
Abstract
A significant group of children suffer from non-specific functional abdominal pain. We argue that the prevalence of coeliac disease is higher in this group than the general population; thus, screening in this group is justified.
Introduction
Functional abdominal pain is common in children and adolescents, affecting up to 19% of children worldwide, contributing to 2%–4% of consultations in all general paediatric practices and >50% of consultations in paediatric gastroenterology. 1 According to the Rome IV criteria, this group comprises irritable bowel syndrome (IBS), functional dyspepsia (FD), abdominal migraine (AM), and functional abdominal pain, not otherwise specified (FAP-NOS). 2 There are no specific diagnostic criteria for distinguishing functional from organic abdominal pain. Investigations are generally not recommended in the absence of red flags, such as failure to thrive, deceleration of linear growth velocity, significant vomiting, chronic diarrhoea, evidence of gastrointestinal blood loss, persistent right upper or lower quadrant pain, unexplained fever, family history of inflammatory bowel disease, or abnormal or unexplained physical findings. 3
Chronic abdominal pain is also a frequent non-diarrhoeal manifestation of coeliac disease (CD). However, it remains underdiagnosed because of a low index of suspicion in the absence of alarm symptoms. Therefore, such patients are at risk of serious complications including impaired nutrition and growth, poor quality of life, long-term autoimmune stimulation, absenteeism from school, unnecessary investigations, and multiple hospital visits4–8. There is insufficient evidence concerning any increased prevalence and thus need for routine CD screening in children with FAP-NOS. 9 Routine exclusion of CD in such children is not yet recommended officially. 3
Methods
Our cross-sectional study was conducted in the paediatric department of a tertiary care hospital in North India over 18 months in 2019–2020. We included children between the ages of two and twelve years with FAP-NOS according to Rome IV criteria, defined as episodic or continuous abdominal pain at least four times per month for at least two months not occurring solely during physiological events and after appropriate evaluation, which could not be fully explained by another medical condition, and with insufficient criteria for IBS, FD, or AM. 2 Children with severe acute malnutrition, chronic diarrhoea, functional constipation, Down's syndrome, chronic diseases (e.g. cardiac, renal, hepatic), neurological disability, known CD or first-degree relatives with CD, family history of inflammatory bowel disease, haematochezia, dysphagia, chronic vomiting, or weight loss were excluded from the study. A detailed past and present history was obtained from the children and their carers. General physical examination and nutritional status were assessed at the time of enrolment.
Written informed consent was obtained from parents or legal guardians as applicable.
We screened for CD using tTG-IgA antibody by recombinant tissue transglutaminase IgA ELISA Kit. Values ≥22 U/mL were considered positive according to the manufacturer, and levels between 18 and 22 U/mL equivocal, and levels <18 U/mL negative.
All children who screened positive for CD, underwent an upper gastrointestinal endoscopy using a flexible endoscope (GIF-H170; Olympus, Japan) and duodenal biopsy. Four biopsy specimens were obtained from the second part of the duodenum and two from the first part of the duodenum for every patient. The samples were oriented on adhesive filter paper, fixed in 10% formalin buffer, and paraffin-embedded. Histopathological examination of duodenal biopsies was performed by a specialist blinded to the clinical history and serological tests. Results were graded using the Marsh–Oberhuber grading system. 10 The final diagnosis of CD was based on positive serology and small-bowel histopathology (Marsh grade 2 or 3). Histopathology showing Marsh grade 1 mucosal injury with positive anti-tTG antibody was labelled potential CD. 4
To assess for any clinical pointer to suspect CD in subjects with FAP-NOS, we compared the age of onset of abdominal pain, duration of abdominal pain, nutritional status (e.g. ferritin, B12, folate, vitamin D, serum calcium, and albumin), and biochemical markers (e.g. liver function tests and haemoglobin) between children with CD and children without.
A sample size of 150 children fulfilling the Rome IV criteria for FAP-NOS was recruited. The statistical software SPSS 17 for Windows (Chicago, IL, USA) was used for the statistical analysis. Descriptive data were presented as frequencies and percentages. Quantitative data were presented as mean and standard deviation. Qualitative data were analyzed using the chi-square test, and quantitative data were analyzed using the independent t-test. Our study was approved by the institution's ethics committee.
Results
We evaluated 150 children with a mean age of 81.8 ± 33.6 months, of whom 84 (56%) were male. The mean duration of abdominal pain was 11 ± 17.8 months, and its most common site was peri-umbilical (72.9%), followed by epigastric (20.3%), lower abdominal (3.4%), and diffuse (3.4%).
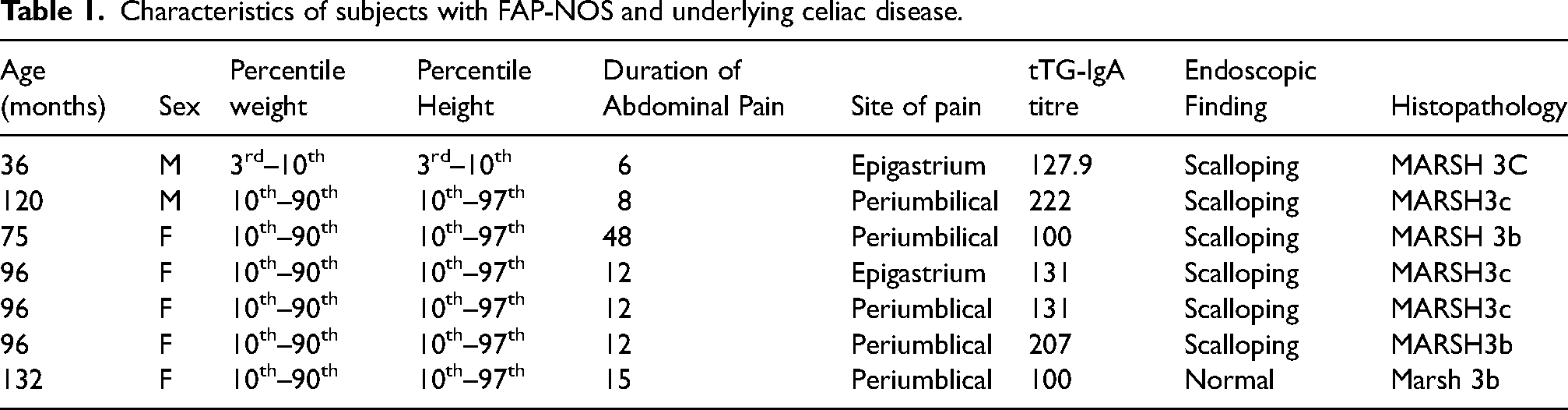
All participants were tested for tTG IgA antibody, of whom 39 (26%) had positive serology. Depending on the histological features of the duodenal mucosa, seven patients had biopsy-proven CD (Table 1). We observed a 4.7% prevalence of biopsy-proven CD and a 21% prevalence of potential CD in children with FAP-NOS.
Characteristics of subjects with FAP-NOS and underlying celiac disease.
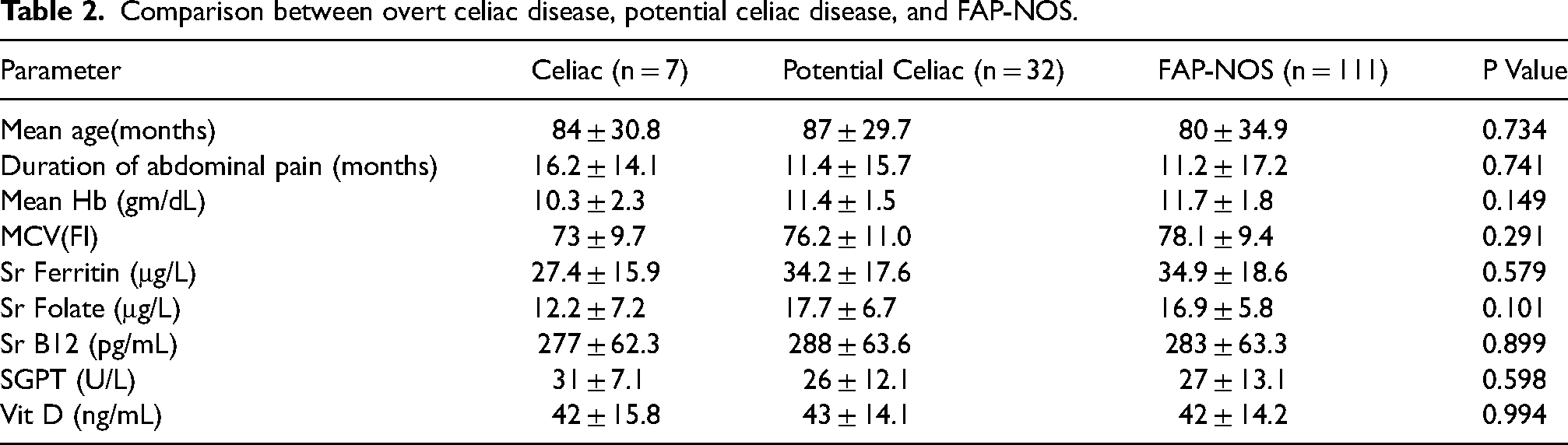
Comparing children with FAP-NOS related to CD and children with FAP-NOS not related to CD (matched for age and sex) revealed no statistical difference in age of onset of abdominal pain, duration of abdominal pain, nutritional status (e.g. ferritin, folate, B12, vitamin D, serum calcium, and albumin), or biochemical markers (e.g. liver function tests and haemoglobin). However, the duration of abdominal pain was longer in CD subjects, as well as lower mean haemoglobin, serum ferritin, serum folate, and serum B12 levels compared to children with only FAP-NOS (Table 2).
Comparison between overt celiac disease, potential celiac disease, and FAP-NOS.
Discussion
Our cross-sectional study showed a significant association between tTG-IgA antibody positivity and FAP-NOS. This was significantly higher (c. twelvefold) than in the general paediatric population. 11 Likewise, CD was diagnosed in 4.7% (7/150), a rate fourfold higher than that in the general paediatric population in North India.11,12 These findings highlight that in children with FAP-NOS without alarm symptoms, a CD diagnosis may be missed or delayed if no active screening is carried out, negatively affecting the quality of life of these children and their families.
A prevalence rate of CD among 110 children with recurrent abdominal pain but no alarm signs was also higher, 13 and likewise with IBS. 14 However, some dispute these figures.5,15,16
The most important finding in our study was that 4.7% of children with FAP-NOS without any associated symptoms or red flag signs had undiagnosed underlying CD and 21% had potential CD. CD screening was not carried out in these patients because there were no associated alarm symptoms. In CD, abdominal pain is a common symptom that can be the only manifestation of the disease without any other symptoms. 17
A limitation in our study is that it was carried out in an area with a high burden of helminthic infestation, even mass deworming programmes with albendazole twice a yearly to children aged 1–19 years. Moreover, IgA levels were not measured, so some cases may have been missed because an IgA-based serological screening test was used; the actual prevalence of CD may be even higher.
Conclusion
The bottom line is that the duration of abdominal pain for six months or more should be considered a clinical predictor to screen for CD. This may actually have an optimal cost-benefit ratio and prevent other fruitless hospital visits.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.