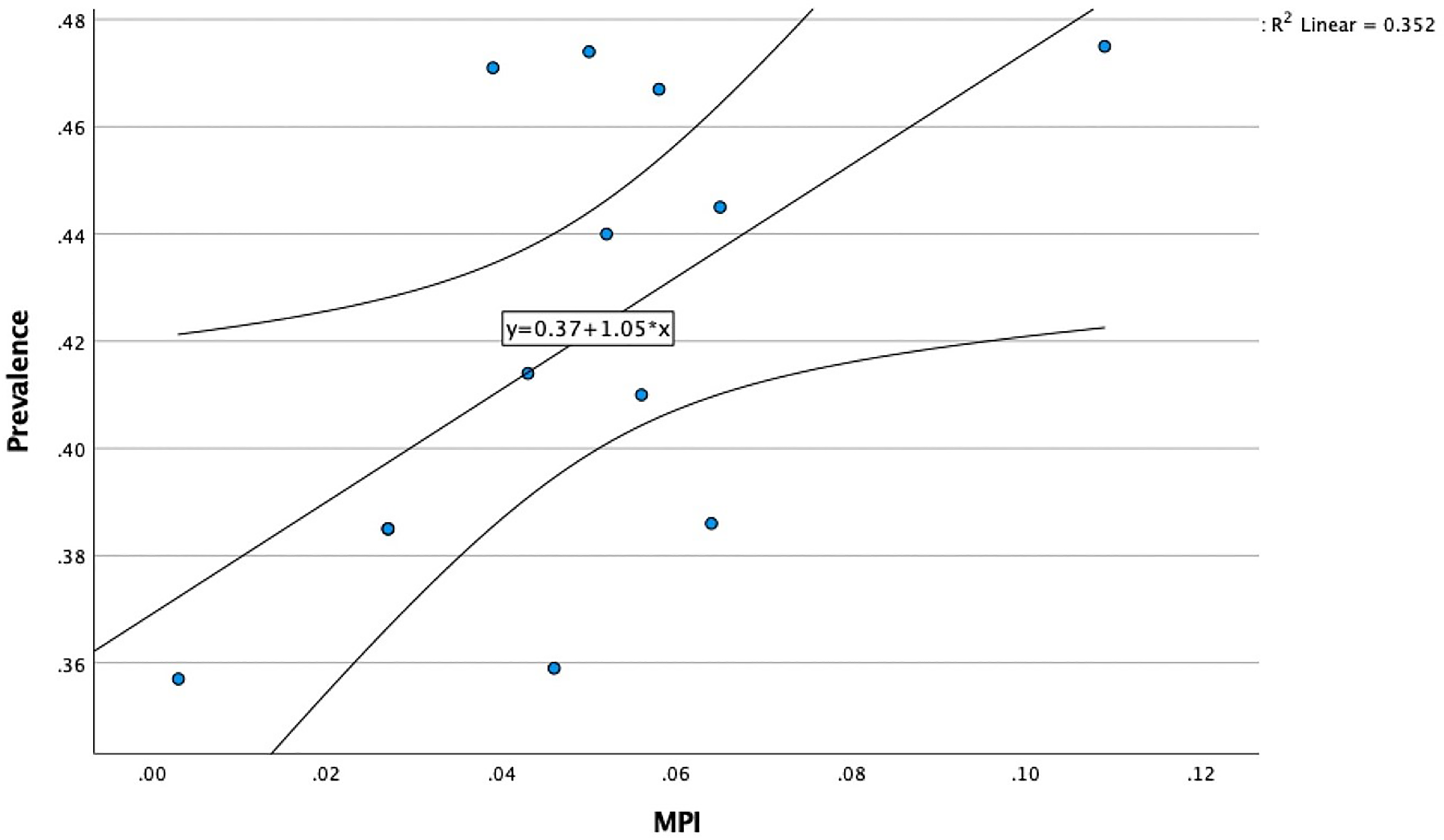
Linear regression model between the Multidimensional Poverty Index (MPI) and prevalence of Helicobacter pylori of each district (p < 0.05).
Distribution of dyspeptic and Helicobacter pylori (Hp) infected patients along with their calculated Multidimensional Poverty Index (MPI) and sample weighted average MPI (swaMPI) across the administrative divisions of Karnataka.
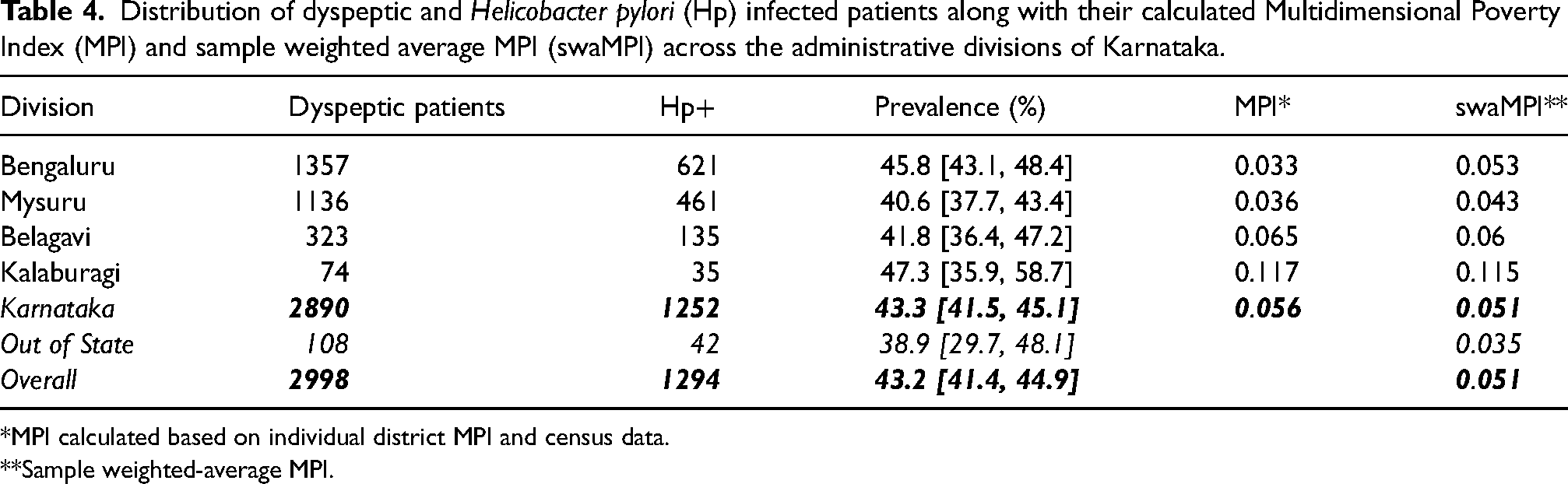
*MPI calculated based on individual district MPI and census data.
**Sample weighted-average MPI.
Discussion
Helicobacter pylori is the most prevalent bacterial infection worldwide, estimated to have colonised 60% of the global population and up to 64% of India's. 5 However, there is substantial regional variation, 1 underscored by studies from Tamil Nadu (41.9%), 6 Kashmir (58%), 7 and Orissa (58.8%). 8 Notably, Hp is highly prevalent in disadvantaged populations where hygiene is a public concern as the bacterium spreads via the orofaecal route.1,5 Therefore, analysing epidemiological population data in relation to poverty indicators becomes critical to understanding these regional variations. In 2021, NITI Aayog published a baseline report on the novel National MPI as a metric to estimate poverty in India by district or state. Multidimensional Poverty Index is a product of the proportion of the population that is multi-dimensionally poor (‘headcount ratio’) and the proportion of weighted indicators of which the population in poverty is deprived (‘intensity of poverty’). 3 Multidimensional Poverty Index quantifies factors such as health, education, sanitation, economic status and access to basic needs into a simple yet all-inclusive metric.
India has a higher MPI than Karnataka (0.118 vs. 0.056) and, subsequently, Hp prevalence among dyspeptic patients in Karnataka is less than the national community prevalence (43% vs. 64%).3,5 Karnataka performs better than most states in India and achieves one of the lowest MPIs in South India, only second to Telangana. 3 However, the variation in poverty indices is not only an interstate phenomenon but also an intrastate one, a phenomenon evident in the Hp prevalence rates as well. The Kalaburagi division exhibited the highest Hp prevalence, MPI and swaMPI. It consists of the poorest districts in Karnataka, with 5/7 member districts having an MPI >0.1. However, immense progress has been made there, with the incidence of poverty reducing from 57.4% to 38.2% between 2004–05 and 2011–12. 9 On the contrary, the Mysuru division had the lowest Hp prevalence and swaMPI, and this has historically been the most developed division in Karnataka,3,9 with 7/8 districts having an MPI < 0.05.
In comparison, the Bengaluru, Belgavi and Kalaburagi divisions have 4/9, 2/7 and 0/7 districts with an MPI < 0.05, respectively. However, overall, the Bengaluru division has the highest MPI. The swaMPI of the Mysuru division may be higher than that of the Bengaluru division, as we received few patients from Bangalore Urban (MPI = 0.008) and Bangalore Rural (MPI = 0.028), the population of which makes up a large proportion of the division. However, we received many patients from the surrounding Davangere, Shivamogga and Chitradurga districts, which all have MPIs of at least 0.05, potentially contributing to an inflated swaMPI and a higher Hp prevalence in this division. 3
We demonstrated a moderate correlation between MPI and Hp prevalence in dyspeptic patients, suggesting that socioeconomic development may reduce Hp population burden. The development of a model based on the correlation between reliable existing surveillance data, like MPI, and a more difficult index to assess in the population, like Hp prevalence, has merit. In fact, MPI could be utilised to predict the likelihood of a dyspeptic patient having Hp. Furthermore, swaMPIs help suggest if the sample population is a good representation of the actual population from a socioeconomic standpoint. In our study, Karnataka's swaMPI and MPI were similar, suggesting that our sample is representative of Karnataka's population. This supports the idea that our results may be translated to Karnataka as a whole.
The retrospective nature of this study is its main limitation; owing to the lack of standardisation of care, all dyspeptic patients may not have undergone endoscopy. In addition, most of our patients come from the southern districts of Karnataka, leading to a possible inconsistency in the reliability of the data between north and south Karnataka. Lastly, our regression model includes data from only 13/31 districts of Karnataka. Multi-centre cooperation across Karnataka or a centralised Hp infection reporting system would allow for data collection that is better representative of the reference population.
Conclusion
Conducting high-quality prevalence studies in multiple regions of the country helps identify Hp hotspots, foster region-specific management guidelines and develop a framework for feedback-dependent quality control measures. Utilising metrics such as MPI to predict Hp prevalence has the potential to help prioritise areas where further epidemiological studies are required to confirm Hp hotspots and design interventions. Such machine learning algorithms may help identify patients at risk for Hp, especially in resource-limited endemic areas. Resources for Hp screening are not widely available in India and are rather expensive for mass screening. This forms the foundation for a future study to develop and test an algorithm to identify patients at risk for Hp infection and requires further evaluation.
Footnotes
Author contributions
Aadithyavikram Venkatesan and Akhilesh Gonuguntla contributed equally to this paper and will be regarded as co-first authors for this paper. Aadithiyavikram Venkatesan, Akhilesh Gonuguntla, Krishna Kalyan Reddy Janumpalli and Badareesh Lakshminarayana contributed to the study design and conceptualization. Material preparation and data collection were performed by Aadithiyavikram Venkatesan and Ashwin Abraham. Data analysis was performed by Akhilesh Gonuguntla. Data representation and illustrations were performed by Ashwin Abraham and Akhilesh Gonuguntla. The manuscript was written by Akhilesh Gonuguntla and Aadithiyavikram Venkatesan. All authors read and approved the final manuscript.
Ethics
Formal ethical approval was obtained from Institutional Ethical Committee, Kasturba Medical College, Manipal prior commencing the study. (Approval Number: 946/2020). This retrospective study involving human participants was in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.