
Abstract
The 21st century has seen tourists from various source markets significantly impacted by non-communicable diseases, including mental disorders. Yet, research and practice frequently overlook tourists with mental disorders. Building on Buckley’s discussion in the Journal of Travel Research about tourism and mental health, this study examines the travel eligibility of tourists diagnosed with four prevalent mental disorders: major depressive disorder (MDD), generalized anxiety disorder (GAD), schizophrenia, and dementia. We present preliminary recommendations for accommodating these tourists and highlight the urgent need for collaborative efforts between stakeholders in tourism, hospitality, and medicine.
Keywords
Introduction
Over one billion people, constituting 13% of the global population, grapple with mental disorders, defined by the World Health Organization as “clinically significant disturbances in cognition, emotional regulation, or behavior” (World Health Organization [WHO], 2022). 1 Contributory factors include rapid population aging and social stressors, driving an escalation in these conditions (Ardelean & Redolat, 2023; Chun et al., 2023; Morrison et al., 2022).
Astoundingly, mental disorders could drain up to $16 trillion from the global economy by 2030, underscoring their significant health implications (Patel et al., 2018). Yet, in 2020, mental health initiatives received a mere 2% of global health investment (WHO, 2021a). Despite this, individuals with mental disorders, who often confront stigma and social exclusion (Lim & Bowman, 2023b; Mabire, Bouaziz et al., 2022), continue to represent a vital segment of the tourism and hospitality industry (Hu, Wen, Zheng, & Wang, 2023).
The intersection of tourism, hospitality, and mental health remains an underexplored area in academic research. Although scholars have occasionally addressed this topic, the majority of studies are limited in scope. Specific studies have delved into the experiences of tourists with conditions like autism (Jepson et al., 2023; Sedgley et al., 2017; Zhao et al., 2023), depression (Christou & Simillidou, 2020; Filep & Bereded-Samuel, 2012; Levi et al., 2019), dementia (Connell & Page, 2019a; Connell et al., 2017; Connell & Page, 2019, 2019b; Innes et al., 2016; Page et al., 2015; Tomej et al., 2023; Wen, Zheng, Hou, et al., 2022), intellectual disability (Ali et al., 2023; Gillovic et al., 2021), and post-traumatic stress disorder (Yu et al., 2021). Most of this research adopts an exploratory and humanistic approach. Key findings have revolved around travel experiences of these vulnerable populations and their caregivers (e.g., family members), the creation of inclusive tourist destinations, and the potential health benefits of travel (Gillovic et al., 2021; Hu, Wen, Phau, et al., 2023; Page et al., 2015; Wen, Zheng, Hou, et al., 2022). However, there is a notable lack of empirical evidence. Many of these studies are conceptually focused, and the few that are empirical often show methodological shortcomings such as unclear disorder definitions, ambiguous participant criteria, and overlooked ethical considerations. Such flaws could compromise the validity of results and mislead stakeholders (Ali et al., 2023; Levi et al., 2019).
Undoubtedly, patient-centered studies in the domain of tourism and hospitality present unique challenges. Among these is the imperative to obtain ethical approval, especially when the research involves vulnerable populations like those with mental disorders. While much of the existing work in this field has occasionally sidestepped ethical considerations (Frechtling, 2018), such oversight is unacceptable when investigating these groups. Ethical approval is not merely a formality—it is essential for safeguarding participants’ rights and well-being. Recommendations by Zheng et al. (2023) have highlighted detailed solutions to overcome these challenges. They underscored the necessity of meticulous interdisciplinary deliberation and adherence to rigorous methodological guidelines. This includes securing ethical approval, defining clear participant inclusion and exclusion criteria, and adopting clinical research methodologies. Yet, amidst these considerations, a significant gap remains: the challenge of identifying travel-eligible tourists with mental disorders. Addressing this would mark a significant stride forward in the field.
Tourism extends beyond mere leisure and recreation (Wen, Kozak, & Jiang, 2022), serving as a powerful tool for mental recovery (Buckley, 2019; Buckley & Westaway, 2020; Buckley et al., 2021; Cooper & Buckley, 2022). Research indicates tourism’s potential in alleviating depressive symptoms (Levi et al., 2019) and even suggests its role as a non-pharmacological intervention for dementia (Wen, Zheng, & Hu, 2022). Yet, despite its benefits, the question of accessibility remains—not every individual with a mental disorder has the means to travel, mainly due to physical and mental constraints (Huang et al., 2019).
The tourism and hospitality industry’s capacity to accommodate such tourists can lead to significant positive impacts. The very definition of a “tourist” has been a topic of debate (McCabe, 2005), with individuals with mental disorders posing unique challenges.
Buckley (2023) has significantly advanced the dialog between tourism and mental health, introducing an innovative theoretical framework that lays the groundwork for deeper exploration in this domain. By underscoring the imperative for scholars to discern, quantify, appreciate, and promote tourism’s contributions to mental health, Buckley (2023) paves the way for further research intersections.
Heeding Buckley’s (2023) appeal for enriched discourse on the confluence of tourism and mental health, this letter narrows its lens on the specific demographic of individuals with mental disorders. This population, while crucial, remains largely unprobed in terms of its interaction with tourism and its potential therapeutic benefits. Further delving into the terrain marked out by Buckley (2023), we have spotlighted an essential yet unresolved inquiry: pinpointing those among this demographic deemed fit for travel (Zheng et al., 2023). Through this letter, our intent is not just to augment Buckley’s (2023) foundational work but to provide specific, actionable insights concerning travel suitability for those with major mental disorders such as major depressive disorder (MDD), generalized anxiety disorder (GAD), schizophrenia, and dementia. In doing so, we aspire to weave a richer tapestry of understanding around tourism and mental health.
Mental Disorders and Travel Eligibility
Tourists with mental disorders often have unique concerns during travel. Their vulnerability can present more challenges than those faced by general tourists (Felkai & Kurimay, 2017). Specifically, mental disorders can impact physical functioning and self-care, leading to difficulties with mobility and accessibility. Depressive and anxiety disorders, schizophrenia, and dementia rank as the leading causes of disability globally (WHO, 2022). 2 As a result, people with these disorders may find it hard to visit certain destinations or partake in specific activities (Innes et al., 2016).
Mental disorders can significantly affect cognitive, emotional, linguistic, and social capacities. Individuals with conditions like depression, anxiety, schizophrenia, or dementia might encounter problems regulating emotions, thinking lucidly, articulating themselves, and forming meaningful relationships (Page et al., 2015). Such challenges can lead to social avoidance and other barriers. Discriminatory services and negative societal attitudes toward these tourists can further diminish their travel experience (Bauer, 2018; Flaherty et al., 2021).
Tourism, by nature, can be stressful due to unfamiliar settings, packed itineraries, extensive flights, and jet lag. For those with mental disorders, these factors can trigger mood shifts, worsen existing conditions, or even induce other mental health issues, such as travel psychosis (Felkai & Kurimay, 2017; Flaherty et al., 2021).
Regrettably, the tourism and hospitality industry is still lagging in accommodating the needs of tourists with mental disorders. There is a significant gap in establishing destinations that cater to this demographic (Bonny-Noach & Sagiv-Alayoff, 2020). The absence of tailored tourism and hospitality products and services makes it challenging for these tourists to find travel options that meet their needs.
Furthermore, there is an essential requirement for prompt medical services, especially in emergencies. However, locating mental health facilities in unfamiliar places can be a daunting task. Such limitations can cause not only inconvenience but also distress during urgent situations. The lack of adequate medical support can deter these individuals from traveling, stemming from concerns for their well-being (Neo & Flaherty, 2018).
Despite the challenges they face, many individuals with mental disorders can safely and enjoyably travel, given the right preparations. Such measures might include support from caregivers, seeking medical advice before the trip, and using assistive technologies (Flaherty et al., 2021).
Travel, however, is not limited to leisure, relaxation, or learning; it can also be a purposeful activity with potential health benefits. In some instances, travel can act as a non-pharmacological intervention, akin to therapeutic practices like music (Hu, Wen, Zheng, et al., 2023). Dubbed “travel therapy,” this approach can foster health and well-being through avenues like physical activity, nutritious diets, the therapeutic ambiance of natural and cultural landscapes, and fostering social connections.
The benefits of travel therapy can extend across a spectrum of health states, benefiting not only those in perfect health but also individuals in suboptimal health or those with diagnosed medical conditions (Wen, Zheng, & Hu, 2022). Notably, non-pharmacological interventions often have a more pronounced positive impact on mental health compared to physical ailments (Cunnington & Junge, 2016).
By alleviating symptoms and enhancing the overall quality of life, travel can serve as a potential tool to reduce the global disease burden for those with mental disorders (Buckley, 2023; Wen, Zheng, Hou, et al., 2022). 3 The incorporation of such populations into the tourism and hospitality industry is not just a business opportunity; it holds deep societal implications. Recognizing and understanding the travel needs and eligibility of these individuals, and leveraging tourism and hospitality’s potential in public health, becomes crucial.
The Diagnostic and Statistical Manual of Mental Disorders Fifth Edition (DSM-5) classifies mental disorders into 20 groups, covering more than 200 conditions (American Psychiatric Association [APA], 2013). These groups encompass neurodevelopmental disorders, depressive disorders, anxiety disorders, neurocognitive disorders, trauma- and stressor-related disorders, schizophrenia spectrum and other psychotic disorders, and more.
Given the vast range of these disorders, it is impractical to delve into every category in a single letter. Instead, we will spotlight four primary categories: MDD (a depressive disorder), GAD (an anxiety disorder), schizophrenia (falling under the schizophrenia spectrum), and dementia (a neurocognitive disorder). Noteworthily, these four represent a substantial 68.1% of all mental disorder cases. Of these, anxiety disorders stand out as the most widespread at 31.0%, followed closely by depressive disorders at 28.9%. Schizophrenia and dementia are also significant, accounting for 2.5% and 5.7% of cases, respectively (WHO, 2022).
The ramifications of the COVID-19 pandemic on global mental health cannot be overlooked; it has led to a 26% increase in anxiety rates and a 28% surge in depression worldwide (WHO, 2022). Moreover, depressive disorders, anxiety disorders, and schizophrenia rank as the top three contributors to the worldwide disease burden among mental disorders (Vigo et al., 2016; Vos et al., 2020). Alarmingly, dementia emerges as the foremost cause of mortality in this realm (WHO, 2020).
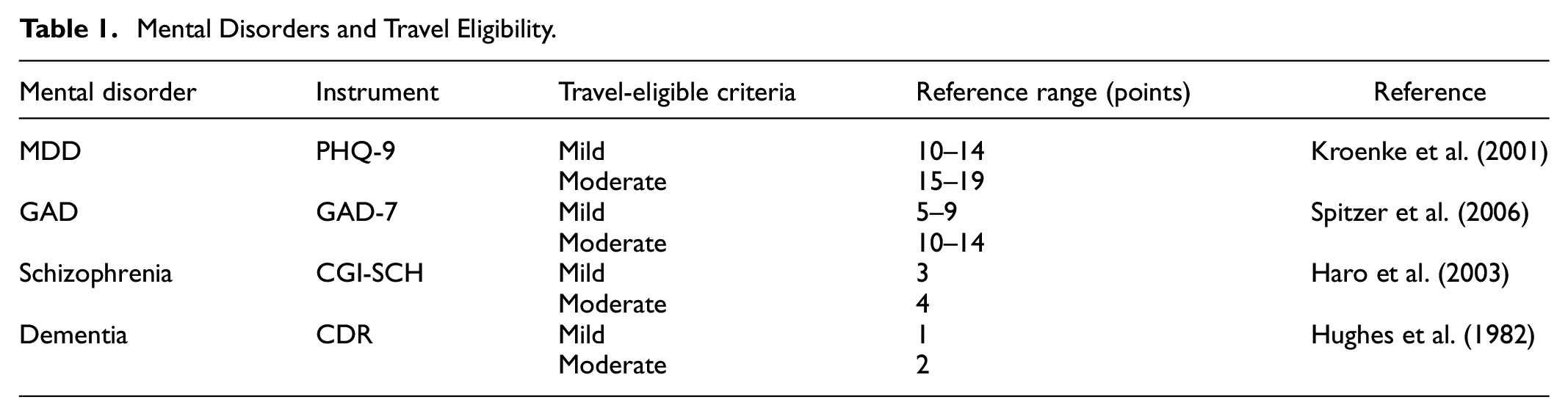
These disorders, with their profound social costs and tangible impacts on patients’ quality of life, emphasize the necessity of understanding travel behaviors and needs for affected populations. By evaluating the travel eligibility of individuals with these representative disorders, we aim to provide invaluable insights for stakeholders. This letter also endeavors to steer further research toward understanding patient travel behavior and assessing the therapeutic potential of tourism, as outlined in Table 1.
Mental Disorders and Travel Eligibility.
Major Depressive Disorder
MDD, also called clinical or major depression, is a unipolar mood disorder that lasts at least 2 weeks and is not caused by substance use or other medical conditions (APA, 2013). Symptoms include depressed mood, loss of interest, significant bodily changes, insomnia, psychomotor agitation, fatigue, feelings of worthlessness, diminished ability to think or concentrate, and recurrent suicidal thoughts or attempts.
MDD is frequently diagnosed—it affected 280 million people worldwide, making it the third largest contributor to global disease burden, and is predicted to be the first by 2030 (Malhi & Mann, 2018; WHO, 2023). Although MDD is complex, it can be treated through means such as antidepressants, cognitive-behavioral therapy, psychotherapy, exercise, and meditation—these interventions can minimize symptoms, restore social functioning, and prevent relapse (Belmaker & Agam, 2008).
Assessing the severity of MDD is often done using the 9-item Patient Health Questionnaire (PHQ-9), which grades MDD as mild, moderate, or severe (Kroenke et al., 2001).
Mild MDD (10–14 Points)
Individuals exhibit symptoms like mild mood changes, fatigue, and reduced interest at this stage of MDD (APA, 2013). These are typically manageable, allowing for daily activities such as travel (Weitz et al., 2015). Encountering new environments and experiences can potentially offset depressive feelings (Belmaker & Agam, 2008).
Moderate MDD (15–19 Points)
This stage of MDD involves more pronounced symptoms, including mood fluctuations, inconsistent sleep patterns, and appetite changes (Malhi & Mann, 2018). While they face greater psychological challenges, their self-management generally remains intact, allowing travel with proper planning (Kroenke et al., 2001).
Severe MDD (20–27 Points)
This extreme form of MDD may manifest with psychotic features like delusions, hallucinations, or potent suicidal ideation (Mitchell et al., 2016; Weitz et al., 2015). These symptoms heavily impact cognitive, emotional, and social functionalities. Due to their heightened vulnerability, travel uncertainties might escalate symptoms, compromising travel safety. Immediate hospitalization might be necessary for some of these cases (APA, 2013).
Diagnosing MDD is complex and typically integrates feedback from various stakeholders like patients, caregivers, and clinicians. Additionally, tests for biological indicators, such as biomarkers, can be employed (Reynolds & Frank, 2016). To supplement the PHQ-9, clinicians might use other tools like the Hamilton Rating Scale for Depression or the Depression Anxiety and Stress Scale 21 (DASS-21) for a comprehensive assessment (Chen et al., 2022).
Generalized Anxiety Disorder
GAD is a mental health condition characterized by excessive and uncontrollable worry about daily issues lasting for at least 6 months (APA, 2013). GAD is often accompanied by physical and psychological symptoms like stomachache, headache, sleep and concentration difficulties, restlessness, fatigue, muscle tension, and irritability (Spitzer et al., 2006).
With 301 million affected worldwide, anxiety disorders rank as the most prevalent mental health conditions (WHO, 2022). Particularly in primary care settings, GAD stands out, escalating risks for other psychiatric conditions like MDD and amplifying the overall healthcare burden. Though the exact cause of GAD remains elusive, it is believed to stem from a mix of genetic, biological, and environmental factors. Management strategies for GAD span from medication (e.g., antidepressants, anxiolytics) to psychotherapeutic approaches like cognitive-behavioral therapy (Santomauro et al., 2021).
Similar to MDD, GAD symptoms and their impacts can range from mild to severe using the 7-item GAD Assessment (GAD-7) scale (Spitzer et al., 2006).
Mild GAD (5–9 Points)
Often termed as subclinical anxiety, this stage of GAD manifests as minor anxiety and sleep disruptions but does not significantly hinder daily life (APA, 2013; Stein & Sareen, 2015). While travel can introduce potential stressors, individuals with mild GAD are equipped with coping mechanisms to manage such anxieties, enabling them to enjoy trips.
Moderate GAD (10–14 Points)
This stage of GAD presents with heightened, persistent worry and physical symptoms like heart palpitations (APA, 2013; Ren et al., 2021). However, even amidst this enhanced anxiety, individuals can navigate their daily tasks activities (e.g., at work, school, or other social settings), albeit sometimes with support or self-help strategies. When traveling, this group can benefit from thorough planning and mindfulness practices, ensuring a pleasurable experience.
Severe GAD (15–21 Points)
Characterized by intense, uncontrollable anxiety, depression, and a range of severe physical symptoms (e.g., headache, dizziness, abdominal pain, diarrhea, heart palpitations) (Santomauro et al., 2021), this stage of GAD can be debilitating, often intensified by concurrent conditions like MDD (Tyrer & Baldwin, 2006). People in this bracket grapple extensively with their symptoms, sometimes necessitating hospital care (Ruiz et al., 2011; Spitzer et al., 2006). Due to the severity, travel is not advisable for this group.
To diagnose and assess GAD, professionals can also utilize tools such as the Zung Self-Rating Anxiety Scale, Beck Anxiety Inventory, and DASS-21 alongside the GAD-7 (Chen et al., 2022).
Schizophrenia
Schizophrenia is a chronic brain disorder characterized by behavioral disturbances, mood dysregulation, and perceptual and cognitive dysfunction (APA, 2013). Symptomatically, it is divided into positive (e.g., delusions, grandiosity, suspicion), negative (e.g., blunted emotions, social withdrawal, stereotyped thinking), and disorganized (e.g., muddled thought, eccentric behavior) symptoms.
Globally, schizophrenia affects around 24 million individuals, often leading to psychosis, health complications, and, in some instances, premature mortality (WHO, 2022). The disorder predominantly emerges in young adults (15–35 years), with a higher incidence in women. Influenced by genetic, environmental, and personal factors, its exact cause remains elusive. Although no cure exists, antipsychotic medications and psychosocial interventions can manage the symptoms, with roughly a third of affected individuals achieving near-complete remission.
The stigma surrounding schizophrenia is profound, yet it is essential to understand that those with milder forms, not in the midst of an acute episode, can partake in activities like traveling if adequately prepared. The Clinical Global Impression–Schizophrenia (CGI-SCH) scale, spanning seven points, helps ascertain the condition’s severity:
Mild Schizophrenia (3 Points)
Symptoms are minimal, such as sporadic delusions or irregular emotional responses (APA, 2013). These individuals, while needing occasional guidance, can largely manage daily tasks and can even benefit from traveling, which might enrich their lives and well-being (Wen, Zheng, Hou, et al., 2022).
Moderate Schizophrenia (4 Points)
Symptoms are more pronounced but still manageable (APA, 2013). Traveling is feasible for these individuals with proper planning, medical oversight, and potentially a companion (Keeley & Gaebel, 2018). Such trips can be transformational, offering personal growth and respite (Hu, Wen, Zheng, et al., 2023).
Severe Schizophrenia (5–7 Points)
Intense symptoms like pronounced hallucinations, extreme mood fluctuations, and potentially self-harming tendencies (APA, 2013). Traveling is not feasible due to the profound impairments in self-awareness, reality perception, and self-care (Galderisi et al., 2018; Keeley & Gaebel, 2018).
For a comprehensive diagnosis and assessment of schizophrenia, tools such as the DSM-5, the Positive and Negative Syndrome Scale, and the Brief Psychiatric Rating Scale are invaluable (Brannan et al., 2021).
Dementia
Dementia is a cognitive impairment characterized by deteriorating memory, thought processes, and behavior (APA, 2013). Symptoms encompass confusion, challenges in task completion, mood fluctuations, and anxiety.
Currently, over 50 million people live with dementia, and Alzheimer’s disease constitutes 60% to 80% of these cases (Lim & Bowman, 2023b; WHO, 2022). Financially, dementia’s global impact was estimated at US $1.3 trillion in 2019, projected to double by 2030 (WHO, 2021b). Despite available treatments, the elusive nature of dementia’s origins results in inconsistent outcomes. Consequently, non-pharmacological approaches, such as art (Hodgson et al., 2023; Marco & Redolat, 2023; Shoesmith et al., 2022), music (Thompson et al., 2023), multisensory simulation (Solé et al., 2022), social activities (Mabire, Gay et al., 2022), and training (Klaming et al., 2023), are favored for their affordability and low side-effect profile (Bowman & Lim, 2022; Livingston et al., 2020).
Tourism emerges as a potential intervention (Wen, Zheng, Hou, et al., 2022), but the feasibility of travel hinges on the severity of dementia and the individual’s functional capacity. The Clinical Dementia Rating (CDR) offers a categorization (Hughes et al., 1982):
Mild Dementia (1 Point)
Individuals may have memory lapses, poor orientation, and judgment challenges but retain self-care abilities (APA, 2013; Regier et al., 2017). Though some behavioral and physical changes can be observed, they are generally minimal, allowing for travel with basic precautions (Arvanitakis et al., 2019; Hu, Wen, Zheng, et al., 2023).
Moderate Dementia (2 Points)
Symptomatic progression is evident, with pronounced cognitive deficits, language barriers, and potential hallucinations (APA, 2013). This stage, which might span several years, necessitates enhanced personal care support. Though travel is feasible, it requires significant assistance and planning (Livingston et al., 2020).
Severe Dementia (3 Points)
This advanced stage severely impacts patients’ quality of life, with pronounced physical issues such as mobility challenges and unresponsiveness to surroundings (APA, 2013). Given their comprehensive needs and decreased awareness, travel is not recommended (Svansdottir & Snaedal, 2006).
To further refine dementia diagnosis and staging, the Mini Mental State Examination and Global Deterioration Scale can complement the CDR (Livingston et al., 2020).
Conclusion
General Discussion
As the prevalence of mental disorders rises, exacerbated by global crises such as COVID-19, there is an increasing recognition of affected individuals as a potentially significant but often overlooked segment within the tourism and hospitality industry. Viewing travel as a non-pharmacological intervention can elevate the well-being and life quality of people grappling with mental disorders (Wen, Zheng, & Hu, 2022). However, determining travel suitability for these individuals demands a collaborative approach, drawing expertise from the tourism, hospitality, and medical industries. Recognizing travel as a fundamental human right emphasizes the need to facilitate such experiences whenever feasible, without being unduly limited by a medical condition.
Generally, tourism emerges as a realistic pursuit for those with mild to moderate mental disorders. Such individuals, with proper guidance from healthcare professionals and meticulous trip planning, can experience the joys of travel and potentially harness its therapeutic benefits. Conversely, those with severe conditions, warranting continuous care or hospitalization, might find regular travel unsuitable. Yet, in their life’s twilight stages, there is a unique niche for “end-of-life tourism” (Rhymes, 1990). This form of travel is not necessarily aimed at therapeutic outcomes but rather embodies the philosophy of “living well with dying”—an opportunity for individuals to live their final moments with dignity, leaving a legacy of cherished memories (Hunter-Jones et al., 2020).
Given the diverse landscape of mental disorders, with their wide-ranging symptoms and severities, a universal guideline for travel suitability is untenable. Decisions should be individual-centric, made after meticulous evaluation. Furthermore, a thorough psychiatric diagnosis, complemented by physical examinations like blood work and imaging, should be coupled with diverse clinical assessment tools to offer a holistic understanding of a patient’s condition and their consequent travel viability (Livingston et al., 2017).
Key Implications
This letter serves as a guidepost for multiple stakeholders (Lim & Bowman, 2023a), spanning individuals with mental disorders, academic and industry professionals in the tourism and hospitality industry, and society at large.
Individuals
For individuals living with mental disorders, this letter represents a beacon of empowerment and self-affirmation. It champions not only the innate right to travel but also highlights the profound therapeutic potential that journeys, be they short or long, can offer. The implications of this understanding are transformative. Recognizing that every trip taken, every new horizon explored, is not merely an escape or leisurely diversion but an active step toward mental well-being can shift personal and societal perspectives. This realization can redefine the narrative around mental health and travel, demonstrating that they can complement each other in therapeutic harmony. Furthermore, having clearly-defined travel eligibility criteria serves as a compass, guiding individuals as they navigate the complexities of planning and embarking on trips. It provides a foundation for stepping out into the world not with trepidation, but with confidence and assurance in making choices that not only celebrate the joy of exploration but also prioritize mental and emotional health. In this context, informed travel emerges as more than just a leisure activity; it becomes an avenue for individuals with mental disorders to advocate for their well-being, deriving healing from every journey.
Academics
As a follow-up to Buckley (2023), academics in the tourism and hospitality discipline stand to benefit significantly from the new avenues this letter unveils. By emphasizing the dearth of research concerning travel-eligible tourists with mental disorders, we are not merely illuminating a neglected research area, but also charting a course for a fresh academic frontier ripe for discovery. As research deepens into this segment, there is potential for the development of novel methodologies tailored to understand the intricate relationship between travel and mental health. Such advancements could reshape pedagogical approaches, equipping the next generation of researchers with a holistic understanding of the potential therapeutic benefits of travel. Furthermore, this confluence of interests might even lead to the birth of sub-disciplines, where the study of therapeutic travel could emerge as a distinct academic niche. Imagine a world where there are psychiatrist-approved travel destinations, curated based on their therapeutic attributes, or travel packages developed in collaboration with mental health professionals that offer structured activities known for their therapeutic effects. Collaborative endeavors are, therefore, not just beneficial but essential. When cross-disciplinary projects merge the nuanced insights of psychiatry with the vast experiential knowledge of travel studies, the potential outcomes—like the development of on-the-go mental health support or training travel staff in mental health responsiveness—could be transformative. Such endeavors could usher in innovative therapeutic travel models, shaping the future of both fields and offering profound benefits to society at large.
Practitioners
For the industry, the underlying message of this letter resonates with the very essence of what service industries strive for: inclusivity and holistic customer care. Recognizing the market potential of travel-eligible tourists with mental disorders not only represents an untapped revenue stream but serves as a clarion call to redefine and broaden the scope of service provision. In an industry teeming with competitors, differentiation is key. Catering to this particular demographic, with its unique needs and preferences, is both a strategic and ethical move. Service providers that rise to this occasion and embed inclusivity into their core offerings can position themselves as frontrunners in a new age of holistic hospitality, reaping both financial rewards and commendations for their forward-thinking approach.
The transformation begins with infrastructure. Accessibility should be the cornerstone of any facility or service upgrade. Ensuring that every touchpoint, be it physical or digital, is designed with a sensitivity to diverse needs can make all the difference. Adopting universal designs, such as accessible pathways, ergonomic furniture, adjustable-height features, and tactile elements, ensures that the environment is welcoming to all. Leveraging assistive technologies, from communication apps to reminder tools, can provide additional layers of support and comfort for travelers with mental disorders.
However, infrastructure alone does not make a service stand out; it is also about human touch. Comprehensive staff training is pivotal. Empathy, understanding, and the capability to respond to a guest’s unique needs can be the difference between a mediocre and an unforgettable travel experience. By fostering an organizational culture that champions sensitivity, awareness, and aptitude, service providers can ensure that their staff are well-equipped to cater to the specific requirements of travelers with mental disorders. They should, however, not be involved in conducting amateur diagnoses.
Tailored offerings are another avenue to explore. The introduction of customized travel arrangements, special dietary options, or even personal assistance services can transform the travel experience for this group. Such bespoke services signify recognition, understanding, and a genuine desire to make a difference.
The importance of collaboration cannot be understated. Building bridges with other stakeholders, especially healthcare professionals, can ensure a more rounded, informed approach to service design and delivery. This cooperative model can aid in pre-travel preparations, crisis management during trips, and even offer critical medical support when required.
Society
In the broader spectrum, society stands at a juncture where inclusivity in travel mirrors the larger ambitions of global inclusivity. When the topic of travel eligibility among people with mental disorders is brought to the fore, it resonates with the principles enshrined in the United Nations Sustainable Development Goals (SDGs). In specific terms, the alignment with SDG 3 (Good Health and Well-being), SDG 10 (Reduced Inequalities), and SDG 16 (Peace, Justice, and Strong Institutions) reinforces the notion that travel is not just a luxury or a leisure activity but an avenue for sustainable societal development (United Nations, n.d.; Rastegar, 2022). 4
The societal ramifications of the alignment are profound. By championing the rights of individuals with mental disorders to travel, we are not only advocating for their inclusion in leisurely pursuits but setting a precedent for their active participation in all spheres of life—be it in workplaces, educational institutions, or within communities. As society becomes more attuned to the unique challenges and strengths of these individuals, it can shape an ecosystem that is founded on empathy, respect, and mutual understanding. This paradigm shift does not merely benefit the individuals in question, but enriches society as a whole by fostering diversity, tolerance, and solidarity.
Furthermore, the emphasis on the therapeutic dimensions of travel for individuals with mental disorders offers an innovative perspective on mental health care. By highlighting travel as a potent therapeutic tool, the strain on traditional therapeutic channels might be alleviated. This not only paves the way for diversified therapeutic approaches but could also lead to more efficient resource allocation in healthcare sectors, translating to potential cost savings.
Limitations and Future Directions
While this letter offers an insightful perspective on the travel eligibility of individuals with specific mental disorders (i.e., MDD, GAD, schizophrenia, dementia), it is imperative to note its limitations. The scope of this letter was confined to only four representative mental disorders, providing merely a glimpse into the vast realm of mental health conditions. The myriad nuances associated with disorder diagnosis and the vast array of diagnostic methodologies mean that not all could be incorporated in this discourse. To this end, the classical clinical assessment tools we referenced serve as a foundational benchmark to gauge mental disorder severity and travel eligibility.
In laying this foundation, we seek to catalyze a broader and deeper investigation into the topic. The horizon beckons for truly interdisciplinary empirical research that extends the scope to encompass a wider array of mental disorders. Such expansive studies should aim for a holistic disorder diagnosis that seamlessly combines both objective biological indicators, such as biomarkers, with subjective informant-reported clinical assessment scales. This would involve perspectives from patients, clinicians, and caregivers alike.
Moreover, future research endeavors should aim to unpack the travel behavior exhibited by tourists with mental disorders. There is a compelling need to delve into understanding how tourism and hospitality might serve as a clinical intervention, potentially altering the trajectory of these disorders in therapeutic contexts.
Envisaging the convergence of tourism and hospitality studies and mental health evokes the prospect of groundbreaking sub-disciplines. These could range from therapeutic tourism studies, examining travel as a therapeutic modality, to mental health-informed tourism design, which tailors travel experiences to the unique needs of those with mental health conditions. The realm of travel psychology might unveil the intricate interplay between travel experiences and the psyche, especially in the context of mental health disorders. Accessibility and inclusive tourism management would expand the purview of accessibility, ensuring inclusivity not just for physical but cognitive and mental health challenges. Data-driven insights could birth travel behavior and mental health analytics, harnessing data to derive patterns and correlations between travel behaviors and mental health outcomes. Not to forget, cross-cultural mental health tourism could unravel how varied cultural contexts and practices can offer therapeutic solace to travelers.
The synergy between psychiatry and travel studies possesses the potential to redefine the contours of therapeutic interventions. Imagine the development of therapeutic travel packages that are sculpted with insights from psychiatric professionals, offering curated experiences like meditation retreats or art workshops. The genesis of psychiatrist-approved destinations could guide travelers to places that resonate with tranquility and therapeutic value. The melding of these domains could also engender on-the-go mental health support during travels, ensuring continuous mental well-being. To ensure this synergy permeates to the ground level, mental health training for travel staff can be instrumental. Research endeavors could also pivot toward quantifying the therapeutic outcomes of travel, offering empirical evidence to refine and enhance travel experiences. Moreover, the birth of therapeutic travel communities can offer a communal therapeutic experience, forging bonds through shared journeys.
Final Thoughts
The intersection of travel and mental health represents a paradigm shift in our understanding of both realms. Recognizing travel as both a right and a therapeutic avenue for individuals with mental disorders illuminates a path toward a more inclusive and compassionate society. By emphasizing the transformative potential of travel, we are not only championing the rights and needs of those grappling with mental health challenges but are also reshaping the contours of the tourism and hospitality industry.
For individuals with mental disorders, the world awaits with the promise of experiences that can heal, rejuvenate, and empower. For the tourism and hospitality industry, this represents an opportunity to foster inclusivity, innovate, and carve out new niches. And for society, this convergence reaffirms our commitment to inclusivity, empathy, and holistic well-being.
As this discourse unfolds, it is incumbent upon all stakeholders—from individuals and professionals to policymakers and society—to tread this path with sensitivity, understanding, and a commitment to positive change. The journey ahead is not without challenges, but the potential rewards—in terms of well-being, fulfilment, and societal growth—are immense.
In embracing the therapeutic potential of travel for those with mental disorders, we are not just exploring new horizons geographically but also charting new territories of understanding, compassion, and societal progress. The journey has just begun, and the promise it holds is as vast and varied as the world itself.
Footnotes
Acknowledgements
None.
CRedIT Author Statement
Fangli Hu (Conceptualization, Investigation, Writing—Original draft, Revision), Jun Wen (Conceptualization, Investigation, Editing and writing), Weng Marc Lim (Conceptualization, Investigation, Editing and writing), Haifeng Hou (Conceptualization, Investigation, Editing and writing), and Wei Wang (Conceptualization, Investigation, Editing and writing).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Fangli Hu’s CSC (China Scholarship Council)—ECU (Edith Cowan University) Joint PhD Scholarship (No. 202109327004) and European Commission Horizon 2020 (Grant number 779238-PRODEMOS).