
Abstract
Thrombotic complications in liver abscess are less commonly identified in the literature. In this prospective observational study, vascular thrombosis was detected in 21.9% cases. However, there was no significant difference in outcome with or without vascular thrombosis, properly treated.
Introduction
The liver is a unique organ owing to its dual blood supply from the portal vein (∼75%) and hepatic artery (∼25%). It is exposed to various toxins and gut organisms when portal venous blood passes through its sinusoids. In a liver abscess (LA) there is localized destruction of parenchyma. The occurrence of LA is associated with several complications, including pleural effusion, rupture into the peritoneal, pleural or pericardial spaces as well as thrombosis in the vessels. 1 Such often go unnoticed since their signs are not obvious, but their consequences may be disastrous. Nonetheless, the presence of thrombosis may be suspected if there is recurrence of fever, pedal oedema, an overtly tender and enlarged liver or signs of portal hypertension. Therefore, a high level of clinical suspicion should be kept and efforts to rule out thrombosis-related complications must be initiated early. Contrast-enhanced CT scan is superior to ultrasound Doppler in this context. 2 Current data on prevalence of thrombotic complications are predominantly retrospective and conflicting.
Materials and methods
Our prospective observational study was conducted in the departments of General Medicine, Radio-diagnosis and Pathology at our hospital over a duration of 18 months. All patients over 18 years old and with clinical and radiological evidence of LA on trans-abdominal ultrasound were enrolled. Informed written consent was obtained from the patients. The study commenced after due clearance of our Institutional Ethics Committee vide letter no. GMC/IEC/2020/502R/156 dated 08.04.2021.
The optimum sample size was calculated on the basis of 42% prevalence of venous thrombosis in LA patients. 3 Assuming 95% confidence levels and 10% permissible error, the optimum sample size was derived to be a minimum of 93 cases. Patients were excluded if they had a known hyper-coagulable state, pregnancy, malignancy, were taking anticoagulant therapy, had a history of abdominal trauma or previous thrombotic episodes, or had known allergy or a contraindication to contrast agents.
Once the diagnosis of LA was confirmed, and after an overnight fast, a plain CT followed by contrast-enhanced study was performed with a Philips Ingenuity Core 64 slice CT scanner. Non-ionic iodine-based contrast, viz. Iohexol 300 mg, was given intravenously and scanning was carried out during the porto-venous phase of contrast enhancement at 50 s after the injection. Delayed scans were taken as required. The CT images were analyzed by a single experienced radiologist, confirming number, size, nature of LA, and complications as well as hepatic, portal venous, or inferior vena caval thrombosis. The patients underwent therapeutic intervention or conservative medical management based on clinico-radiological decision. Guided aspiration of the abscess or pig-tail drainage was carried out if the LA was in left lobe, had impending rupture on imaging, or if it had a thin (<10 mm) rim of liver parenchyma around it, if multiple LAs were present and if there was no response to medical therapy. Simple aspiration was carried out if the abscess was 5–10 cm in size and pigtail catheter drainage if >10 cm. If purulent fluid was aspirated, it was sent for microscopy, culture and sensitivity. Patients were monitored for complications during their hospital stay, and disease outcome was evaluated at the time of discharge and at 3 months following discharge by ultrasound. Follow-up Doppler was done additionally in patients with prior thrombotic complications.
The association of qualitative variables was analyzed using the χ2 test. Paired t-test was used for comparison of size as estimated by USG and CT scan. Logistic regression was used for association of quantitative variables with thrombus. The analysis was done using Statistical Package for Social Sciences software, IBM manufacturer, Chicago, USA, version 25.0. For statistical significance, p-value of < 0.05 was considered significant.
Results
A total of 98 patients were enrolled, 2 had a liver malignancy, and were excluded, leaving 96 in the study group. Their mean age was 42.2 ± 12.1 years. The male:female ratio was 11:1. The majority (59.4%) belonged to the upper lower class of the modified Kuppuswamy's socioeconomic scale. 4 41.7% came from a rural background. Use of alcohol was observed in 35.4% while 9.38% had diabetes mellitus.
The most common symptom was right upper quadrant pain (96.9%) followed by fever (93.8%) breathlessness (27%), extreme fatigue (21%) and dysentery (4.2%).The mean body mass index of study participants was 22.7 kg/m2. Icterus was present in 14.6%, pedal oedema in 8.3% and lymphadenopathy in a single patient. Abdominal tenderness was present in 96.9%, and 84.4% had hepatomegaly.
Liver function tests were deranged in 65%, while acute kidney injury was seen in 7.2%. Abscess aspirate culture was obtained in 80 patients, of whom 66 were sterile. The most commonly detected organisms were E. coli and Klebsiella, others being Salmonella, Acinetobacter and Proteus.
The most common LA location was the right lobe (87.5%) followed by left lobe (9.4%) and a single abscess in the caudate lobe. The mean size of LA on CT was 8.6 ± 2.8 cm. CT scan was able to detect multiple LA in 15.6%. Intestinal colitis and appendicitis were commonly associated abnormalities, followed by biliary and pancreatic disorders.
Vascular thrombosis was observed in 21.9%, affecting the hepatic veins (HV) in 13, portal vein (PV) in 10 (Fig. 1). Vena caval thrombosis was seen in 7. Concurrent hepatic and portal vein thrombosis was seen in 4.
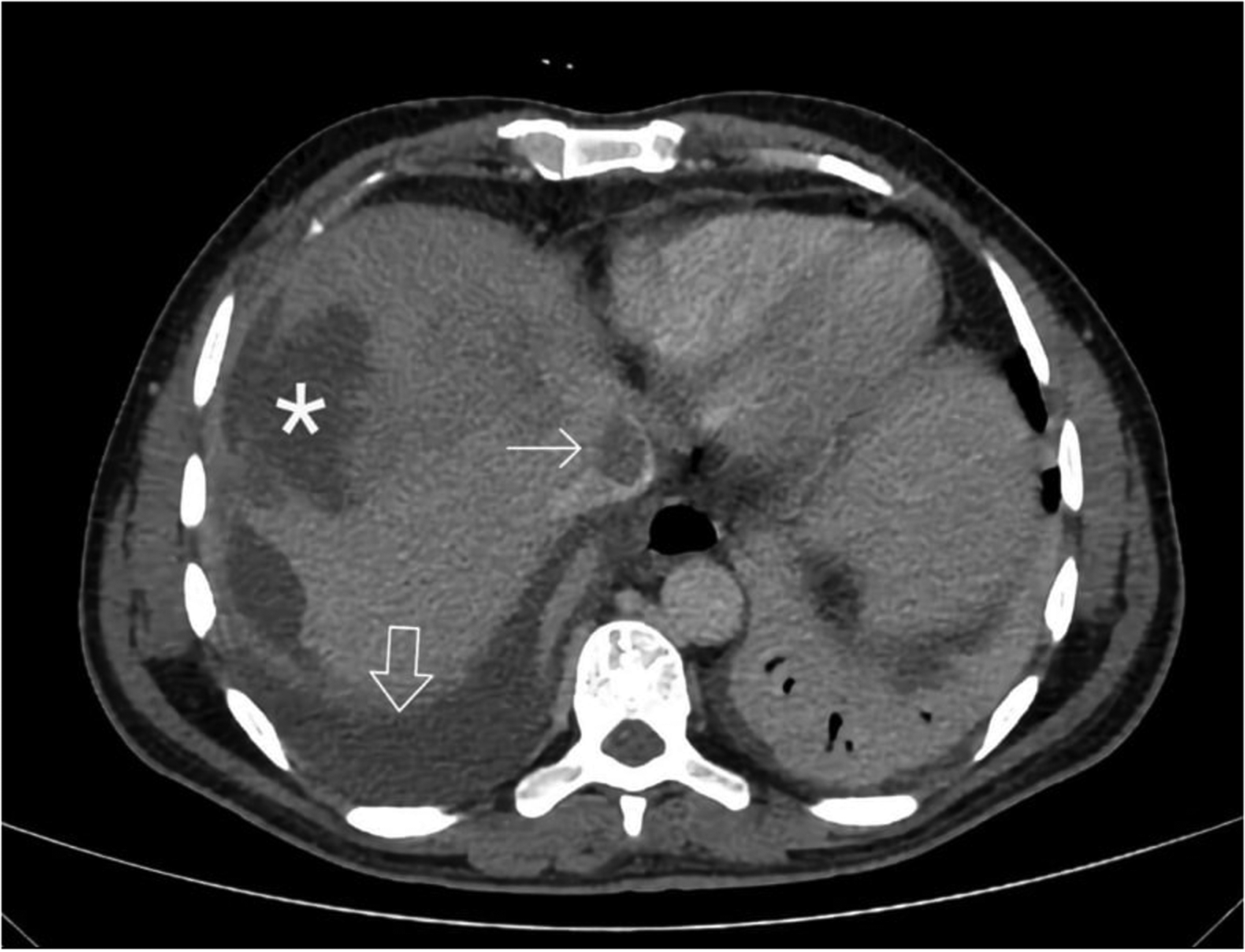
CT scan axial image of patient showing ruptured liver abscess (asterisk) with ascites (bold arrow) and IVC thrombus seen as a hypo dense filling defect with in hyper dense contrast surrounding the thrombus (thin arrow).
Abscess rupture occurred in 37.5%, most commonly into the peritoneal space, followed by pleural rupture. 28% had a pleural effusion, 58.3% of which being transudative. Ascites was noted in 18, 9 of whom were rupture-related, 4 were reactive and the remaining 4 had a high serum ascites-albumin gradient (SAAG) suggestive of portal hypertension. One had low SAAG low protein ascites. Other complications seen are noted in decreasing order of prevalence (Table 1).
Complications of liver abscess.
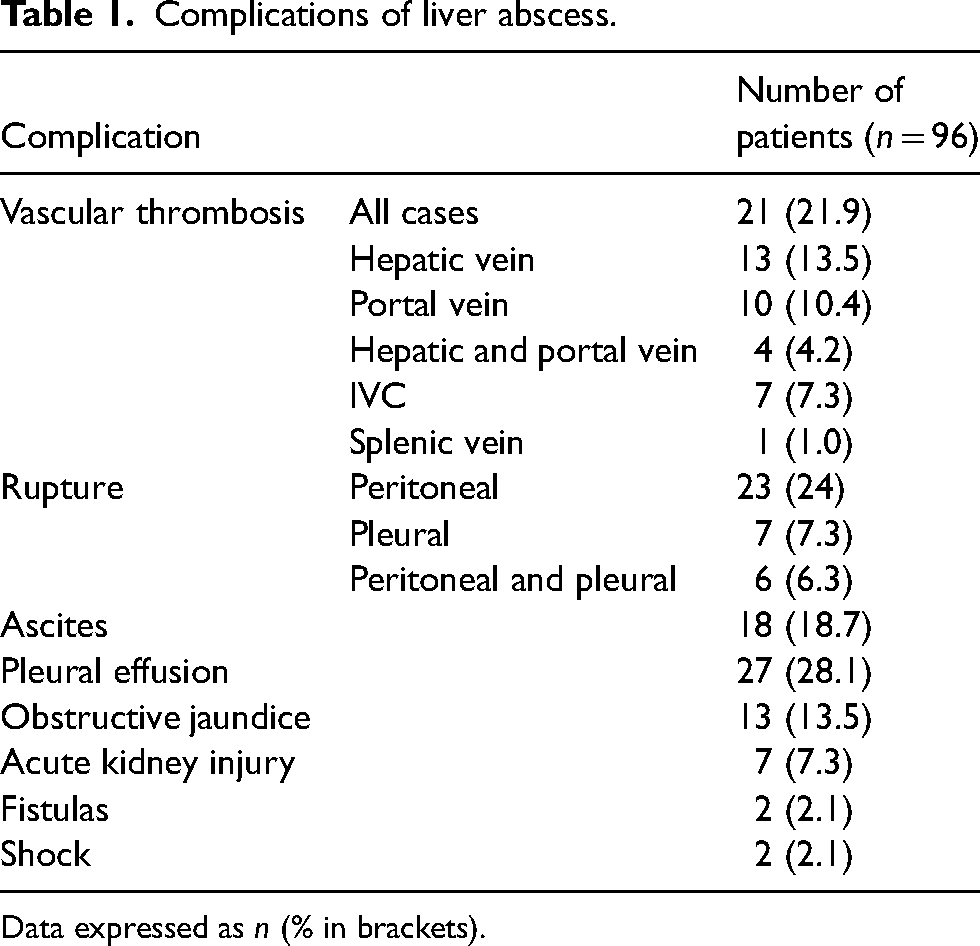
Data expressed as n (% in brackets).
The mean duration of hospital stay was 8.2 ± 7.5 days. Some 55.2% underwent pigtail drainage and 27.1% underwent single-time aspiration. Three patients needed surgical intervention, one of whom died. A higher percentage (71.4%) with vascular thrombosis required pigtail insertion as compared to those without (50.6%) and the difference was statistically significant. At 3 months, LA showed complete resolution in 56.3% while in 35.4% abscesses decreased by less than half the previous size; 7 needed readmission. Of the 20 patients with thrombus who were discharged, LA was reduced in size by >50% in 10 patients, and completely resolved in 40%. There was no mortality in the following 3 months of discharge (Table 2). Thrombus resolution was noted in 11 out of 21.
Association of outcome at discharge and 3 months.
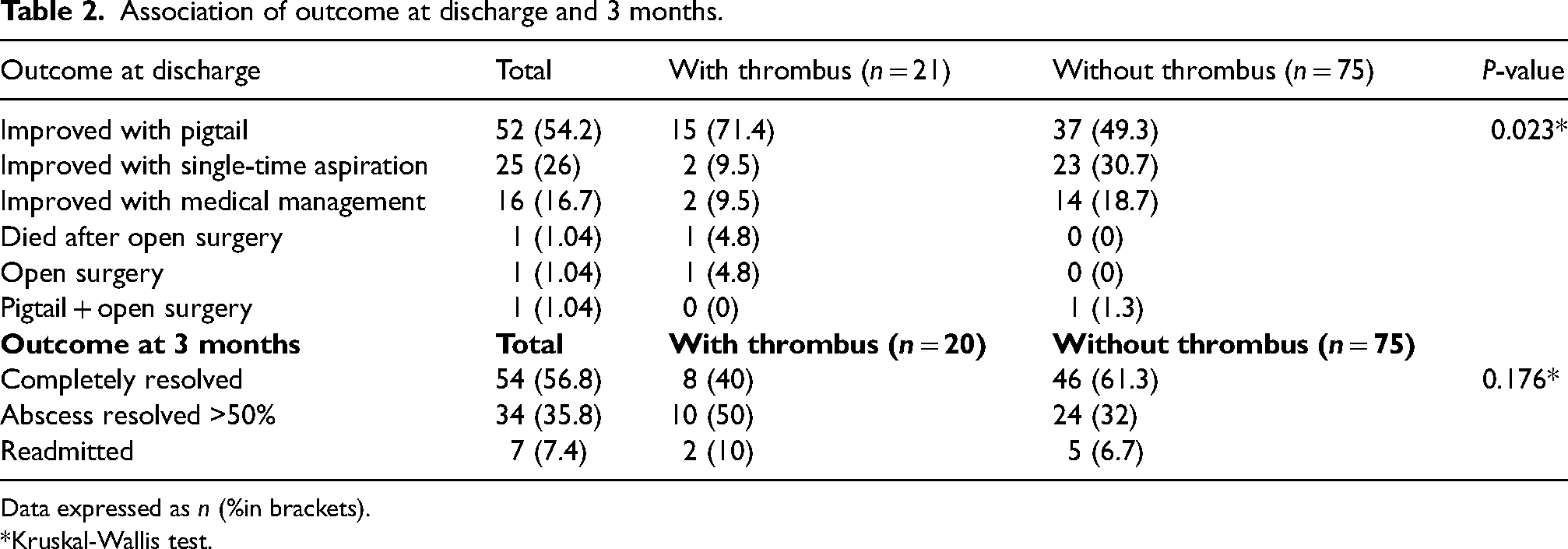
Data expressed as n (%in brackets).
*Kruskal-Wallis test.
Age, symptoms, comorbidity, LA characteristics and complications had no bearing on the outcome in patients with or without thrombus. However, the mean LA dimensions were larger in those with thrombus and the difference from those without was statistically significant.
Discussion
Septic portal thrombophlebitis in a case of LA was first described by Waller in 1846. 5 The majority of reports on HV and PV thrombosis are from autopsy studies; thrombosis was found involving HV in 29.5%, PV in 27.5% and IVC in 4%. 6 Thrombophilic factors and local factors such as appendicitis, diverticulitis, inflammatory bowel diseases and cholecystitis were identified in ∼60% and 40% of patients, respectively. 7 Such thrombotic complications could arise through mechanical compression of vessels or a result of thrombogenic foci induced by the inflammation and sepsis,8,9 or in amoebiasis through activation of the complement coagulation system. 10
In our study, thrombotic complications were detected by CT in 21.9%; this prevalence is variably reported, from 41.8% to only 4.2%.3,11
Abdominal pain and jaundice are predominant symptoms noted in patients with these complications. 11 Obstruction of hepatic vein or IVC blood flow may rarely produce the Budd-Chiari syndrome or pulmonary embolism (PE).12,13
Abscess rupture was seen in 37.5%, followed by pleural effusion in 28.1%. An increased frequency of LA rupture was noted in the thrombosis group. This finding was similar to other studies. 14
Medical management of all patients was with antimicrobials including metronidazole at a dose of 800 mg tds for 14 days as well as cephalosporins or fluoroquinolones, followed by a course of diloxanide furoate as a luminal amoebicide.
Regarding the management of thrombotic complications, there exists no standardised protocol. Most reports or series in which anticoagulation or thrombolysis was used involved pulmonary arteries, the vena cava or the right side of the heart.1,15 We used three months of anticoagulation where caval thrombus was present owing to the risk of PE.
Prior to 1945, there was a 100% mortality noted in cases of LA with thrombus. 5 In our series, the presence of vascular thrombosis per se did not modify the case fatality rate. 11 Vascular thrombosis also did not influence the post-discharge outcomes at 3 months.
Limitations
This was a single-centre, tertiary hospital-based study, thus, it may overestimate the complications associated with LA. In addition, it was not feasible to perform the full coagulation workup for the patients presenting with thrombotic complications and it was assumed that the thrombosis may be a result of local mechanical factors and infection-inflammation-induced coagulation cascade. Due to logistical constraints, it was not possible to perform a repeat CT scan at 3 months to identify resolution of the vascular thrombosis.
Footnotes
Author Contributions
Rayidi Rajesh and Monica Gupta: concept, design, intellectual content, literature search, data acquisition, manuscript preparation, editing and review. Sarabmeet Singh Lehl and Narinder Kaur: concept, data acquisition, manuscript preparation, editing and review. Anita Tahlan and Daljinderjit Kaur: data acquisition, manuscript editing and review. All the authors have made substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data. All the authors have been involved in drafting the manuscript or revising it critically for important intellectual content and have given final approval of the version to be published. Each author has participated sufficiently in the work to take public responsibility for appropriate portions of the content. The corresponding author takes responsibility for the article during the submission and review process.
Consent to participate
The participants, who gave written informed consent after explaining the study and objectives, were included in this study. All of the participants were assured that confidentiality of their personal data would be maintained.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by institutional ethics committee vide letter no. GMC/IEC/2020/570R/156 dated 08.04.2021.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.