
Abstract
In 2007, the WHO and UNAIDS established male circumcision as the first surgery ever implemented as a preventive health policy, via their Voluntary Medical Male Circumcision (VMMC) anti-HIV programme that delivered 18.6 million circumcisions in Southern and Eastern Africa by 2017. This article investigates how this genital ritual became a global health policy taking discourse as the entry point. Based on a mixed-method research design, we argue that global health International Organisations are at the forefront of the latest stage of a meaning-making process started in the 19th century: the transnational resemantisation of male circumcision into a medical procedure. First, we introduce the concept of resemantisation to the study of International Relations. Second, we conduct a computational discourse analysis of 396 VMMC policy documents and demonstrate the discursive mechanisms through which they play a role in this process. Third, we combine primary and secondary data to trace the transnational history of the circulation of medicalised male circumcision until its implementation as a global health policy. Overall, we introduce resemantisation as an analytical and methodological framework that nuances our understanding of meaning-making processes and builds bridges between the study of discourses and practices.
Keywords
Male circumcision (MC) refers to a wide range of practices of genital cutting, from the clipping of 1 or 2 cm of skin to the complete removal of the skin surrounding the penis. It has been used for millennia as a ritual organising the societies that have adopted it, through the meanings it carries and the identities and norms it produces. In 2007, the World Health Organization (WHO) and the Joint United Nations Program on HIV and AIDS (UNAIDS) – two major global health international organisations (IOs) – instituted this ancestral practice as the first mass surgical campaign in human history. By 2017, this Voluntary Medical Male Circumcision (VMMC) programme had circumcised 18.6 million men and boys in Eastern and Southern Africa. 1 Among the diverse meanings attached to the practice, within less than 10 years, global health discourses supporting VMMC promoted a medicalised version of MC – which had, hitherto, been marginal globally – as a new global norm for male genitalia. How did male circumcision – an ancient religious ritual – become a global health policy, and what role did the discourses endorsed by IOs and their partners to promote VMMC play in this process?
This article introduces resemantisation as an analytical and methodological framework to address this question. We define resemantisation as a process through which agents – for example, organisations, social movements, communities of expertise – reconfigure the meaning of a physical or symbolic object – for example, a tool, a building, a number, a practice – by privileging a new meaning over previous meanings. We argue that global health discourses promoting VMMC represent the latest stage of the resemantisation of MC into a medical procedure that enabled its expansion to the domain of global health – a new stage of a transnational process that started in the 19th century.
In doing so, this article makes three contributions. The first contribution is theoretical, with the article expanding the existing frameworks developed to investigate the traditional question of meaning-making in world politics. 2 Here, our position aligns with the pluralist stance of International Relations (IR) discourse studies, which advocates for conceptual initiatives to nuance our understanding of the diversity of situations involving discourse in world politics. 3 As we will see, resemantisation offers a flexible framework compatible with a variety of case studies (dealing with organisational and other types of discourses), methodological approaches (macro/micro, mixed-method or qualitative) and conceptual traditions (from securitisation to resignification, from framing to narrative and beyond). More specifically, the concept of resemantisation widens our understanding of the role of discourse in macro processes involving social change and contributes to explaining phenomena that require the joint analysis of textual and non-textual data.
The second contribution is methodological as resemantisation is an analytical framework that comes with a multi-method research design template to help empirical operationalisation. As such, the article builds upon existing initiatives to tackle methodological imperatives for constructivist research in IR 4 and expands the range of research designs adapted to the study of discourse in world politics. 5 More precisely, the profusion of discourse-related concepts that only emphasise the analysis of textual data contrasts with the scarcity of research designs guiding the operationalisation of research problems that require the joint investigation of textual and non-textual elements. As a result, the lack of templates addressing ‘the relationship between analytical and methodological decisions’ 6 for a wide range of IR questions involving discourse runs the risk of researchers limiting themselves to research problems for which such guidance exists. Through our case study, we demonstrate how to implement resemantisation by combining textual and historical analysis. In particular, we conduct a computational discourse analysis of 396 documents curated by global health IOs and their partners to promote VMMC between 2007 and 2016, and use primary and secondary data to develop the first transnational history of medicalised MC up to the start of the VMMC programme.
The third contribution is empirical. We (a) identify the representational strategies in VMMC policy documents that contribute to the resemantisation of MC through global health discourse and (b) show that at the origin of VMMC is a religious practice that has acquired a new medicalised meaning by circulating transnationally between different groups and institutions since the 19th century. In doing so, the article introduces medicalised MC to IR through a focus on its international/transnational dimensions – a case neglected so far despite its relevance to questions concerning IO discourse, global norms, expertise, gender and race. 7 Readers primarily interested in the empirical results can directly proceed to the sections ‘VMMC representations of Male Circumcision’ and ‘The transnational history of the circulation of medicalised MC until VMMC’.
Before going further, we would like to note that both authors have been socialised in European contexts where alternative health policies and medical procedures are privileged over genital surgery. More broadly, the history of the origins of medicalised MC and its effects on male sexuality may cause discomfort, especially for readers who have been circumcised without (or before the age of) consent. Ethical approval for this research was obtained through the London School of Economics and Political Science Research Ethics Committee.
Resemantisation as an analytical framework
The concept of resemantisation was developed in linguistics to account for the process through which social agents begin privileging a new meaning over previous meanings for a linguistic unit. In the last two decades, scholars have begun using resemantisation to investigate objects other than linguistic units, such as territories, borders and artistic productions. 8 While these interventions join IR scholars’ interest in how discourses produce and stabilise dominant meanings, 9 they have not conceptualised resemantisation in a way that facilitates its adoption by social scientists within and beyond IR.
In this article, we define ‘meaning’ as the significative relation between something that acts as a sign and the things that this sign symbolically refers to: what it ‘represents and which can be explained using other words’. 10 In line with the literature, we acknowledge that meaning is not intrinsic to the signified object – for example, immanent – but, rather, is co-constituted by the agents producing discourses associated with the sign it represents and the agents socialised to interpret what this sign means in specific contexts. 11 Meanings are therefore relatively stable but never fully stabilised. This tension, we believe, makes the analysis of processes involving changes of meaning highly relevant as it contributes theoretically and empirically to broad fields of study focusing on the conditions of social change and socio-political reproduction.
First, the concept of resemantisation facilitates the identification of a process that is already of interest in IR and illustrated in a wide range of case studies but is not yet named. Koch, for example, shows how the United Nations High Commissioner for Refugees and the International Organization for Migration have contributed to producing a governance regime of repatriation by shaping the meaning of ‘return’. 12 Felli, meanwhile, shows how the evolution of the World Bank’s use of ‘resilience’ correlates with the emergence of neoliberal forms of governmentality. 13 Similarly, Lemay-Hebert and Mathieu investigate how the OECD’s construction of the meaning(s) of ‘legitimacy’, ‘state-building’ and ‘state fragility’ affect the actions and practices of state builders. We argue that these processes are processes of resemantisation. 14
Beyond the relevance of the concept for the study of (political) terms, we argue that resemantisation also pinpoints a discursive process at the core of socio-political phenomena commonly studied as distinct. Building upon Aykut and Maertens’ argument that several processes using the suffix ‘-isation’ – climatisation, judicialisation, financialisation, medicalisation – are in fact related through a similar logic, 15 we argue that such processes, and other examples such as legalisation, securitisation, sacralisation, are instances of resemantisation. These processes can occur unintentionally or intentionally, for example in the case of resignification – a process through which a stigmatised group transforms the meaning of a category used to cause harm into a positively loaded identity marker, for instance, ‘queer’ or ‘drag’. 16 Rather than representing a substitute for these concepts, the concept of resemantisation sheds light on a fundamental discursive mechanism that links these phenomena together and refines our understanding of the discursive construction of society and international orders.
In the case under scrutiny here, the resemantisation of MC illustrates a case of medicalisation. The concept of medicalisation was developed to grasp the definitional power of medicine and its expansion to include in the medical terrain activities of human life previously outside of its scope. This process has been approached either as a positive or negative phenomenon – a ‘medical form of life’ 17 or an act of ‘medical colonisation’. 18 In line with our emphasis on discourse, we interpret medicalisation as the process through which medical or non-medical agents resemantise something with a medical meaning. In a broad interpretation of the term, any reference to medically-related elements regarding an object means this object can be considered medicalised. For example, many societies that circumcise for religious purposes have mobilised the idea that MC has medical benefits in order to support its promotion. In a stricter sense, to which this article abides, medicalisation applies when a ‘problem [is put] under medical jurisdiction’. 19 In that sense, MC is a unique case: the only instance of a practice undergoing a full medicalisation-demedicalisation-remedicalisation cycle. 20
Second, the concept of resemantisation addresses the demand for analytical tools focusing on the interplay of discourse and other dimensions of international life such as practices and objects of expertise. 21 In line with these developments, we define resemantisation as a process through which agents – for example, organisations, social movements, communities of expertise – reconfigure the meaning of a physical or symbolic object – for example, a tool, a building, a number, a practice – by privileging a new meaning over previous meanings. More specifically, the article explores the interplay between discourse and practice – the discourse supporting the VMMC programme and the practice of MC. Regarding the meaning of practices, we agree with Adler and Pouliot that ‘for practices to make sense, then, practitioners must establish (contest, negotiate, and communicate) their significance’. 22 The concept of resemantisation sheds light on this process articulating two fundamental dimensions of social and political life. It conceptualises how significative dimensions of practice represent discursive sites and, therefore, socio-political opportunities for social agents – such as the IOs curating the documents promoting VMMC – to produce meaning about the world and themselves through discourse.
Third, resemantisation also contributes to expanding the conceptual toolbox for the empirical study of discourse in IR. As discourse is often defined as ‘text in context’, discourse scholarship oscillates between (a) focusing primarily on textual data and using the contexts of production/reception (e.g. sensory, socio-historical) to support the interpretation of the textual material, and (b) using both texts and contexts as sources (e.g. by conducting text analysis alongside another method such as ethnography to investigate how social agents use in practice the discourses identified). So far, research focusing solely on textual data has been dominant. We argue this may be due not only to multi-method research being more complicated, but also because of the lack of concepts guiding the empirical study of complex research problems that require the joint study of both text and context. The concept of resemantisation addresses this gap. In doing so, it answers the calls from IR scholars to expand the scope of discourse research beyond text-focused frameworks 23 and from interdisciplinary literature to go beyond the entrenched domains dictated by single-method traditions. 24
To clarify how resemantisation fits within related concepts that IR readers might be familiar with, we analytically organised a three-level typology of discourse-related concepts, from those whose empirical study is most often focused on text to those that most require the joint analysis of text and context.
- The first type of concepts includes those such as ‘representation’, ‘repertoire’, ‘narrative’ and ‘script’. They refer to organised pools of meaning from which social agents can draw to produce and stabilise meaningful associations, and from which these associations ought to be understood in the context in which they are deployed. For example, ‘frame’ has been defined as ‘the way in which an issue is understood and portrayed publicly’. 25 Concerning resemantisation, these concepts represent pieces of the puzzle that resemantisation aims to solve. On the one hand, these organising significative resources are the medium that provides resemantised objects with new meanings. On the other hand, resemantised objects provide a discursive opportunity for social agents to expand and normalise the pools of meaning that fit their interests and world vision. Empirically, these concepts require the study of textual material interpreted in either their contexts of production or reception to answer questions such as ‘how does X represent/frame Y?’. 26
- The second type of concepts focuses on processes. They often take concepts of the first type as their main unit of analysis and add processual dimensions that address questions of socio-political change and reproduction. The questions these concepts enable us to answer are as old as the interest in discourse itself. Indeed, Foucault’s first coining of the term discourse dealt with the identification of ‘discursive events’ that led to the emergence of new ‘discursive formations’. 27 Since then, processes of meaning-making involving change – explored through concepts such as ‘narrative shifts’ and ‘recontextualisation’ – have been of great interest to IR scholars. However, the terms used to talk about such processes are often under-conceptualised in comparison to the terms in the first group. For instance, ‘reframing’ is mostly used as a lay term in passing and, when defined, ‘framing’ focuses on more specialised issues than the general question of change of meaning. 28
- The third type of concepts deals with multi-dimensional discourse-related phenomena and requires multi-method research designs involving textual and non-textual data for their operationalisation. One main framework has been developed in this vein: genealogy. Developed by Foucault, genealogy aims to trace the correlative emergence of discursive formations and non-discursive elements – such as ‘institutions, architectural forms, regulatory decisions, laws, [and] administrative measures’ 29 – and how this relationship both co-produces them and leads to the emergence of new socio-political orders. Resemantisation is another concept combining an analytical framework with an operationalisable multi-method research design. It offers an alternative way of thinking about the articulation between discourse, social change and reproduction than genealogy, which we argue has dominated social sciences’ imaginary regarding these questions due to the large absence of other concepts of this type. While the relevance of genealogy has been demonstrated within and beyond IR, 30 we argue that its success has normalised correlating the emergence of new discourses with social change, and discourse continuity with socio-political reproduction. Resemantisation accounts for potential alternative scenarios. For example, it enables us to study how the introduction of new discourses can lead to the reproduction of dimensions of contexts by providing new meanings to existing objects. In our case study, the pro-MC discourses promoting medical meanings have changed to adapt to the social norms within which MC is entangled. While MC first acquired medical meanings to curtail ‘excessive’ masturbation, it is now being advertised by medical literature as a way to enhance sexual pleasure and prowess. In both cases, the stamp of medical authority serves to legitimise the practice – from abstinence to virility.
Resemantisation as a multi-method research design
While discourse is largely considered a useful theoretical lens, its study is often inhibited at the stage of empirical operationalisation 31 – a lacuna that ‘has, in the past, turned many innovative theoretical frameworks into rather underdeveloped and unsystematic empirical analysis’, 32 leading engagements with discourse to be ‘regularly criticised as bad science’. 33 To address this challenge, we develop resemantisation as a two-stage multi-method research design to guide researchers interested in empirically accounting for such a process across a variety of case studies:
- The first stage aims to identify discursive strategies that contribute to assigning new meanings to an object. If such discursive strategies are identified,
- The second stage aims to assess if these discursive strategies reflect a process of resemantisation by investigating whether they deal with one object whose meaning is being changed rather than other phenomena (such as different objects whose meanings compete).
First stage: searching for discursive strategies
The first step aims to analyse textual material via methods of text or discourse analysis to identify meaning-making strategies. To help researchers structure their work, we invite them to look for:
- Definitional strategies – by identifying how discourse gives meaning to an object, using the first type of concepts identified above (see p. 5). In this project, we use the concept of ‘representation’, following Matus’s definition of representation as something that ‘gives meaning to one thing by means of another’, and because the flexibility of the concept matches our inductive approach. 34 How do VMMC documents represent MC?
- Oppositional strategies – by identifying how the resemantised object is discursively represented/labelled and in relation to what. In this article, we use tools such as relative term frequency and collocation analysis to look for oppositions. Other analytical tools used by the literature include opposites and differentiation. Are there structural oppositions in the text – manifested by lexical fields, binary categorisation etc. – that construct an opposition between the new meaning and what distinguishes it from previous perceptions?
- Limits to the process of resemantisation – by searching for tensions and discrepancies between the discursive strategies/meanings identified in the two previous steps and other dimensions of the text. As meanings are ‘never inherently fixed or stable’, 35 processes of resemantisation are never complete. This can, for example, be explained by the variety of agents involved in the resemantisation process, the diversity of their target audiences, the existence of competing legitimising logics, discursive inconsistency, or ideological and normative dissonances. To put it differently, discourses that overall resemantise an object can contradict this strategy in the process of implementing it. Identifying these tensions enables us to shed light on the degree of resemantisation as well as the resemantisation capacities and limits of the agents whose discourse we study.
To operationalise this framework for our case study, we conduct a computational discourse analysis of 396 documents hosted by the Clearinghouse on Male Circumcision for HIV Prevention to investigate whether discourses promoting VMMC contribute to the medical resemantisation of MC. The Clearinghouse is an online ‘resource library’ curated by the ‘Clearinghouse partners’, namely WHO, UNAIDS and the NGOs AIDS Vaccine Advocacy Coalition and FHI 360, which describe their mandate as follows:
to generate and share information and resources with the international public health community, civil society groups, health policymakers, and programme managers [and to offer] current evidence-based guidance, information, and resources to support the delivery of voluntary medical male circumcision (VMMC) services (Clearinghouse 2021).
Through this database, IOs and their NGO partners share material related to VMMC such as ‘summaries of research on male circumcision’, ‘tools and guidelines for program planning, implementation, and evaluation’ and ‘materials for communicating and advocating with policy-makers, clients, and potential clients’ (Clearinghouse 2021). The database effectively acted as a sampling frame. To focus more specifically on the process of resemantisation, we limited our corpus to the first stage of the development of the policy (2007–2016) following the premise that promotional material would be more likely to engage in strategies aiming to change the meaning of the existing practice in the early stages of the programme. One thing that distinguishes this corpus from bodies of texts more commonly analysed is that it comprises texts curated and endorsed by IOs and their partners – that is to say, not only produced by IOs but also by other organisations such as funding agencies and national governments.
This article uses computational discourse analysis: an emerging approach in the social sciences that uses the tools developed by quantitative text analysis to study discourse. This approach is suited to the study of resemantisation as its focus on discourse aligns with resemantisation’s analytical ambitions, while its use of quantitative automated techniques facilitates the study of large bodies of texts. In a sense, computational discourse analysis goes beyond ‘text-as-data’ as a paradigm for quantitative text analysis to quantitatively assess linguistic dimensions as markers of discourse. 36
The study builds on the use of the following tools of quantitative text analysis:
- Word count, which measures the number of occurrences of a specific word or set of words;
- Term frequency, which is a measure of how often a term appears in the corpus;
- Collocation analysis, to determine which terms appear together more than they would do so at random;
- Semantic similarity, as measured by the cosine similarity (
- Sentiment analysis, which quantifies the affective states (i.e. ‘positive’ or ‘negative’) of a text by matching its words with external ‘sentiment dictionaries’. We use Mohammad and Turney’s dictionary for sorting words into more nuanced emotional categories (e.g. ‘trust’ and ‘fear’). 37
More information about the organisations curating the corpus, sampling strategies, corpus pre-processing, documents cited as illustrations and procedure of analysis can be found in the Supplemental Material. Replication files, data and additional analysis are available online. 38
Second stage: assessing the continuity of the object under scrutiny through the history of its circulation
This second step aims to trace the history of circulation of the object whose resemantisation we aim to assess. The objective is to identify whether it is one object that is resemantised or different objects with different meanings that we improperly associate. If we cannot identify the process that shows this link, we might not be able to conclude it is a case of resemantisation. For example, in the case under scrutiny, we need to confirm that we are dealing with one practice whose meaning has changed: is medicalised MC a resemantised version of non-medicalised MC or are the two different types of practices only related through our research question? To do so, we trace the transnational history of the circulation of MC that led to its medicalisation and introduction into the VMMC programme.
In doing so, we highlight the political, sociological and geographical dynamics and logics of resemantisation. We identify the key events and stages of this process, as well as the agents and institutions involved. This work also provides contextual information that enables us to contextualise the text-based analysis and put into perspective the discursive agents that we chose to focus on. Moreover, it provides a decentring ground through which researchers who may have internalised the discourse they study can reflexively question these discourses. For instance, in the case of global health, academic and non-academic discourses often share the same underlying assumptions and are therefore analysed jointly by discourse analysts on this basis. 39 For example, regarding MC, pro-circumcision scholarship has advocated for embedding implicit frames in policy documents to help ‘advocates and program implementers as they attempt to promote male circumcision’. 40
Historians have long investigated the transnational history of circulation of a vast array of symbolic and physical objects such as practices, social policies, institutions, identities and pathogens. 41 Similar to other types of large-scale historical analysis like global history, transnational history often implies moving ‘from the archive to the library’ and using secondary data. 42 The use of secondary data is especially relevant when such material exists but has been analysed through mainly national or sub-national lenses. The specific case of medicalised MC invited us to adopt a macro longue durée perspective; but researchers working in more micro-sociological traditions might be interested in exploring the more short-term contexts of interactions in which resemantisation occurs – at the conversational level across a series of IO meetings, for example.
In line with the literature, our work draws on secondary data collected by historians, sociologists, ethicists and health practitioners. We complement these sources with primary data collection when data is missing – using institutional documents accessible online. Practically, we reviewed the interdisciplinary literature until reaching saturation and then analysed it following Saunier’s guidance for transnational history work 43 : finding the balance between drawing connections and relations between institutions, spaces, social groups (‘track and move’) and contextualising key moments and events (‘capture and dig’). In doing so, we established chronologies to identify the main turning points of the resemantising process under investigation and how they led to the VMMC programme. It is important to note that this exercise is different from a global history of MC, which would consider the many manifestations of this practice across the world, and how they came to relate to each other and change through this process.
Our case study deals with the production of medicalised MC, rather than the reception of VMMC policy in the national contexts that were beneficiaries of the programme. As such, the historical analysis focuses on the circulation of MC to the extent that it has enabled MC to acquire its medicalised meanings until the VMMC programme. Other researchers might use resemantisation to produce a textual and historical analysis of reception, by investigating, for example, how the meaning of MC varies between beneficiary countries and social groups within these countries. Indeed, the meaning of the practice goes beyond the results of the text analysis and varies according to the social contexts in which MC is enacted and by whom – for example, being circumcised by an elder in a ritual does not mean the same thing as being circumcised by a doctor in a hospital, and groups who practice MC as a rite of passage to masculine adulthood can themselves interpret the same act as emasculating in the case of forced circumcisions.
To summarise, we develop resemantisation as an analytical framework coming with a research design template that expands the toolbox for the study of multi-dimensional phenomena involving discourses. More specifically, this article follows a mixed-method research design combining the breadth and systematicity of computational approaches with the contextualisation brought forward by qualitative methods – and that computational approaches often lack. 44 Doing so echoes previous IR initiatives to study discourse via transnational approaches 45 and multi-method research design. 46
VMMC representations of Male Circumcision
In this section, we synthesise the results of our computational discourse analysis. We show how VMMC documents display discursive strategies that provide MC with a medical meaning. We also show the limits of this process of resemantisation as our analysis reveals inconsistencies and contradictions within the corpus regarding how MC is represented.
VMMC as a ‘medical service’: between evidence-based medicine and marketisation
Our results align with literature that shows how neo-liberal health discourses of ‘evidence-based medicine’ and ‘cost-effectiveness’ are commonly mobilised to justify development interventions and health policies since the 1980s.
47
VMMC is represented as a ‘service’ justified by rational evidence and individual free will, as well as correlated logics of market and cost-effectiveness. Indeed, ‘male circumcision service’ is the third top-ranked collocation (with maximum length 3) in the corpus
First, VMMC is represented as a modern service grounded in evidence-based medicine. This can be seen through relative term frequencies: ‘medic[al] servic[e]’
Second, VMMC is represented a as service operating according to the logic of the market and market strategies. The documents promoting VMMC reconstitutes medical research with economic terms such as ‘targets’, ‘cost-effectiveness’ and ‘demand creation’. They represent African men as the consumers of this service in alignment with the promotion of ‘demand creation’
To a certain extent, the discourses of evidence-based medicine and marketisation support each other, grounding their rationale in the same logic of modernity and free will. However, tensions can exist between the medical and market logics operating within global health. 48 One may wonder, for example, how the advertisement campaigns of the service align with medicine’s imperatives of ethical transparency. The marketisation of VMMC through posters, hats and T-shirts emblazoned with the ‘national MC logo’ in the ‘A Man Who Cares?’ campaign in Zambia (PEPFAR 2013d) illustrates this tension, as it turns VMMC into a brand and a lifestyle choice (see Figure 1).

Male circumcision ‘merchandise’ in Zambia (PEPFAR 2015).
The ‘medical service’ of VMMC versus the ‘traditional practice’ of male circumcision
VMMC is explicitly represented as medical as opposed to traditional, in a context where most beneficiary countries of the programme have traditionally practised MC prior to VMMC – for example, 92.2% of male population in Ethiopia, 84% in Kenya, 12.8% in Zambia and 9.2% in Zimbabwe.
49
‘Medical service’ appears substantially more than ‘medic[al] practic[e]’
Governments, implementers and advocates must distinguish clearly between traditional and medical male circumcision in all program literature, communications and counselling in regions where traditional male circumcision is practiced.
This dichotomy juxtaposes VMMC against ‘traditional’ MC by explicitly associating VMMC with positive values and ‘traditional’ MC with negative ones. For example, VMMC, as a ‘medical’ intervention, is repeatedly represented as ‘safe’, in opposition to the risks involved in the performance of MC as a rite of passage to masculine adulthood (as pain and risk often constitute an integral part of the ritual to prove masculine values such as courage and self-control).
50
‘Safe’
Another positive value associated with VMMC in the corpus is its ‘voluntary’ dimension, resulting from the idea that, as a medical service, ‘it is an individual choice’ (IDI 2014). In a document endorsed by USAID titled ‘The unpeeled mango’ (Plotkin et al. 2011), it is the very individualism of VMMC that makes it modern; ‘traditional’ MC, by contrast, is collectivistic:
In traditional culture (which could be described as more authoritative, intrinsic, customary, collective and inherited in blood and heart), VMMC was known largely as something that other ethnic groups did. In the modern culture (which could be described as more independent, rational, reasonable, individual, extrinsic and voluntary), VMMC is seen as something that may be done based on perceived health benefits, aesthetics, social status and self-confidence.
Accordingly, the corpus contrasts the incentives to take VMMC – based on ‘inform[ed] consent’
Male circumcision as sexual enhancer: promoting VMMC using ‘traditional’ non-evidence-based representations
When it comes to the potential limits of resemantisation, our analysis shows that this process is incomplete. The VMMC documents do not represent MC in a consistent way, as they also represent it in ways that oppose the meanings and discursive strategies demonstrated so far.
Firstly, in contrast with the definitional and oppositional strategies identified above, the documents also mobilise representations associated with ‘traditional’ MC to promote VMMC – in line with the use of MC as a rite of passage to masculine adulthood which contributes to the discursive construction of sexual masculine norms.
51
As such, medicalised MC is represented as an enhancer of virility, sexual pleasure and sexual performance. For example, the Centre for AIDS Development, Research and Evaluation (CADRE 2016) puts the idea into practice in their ‘salon’ campaign in South Africa, using television and radio to advertise that ‘[s]exual pleasure is enhanced if a man is circumcised’. Elsewhere, the narrator of a video played to discussion groups in Uganda suggests that circumcised men are ‘better lovers’ (Ministry of Health Uganda 2013). In their ‘creative brief’ for MC in Swaziland (now eSwatini), Population Services International (PSI 2009a) underlines the interest in using ‘pleasure-enhancer’ as a marketing ploy based on the national perception that circumcised men ‘can last longer during sex and please their girlfriends, their penises look larger etc.’:
While at this point, we certainly don’t want a campaign that promotes this as the sole reason to go for circumcision, it would still be nice to be able to use this pre-existing perception to our marketing advantage.
Furthermore, the discourses in the corpus reinforce the promise of increased virility by ‘masculinising’ MC. For example, the International Initiative for Impact Evaluation (3ei 2016) distributed pro-VMMC postcards with the slogan ‘Are you tough enough?’, following the fetishisation of pain associated with rituals that test bravery. Similarly, Population Services International produced a series of posters in which they associated VMMC with football – a conventionally ‘male’ pursuit – showing a man in front of a stadium with the following caption: ‘I’m a winner because I have been circumcised’ (PSI 2009b) (see Figure 2).
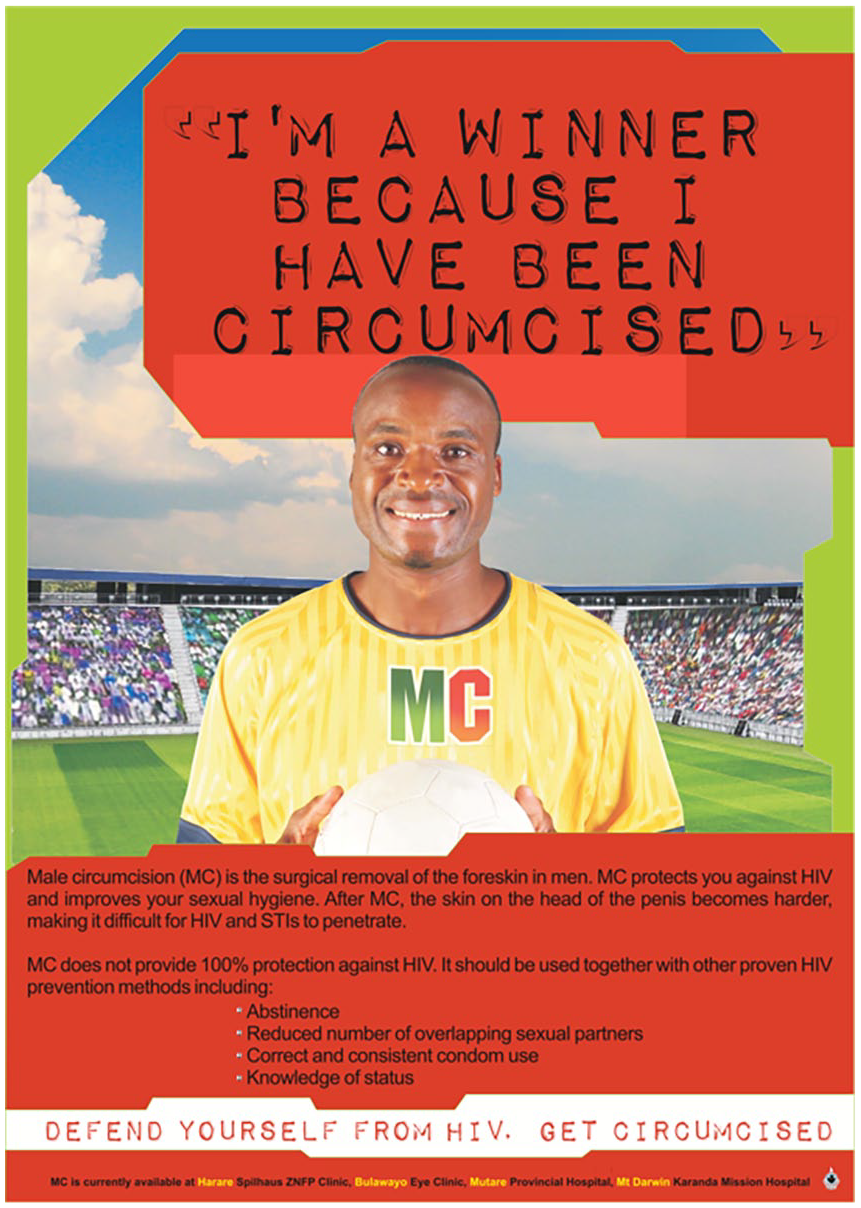
Poster for a football-themed campaign in Zimbabwe.
Albeit rarer, some documents also vindicate the VMMC policy through MC’s religious and historical legacy. Nine documents introduce circumcision as ‘one of the oldest and most common surgical procedures’ worldwide, with another opting to call it ‘an ancient medical and cultural procedure’ (UNAIDS & AIDS Laws Project 2008). The most fervent invocation of VMMC’s long tradition comes from a research synthesis by Wamai et al. (2012):
Male circumcision has been a historical, cultural and religious practice since the beginning of civilisation, and there is evidence that it predates recorded history, with evidence of male circumcision in art forms from Paleolithic Europe. If it really did have any adverse effects, one would have expected the practice to have died out long ago.
Such occurrences also appear in WHO and UNAIDS’ flagship documents as illustrated by the use of an ancient Egyptian relief representing the procedure (see Figure 3).
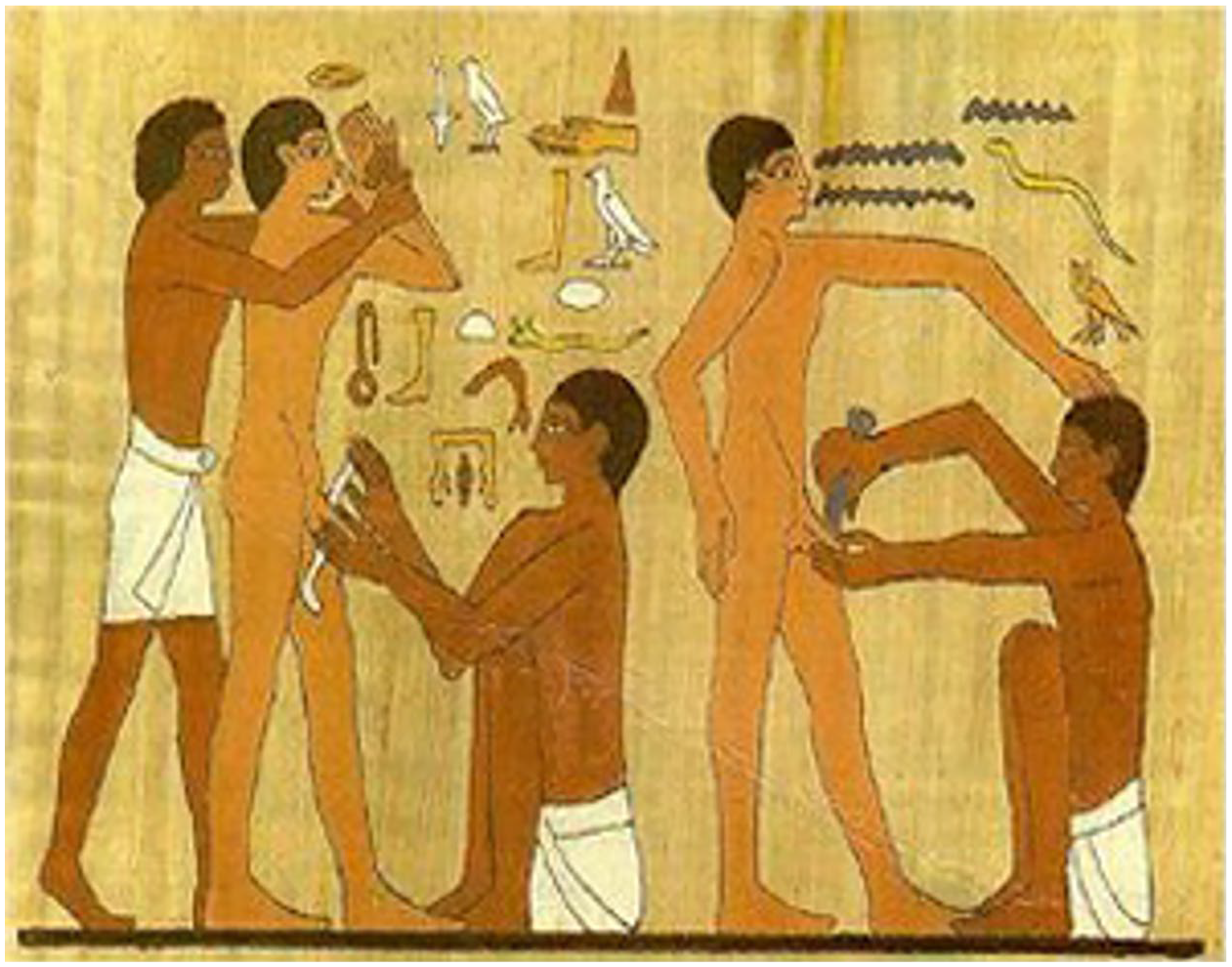
The oldest visual representation of MC 2400 BCE (WHO and UNAIDS 2007).
These contradictions are sometimes acknowledged in the corpus: efforts to demedicalise MC in discourse are sometimes explicitly justified as a means to facilitate its adoption. In a report of their ‘VMMC Demand Generation Meeting’, the Bill & Melinda Gates Foundation (2015) argues that ‘[m]essages of modernity, group cohesion, sexual pleasure, and appeal to women may be stronger motivators for MC than preventing HIV or other STIs’.
An example of this approach can be seen in the ‘Stylish Man’ campaign, also funded by the Bill & Melinda Gates Foundation, which aims to ‘[d]emedicalise SMC [safe MC] and HIV prevention, and reposition HIV services as stylish and desirable for the modern Ugandan man’ (PEPFAR 2013d). Through ‘Stylish Man’ radio programmes, community video clubs and posters (see Figure 4), the campaign associates circumcision status with social status; the circumcised ‘Mr Stylo’ is the embodiment of desirable modern masculinity. The slogan on both campaign posters – ‘Do the right thing. Be a man of style’ – yokes together moral and modish concerns: the right thing is the stylish thing. It is therefore doubly normative, implying that circumcised men are both ethically and fashionably superior to their uncircumcised counterparts. Notice that these posters do not use the term ‘VMMC’ – it is circumcision in general that is modern, temporarily dissolving the medical/traditional dichotomy (in line with the name of the Clearinghouse website: www.malecircumcision.com).
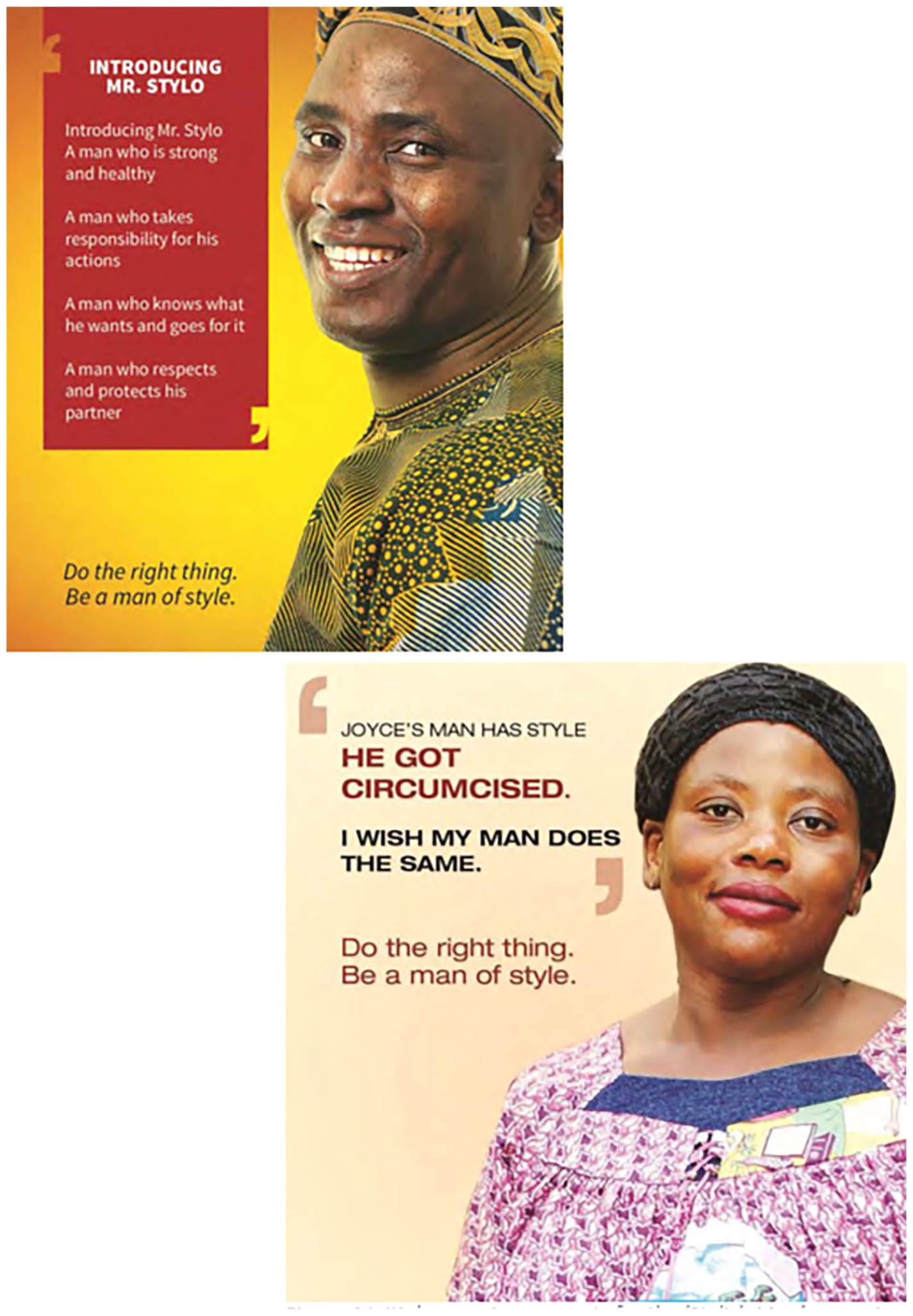
Initial campaign concepts for the ‘Stylish Man’ campaign.
Secondly, while representations of VMMC as a ‘medical service’ support the idea that the policy is born of science and promoted on the grounds of evidence, our analysis reveals inconsistencies between discourse and practice as the rhetoric of evidence-based medicine co-exists with promotional strategies that contradict evidenced documentation and evidence-based standards.
While the medical service of VMMC is opposed to the ‘cultural’ practice of MC on the basis of ‘safety’, the advertisement campaigns tend to hide the risks involved in any surgical act. Like any surgery, VMMC involves risks, as illustrated by the increase in cases of tetanus occurring in VMMC recipients (PEPFAR 2017). However, mentions of risks represented by the procedure tend to be erased by the rhetorical juxtaposition representing VMMC as safe in comparison to ‘traditional’ MC. Although several documents are dedicated to maximising the safety of VMMC, the emphasis on the ‘safe’ nature of the procedure and the relative absence of emphasis on the risks involved directly contradicts the transparency expected from an evidence-based policy matching the ethical standard of current medical norms (see our additional sentiment analysis results related to ‘risk’ 52 ).
Moreover, while the documents emphasise that the medical service of VMMC lies in free will, in contrast with the ‘cultural’ practice of MC, the extent to which VMMC is a truly ‘voluntary’ procedure is debatable. Indeed, the documents promote the circumcision of children as young as 10 in their ‘services’ (WHO and UNAIDS 2016). Moreover, the advertisement campaigns are based on shaming as the material promotes social pressure and plays with masculine insecurities. For instance, Figure 5 belongs to a series of posters for public spaces and urinals, which aligns with previous literature showing that the documents tend to ‘exploit male anxieties about appearance and performance’. 53
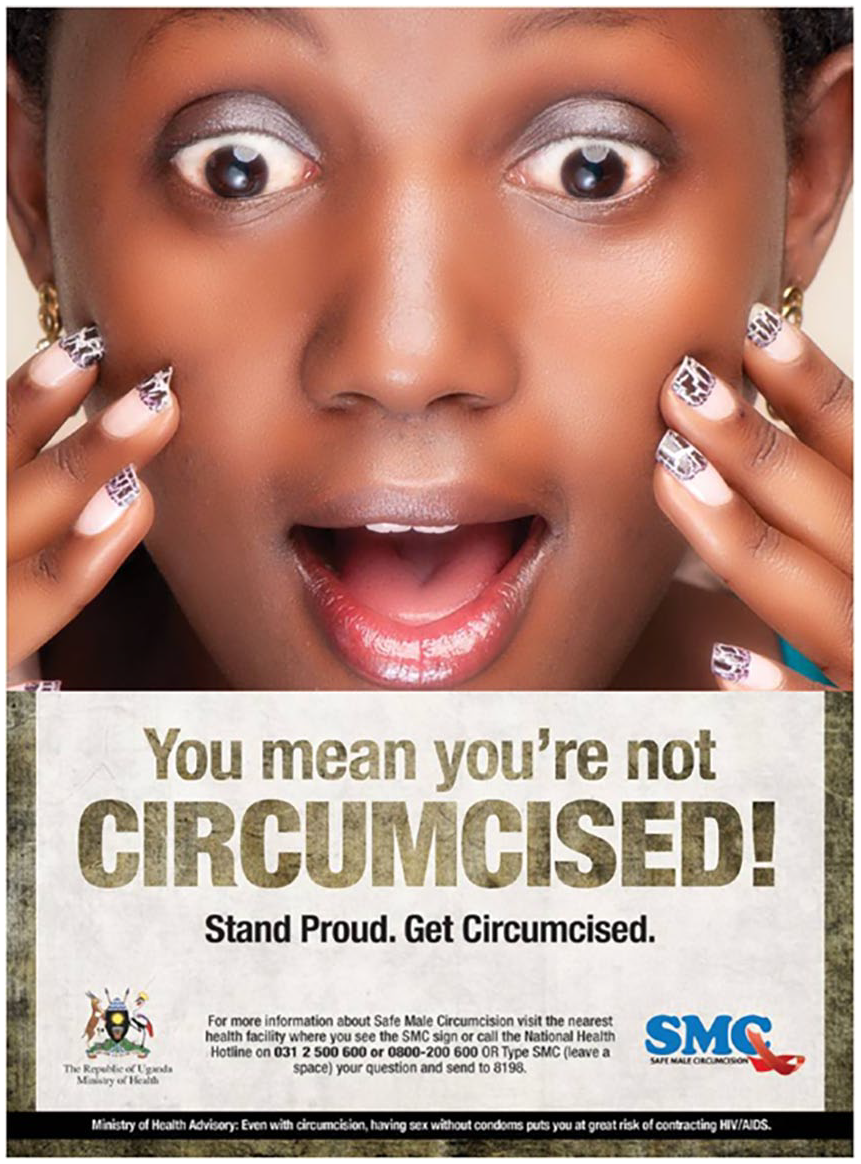
Campaign poster designed by Uganda’s Ministry of Health (2014).
Finally, by including only pro-MC literature, the database does not represent the diversity of evidence-based research dealing with MC, departing further from the medical ideals with which it identifies. For instance, the documents evade engaging with the evidence documenting the role of the highly sensitive foreskin in sexual pleasure and the potential negative effects of circumcision on sexual and psychological well-being (see the additional analysis to learn more about how VMMC documents pathologise the foreskin 54 ). 55 This absence is especially striking considering that anti-MC transnational movements are spurred by precisely such evidence. 56 This point is further illustrated by the lack of engagement with the global health literature questioning the evidence supporting VMMC (see pp. 22–23).
To conclude, our analysis shows that VMMC documents produce definitional and oppositional strategies that endow MC with medical meaning by distinguishing medicalised MC from non-medicalised MC. However, such strategies could reflect the existence of two different practices and the effort of global health actors to unpack their differences. Therefore, in order to demonstrate that this case is in fact a case of resemantisation, we need to trace the process through which non-medicalised MC became medicalised and the factors that contributed to global health organisations becoming part of this discursive process.
The transnational history of the circulation of medicalised male circumcision until VMMC
The historical analysis confirms that at the core of the VMMC programme was a religious practice that acquired new medical meaning(s) through its resemantisation. The medical resemantisation of MC does not start with VMMC, though, as MC’s introduction to global health represents only the latest stage of a longue durée process mobilising representations and discursive strategies trialled over more than a century. We identify three stages in this process. First, South Asian Muslim populations introduced MC to British colonisers, who in turn introduced it to Britain where it became medicalised in the context of anti-masturbation movements. Subsequently, the transnationalisation of the medical sector in the British Empire supported the transnationalisation of this new meaning in the British dominions. Second, the establishment of evidence-based medicine led to the demedicalisation of MC across the empire in the mid-20th century, except in the US, where it was only partially demedicalised. Third, the second wave of the transnationalisation of MC’s medicalised meaning via its introduction to global health is concomitant with the remedicalisation of the practice in the US at the end of the 20th century.
From the British Empire in South Asia to the medicalisation of male circumcision in anti-masturbation Britain
The transnationalisation of MC is ancient, following the migration of circumcised populations and the globalisation of religions practising it like Judaism and Islam. The territorial and economic ambitions of European imperialism opened new routes for the circulation of MC in the modern era. This is particularly the case for the British, who were the first European population to adopt circumcision for non-religious reasons, because of their colonial encounters with circumcised Muslim populations in South Asia. 57 In his ‘Social History of Male Circumcision’, Aggleton shows the diversity of British experiences of MC in South Asia, from being a condition to business dealings to forced MC happening on colonial battlefields to the subsequent preventive circumcision of British troops to avoid such acts of sexual violence. 58 As such, imperial trade and war relationships, combined with religious, moral and class systems in Britain, shaped the adoption of the practice by British colonisers and its subsequent introduction to the metropole, where it changed male body norms.
With MC becoming more common among British men in South Asia, officers became growingly socialised into the local meanings associated with this practice; and religious discourses promoting MC based on sexual temperance echoed British society’s emerging value system. More precisely, MC could represent a solution to what Victorian England perceived as the problem of masturbation, amid the ‘great masturbation panic and the discourses of moral regulation’ raging in 19th and early 20th century Britain. 59 Discourses of social purity – combining the purity of the soul with physical hygiene – turned the foreskin into the symbolic representation of impurity, both unclean and sinful. These newly acquired moralist and hygienist meanings provided legitimising grounds for anti-masturbation movements to promote MC outside the colonial context. As a result, British nobility adopted MC in the metropole in the mid-19th century, where it acquired yet new meanings associated with the class system. 60
It is at this time that MC’s medical and sexual meanings identified in the previous section became first normalised in Western contexts. The medicalisation of masturbation as an illness to be cured had started with the publication in London of the best-seller of its time: Onania, or the Heinous Sin of Self-Pollution and all its frightful consequences (in both sexes) considered with spiritual and physical advice to those who have already injured themselves by this abominable practice. 61 As anti-masturbation movements grew throughout the medical sector, so did the list of masturbation’s alleged ill effects. The search for a cure fot masturbation subsequently led to the medicalisation of practices already perceived as preventing masturbation, such as MC.
Indeed, British medicine ‘discovered’ MC in the late 19th century as a cure for masturbation, 62 starting a quest to justify MC on medical grounds that would last until the VMMC program. MC began to be represented as a miraculous prophylactic and curative solution not only for masturbation but for all kinds of diseases such as paralysis, oedema, elephantiasis, gangrene, tuberculosis, hip-joint disease, impotence and hystero-epilepsy, as well as a variety of other mental disorders. 63 The entry of MC into the medical sector marked a new chapter in its history, which departed from previous meanings to become a ‘procedure in search of a biomedical rationale’ legitimised via ‘extravagant medical claims lacking scientific justification’. 64
All in all, the medicalisation of MC – the resemantisation of MC as a medical procedure in 19th century Britain – endowed the agents promoting this practice with unprecedented institutional resources to legitimise MC via a new type of ‘expert’ discourses.
The transnationalisation of medicalised male circumcision in the British dominions and its subsequent demedicalisation
Beyond enabling MC’s circulation from religious to medical sectors and introducing non-religious MC to European populations, the British Empire played yet another role in the history of its circulation by facilitating its globalisation from the metropole to its dominions. The transnationalisation of medical doctors and their educational trajectories from Britain to North America, Australia and New Zealand led to the transnationalisation of the medical representations of the foreskin and its clinical governance. The evolution of the practice in these territories followed Britain with a delay: MC appeared later in the British dominions but endured longer than in Britain. In Australia and New Zealand for example, MC reached its peak around the 1950s with more than 80% of men and boys circumcised in that period. 65
The transnational success of medicalised MC came to an end when new generations of British doctors started investigating the actual medical benefits of the practice. 66 The very expert community that contributed to resemantising MC with medical meanings ended up being the one that actively delegitimised the practice from this association. Theories supporting the medicalised use of MC and the prescientific notions underlining them did not survive the transition from ‘traditional’ to ‘scientific’ medicine. 67 In 1949, a medical report questioning the procedure was published in the UK, highlighting that phimosis – that is, the inability to retract the foreskin (and the main concern that justified preventive MC) – had been misdiagnosed due to the fact that most boys do not have retractable foreskin before age 3–4. 68 The results of what became referred to as the ‘Gairdner report’ had a major impact on the practice in the UK, with a decline of neonatal medicalised MC reaching 6% by 1975 (based on army records, it had been estimated that ‘before the Second World War 50 per cent of working class and 85 per cent of upper class men in England were circumcised’). 69
The impact of the Gairdner report followed with a generation’s delay in the dominions. The report started changing practices in the 1960s, with medical associations officially recommending against medicalised MC in Australia (1971), Canada (1975) and the US (1975); the most spectacular shift being New Zealand ‘where circumcision rose suddenly to near universality and later fell to vanishing point even faster’. 70
A broader shift of context favoured the positive reception of new knowledge about men’s genital and sexual health. Economic and institutional factors contributed to the demedicalisation of MC in the United Kingdom. One year before the publication of Gairdner’s report, the newly established National Health Service declined to allocate funds to routine MC due to a lack of evidence of its medical properties and the existence of efficient alternative non-surgical procedures. 71 At the same time, cultural norms regarding sexuality were shifting away from sexual disciplining and temperance, which made the desensitisation of the penis a less appealing proposition. 72
The remedicalisation of male circumcision in the United States and the second wave of the transnationalisation of its medicalised meaning via the VMMC programme
Since then, however, the US medical community departed from the international consensus by promoting MC remedicalisation at the end of the 20th century. Globally, 68.8% of men over 15 years old circumcised were Muslim, 0.8% were Jews and 12.8% were Americans circumcised for non-religious reasons. 73 The only other country where MC is primarily performed under medical jurisdiction is South Korea, whose unusual trajectory has been considered influenced by American culture. 74 After stating in 1999 that the risks and benefits of MC were relatively balanced, the American Association of Pediatrics stated in 2012 that ‘the health benefits of newborn male circumcision outweigh the risks’. 75
Meanwhile, the rest of the global medical community has not changed its position regarding the lack of prophylactic or curative evidence on which grounds the practice should be medically justified. Rather, it recommends non-surgical interventions for the predicaments MC is supposed to prevent and cure. 76 As a result, the medical sector worldwide tends to consider US male genitalia exceptionalism as a ‘cultural bias’ and ‘cultural prejudice’. 77 Authors question why routine MC ‘is still practiced in the US at a time when evidence-based medicine is the global standard’ since ‘there is no scientific evidence that a possible minimal advantage of circumcision counterbalances the disadvantages’. 78 The complex set of domestic reasons – from social conformity, class and xenophobia to health insurance coverage and family dynamics – explaining this unique situation falls outside the scope of this article. It is important to note, however, that the remedicalisation of the practice in the country did not go without resistance as research shows that younger, female, and (uncircumcised) doctors have historically been less supportive of MC than their older male circumcised counterparts. 79
This remedicalisation of MC represents an important stage in its resemantisation as pro-circumcision medical sectors re-mobilised meanings developed in the first stage of the medicalisation of MC in the 19th century to try to justify the practice at the end of the 20th. As Carpenter underlines: ‘after a phenomenon has been demedicalised, subsequent rounds of medicalisation do not start from scratch, but rather are facilitated by lingering medical definitions and medicalisation proponents’. 80 Illustrative of this argument is the persistent attempt to justify MC mass implementation by associating it with STIs. Indeed, this domain of research was both critical to the initial medicalisation of the practice (as it enabled medical expertise to enter normative debates of morality and sexual management) and at the core of the latest stage of the transnationalisationation of the (re)medicalised practice via global health IOs.
Doctors started trying to justify MC through the treatment of venereal disease in the 1880s, 81 claiming, for example, that lower syphilis rates happened among Jews than Gentiles due to the use of the practice. 82 However, analyses of STI rates by circumcision status found that evidence was inconclusive. 83 But the fact ‘that no scientific research validated the theory that circumcision inhibited the spread of venereal disease did not keep physicians from continuing to promote the view that it did’, nor from targeting discriminated-against groups based on their alleged ‘promiscuity’ – for instance, the African American population. 84 The fear of syphilis between 1910 and 1920 contributed to an increase in medicalised MC in the countries practising it. 85
As Carpenter’s work highlights, pro-MC medical researchers have been following the same logic to justify anti-STI mass circumcisions in Africa since the 1980s, despite these works being debunked due to the neglect of controlling variables (e.g. the fact that ‘circumcision was associated with other factors, such as Islamic beliefs, that prompted relatively conservative sexual behavior’). 86 Yet, the quest for a medical rationale for MC in relation to STIs continued and acceptability studies kept being conducted in the absence of medical breakthroughs. 87
The evidence finally came in 2007–2008, with Randomised Control Trials (RCTs) in Kenya, Uganda and South Africa that propelled the remedicalisation of MC to a new level by concluding that there was a 50%–60% reduction in female-to-male HIV transmission for a follow-up period of 21–24 months after circumcision. 88 These experiments provided a new rationale to further legitimise the medicalised meaning of the practice.
The RCTs, however, were met with scepticism regarding their methodology, which was perceived as departing from existing medical standards – for example, the fact that MC groups received additional counselling on safe sex practices compared to control groups, that the sample was too small, that the duration of the experiments was too short or that the trials were conducted in countries where uncircumcised men were more HIV-positive rather than in countries where circumcised men were more likely to be HIV-positive. 89 The generalisability of the results was contested due to a failure to account for confounding factors such as social/religious characteristics, sexual attitudes or penile hygiene, and due to the fact that no field test had been performed to account for ‘the classic distinctions between efficacy and effectiveness trials, and between internal validity and external validity’. 90
Beyond these methodological problems, a second area of concern was the lack of evidence regarding (a) the process through which MC was supposed to prevent HIV transmission and (b) the lack of comparative analysis with contexts in which both MC and HIV rates are correlatively either the highest or the lowest. 91 Finally, literature highlighted that MC could lead to increased HIV transmission due to inadequate promotion – introducing MC as ‘as good as the HIV vaccine’ 92 – or existing behaviours and beliefs in the target contexts, for example the idea that MC works as a ‘natural condom’. 93 Experts were especially concerned regarding male-to-female transmission as the RCT in Uganda showed a 61% relative increase in HIV infection among female partners of HIV-positive circumcised men. 94 Additionally, social scientists raised concerns about pro-circumcision biases underpinning the medical literature and its representation of the foreskin. Indeed, the results offered a ‘new etiology for HIV [by] positing the foreskin as a disease vector and circumcision as the treatment’, 95 which aligns with the results of our discourse analysis (see our additional analysis). 96
Despite these concerns, the President’s Emergency Plan for AIDS Relief of the United States government (PEPFAR) started funding VMMC interventions the same year the results of the RCTs were published. Soon after, the WHO and UNAIDS endorsed the initiative and recommended MC as a key component of anti-HIV prevention policies via the VMMC programme, implemented in partnership with national governments and NGOs. Between 2007 and 2017, PEPFAR remained the main funder of VMMC. It is estimated to have supported 84% of all VMMC surgery during this period, with USAID being the forefront agency leading the initiative in collaboration with the Bill & Melinda Gates Foundation, UNICEF, the World Bank, the WHO, UNAIDS and the Global Fund to Fight AIDS, Tuberculosis and Malaria. 97 These organisations have either produced or funded many of the documents analysed in the previous section.
In the beneficiary countries, the medicalisation of MC not only expands MC to populations not practising it, but it also medicalises the practice among populations practising it outside the medical sector. 98 In line with the historical use of the practice for the production of sexual norms, literature shows that VMMC represents an opportunity for the actors supporting it to produce sexual health advice normalising moral and sexual agendas in beneficiary countries. 99 HIV, rather than syphilis, had offered the breakthrough pro-MC health actors had been looking for. However, the sector has not given up on syphilis as the disease continues to be considered a useful discursive resource for the promotion of medicalised MC ‘in settings where HIV is not prevalent, or where the main mode of HIV transmission is intravenous drug use’. 100
Ten years after the start of the programme, ‘the biological mechanisms by which circumcision is protective remain incompletely understood’ even though extensive research in that direction has led to promising research hypothesising mechanisms based on a meta-analysis of the literature. 101 However, as the authors of one such meta-analysis suggest: ‘It might appear that understanding these mechanisms would be a moot point for men who undergo circumcision’. 102 The same is true for VMMC critics who still call for more contextualisation in the methodology – for example regarding the fact that RCTs data inform mathematical modelisation estimates 103 – and also denounce the politics of the policy. Indeed, since its inception, the policy seems to have been increasingly politicised, for example with its denunciation in anti-circumcision social movements in the US. 104
To conclude, the historical analysis confirms that at the origin of VMMC is a practice that has acquired medicalised meaning by circulating between different groups and institutions over more than a century. We show that the resemantisation of MC involves different stages (medicalisation, demedicalisation, remedicalisation) and a vast range of social actors, including epistemic communities such as the British medical sector, as well as the global health organisations leading the latest stage of the process.
Conclusion
This article has introduced resemantisation as an analytical and methodological framework illustrated through the case of the medical resemantisation of MC until the VMMC programme.
This case illustrates how in contrast with approaches that emphasise the correlative emergence of new discourses, practices and socio-political orders, resemantisation helps analyse scenarios where changes within socio-political-normative orders are accompanied by a change of discourse to enable the reproduction of a medical meaning justifying the reproduction of a practice. It also shows the tensions inherent in this process. Although the documents promoting VMMC distinguish between ‘medical’ VMMC and ‘traditional’ MC, they also invoke its cultural significance to vindicate its implementation as an anti-HIV procedure when it serves marketing strategies.
One article alone cannot do justice to all the dimensions through which (VM)MC can contribute to the study of world politics. Questions such as who benefits from the resemantisation of MC within and outside VMMC priority settings, what VMMC reflects about the gendering of international regimes or the role racist tropes and (post)colonialism played in its success fall outside the scope of this article. For further research, it would be valuable to conduct interviews with the intended beneficiaries to see how discourses about VMMC are being understood, reproduced or challenged in priority contexts. Likewise, an analysis of the socio-demographic characteristics of health practitioners promoting VMMC within and outside IOs would provide interesting insights regarding the concomitant remedicalisation of MC within the US and the new wave of transnational medicalisation occurring via the VMMC programme.
Supplemental Material
sj-docx-1-ire-10.1177_00471178241249641 – Supplemental material for The discursive process of resemantisation: how global health discourses turned male circumcision into an anti-HIV policy
Supplemental material, sj-docx-1-ire-10.1177_00471178241249641 for The discursive process of resemantisation: how global health discourses turned male circumcision into an anti-HIV policy by Audrey Alejandro and Joshua Feldman in International Relations
Footnotes
Acknowledgements
We would like to thank Nancy Breton, Gokhan Ciflikli, Chris Deacon, Stefano Guzzini, Jens Steffenk, the three anonymous reviewers, the participants of the ECPR 2021 panel ‘International Organisations through a Discursive Lense: Challenges, Contributions and Emerging Issues’ and the participants of the workshop ‘Objects of expertise I’ for their feedback on previous versions of the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Notes
Author biographies
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.