
Abstract
During the Coronavirus epidemic in Slovenia (March 2020 to June 2021) and during the period of global public health emergency due to COVID-19 (January 2020 to May 2023), public discourse about physicians in the Slovenian media and on social media fluctuated between extremes ranging from idolisation, hero worship and contempt to verbal and physical threats. These diametrically different images of doctors coincided with the measures taken in the country to contain the epidemic and the consequences for the lives of people who suddenly lost their livelihoods and sense of freedom. The discourse observed in comments under media reports and on social media about physicians between January 2020 and May 2023 shows that the entire burden of staff shortages and otherwise poorly organised healthcare fell on medical personnel, who had to deal with long queues, exhaustion and escalated verbal and physical aggression. The depriving of the right to treatment for anyone within a reasonable period of time, which loomed over the entire healthcare system due to the Coronavirus, together with the circulation of different conspiracy theories, caused intense anger, vulgar insults and comparisons of all kinds, physical harassment and death threats against individual physicians, as well as an unjustifiably growing distrust of medicine in general. This article analyses the hostile and abusive online communications that, in real life, were unleashed in occasional physical attacks and other forms of violence against medical personnel in Slovenia. It highlights the complicated interplay between medicine and the social and cultural context during the COVID-19 pandemic and illustrates the complexity of medicine beyond biological understanding.
Introduction
This article analyses the contexts of verbal-pictorial representations of violence and the echoes of real events of violence towards medical personnel during the Coronavirus epidemic in Slovenia. It was found that the three most common types of verbal and psychological ad hominem violence were prevalent in Slovenia, with medical staff being among those blamed for everything that went wrong during the COVID-19 epidemic, as well as the general perception of the epidemic situation itself, namely negative animal associations, sports metaphors associated with COVID-19, and medical war metaphors. These linguistic expressions are placed and explained in the Slovenian context and compared with similar phenomena in other countries.
The review of violent events in healthcare during the COVID-19 epidemic is based on media and social media reports. Observation of communication in open Slovenian Facebook groups (such as Slovenian public hospitals, university clinical centres, health centres, research and educational institutions such as both medical faculties and several faculties of health, nursing homes, the government COVID-19 pages, COVID-19 meters with daily and weekly updated statistics tracking the number of COVID-19 cases, recovered and deaths, professional medical associations, various groups against wearing masks and vaccination, advocacy groups where members searched for information they did not find elsewhere, groups in support of people who exposed themselves during the epidemic while warning about corruption related to purchases of protective equipment and articles in online media, including comments below them, took place between January 2020 and May 2023. The observation period covers the time between the official declaration of the epidemic and the end of the global public health threat from COVID-19 declared by the World Health Organization (WHO). The number of groups observed was not always the same during this period as new groups formed during the epidemic, focusing on providing information about specific problems or about their own activities. Accordingly, it increased from about 10 originally to several dozen.
The process of collecting materials included a daily review of the content of listed sources and accurate documentation of articles, statements, opinions, memes, photo collages, and other images that contained threats, insults, and other shaming statements about healthcare professionals. The criterion for selecting this material was a clearly expressed intent to hurt, shame and offend.
The aim of this process was to capture the psychological diapason of violence caused by the epidemic situation, expressed to release the stress, impress the followers, and directed against health professionals. At the same time, published anonymous or signed personal confessions were collected from health professionals about their experiences and stress due to violence directed against this professional group. These confessions were fewer in number than the above-mentioned threats. Also, articles published in the media about various forms of violence related to COVID-19 were collected and documented (date, location, type of violence and their follow-up stories). Simultaneously with the daily documentation of the published media material and the reflections on the types and causes of violence, its consequences, social tolerance and the systematic search for additional literature, a comprehensive picture of this problem was created.
Violence against medical personnel
Background
The WHO defines an attack on healthcare workers as any act of verbal or physical violence or obstruction or threat of violence that interferes with the availability, access and delivery of curative and/or preventive health services during emergencies. The nature and types of attacks can range from violence with heavy weapons to psychological threats and intimidation. Examples of types of attacks on healthcare staff can include: violence with individual weapons, violence with heavy weapons, psychological violence/threat of violence/intimidation, obstruction to delivery of care, assault without weapons, sexual assault, denial of access to services, armed or violent search of health resource, removal of healthcare assets, setting fire to health resources, and militarisation of healthcare facilities (WHO, 2020).
Violence against health professionals increased significantly at the start of the pandemic, but was a major problem worldwide even before. As a result, the WHO has made many efforts to stop violence and prevent harm, provide support and educate about the causes and prevention of violence in healthcare by publishing guides and training tools in accessible formats to educate about the issue (see WHO, 2022b). The WHO reports that there is a significant risk of violence against medical personnel worldwide (WHO, n.d.). It estimates that between 8 percent and 38 percent of health professionals at the beginning of the twenty-first century have experienced physical violence at some point in their careers (WHO, n.d.). Many more have been exposed to verbal violence by patients and visitors. Health professionals can also be targets of collective or political violence during natural disasters and armed conflicts. Among the most vulnerable health professionals are nurses, emergency medical personnel and other staff directly involved in patient care. Violence against healthcare professionals not only affects the mental and physical well-being of healthcare workers but also affects their motivation to work. As a result, this violence threatens the quality of care and jeopardises the delivery of health services. It also results in major financial losses for the health sector. Prevention of violence against health professionals in emergencies focuses on strategies to improve communication with violent patients and high-risk visitors. Violence prevention interventions aim to ensure the physical safety of healthcare facilities (WHO, n.d.).
Cooper and Swanson (2002) pointed out that a variety of factors can contribute to workplace violence. 1 Healthcare workers may be more vulnerable to violence due to factors like their gender, mental illness or patient alcohol or drug use, for instance. Environmental factors, such as poor lighting, insufficient safety measures and the accessibility of potentially lethal objects, increase the risk of violence. A lack of staff can increase the risk of violence due to prolonged waiting times for patients and leaving staff members alone with patients. Increased violence in healthcare settings may be influenced by workplace stressors, such as mistrust and miscommunication, as well as larger societal factors like social tolerance of violence. Health professionals also work in hazardous settings, such as with refugees from war or in combat zones, where there are inherent risks to the physical and mental health of the workers (Cooper and Swanson, 2002: vi–vii).
A 2008 Slovenian survey on violence against physicians found that patients most often justified their violent behaviour by dissatisfaction with the healthcare system as a whole, with the form and scope of rights under the health insurance system, and because of long waiting times. Less important factors influencing patient dissatisfaction and consequently violent behaviour were dissatisfaction with the physician’s attitude towards the patient, dissatisfaction with the infrastructure and office space, and dissatisfaction with the amount of time the physician allocated for the patient (Dobnikar and Vidmar, 2008: 23). Among the new forms of violent patient behaviour, Slovenian physicians mentioned: rude, insensitive and disrespectful behaviour; more verbal violence by patients and relatives; threats with the media and lawsuits; threats by phone, e-mail and the Internet; blackmail and threats related to treatment; threats of complaints to monitoring institutions; physical violence; and threats of using weapons (Dobnikar and Vidmar, 2008: 22). A 2019 study by the Medical Chamber of Slovenia found that the organisation of work, such as ordering the patients and long waiting in the waiting room, was most often to blame for the outbreak of violence, followed by psychological causes on the part of the perpetrator and rejection of unjustified referral requests (Zdravniška zbornica Slovenije, 2019: 9).
Violence in the time of the COVID-19 epidemic
The worldwide pandemic aggravated public anger towards medical professionals. According to CBC (2020), UN Secretary-General António Guterres said at the outset of the Coronavirus pandemic that the pandemic was unleashing a tsunami of hatred and xenophobia, scapegoating and fear-mongering, and he called for a comprehensive effort to end hate speech worldwide (CBC, 2020). Unfortunately, his wish went unheard. In the first 2 months of the pandemic, there were many reports in the media about how healthcare workers were attacked on their way to or from work, as summarised by McKay et al. in May 2020: In Mexico, nurses and doctors were pelted with eggs and physically assaulted; in the Philippines, a nurse was reportedly attacked by men who poured bleach on her face and impaired her vision; and across India, healthcare workers were reportedly beaten, stoned, spat on, threatened and driven from their homes (McKay et al., 2020: 1743–1744).
The reasons for the attacks varied locally, usually triggered by fear, panic, misinformation about the transmission of the virus, and anger that life had become upside-down and unpredictable. Some governments have threatened the perpetrators of violence, which has not eliminated the causes of the violence. Surveillance and condemnation of violence are not enough because the violence was usually triggered by misinformation and conspiracy theories resulting in the demonisation of certain groups (McKay et al., 2020: 1743–1745).
During the pandemic, attacks on medical personnel increased, which made it difficult for many nations to respond to COVID-19. Known perpetrators were civilians, including local community members and protesters (67%), security forces (30%) and non-state actors (3%; Threats and Violence against Health Care during the COVID-19 Pandemic in 2020, 2021: 4–5). Security forces checking compliance with the lockdown measures also led to violence against health workers who were on their way to work and were falsely accused of ignoring the lockdown measures. Such cases were reported in Burkina Faso, Nepal, India and Mexico. In Egypt, India and Venezuela health workers were threatened, suspended, fired and arrested for speaking out against difficulties they had experienced in their work. In some countries, governments responded to the attacks on health care and took action by introducing new policies to protect health workers and facilities (Threats and Violence against Health Care during the COVID-19 Pandemic in 2020, 2021: 5). Even though attacks on medical professionals are frequent in violent conflicts, the COVID-19 pandemic has highlighted the dangers that these professionals face from both the virus and the general public, as communities were fearful, enraged and frustrated. The constant threats and having to deal with the trauma of seeing patients die also caused health professionals psychological harm.
The Medical Chamber of Slovenia conducted a survey of physicians and dentists between 25 January and 18 April 2022, in which 1761 people responded. They highlighted conflicts in patient care relating to COVID-19 vaccination. A little more than a fifth (20.38%) had experienced or witnessed physical violence associated with vaccination, and just over a quarter (27.38%) had been threatened by patients. Due to their opinions on the benefit of vaccination, one-third of respondents (35.64%) experienced public insults (Zdravniška zbornica Slovenije, 2022).
The first reported death threats against a physician in Slovenia surfaced in May 2020, when an intensive care physician and member of an expert group assessing the supply of emergency equipment commented on national television about the government procurement of ventilators that proved inadequate (Pomurec.com, 2020). This was only the prelude to the escalation of verbal, psychological and physical violence that followed over the next 3 years. During the restrictive measures to contain COVID-19, another epidemic of intolerance and hostility broke out. There was an increase in verbal attacks, incitement and intimidation, and direct death threats against healthcare workers, researchers, politicians and the media. An increasing number of healthcare workers reported threats of physical violence and intimidation with death (Uredništvo, 2020); stalking and unauthorised filming (STA LA, 2020); slander of politicians (Mladi zdravniki Slovenije, 2023); destruction of property such as damaging cars and spraying the facades of private healthcare facilities with paint (Bračko, 2022; STA LA, 2021); harassment at vaccination sites, harassment due to the wearing of masks, vaccination and harassment owing to pandemic fatigue (Čuk Rupnik, 2021; KG, 2021; R B et al., 2022; STA, 2020); burning the containers for rapid testing for the Coronavirus (Hina, 2021; Z M, 2021); the attempted invasion of a university clinical centre by COVID sceptics who wanted to see for themselves whether COVID-19 patients were really being treated there, entering into a fight with hospital security staff (Klipšteter, 2021); anti-vaxxers storming into the vaccination centre (Mariborinfo, 2021); actual physical violence by patients towards medical staff (N R, 2020; Planet TV and IH, 2022; Zavrtanik, 2022); or organised comments on live video conferences on Coronavirus prepared by doctors, medical institutions or associations with the intention of disrupting them.
The wave of public violence against medical professionals seemed unstoppable when, in the midst of the epidemic, democratic freedoms were curtailed for safety reasons. One act of violence or insolence precipitated others. It seemed that anonymous aggression was permanently compromising the safety and dignity of the most exposed people in the healthcare system.
Analysis
General observations concerning human behaviour, beliefs and speech in Slovenia during the COVID-19 epidemic
The general uncertainty created by the sudden advent of the Coronavirus pandemic sparked a number of theories in 2020, especially on the Internet, suggesting or claiming that the pandemic was not random and was managed with the intent to manipulate people so that certain groups could benefit at the expense of others. This contributed to the scepticism concerning COVID-19 measures in parts of the population and to the forming of two opposing camps. The most widespread conspiracy theories claimed that the virus was artificially created to reduce and subdue the world’s population; that it was intended to be deliberately spread; that measures against the coronavirus were intended to control the population such as through the wearing of masks, phone applications and a vaccine with microchips; that the vaccine was changing our DNA; that the vaccine was not safe because it was developed quickly; that the vaccine had severe side effects; that hospitals were empty and doctors did nothing; that they were paid by the pharmaceutical industry or politicians, and so on.
At the same time, some of the medical staff active on social media created closed Facebook groups or used their own personal social media profiles to ridicule and demonise COVID sceptics. Even among the physicians who participated in public debates, there were different opinions and beliefs about the COVID-19 disease, which further fuelled the COVID sceptics’ distrust of science.
Hate speech was also provoked or practised by some politicians who were communicating the situation in the media and through their private social media profiles (Facebook, Twitter). Their hate speech was mainly directed at their critics and civil society. With this, they were reinforcing intolerance among people who already harboured some existential concerns about the epidemic itself. Their often inappropriate and degrading communication also indirectly triggered violence against health professionals.
The outbreak of COVID-19 triggered an avalanche of changes in the patterns of human behaviour and speech. The speed of language modification related to COVID-19 was unprecedented. These changes can be attributed to several factors: the dizzying speed at which our understanding of the Coronavirus kept evolving and its dominance in the media, as well as the increased global interconnectedness at a time when social media and remote contacts were so important. A multitude of new expressions also entered the Slovenian language. The use of epidemiology-related terms greatly increased among laymen, and some new expressions emerged, such as corona time, corona crisis, corona panic, corona idiot or covidiot, corona hero, corona greeting, corona singing, corona humour, corona selfie, corona shopping, corona queue, corona fatness, corona washing and plandemia. Moreover, the bold and confident use of various acronyms such as WHO and PPE (Personal Protective Equipment) became common, and people drew upon historical memory to create certain plague-related words and synonyms which acquired a new meaning in the pandemic situation (e.g. lockdown, quarantine, corona plague). Due to the anti-COVID-19 measures, certain legal phrases were appropriated in public discourse as well (such as corona legislation, corona package (of laws)), and they were related to even more various notions: compliance with measures, behaviour in public places, work in exceptional circumstances, work from home, temporary waiting for work during an epidemic. During the course of COVID-19, the saturation of language with anthropomorphisms and the transfer of human characteristics or relationships to other beings, objects, phenomena or completely abstract concepts, was noticeable.
Negative animal association
In Slovenia, the more the general discontent was spreading among people due to the measures introduced by the government – its mostly arrogant rhetoric, degrading communication, corruption in the purchase of masks and respirators, countless examples of government representatives and officials saying one thing and doing another, frequently violating their own strictly enforced measures in full public view, demanding that citizens adhere to the rules to the point of irrationality – the more conspiracy theories and disbelief in the disease’s existence proliferated. At the beginning of the epidemic, the criterion in public discourse on social media for the existence of this new Coronavirus disease was oftentimes simply whether anyone knew someone who had fallen ill. Corona sceptics were insulting those who were mindful of self-protective measure, calling them names and using various typical images usually taken from the animal world. For example, those who wore masks and followed others’ recommendations were called ‘sheep’ (ovce), to suggest they could not think with their heads, and those who believed that a vaccine would be developed to save the world or later took the vaccine were ‘guinea pigs’ (poskusni zajci). Self-protection was conflated with the idea of meekness and the incapacity of judgement attributed to sheep, and the hope of long-standing protection with a possible vaccine was labelled as a willingness to become an experimental laboratory animal. Comparisons with the ‘boiling frog’ (kuhana žaba) conformed to similar lines: Coronavirus was said to be slow brainwashing, just like a frog that allows itself to be slowly boiled alive. If a frog is suddenly put into boiling water, it will jump out, but if the frog is put in tepid water which is then brought to a boil slowly, it will not perceive the danger and end up cooked to death. This story is often used as a metaphor for the inability or unwillingness of people to react to – or be aware of – sinister threats that arise gradually rather than suddenly.
The more the public perceived the measures imposed by the Slovenian government, especially those arriving in the second wave during autumn 2020, as some kind of random irrational mix, the more uncertain people became about what they could and could not do under the convoluted and erratically changing measures. The more bureaucratic and impractical the implementation of the measures, the more disrespectfully the government communicated with citizens. Besides, the more the government was perceived by people as non-transparent and untrustworthy on account of the seemingly endless corruption disclosed during the epidemic, the more frequently its activities were accompanied by terms traditionally used for smaller, economically and politically underdeveloped countries, that is, ‘banana republic’ (banana republika) and the allegory of the ‘ship of fools’ (ladja norcev), originating from Book VI of Plato’s Republic about a ship with a dysfunctional crew.
Naturally, curse words referring to animals are those for which humans attribute particularly negative characteristics. Rough, disrespectful, insulting words and phrases expressed dissatisfaction with the situation in general and fear of the future, but they were pointed in the wrong direction. Physicians, who were at the beginning of the first wave idolised and promoted into stars, became in the second wave of autumn 2020 ignorant fools, irritating ‘vermin’ (golazen), disgusting insects and worthless, lying ‘pigs’ (svinje) and ‘swine’ (prasci) who are stained with bribery, governmental collusion or are generally bad, lazy people. Some other insults compared them to animal excrement, to ‘dung’ (govno), to insult them, hurt them, humiliate them, belittle and diminish their human and professional value. It was simply impossible to convince a significant part of the public why waiting rooms needed to be empty, why it was necessary to wear masks and take care of hand hygiene and cough etiquette. Any further clarification, especially by female doctors, coined new insults measured on a small scale of the brain, comparable to poultry (‘hen’, kura; ‘stupid goose’, neumna gos). The entire weight of deficient staff and otherwise poorly regulated healthcare fell on the medical staff who were forced to deal with long queues. This was accompanied by the gradual, increasing verbal and physical aggression of patients and their relatives who were unable to get treatment for other maladies in time. The depriving of the right to treatment for everyone within a reasonable time, which loomed over the entire healthcare system due to the Coronavirus threat, triggered severe anger, vulgar swearing, crude comparisons of all kinds and a growing distrust of medicine in general. Many ‘covid-plotters’ who believed the disease was a plot trapped themselves in their beliefs when referring only to their rights while conveniently overlooking all duties (See also Table 1).
Comparative table of animal expressions for medical personnel and individuals who followed protective measures during Coronavirus from March 2020 to May 2023 in Slovenia.
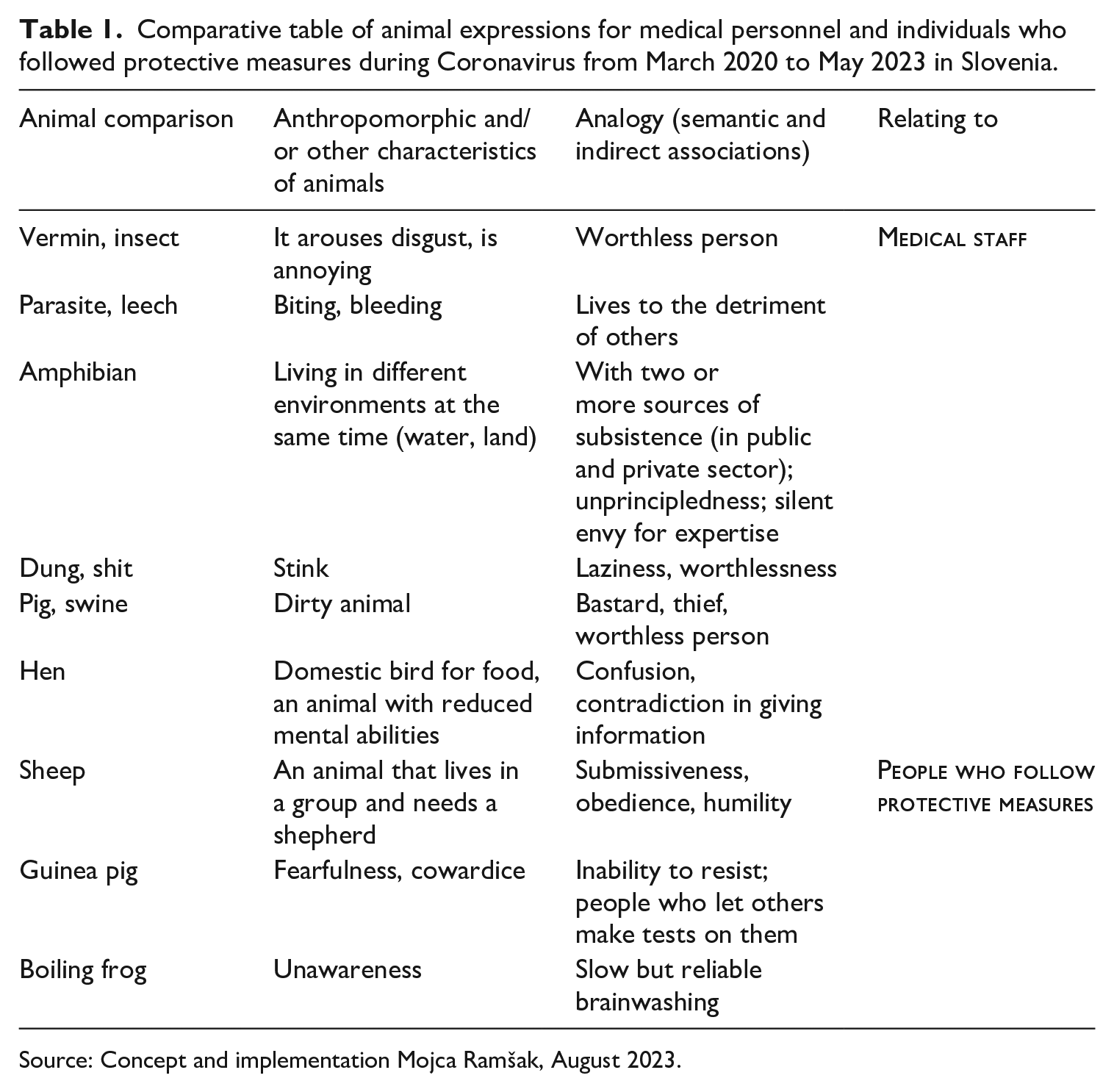
Source: Concept and implementation Mojca Ramšak, August 2023.
Among them were even some physicians of various specialisations whose public statements contributed to significant confusion, thus further undermining public confidence in the recommendations of many other epidemiologists and virologists who agreed on one position. The medical professionals who went along with the oppositional narrative and denied the catastrophic dimension of the disease, developed alternative theories about it and/or did not support measures such as wearing masks and keeping safe distances. Their public appearances, mostly in private and social media, fuelled public anger and upset the official medical discourse. These physicians who disagreed with the opinion of the ‘official medical profession’ had doubts related to COVID-19 and sent their questions publicly to COVID-19 professionals. They received public answers, mainly so that the public would not get the impression that the medical profession did not know how to respond to the epidemic, which would harm efforts to get people to behave preventively (such as in Ihan, 2020, 2022).
Sports metaphors and outer appearance of medical staff
In contrast, the use of sports metaphors served to activate the population to engage in protective behaviour. By referring to sports strategies and ethics, these metaphors tried to motivate people to keep up the good work and continue with the success achieved in the first wave of the disease, for example, limiting the epidemic was ‘a long-distance run’ (tek na dolge proge). At the same time, for the COVID sceptics, the image and fitness of medical staff were also important in this discourse. The perceived image of medical staff that appeared in the media and their physical features, such as dishevelled hair or beards, clothing and obesity, as well as their beliefs and sexual orientation, were often at the forefront of abuse. If the perceived image was not in line with general health beliefs or ‘normal’ lifestyles, this was usually also a reason for not accepting the COVID-19 recommendations and for ad hominem insults. Some local officials addressed the population in metaphors that were close to people from certain regions, for example a football match. For instance, the mayor of the second largest Slovenian city Maribor, where football is a very popular sport, compared the first wave of the disease, when measures worked because people were mostly engaged and followed the instructions, with the second wave, when infections spread rapidly due to the growing mistrust of government measures. He strategically urged residents to cooperate and behave responsibly, as it was not known ‘how many half-times would be played’ (koliko polčasov se bo igralo), that is, how long the illness would persist, and he also warned against a false sense of success and possible subsequent disappointments, since ‘in the first half-time [in March and April 2020] we scored two goals, and in the second wave [in August and then also in autumn] we got ten goals [against us]’. This referred to an increase in infections during the second wave due to easing discipline around protective measures, loss of faith in Coronavirus measures and the fact that the opportunity to defeat the disease was not yet completely lost. Such a football-epidemiological rhetorical strategy was a charge to ‘repeat the exercise and tighten the lines’ (ponoviti vajo in strniti vrste) to regain control over the illness. In a figurative sense, this represented a call for uniformity of behaviour and to consider known facts for illness prevention. The rhetoric that ‘we will defeat the virus together’ (s skupnimi močmi bomo premagali virus) was misleading, but it persisted in November 2020, when it was more than obvious that the resources and capacities were limited. Such well-intentioned deception aroused false hope, which dissipated in great disappointment. Disappointed people no longer trusted and cooperated. Wrongly set misleading goals resulted in wrong actions.
Similarly, in the second wave in autumn 2020 expressions such as ‘a new record in the total number of infections’ (nov rekord števila okuženih), ‘the number of infections set a record’ (rekord v številu okuženih) and ‘another record was broken’ (padel je nov rekord) were used when there was a daily increase in new Coronavirus cases, for example, in September and October. Thus, the word ‘record’ was conceptually used in the opposite sense of its conventional context, that of top achievements.
Some media sensationally presented the records, although it would have been much more precise and strategically wiser to report on the proportion of positive cases (expressed as a percentage of positive cases in relation to the number of tests performed) in laboratory testing. Besides, certain data were published too infrequently, for instance, how many of the laboratory-positive cases were also ill? how many of them were hospitalised? what proportion of these hospitalised patients was seriously ill? how many people recovered? It was also important whether the statistics showed that the people tested were randomly selected or were people suffering various respiratory problems or those who were known to have been in contact with infected persons. There was little talk about this in the media, but this was essential for the epidemiological interpretation of the results. Journalists, of course, are not trained enough in medicine to know what information is most important in such a situation. But over time, because medical professionals explained so often the dangers of the disease and its social consequences, they became more sensitive to the issue.
In September 2020, the majority of ‘covid rebels’ increasingly mocked the measures, the entire information strategy and the doubtful government statistics based upon manually collected information, while some insulted medical personnel ad hominem. These insults were most often related to the appearance of physicians appearing daily in the media explaining details of the danger and the necessary protective measures (e.g. that they were overweight and did not exercise enough to be good role models for the population or that they were bearded and probably, in their opinion, infected (zaraženi), and that they urgently had to visit a hairdresser or barber, that they do not look healthy), as well as numerous other circumstances supposedly affecting their professionalism (e.g. that they let themselves be bought, that they were government mercenaries, that they were former womanisers, passionate smokers, ‘stutterers’, ‘fags’). They inquired about the sex of female doctors: ‘Is that a woman in the picture?’ alluding to an exhausted and unkempt appearance; and likewise, they added, according to appearance, that a woman doctor looked like an ‘aunt’ or a witch (coprnica) and from such a statement it was not far to conclude that ‘witches used to be burned’. Those rhetorical strategies with attacks on appearance, character, motives or any other attributes were intertwined with some other well-founded reasons (e.g. bad, reckless communication, haughtiness), as they sought to convince as many people as possible that measures taken to contain the spread of Coronavirus were not credible.
The insults also came from Twitter profiles with stolen profile pictures (so-called astroturfing; see Voh Boštic, 2021a, 2021b); which exclusively disseminated the ideas of the largest ruling party and produced hostile remarks that appeared to come from random tweeters, but in reality, the authors or subscribers of these remarks were either corporations or political parties. One of these was the attack on a doctor who, in a televised confrontation in April 2020, called the ventilators purchased by the government at the height of the first wave of the epidemic as unsuitable. This doctor, along with two others, was a member of the expert group that evaluated the suitability of Slovenian providers’ offerings. Of all the ventilators, the group ended up rating the model the government bought the worst. Fake profiles immediately after the broadcast began attacking him on Twitter, discrediting him by accusing him of belonging to an opposition political party, insulting his appearance, sexual orientation, political and religious beliefs. A tweet from one of the profiles calling the doctor a liar was also shared by the Prime Minister, who shared a total of 20 different tweets attacking the doctor over the next 6 days after the doctor’s television appearance. In addition to people from the ruling party, media outlets controlled by that party also actively participated in the attack. They shared insulting articles about the doctor on Twitter and tried to discredit him, accused him of acting politically instead of professionally (Voh Boštic, 2021b).
‘Covid rebels’ referred to freedom of all kinds on various virtual and live meetings, encouraging people to ‘wake up from hypnosis’ (prebudijo iz hipnoze) and ‘stop functioning like robots’ (nehajo delovati kot roboti), ‘to seek and follow the truth’ (iščejo in sledijo resnici), ‘to aim for truth’ (delujejo v smeri resnice), ‘follow nature’ (sledijo naravi), ‘think positively’ (razmišljajo pozitivno), and similar phrases which in themselves had no bearing or chance of prevailing over the virus. This ‘following nature’ mentality was strongly related to the notion that living a healthy lifestyle was adequate for protection and survival.
On social media, some asserted known facts about a healthy lifestyle with enough exercise and a balanced diet as a sufficient strategy to keep healthy. However, relying on a healthy lifestyle can be a risky and deceptive stance in the case of an infectious disease. People in good physical shape have, at best, a greater chance of surviving an infection without suffering severe repercussions.
Beyond sports related metaphors, the ideas about ‘natural life’, the need for leading an active life and the harmfulness of the measures that made Slovenians static in the first wave, increased in parallel. The already known facts available on the Internet about the importance of healthy movement were riddled with a cacophony of growing beliefs about COVID-19. People who systematically exposed their ideas on social networks claimed that they had been ‘struggling to breathe freely’ (borijo za svobodno dihanje) since the beginning of the epidemic. In particular, the idea that wearing a mask impeded ‘free breathing’ led to opposition from a section of the public who saw the mask as an obstacle to the exercise of this freedom.
Accordingly, some minors also violated public order and followed the example of some adults by ignoring the measures against the Coronavirus. Some even went to the extreme, hoping that their behaviour would have no consequences. One such extreme case was a 17-year-old schoolgirl who ended up in handcuffs in September 2020 for not wearing a mask on a local bus. Apart from not wearing a mask, she was also rude to the driver and other passengers; she behaved indecently towards the driver and she verbally attacked him after he asked her to put on a mask. As the driver was instructed that passengers must wear a mask for their own safety and the safety of other passengers, he called his supervisor for help, and he called the police since he himself did not have the authority to solve such problems. Even after the police arrived, the passenger did not calm down and insulted them as well. Later, the girl did not cooperate with the police officers and did not give them her personal information. The two police officers informed her that they would take her to the police station for identification. Since she did not comply with their request to leave the bus, they used force and eventually handcuffed her. The passenger’s mother then arrived, with whose help the police officers established her identity. The two police officers subsequently removed her handcuffs (Kralj and Pušnik, 2020). The girl’s behaviour, which was consistent with her mother’s refusal to follow COVID-19 measures, including not wearing a mask, was the first incident in Slovenia in which a minor violated public order and disturbed the peace.
At the same time, there were some cases of misuse and manipulation of public announcements of the official positions of the medical institutions on the epidemic, which were later used in changed contexts. These were not isolated cases, but a recurring pattern that ran like a ‘long-distance race’ (tek na dolge proge) through the epidemic.
By the end of 2020 and the beginning of 2021, it was clear that the ‘dance with the epidemic’ (ples z epidemijo), given the dancing partner, was not going to go well. For a time, Slovenia occupied third place in the world for the number of deaths per million inhabitants. According to the official Coronavirus Meter (Worldometer, 2023), by the end of the epidemic in 2023 a total of 7100 people had died in relation to the Coronavirus in Slovenia (the cumulative number of deaths among detected cases), and 1,344,424 people – 63 percent of the Slovenian population – were found to be infected, as confirmed in laboratories. For a country with a population of just over 2 million, this is an enormous loss. Economic losses, social unrest and political instability are other indirect consequences.
Medical war metaphors
There were other examples of violence, such as the constant refrain that the health workers were Nazis, fascists, that they were genocidal, and that the people would condemn them. Such comparisons of healthcare workers to Nazis appeared not only on social media, but also in the form of graffiti on the facades of medical facilities, in the comments of public lectures by doctors through videoconferencing, and in threatening letters received by healthcare workers.
This leads to the next strand of the analysis: war metaphors. ‘To fight’ and ‘to combat’ were the two words that got under people’s skin, which is not surprising, since everyday COVID-19 discourse was also markedly flooded with medical war metaphors. These had become prominent in the nineteenth century during the cholera epidemic and the rise of epidemiology in general. They assumed even greater prominence at the beginning of the twentieth century, during the First World War, when people were taught about Spanish flu and syphilis, and after the war, when they learned about typhus. These metaphors frequently contained various comparisons such as war, attack, defence, destruction, defeat, enemy and invasion. The concept in which patients themselves represent the ‘material’ on which the battle is waged against an illness is reflected in various forms (Hodgkin, 1985; Lakoff and Johnson, 1980: 291). An illness is seen as an ‘invasion’ of alien organisms to which the body responds with ‘combat actions’, for instance, by mobilising its immunologic defence system; the treatment has become ‘aggressive’; an illness is generally described as an ‘intrusion’; the efforts to reduce mortality represent ‘a battle, a fight, combat, a war’. COVID-19 had become an ‘invisible enemy’. While once a battle with the disease was fought by a doctor, now it was fought by an entire society. Mass ideological mobilisation used the concept of war as a metaphor in various educational endeavours where the main goal was to ‘defeat an enemy’.
For doctors and patients, discourse based on war metaphors is a dominant one, for which there are several reasons:
this metaphor is present everywhere in society (e.g. fight against drugs, alcohol, cigarettes, cancer and, in this case, against the Coronavirus);
the metaphor is easy to understand because there is a metaphorical matching between the opposite poles: enemy (illness), commander (doctor), fighter (patient), allies (medical personnel) and mechanical, chemical and biological weapons (devices and medicines) (See Graph 1);
the logic of war lies in power and aggression on one hand and helplessness and passivity on the other hand, which is often reminiscent of a serious illness (see Hunsaker Hawkins, 1999: 61–90).
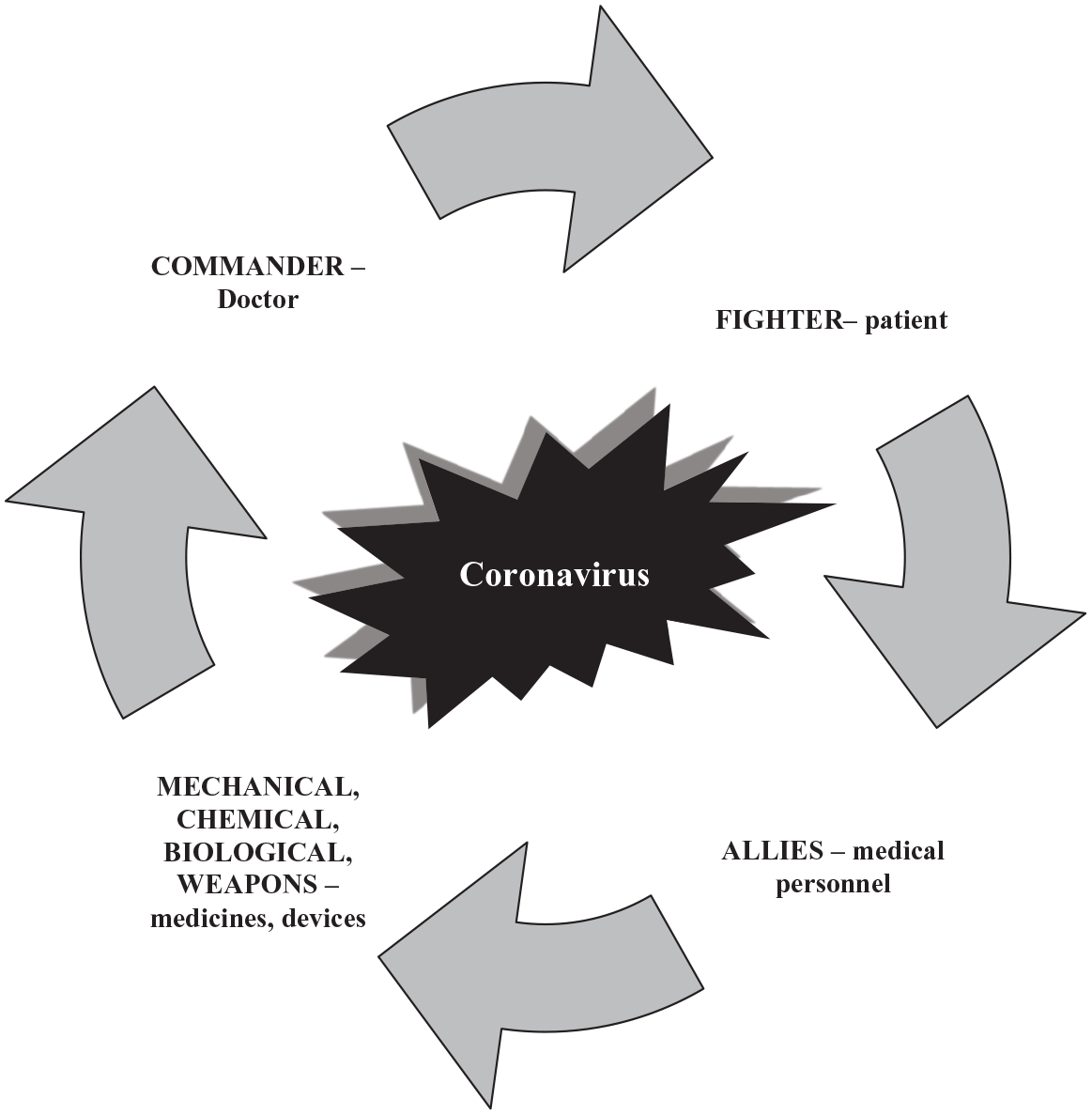
Schematic representation of the treatment strategy with war metaphors regarding COVID-19.
Metaphors of war are contextual: a metaphor can have positive or negative consequences depending on the context. For example, the war metaphor for COVID-19 may resonate with the public, it may help people recognise a threat to public health, it may help them take seriously the duty of physical distancing. The projection of the war metaphors around COVID-19 may be a defence mechanism: fears and anxieties are projected into a war with a sub-microscopic enemy, giving a sense of power and control. However, the oversimplification of complex issues reduces the weight of ethical complexity and trivialises moral choices. The American writer Susan Sontag warned of the dangers of using metaphors in medicine. In her essay Illness as Metaphor (Sontag, 1978), written during her recovery from a cancer that eventually killed her, she describes how metaphors about tuberculosis, leprosy, plague and cancer can lead from fighting the disease to fighting, blaming and stigmatising the patient.
According to Isaacs and Priesz (2020), the use of war metaphors in COVID-19 has some positive aspects, for example, it promotes the mentality of sticking together in this situation, strengthens the public’s identification with the doctors’ efforts to keep the disease under control and emphasises the need to fund adequate personal protective equipment for health workers. The flip side of the coin, however, is the fear that any war brings.
The opposite is also true, namely that the disease is characterised by social disintegration, as Sontag explained: Nothing is more punitive than to give a disease a meaning – that meaning being invariably a moralistic one. Any important disease whose causality is murky, and for which treatment is ineffectual, tends to be awash in significance. First, the subjects of deepest dread (corruption, decay, pollution, anomie, weakness) are identified with the disease. The disease itself becomes a metaphor. Then, in the name of the disease (that is, using it as a metaphor), that horror is imposed on other things. The disease becomes adjectival. Something is said to be disease-like, meaning that it is disgusting or ugly. (Sontag, 1978: 58)
Sontag is arguing here that illness is not a metaphor and that ‘the most truthful way of regarding illness and the healthiest way of being ill is one most purified of, most resistant to, metaphoric thinking’ (Sontag, 1978: 3). She also derides the belief, widespread in plague-ridden England in the late-sixteenth and seventeenth centuries, that ‘the happy man would not get the plague’ (Sontag, 1978: 55). She suggests that the fantasy that a happy mental state would ward off disease probably flourished in all cases of infectious diseases before the nature of infection was understood. Theories that diseases are caused by mental states and can be cured by willpower are always indicative of how much is not understood about the physical terrain of a disease. Sontag is also convinced that there is a peculiarly modern predilection for psychological explanations of disease, as there is for everything else. Psychologising seems to allow control over experiences and events (such as serious illness), over which people actually have little or no control, while psychological understanding undermines the ‘reality’ of illness (Sontag, 1978: 55). Throughout the book, Sontag defends a purely physical understanding of disease, not a holistic approach that includes social and psychological dimensions. In this, she is not entirely wrong, because often such holistic approaches can be misused or misled, which was also observed during the Coronavirus epidemic.
Underestimation and complacency became an essential part of medical war metaphors during the Coronavirus epidemic (Strathern, 2020). In such circumstances, medical war parables prove to be a poor means of expression, for once, the enemy is created one hardly notices anthropomorphism any more. One may indeed see the Coronavirus as the enemy which took one hostage, but the virus does not ‘see us’ that way. If one thinks of the Coronavirus as a human enemy, one radically underestimates its danger in terms of its power to spread; furthermore, one also underestimates the danger one poses to others. Therefore, it is better to look at the virus from the point of view of its resilience because the ‘goal’ of the virus is to find a host, not to fight it. This understanding of colonisation in microbiology, namely that colonisation means the expansion of mucous membranes with the virus, cannot be dangerous like a metaphor. Therefore, in this case, the language of war should not become a means to call the world to action, because there are better ways to do it.
Many political leaders around the world resorted to images of conflict to describe the Coronavirus pandemic. According to Paulus (2020), in France, President Emmanuel Macron said his nation was at war with an invisible enemy. In the United States, President Donald Trump looked forward to the idea of being a ‘wartime president’. In the United Kingdom, Prime Minister Boris Johnson spoke of the virus as an ‘enemy’ and even said that ‘we must act like any wartime government to protect the economy’. But this kind of language did not circulate in Germany. The virus was not an ‘enemy’ and the process of containing it was not war. Perhaps this was because German politicians avoid war metaphors for historical reasons. When German Chancellor Angela Merkel spoke about the Coronavirus, she hardly used a metaphor. In her first major public speech during the Corona crisis on 18 March 2020, she spoke simply and directly, calling the crisis ‘this situation’, a ‘historical task’, and a ‘great challenge’ ahead. In a speech to the German Parliament on 23 April 2020, she again used few metaphors. She described the situation at the time as a ‘real test’, ‘serious times’, a ‘dramatic crisis’ and a ‘gigantic challenge’. The only figurative terms she used were ‘thin ice’ and ‘long-distance run’. These metaphors evoked a challenge, but not a struggle. Other German politicians did the same. Overall, Germany came out of the crisis clearly better than Slovenia in terms of mortality and economic consequences, and most Germans responded positively to the communication strategy of government officials (Paulus, 2020).
In Slovenia, it was different. In communicating and addressing its citizens, the Slovenian government took a militant path that led to distrust, anger and rebellion. The most obvious example of miscommunication was a government spokesman who communicated as if it was a war. Unnecessarily, he often preached from a position of strength, looking for culprits, wagged his finger, inciting panic, intimidating, underestimating: ‘Enjoy while you can!’ (Uživajte, dokler lahko!), ‘Where to, happy excursionists?’ (Kam pa kam, veseli izletnik?), ‘All bad things are yet to come!’ (Vse hudo nas še čaka!) and ‘Let’s have a little joke’ (Pejmo se malo hecat). Tweets from other top government officials also had the same intent.
According to Mikolič (2021), a triangle of power was created in which the new Coronavirus was the aggressor, the population the victim and the government a stern, paternalistic saviour. There was no trust between the human actors of this triangle, and their roles were constantly changing; the government often attacked instead of rescuing, and consequently, the reaction of the people, the victims, was violent. The Slovenian population was involved in a conflict, strong emotions were present, often expressed in the form of fear or hatred, which provided fertile ground for various conspiracy theories and their self-declared saviours. If we wanted to change these attitudes, we would have to get out of the conflict triangle and start treating the health crisis with the appropriate distance that the medical profession provides and approach people with sincerity and compassion (Mikolič, 2021).
Instead, the media and the government were, at the beginning of the epidemic (in March and April 2020) and during the second wave of the epidemic in the autumn, full of messages about sending supplies to the front line, about extraordinary night meetings, about the government which took care of people in wartime (‘We were saving lives’ (Reševali smo življenja) claimed one of the Slovenian ministers, thus trying to defend himself after being caught in the procurement of protective masks through corrupt deals). In speeches, commentaries and discussions about Coronavirus, phrases kept popping up that ‘we were at war/in a state of readiness’ (bili smo v vojni/v stanju pripravljenosti), that the country was dealing with an ‘invisible enemy’ (neviden sovražnik), that ‘an invasion of infection’ (vdor okužbe) occurred in the safe hospital zone or that there were ‘intrusions of infections from the external environment’ (vdori okužb iz zunanjega okolja), that after the official end of the epidemic ‘no one signed a treaty or contract with the virus’ (nihče ni podpisal pogodbe/pakta z virusom), that ‘no one had a round table discussion with the virus’, telling it: ‘You will be allowed to start with your activities here, but you should be a good person there’ (nihče ni imel okrogle mize z virusom in mu rekel tu začni delovati, tam pa bodi priden), that the medical personnel was ‘on the front line’ (na fronti). The latter metaphor arose because medical personnel performed their work under various, crisis-like circumstances, in improvised facilities and not infrequently with equally improvised equipment. At the end of May 2020, the government ‘took credit’ (pripisala zasluge) for the ‘victory over Coronavirus’ (zmago nad koronavirusom), which was marked by a flypast of military aircrafts, followed by a summer ‘period of peace’ (obdobje miru). At the beginning of October, when hospital wards began to close because staff and patients were infected, ‘a war regime’ (vojni režim) was re-introduced in hospitals. When the second wave of the epidemic was declared in Slovenia on 19 October 2020, stemming from a sharp increase in the number of those who fell ill, the public heard pessimistic predictions from scientists that ‘the virus tore down our defensive wall of measures’ and that, ‘fortunately, we had already set up a new defensive wall with new measures’ (virus je podrl obrambni zid ukrepov, a smo k sreči postavili že nov obrambni zid z novimi ukrepi) but ‘the virus leaves a great deal of devastation along its destructive march’ (virus med svojim rušilnim pohodom pušča veliko razdejanje). Nevertheless, politicians promised Slovenians that they ‘would emerge victorious from the health crisis, but only if we all cooperated and worked together’ (iz zdravstvene krize bomo izšli kot zmagovalci, a moramo pri tem vsi sodelovati). Public discourse comprising defence-like rhetoric was riddled with both threats and the hope that the Slovenian people would survive somehow, and it was the use of war language which induced dangerous complacency, where it seemed that it was enough just to say something, particularly if one was, for example, a politician.
In Slovenia, a very peculiar and questionable political folklore accompanied the epidemics. For a politician, even if he was ‘perhaps’ organisationally or otherwise incompetent, it was enough to say something, to be present, to appear in the media and to give the impression of seriousness. This attitude, the paradox arising from their incompetence, became so commonplace that it seemed as if it was completely normal. This contradictory position, in which ineptitude mixed with a public appearance made the person seem respectable, at least from his point of view, went hand in hand with arrogance and the need to appear in public, to leave a mark.
The projection of war parables consequently created new ‘heroes’, namely physicians and nurses, who were highly disparaged in the eyes of the public before the epidemic. During the first wave of the Coronavirus crisis, many slogans of gratitude were coined for ‘corona heroes’ (koronajunaki; heroji korone), namely doctors and other health workers (e.g. ‘Thank you all for being here for us’, ‘Guardians of the nation, thank you’, ‘You are our heroes’, ‘Slovenian heroes, hats off to your effort’, ‘Thank you for your selfless help’ (Hvala vsem, ker ste; Čuvaji naroda, hvala vam; Vi ste naši heroji; Slovenski heroji, kapo dol za vaš trud; Hvala za vašo nesebično pomoč)). Those expressions of gratitude united the community in the slogan ‘Slovenia can do it’ (Slovenija zmore) and mobilised widespread mutual assistance. But the ease with which these heroic phrases were coined soon turned into their complete opposite in the second wave, when doctors became the main culprits for the limited availability of all other treatments, even if restrictions were only necessary at the beginning of the epidemic, as with cancer screening programmes and dental services.
In the summer liminal phase, when measures became more relaxed, doctors became those ‘others’, and they were no longer the ones the population addressed with respect, entrusting them with their health and life, appreciating their Coronavirus expertise. Instead, they were portrayed as bribed liars who deceived the population. This (devolved) leap in thinking was not rooted in the introduction of some new social discipline and a lesser amount of freedom, but exclusively in the turning of certain doctors into celebrities at the government press conferences. From that moment onwards, whoever had any relations with the government fell prey to public ridicule and disbelief.
The meaning of the word ‘hero’ during the epidemics was ambiguous and elusive. Once, heroism contained the idea of duty; today, it represents the dominant public virtue. In the last 150 years, heroism has proven to be an important means of shaping the idea of a perfect soldier – a brave, manly, self-sacrificing one. The idea of heroism spread beyond the manly and the military, and sometimes it even turned into absurdity (Higgins, 2020). The danger of idolising doctors by calling them heroes is that such language can silence criticism and debate: heroes are not supposed to complain about inadequate protective equipment, lack of tests or systemic problems due to years of budget savings in healthcare. One should not expect such heroism from health professionals, but professionalism in the framework of well-funded, well-managed health services. Most doctors would not perform their duties to gain a sense of heroic sacrifice. Many felt quite uncomfortable with that label (Higgins, 2020). In the case of the United Kingdom, nearly 7 in 10 doctors said that ‘Clap for Carers’ did not boost morale in the long term. ‘While the “Clap for Carers” was appreciated, it did little more than paper over the cracks when the true causes of low morale in the NHS run much deeper’ (Locke, 2020).
In Slovenia, before Christmas 2020, columns began to appear in some online media about other ‘heroes of the corona’ chosen by readers. They suggested people who stood out from the average by their actions and solidarity in favour of the common good, ending the epidemic as quickly as possible, or other professional work that the public did not know much about. The focus of the concept of hero has shifted from healthcare to everyday life. These other epidemic heroes met the needs of people whom society could no longer provide for with the help of medicine or measures alone.
The greatest ‘collateral damage’ (kolateralna škoda) was suffered by healthcare workers abroad, as the numbers of deceased doctors from Italy, Spain, the United States and other countries reached well into the thousands (Jones, 2020). In Slovenia, at the same time, everyone warned that if healthcare institutions became the epicentre of the disease and treatment became dangerous and inaccessible, patients with other diseases could become ‘collateral damage’ as a result of COVID-19. In mid-October, there were more than 1000 infected healthcare workers in Slovenia, and due to COVID-19 absences on account of infections, quarantine, possible contacts, and so on, healthcare institutions were faced with organisational problems and forced to suspend non-urgent medical interventions and procedures, while specialist clinics admitted only those patients with emergency referrals. More and more health workers were burned out, which threatened the population that adjusted daily to measures that did not work in the short term. Anger and helplessness were on the rise, and by early 2021, this was spilling over into medical staff in the form also of physical violence. All of the people’s stress, which had previously been channelled on the Internet, began to materialise. In early February, for example, insulting comments were made to medical staff in Maribor who were diagnosing the Coronavirus, calling for someone to shoot them with a Kalashnikov, slap them and beat them. The incident was triggered by fake news (from the Internet) that tests would be done from the throat instead of the nose, which was considered less invasive. Throat tests instead of nose tests were now demanded. When fake news did the rounds, it seemed that those who had already undergone nose tests were deceived and that these tests were unnecessarily forced on them.
When the epidemic was over, the heterogenous forms of violence against healthcare workers did not stop. Commentators repeatedly emphasised that doctors at the time were only ‘fighting for higher wages’ (borili so se za večje plače). A portion of the public, nicknamed ‘couch warriors’ to reflect their ignorance and the pose of the one who sits on the couch as a spectator, sharing his or her opinion with utmost confidence to anyone who will listen, struggled to overcome their conviction that ‘all would be killed’ (vse bodo pobili) by a higher power – groups such as the Illuminati, Bill Gates, the rich and influential in general, or other privileged people, including doctors – and that the majority of people would accept these killings ‘without resistance’ (brez odpora) and ‘by the path of least resistance’ (po liniji najmanjšega odpora). Such ideas contributed to hate speech and violence against those who implemented or adhered to anti-epidemic measures.
Just as metaphors of illness are used for society (e.g. ‘cancer wound’ (rak rana)), social metaphors are used in the same way for diseases, with the war metaphors again taking the lead. However, the uncritical use of war metaphors can have numerous and real consequences, as the imagery and context of these metaphors are politically flammable and dangerous. It allows for xenophobic, racist rhetoric (e.g. against Asian-looking people) and encourages violence. In extreme conditions, sensational war-medical metaphors, in addition to poor health conditions, further promote a tunnel vision, as they lead the population to focus only on an enemy, in this case, medical personnel.
Conclusion
Violence against medical personnel is a complex problem with no simple solutions. There are several strategies to prevent and mitigate this violence, including raising awareness of the problem, supporting medical personnel, and holding perpetrators accountable. The practice and science of medicine are intimately interwoven with the social and cultural contexts in which diagnosis and treatment are offered, and the purpose of medicine can never be fully understood in purely biological terms. People always give a meaning to a disease, and to interpret these meanings is to interpret society. This relationship was unequivocally demonstrated during the turbulent outbreak of COVID-19.
From the contexts presented in this article, we can see that the attitude towards Slovenian medical professionals changed from initial idolisation to contempt to verbal and physical attacks as the epidemic increased at a time of uncertainty, fear and strict epidemic measures. Verbal attacks were dominated by animal terms for medical personnel, such as vermin, insect, parasite, leech, amphibian, dung, shit, pig, swine, hen, to express their worthlessness, laziness, stupidity and confusion. Similarly, people who followed protective measures were often compared to animals and referred to as sheep, guinea pigs and boiling frogs to express their submissiveness and brainwashing. Sports metaphors were created to raise awareness and strengthen the collective spirit, as in team sports. War metaphors were used to describe the situation (war zone, battlefield), but also as offensive tools. Anthropomorphising the virus is dangerous and, when used as a weapon against someone, offensive. There is certainly no point in banning war metaphors, but one can point out their hidden meaning and use other alternative virus-related expressions, such as from the field of music, comparing the immune system to an orchestra, or forming sentences with the expression ‘as if’ (e.g. as if we were at the front, as if we were fighting, etc.). Medical metaphors otherwise only reflect our opinion about the relationship between medical staff and patients, and they show how medicine is anchored in our society. Metaphors, like various other forms of expression, can either contribute to better health or harm it, depending on how we use them and how individuals understand them.
Metaphors during the epidemic can thus be understood on one the hand as an analytical tool for understanding socio-cultural processes, while on the other hand they also help shape social reality through their enforcement. The choice of words and the use of metaphors, which are rooted in military language and permeate everyday use, can also lead to militant thinking and behaviour as well as changes in people’s attitudes towards their environment. At this point, we can repeat Wittgenstein’s thought that the limits of my language are the limits of my world. The changed language associated with the Coronavirus confirms this.
Footnotes
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was conducted during and immediately after the COVID-19 epidemic, while I was working for two faculties: the Faculty of Medicine and the Faculty of Arts at the University of Ljubljana. It was not part of a research project, but rather an additional result. As I am no longer employed at the Faculty of Medicine at the time of submitting this article, the affiliation belongs to the Faculty of Arts.