
Abstract
Outcomes of arthroplasty in sub-Saharan Africa are not widely reported. To our knowledge, this systematic review is the first to explore this topic. Scopus, EMBASE, Medline and PubMed databases were searched, utilising MeSH headings and Boolean search strategies. All papers from South Africa were excluded. Twelve papers reporting 606 total hip replacements (THRs) and 763 total knee replacements (TKRs) were included. Avascular necrosis was the most common indication for THR, whereas osteoarthritis was the main indication for TKR. HIV prevalence of up to 33% was seen. Improvements were seen in patient-reported outcome measures in both THR and TKR. The dislocation rate in THR was 1.6%. The deep infection rate was 1.6% for TKRs and 0.5% for THRs. Positive results were reported, with comparable complications to high-income countries. However, there is likely to be significant reporting bias and the introduction of mandatory registries would enable more accurate monitoring across the region.
Introduction
There are many patients in sub-Saharan Africa (SSA) suffering from conditions that may benefit from total joint replacement (TJR). However, these countries commonly do not have adequate resources to offer this service to all eligible patients. 1 TJR of the hip and knee is performed frequently in high-income countries and evidence supports that these procedures are cost-effective. 2
Little is known about the outcomes or the number of TJRs performed in SSA. The age of patients and their indications for TJR differ considerably from those in the developed world and include a larger proportion of patients living with HIV.3,4 Facilities, resources and training of surgeons and allied health professionals are substantially different from those of a high-income country. 5 It cannot be assumed that outcomes as seen on TJR registries, such as the UK National Joint Registry, will directly transpose to SSA. 4
The cost of TJR is significant; costs in the USA are in the range of US$16,000–60,000 for the procedure alone, depending on the institution. 6 In the UK National Health Service, where prices are dictated more by true cost than profit, total knee replacements (TKR) and total hip replacements (THR) are thought to cost approximately US$7000–9000 per procedure. 7
There are currently no systematic reviews in the literature investigating the outcomes of TJR in SSA. This review explores the literature surrounding outcomes of THR and TKR in SSA, including patient-reported outcome measures, evidence of complications, length of inpatient stay, inpatient mortality and revision rates.
Methods
Inclusion and exclusion criteria.

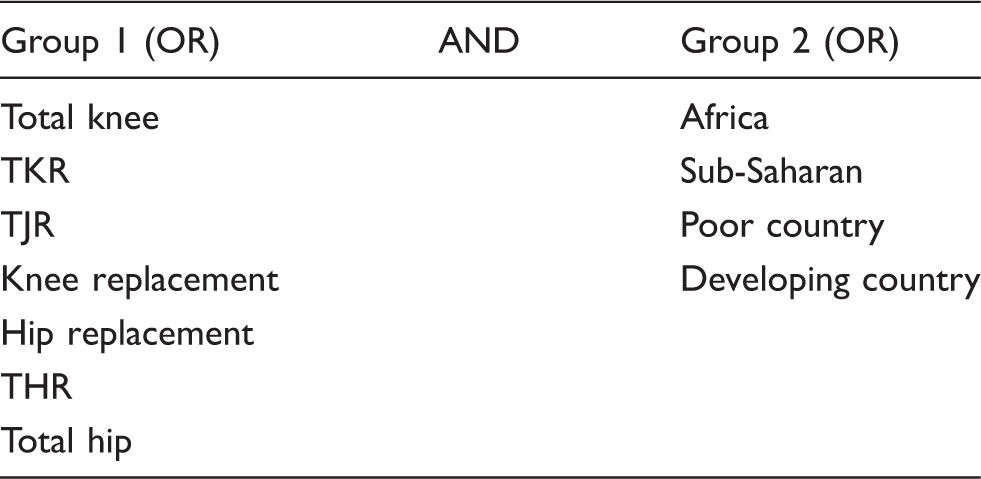
Medical subject headings (MeSH) were combined using a Boolean strategy, using synonyms, alternate spellings and abbreviations, and are listed in Table 2. Eligible studies were backwards referenced to improve the search. Where papers were identified to duplicate reporting of earlier work, they were included with explanations provided.5,10–12 The final search was undertaken on 4 November 2018. The preferred reporting items for systematic reviews and meta-analyses (PRISMA) process was followed (Figure 1).
PRISMA diagram. MeSH headings.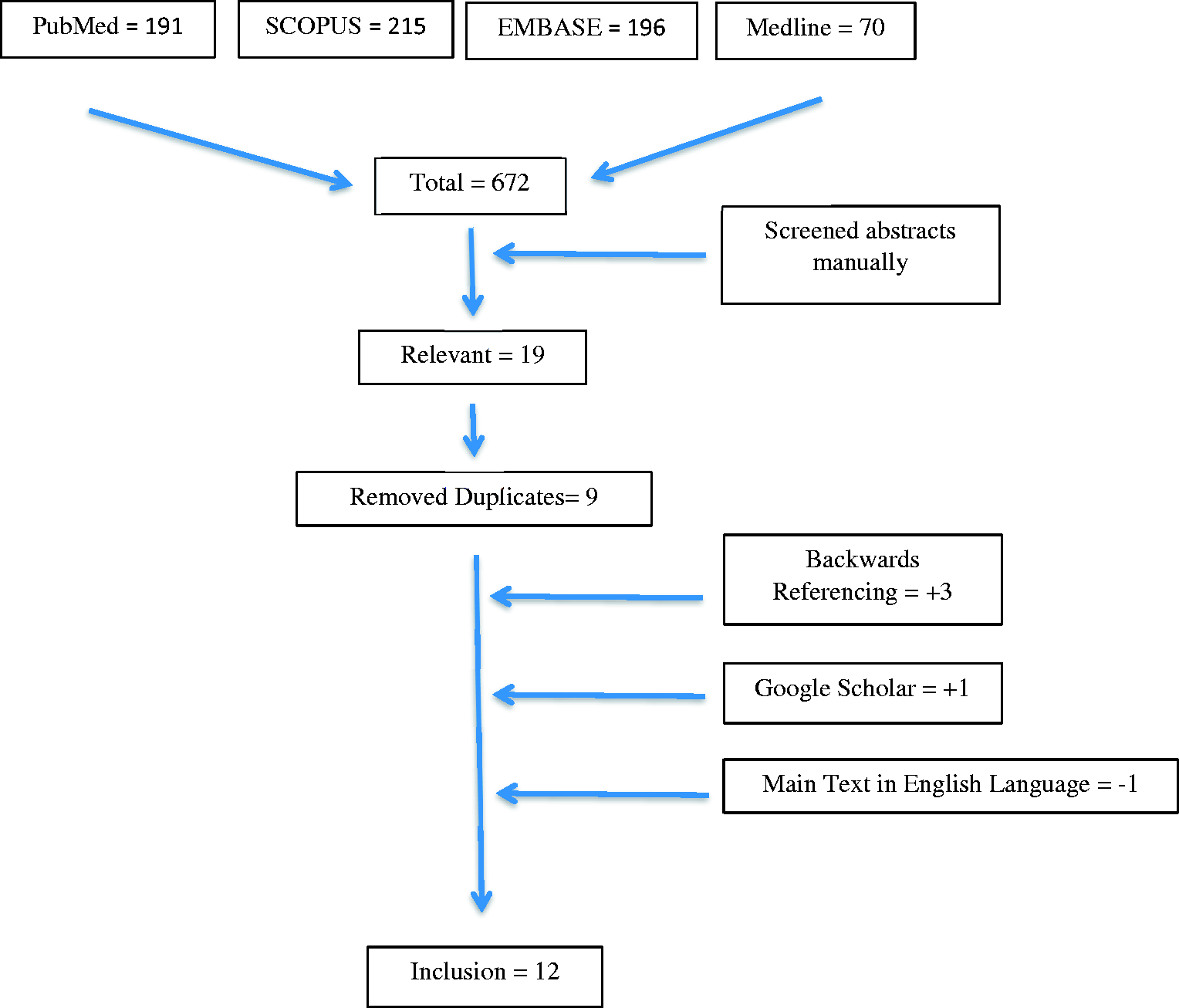
Results
Studies of arthroplasty in sub-Saharan Africa.
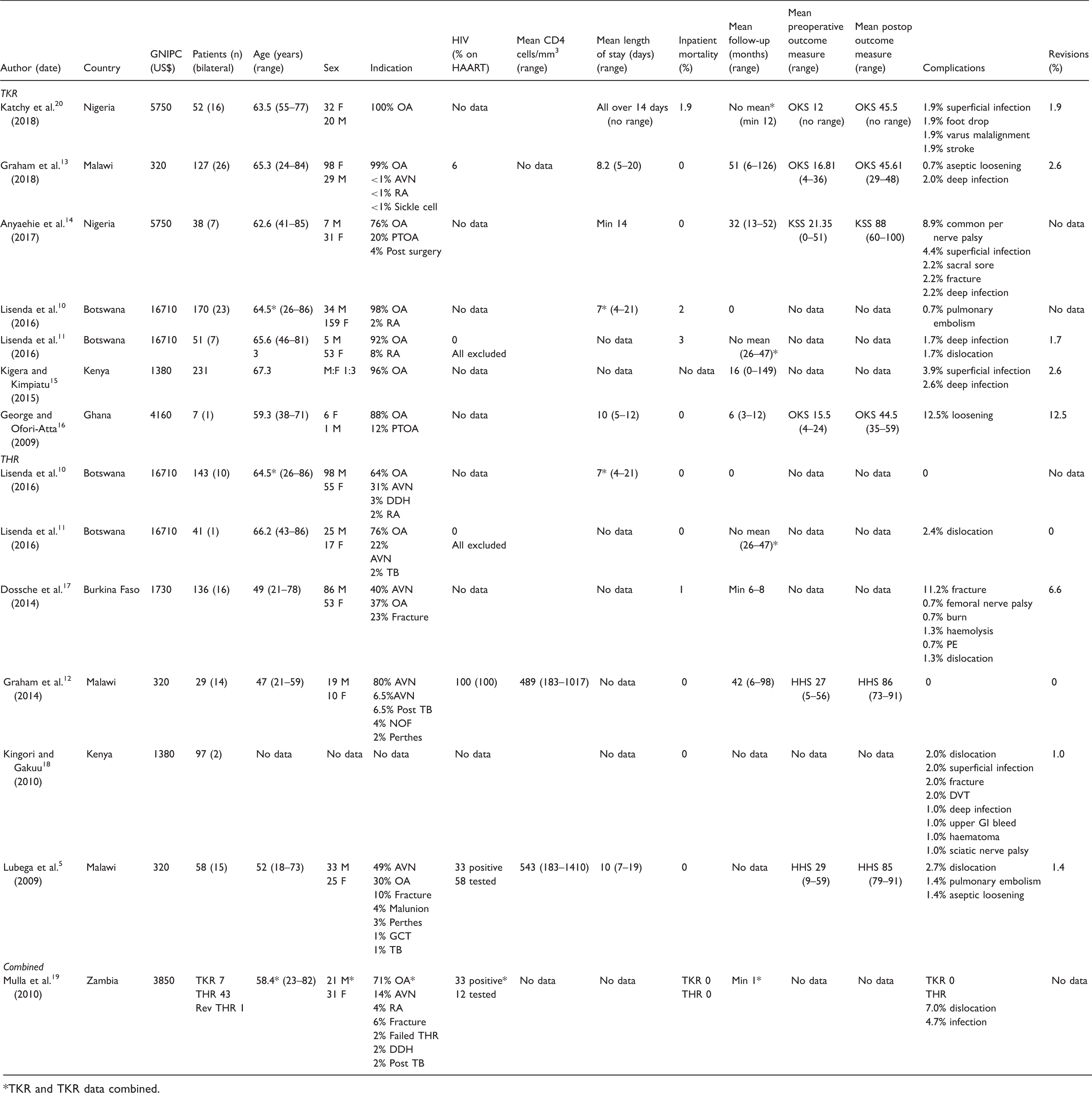
TKR and TKR data combined.
Patient demographics
The median number of patients included in each paper was 58 (range = 8–313 patients). Patient demographics are included in Table 3 for each paper individually.
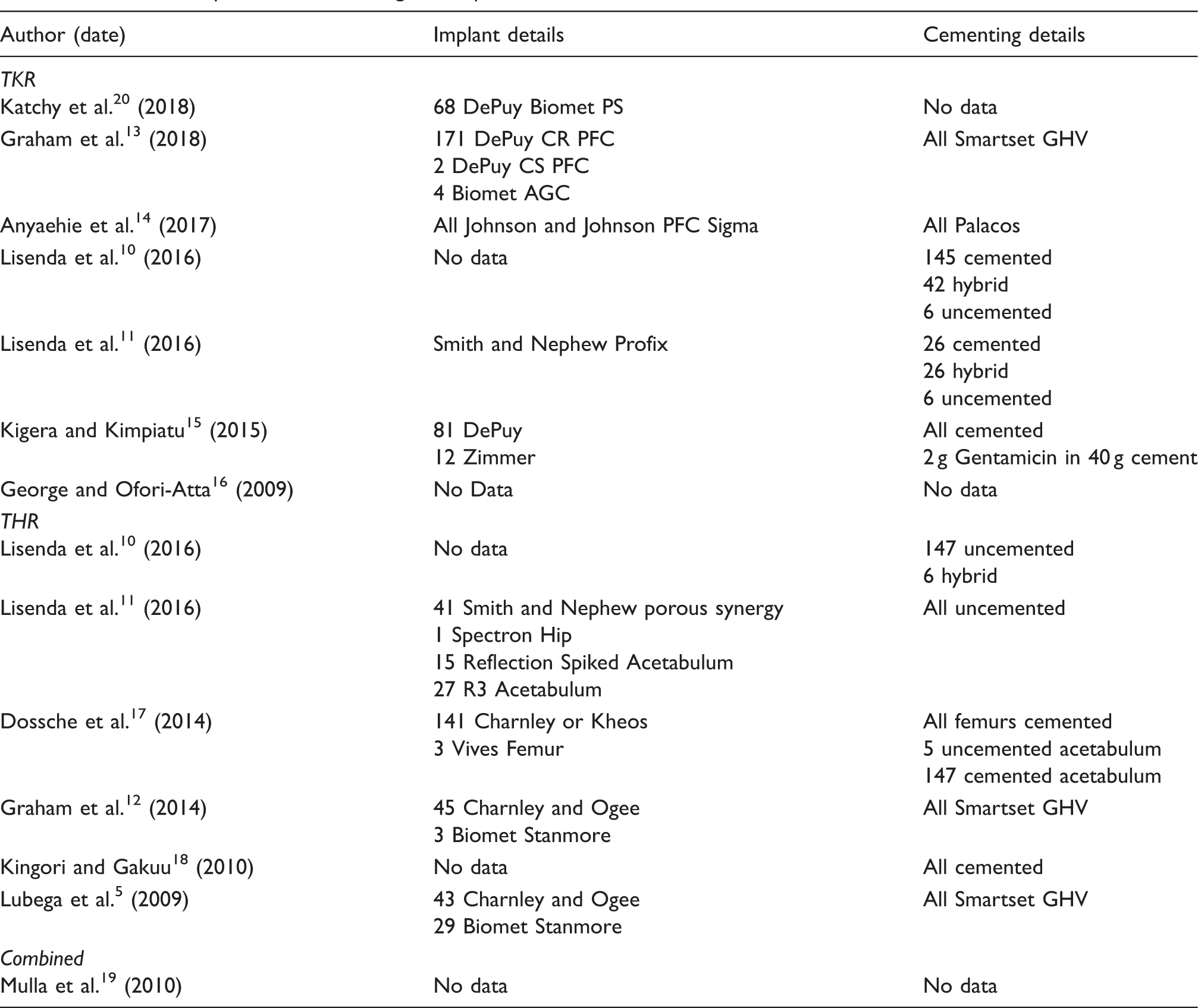
Surgical methods
Details of implants and cementing techniques used.
HIV-positive patients
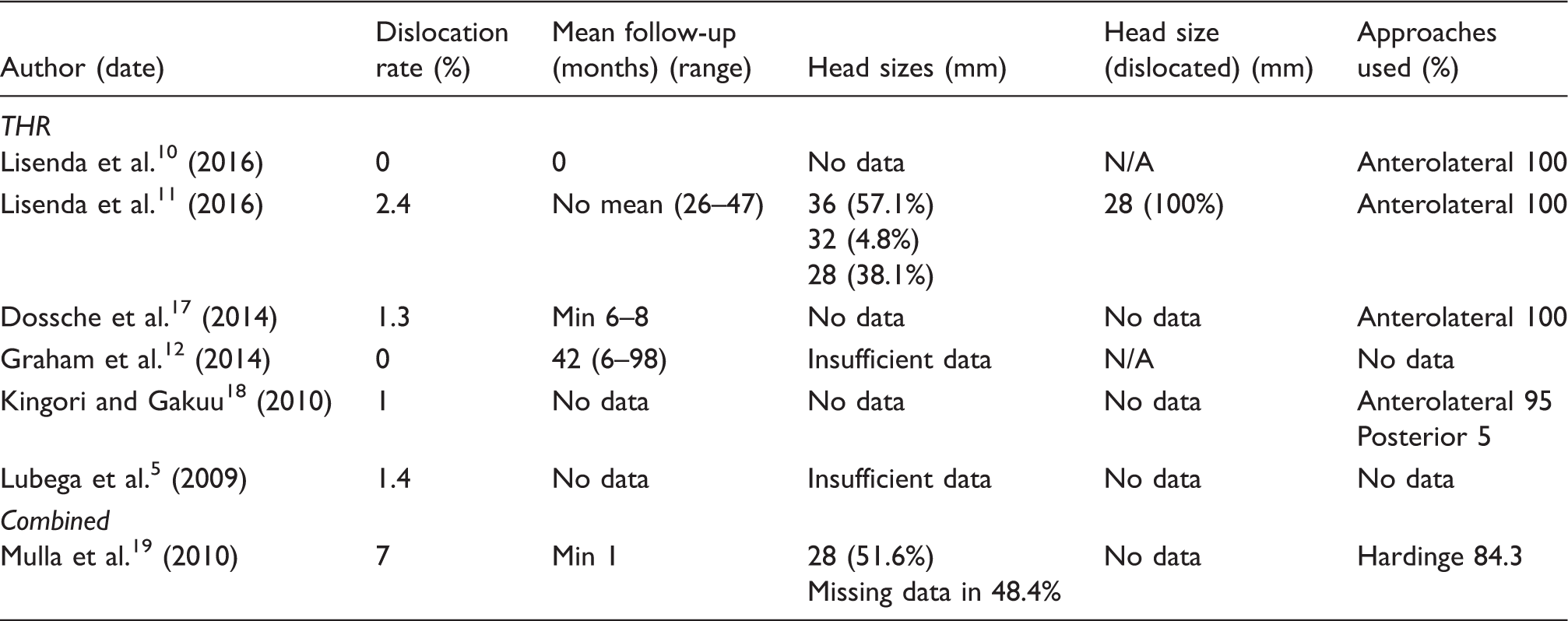
Graham et al. reported on a cohort of patients with HIV undergoing THR, with excellent results. No complications were seen at a mean follow-up of 42 months. 12 A second paper by Graham et al. reported no complications in the nine HIV-positive patients undergoing TKR. 13 Data on HIV status were otherwise poorly reported. Lisenda et al. excluded all HIV-positive patients; 11 Lubega et al. tested 42 of 58 patients undergoing THR and found one-third were HIV-positive; and Mulla et al. tested only 12% of patients and found a similar prevalence.5,19 No further papers reported on HIV status and no studies were designed to compare outcomes of patients living with HIV to healthy controls.
Outcomes
Detailed outcomes are displayed in Table 3. Length of inpatient stay was reported in six papers and mean values were in the range of 7–14 days.5,10,13,14,16,20 No information was provided in other papers. Inpatient mortality was well reported, with only one paper not specifically stating a value. 15 The overall rate in TKR was 0.9%,10,11,13,14,16,20 while in THR it was 0.2%.5,10–12,17,18
Patients were followed up for various times (mean = 18 months; range = 0–149 months).10,12–16 Incomplete data regarding follow-up were provided in four papers.11,17,19,20 No data were provided in two papers.5,18
Head sizes and approaches used in THRs.
Discussion
To the authors’ knowledge, this is the first systematic review of TJR in SSA and there are many differences between the environment, patient cohort and healthcare provisions when performing TJR in SSA, compared to high-income countries.
Model of healthcare in sub-Saharan Africa
Healthcare may be provided ‘free at the point of use’ and funded through taxation or through health insurance or self-payment. 21 Most high-income countries have a coexisting healthcare model where healthcare insurance is available to those who can afford it, with a state-run safety net for those who cannot. Examples of both types of healthcare are found in SSA, but each comes with its own limitations in these populations. Nigeria, for example, has historically had no healthcare insurer. 14 Different countries within SSA have hugely variable economic circumstances, as demonstrated in Table 3. 22 The gross national income per capita is US$16,710 in Botswana but only US$320 in Malawi. 22 Average government spending on healthcare across SSA has been reported as US$90 (range = US$14–663) per year per person, which compares to a typical value of >US$5200 in high-income countries.23,24
Several institutes in SSA work in collaboration with experienced high-volume TJR surgeons from high-income countries, who visit them temporarily to perform surgery.10,11,17 This has the benefit of training locally based surgeons to become independent arthroplasty surgeons in areas where this training is otherwise not available. However, one of the main drawbacks of using visiting surgeons is continuity of care and that these surgeons are unlikely to be available to follow up the patient if they develop a complication requiring further surgery.
From our experience, we believe the best provision of any arthroplasty service is by a local multidisciplinary arthroplasty team. This team can benefit from input from international support if the appropriate training and experience is not initially established but should aim to become self-governing. An example of this approach is the Malawi National Joint Registry.5,12,13
Differences in patient demographics in sub-Saharan Africa
In SSA, the adult prevalence of HIV in 2013 was approximately 4.7%, compared with 0.3% in Europe and North America. 3 Within SSA, prevalence estimates also vary between countries; for example, in 2013 the estimates for Malawi and Botswana were 21.9% and 10.3%, respectively. 3 Only five of our papers documented HIV status.5,11–13,19 Graham et al. demonstrated no increased risk of complications in HIV-positive patients undergoing THR, including infection. 12 However, no other papers reported outcomes related to HIV-positive patients undergoing TJR.
In patients from SSA, avascular necrosis was a frequent indication for THR and has previously been associated with HIV infection. 25 Lubega et al. found 49% of patients in their study had avascular necrosis and, of these, 44% had HIV. 5 Mulla et al. did not find such a high rate of avascular necrosis (14%) but acknowledged they did not have magnetic resonance imaging facilities and may have attributed painful hips to osteoarthritis without further consideration. 19 Patients were younger than those seen with osteoarthritis in high-income countries, which may indicate an increased prevalence of avascular necrosis than that which was reported. Mulla et al. found a higher rate of dislocation at 3.9% and suggested several cultural reasons. 19 Patients often use squat toilets and kneel for prayer, requiring deep hip flexion, which contradicts routine THR precautions. Patients may also be manual workers, e.g. farmers, and need to work as soon as possible after their surgery, owing to minimal social support. Patients’ occupations were not reported in any study, so conclusions may not be drawn.
Outcomes of surgery in sub-Saharan Africa
Use of laminar flow is rare in SSA but has been standard for TJR in high-income countries since it was introduced by Sir John Charnley in the 1970s. 26 However, its necessity has recently been questioned. 27 An underlying diagnosis of avascular necrosis has previously been linked to increased risk of infection, 90-day mortality, readmission and revision, in some studies.28,29 Overall infection rates in SSA appeared satisfactory, as demonstrated in Table 3.
The observed improvement in mean OKS was a greater increase than typically seen in high-income countries. 16 The 2013 report of the UK National Joint Registry presented an average increase from 19 to 26. 30 An improvement in mean KSS was reported and data from a high-income county have shown smaller improvements in KSS from 53 to 80.14,31 Allowing for some natural decline in function with 3–6 years of extra follow-up in the high-income group, these data are still likely to represent a similar if not superior improvement in function in the SSA paper. 14 Improvements in HHS from 29 to 85 were noted. 5 This compares with data from a high-income country, showing improvement from 43 to 87. 32 Again, inferior preoperative scores were noted in SSA, indicating that patients are more likely to have advanced disease and may stand to benefit more from TJR than patients in high-income countries, who are likely to present earlier for treatment.
Joint registries in sub-Saharan Africa
Malawi is the only country in SSA to have a dedicated national joint registry.5,12,13 The majority of the data from SSA was collected using local prospective databases.10,11,14,16,17,19 Reported study size varied but was generally small. This compares with the most recent report on the UK National Joint Registry, which included 2.35 million records. 4 The first country to develop a national orthopaedic registry to determine outcomes of TJR was Sweden in 1975. 33 Since then, many high-income countries have developed similar programmes. The benefits of national registries are many and include eliminating reporting bias, allowing comparison between units, and early identification of problem implants and techniques.
Follow-up
There are several limitations to the follow-up process in SSA. Patients may have to travel large distances to attend follow-up, with significant time or cost investment to do so. In a study from Kenya, Kingori and Gakuu found 34% loss to follow-up at six months. 18 However, with investment in a dedicated TJR follow-up clinic and dedicated nurse, as well as provision of outreach clinics, Lisenda et al. were able to maintain 100% follow-up. 11 Improvement in follow-up is likely with increasing access to mobile phones and reminders through this method have been shown to work well in antiretroviral therapy programmes. 34
Limitations
There is likely to be a profound reporting bias in studies from SSA with only those centres with good results publishing their outcomes. Centres with poor results would probably choose not to do so. The only way to avoid this is to introduce mandatory national registries that would eliminate this bias. This would also increase the number of patients reported on and thus give more reliable data.
Two papers duplicated follow-up of earlier papers.10,12 Graham et al. reported from the same database as the previous Lubega et al. paper but specifically looked only at patients with HIV and therefore it was useful to include this paper.5,12 Lisenda et al. published two papers, one of which looked only at the inpatient period of care.10,11 This included a larger cohort of patients but is likely to have duplicated some reporting. It was impossible to identify the significance of this from the manuscripts.
The overall outcomes of TJR surgery in SSA are positive; however, it must be noted that the patient population reported on, of predominantly self-paying patients, is likely to be healthy, well-nourished and well supported socially. Surgery is also likely to be performed in private well-funded hospitals. The included studies are not likely to represent results of the general population undergoing surgery in government hospitals. If it were financially possible to extend TJR across all population groups, it may be found that complication rates and outcomes vary. Implementation of mandatory national registries would ensure transparency of outcomes and allow appropriate targeting of resources and training.
This research only included studies that were published in the English language and as a result, relevant studies published in other languages are likely to have been missed.
Conclusions
Overall, positive results were reported from TJRs in SSA, with comparable rates of complications to those reported in high-income countries. However, there is likely to be significant reporting bias, and the introduction of national and regional joint registries would have the benefit of allowing more accurate monitoring of outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.