
Abstract
Under Saudi Arabia’s Vision 2030, public-private partnerships (PPPs) have become a key mechanism for implementing the Health Sector Transformation Program (HSTP). However, limited quantitative evidence identifies which governance capacities stakeholders perceive as most critical to PPP implementation. This study examines how health sector stakeholders assess PPP governance and how key governance dimensions relate to perceived achievement of HSTP objectives. An exploratory cross-sectional survey was conducted among 505 public and private stakeholders in Riyadh with knowledge of healthcare PPPs. A structured questionnaire assessed 3 governance capacities regulatory financial governance, technical capacity, and institutional risk climate and their perceived contribution to HSTP objectives. Data were analyzed using exploratory factor analysis, correlations, and multiple linear regression. Overall perceptions of PPP contributions to HSTP objectives were positive (M = 4.08). Institutional risk climate (M = 4.12) and regulatory financial governance (M = 3.98) were rated positively, whereas technical capacity scored substantially lower (M = 2.75). Greater PPP exposure was associated with more negative technical ratings. Institutional risk climate was the strongest predictor of perceived HSTP goal achievement (β = .795), followed by technical capacity (β = .092) and regulatory financial governance (β = .083). Stable regulation and strong institutional governance were the leading enablers, while unclear contracts and limited specialized expertise were the main barriers. In the Saudi reform context, PPP implementation appears to depend more on institutional governance and public stewardship than on financial structuring alone. Future contracts should include explicit provisions for innovation, knowledge transfer, and workforce development.
Keywords
Introduction
Healthcare systems worldwide are facing persistent and multifactorial pressures, including rising demand for healthcare services, increasing healthcare costs, aging populations, and the increasing burden of chronic disease.1,2 These pressures have prompted discussions among governments about reconsidering traditional models of public service delivery and exploring reform strategies that can balance financial sustainability, service quality, and public accountability. Within this broader reform context, public-private partnerships (PPPs) have become a widely used policy instrument in health systems.
PPPs are commonly defined as long-term contractual arrangements in which public and private actors share responsibilities for financing, developing, managing, or delivering public services under continued public oversight.1,3 In healthcare, PPPs range from infrastructure-focused models such as hospital construction under Design Build Finance Operate schemes to service-based arrangements involving diagnostics, clinical services, facility management, or integrated care provision.4,5 Governments have often adopted PPPs to mobilize private capital, improve operational efficiency, share risks, and introduce managerial expertise, while retaining ultimate responsibility for regulation and stewardship.6-8 PPPs also reshape the relationship between the government and private providers, operating within institutional and regulatory frameworks that determine how risks, responsibilities, and performance expectations are distributed.
International experience shows that the outcomes of healthcare PPPs vary considerably across contexts. In the United Kingdom, the Private Finance Initiative (PFI) facilitated rapid hospital construction and short-term capacity expansion; however, it created long-term fiscal commitments, contractual rigidity, and renegotiation pressures that limited flexibility.9,10 Large-scale infrastructure programs in countries such as Turkey have also raised concerns regarding fiscal exposure and governance complexity.1,11 In contrast, countries such as Canada and Denmark have used PPPs within strong public stewardship frameworks, where partnerships supported coordination and service integration rather than functioning primarily as finance-driven models.6,12 Evidence from middle-income settings including South Africa, India, and Uganda indicates that PPPs can expand access or address service gaps, yet sustainability and performance depend heavily on regulatory capacity and contract management strength.13-15 These contrasting experiences suggest that PPP outcomes are shaped less by contractual design alone and more by institutional and governance conditions. PPP performance is therefore context-dependent rather than inherently efficient “Critical assessments of PFI-type models also caution against treating PPPs as inherently efficiency-enhancing, as weakly governed arrangements may generate long-term fiscal commitments and reduce strategic flexibility in health systems.” 10
Beyond efficiency concerns, healthcare PPPs also raise important questions about institutional capacity, equity, and public value. Because healthcare directly affects population well-being and social legitimacy, distributive consequences are central to evaluating partnerships.1,3 Supporters argue that PPPs can expand capacity and contribute to progress toward universal health coverage, particularly where public systems face resource constraints. 16 Critics, however, warn that market-oriented arrangements may concentrate services in commercially attractive areas, prioritize revenue-generating activities, or shift financial risks onto patients unless equity safeguards are clearly embedded in regulatory and contractual frameworks.17,18 Comparative evidence shows that equity outcomes vary depending on the strength of public oversight and the clarity of regulatory conditions. The equity implications of PPPs remain particularly contested in health systems undergoing structural reform.
A growing body of governance research posits that the performance of PPPs ultimately depends on institutional capacity. Institutional capacity includes the ability of governments to define roles clearly, allocate risks appropriately, enforce contracts, maintain regulatory coherence, and sustain public accountability over time.1,3,19 However, understanding PPP performance requires analysis beyond contractual design alone. Partnerships operate within existing health systems and interact with complex institutional, regulatory, and professional environments. In such settings, the perceptions of policymakers, managers, and health professionals play a critical role in shaping how formal partnership strategies are translated into day-to-day practice.3,20 Collaborative governance research further suggests that gaps between “designed” and “implemented” strategies often depend on whether stakeholders’ interpretations align with stated partnership objectives. 21 In complex sectors such as healthcare, weak risk allocation or poor contract management can undermine partnerships regardless of their financial structure. Conversely, systems with strong stewardship, clear oversight, and aligned stakeholder expectations are better able to connect private participation to system-level objectives such as access, quality, and sustainability.6,12 This perspective reframes PPPs as governance arrangements whose outcomes depend not only on financial design, but also on institutional coherence and stakeholder legitimacy.
These governance demands become more pronounced in countries undertaking large-scale health system reform. In reform-driven contexts, governments often shift from direct service provision toward a stewardship role, focusing on regulation, strategic planning, and performance oversight while engaging private actors in defined operational functions.7,8 PPPs in such settings are embedded within broader institutional restructuring processes rather than implemented as isolated projects. Experience from reform-oriented systems, including the United Arab Emirates, shows that centralized oversight and regulatory alignment are critical to ensuring that PPPs support integration and modernization rather than fragment service delivery.1,22
Saudi Arabia represents one such reform-driven context. Under Vision 2030, PPPs were formally incorporated into the national reform agenda in 2018 as part of a broader strategy to modernize public services. In the health sector, the Health Sector Transformation Program (HSTP), launched in 2020, set out to implement comprehensive system reform aimed at improving quality of care, expanding access and coverage, strengthening financial sustainability, and gradually shifting toward a more preventive and integrated model of service delivery.23,24 Within this framework, PPPs are positioned as strategic instruments for reform implementation rather than as substitutes for public provision or steps toward privatization. The government retains a central leadership role in planning, regulation, and oversight, reflecting a shift toward an enabling state model under strong public stewardship.
Saudi Arabia is analytically distinct because PPPs are being advanced within a centrally steered national transformation agenda, in which Vision 2030 and the HSTP position private participation as an instrument of system reform under continued public stewardship rather than as a stand-alone financing device or an ad hoc privatization measure. This policy configuration creates a specific research gap: despite growing Saudi interest in PPPs, limited quantitative evidence identifies which governance capacities stakeholders perceive as most critical for translating this reform model into health-system outcomes.23,25
Despite extensive global debate on PPP, limited quantitative research identifies which governance capacities most strongly influence PPP implementation within reform-driven health systems. Existing studies predominantly focus on financial efficiency, infrastructure delivery, or high-level policy analysis, with relatively little attention to mechanisms through which distinct governance components translate into practice. In complex institutional settings, PPP effectiveness is determined not solely by formal institutional design but also by how partnership roles, objectives, and boundaries are understood by key system actors. Research on governance and collaborative management indicates that implementation gaps frequently arise when stakeholder expectations are misaligned with reform design.19,21,26 However, quantitative, stakeholder-centered assessments that link governance dimensions to specific reform objectives remain scarce, particularly within large-scale health transformation programs.
This study addresses this gap by examining PPP implementation under the HSTP through a large-scale stakeholder survey. It assesses how key actors perceive core partnership dimensions and analyzes their relationship to system-level reform objectives, including coordinated care, accountability, quality, sustainability, accessibility, and service comprehensiveness. Rather than assuming that PPP design automatically produces reform outcomes, the study organizes partnership dimensions into 3 governance capacities (Regulatory Financial Governance, technical capacity, and institutional risk climate) and assesses how these capacities relate to perceived implementation. Through this analysis of governance capacities, the study advances conceptual clarity, empirical evidence, and policy-relevant insights into the governance conditions under which PPPs are more likely to function as instruments of health system transformation rather than as isolated operational arrangements.
Study Design
This study employed an exploratory, cross-sectional design. A survey-based design was used to collect data from a sample of stakeholders working in both public and private sectors assessing PPP governance dimensions and predictive factors associated with PPP implementation.27,28
Eligible participants comprised policymakers, administrators, healthcare professionals, and decision-makers from organizations engaged in, or knowledgeable about, healthcare PPP projects. These organizations included the Ministry of Health, Private Sector Participation (PSP) units, the National Centre for Privatization and Public-Private Partnership (NCP), the Vision Realization Office (VRO), and private healthcare organizations. Institutions were identified through publicly available official sources and disclosures related to healthcare PPP initiatives.23,29,30 Participants were eligible if they were currently working in these organizations and had direct involvement in, or sufficient knowledge of, PPP-related activities in the health sector. Individuals were excluded if they were not employed in relevant organizations, had no PPP-related role or knowledge, or submitted incomplete questionnaires that could not be used in the analysis.
A purposive convenience sampling strategy was employed to recruit participants possessing relevant knowledge or experience related to PPPs in healthcare. This approach is commonly used in exploratory policy and governance research where specialized expertise is required and probability sampling is not feasible.31,32 Data were collected in Riyadh, the capital city of Saudi Arabia, which houses the headquarters of national health authorities, regulatory agencies, and major public and private healthcare organizations. Data collection was conducted from April to October 2024, allowing sufficient time to recruit respondents across different institutional settings.
The questionnaire was distributed electronically via professional networks and targeted institutional emails. Out of ~800 distributed surveys, a total of 505 respondents completed the questionnaires, yielding an estimated response rate of 63%. Based on Krejcie and Morgan’s sample size determination, a minimum of 384 participants was required. 33 Thus, the sample of 505 exceeded the minimum requirement, ensuring adequate statistical power for multivariate analyses. While the recruitment strategy successfully targeted experts, it naturally resulted in a high proportion of respondents with prior PPP experience.
This cross-sectional survey is reported in accordance with the STROBE guideline for observational studies, and a completed STROBE checklist is provided as a (Supplementary File 1). 34
Ethical approval was obtained from the Institutional Review Board (approval reference no: KSU-HE-23-947; approval date: October 10, 2023). All procedures complied with ethical standards for research involving human participants. Informed consent was obtained electronically from all participants through a mandatory consent checkbox (agree/yes) before accessing the questionnaire. Participants were also informed of confidentiality and their right to withdraw at any time. 35
Instrument Development
A structured, self-administered questionnaire was developed based on a comprehensive review of the literature and a conceptual framework grounded in established theories of public management and governance, including New Public Management (NPM), Institutional Theory, Risk Governance Theory, and Governance Theory.6-8,19,25,36 These theoretical perspectives guided the identification of key constructs proposed by Hodge and Greve. 37
Initially, the questionnaire included items addressing participants’ demographic and professional characteristics. The questionnaire was designed to capture stakeholder perceptions across 5 core PPP dimensions: the financial dimension, the legislative and regulatory dimension, risk mitigation, the technical dimension, and the institutional dimension. Items within each dimension were measured using a 5-point Likert scale ranging from strongly disagree (1) to strongly agree (5), capturing perceptions of resource adequacy, regulatory clarity, accountability, risk allocation, technical capacity, and institutional coordination.
A separate section of the questionnaire assessed perceived PPP contributions to the 8 HSTP objectives of the Saudi healthcare system, including accessibility, coverage, quality, sustainability and continuity of care, patient-centeredness, coordinated care, accountability, and service comprehensiveness. These items are consistent with the Saudi Vision 2030 priorities and were also measured using a 5-point Likert scale.1,23 Additionally, the questionnaire examined enabling factors associated with PPP success, perceived barriers to effective PPP implementation, and opportunities for future PPP collaboration, thereby providing a multi-stakeholder assessment of PPP performance.
The questionnaire used in this study is provided as Supplementary File 2. Content validity and reliability of the questionnaire were established through expert review by specialists in healthcare management and public-private partnerships. Instrument reliability was also assessed using Cronbach’s alpha, which demonstrated acceptable internal consistency for the full instrument (α = .89). 27 Following factor consolidation, Cronbach’s alpha values for the empirically derived PPP governance capacities and the HSTP objectives scale are reported in (Table 1).To examine the underlying structure of the conceptually related PPP dimensions and support the derivation of composite governance measures, an Exploratory Factor Analysis (EFA) was conducted prior to regression modeling. The Kaiser-Meyer-Olkin (KMO) measure indicated excellent sampling adequacy (KMO = 0.937), and Bartlett’s Test of Sphericity was statistically significant (χ2 (276) = 12 305.64, P < .001). EFA using Principal Axis Factoring with Oblimin rotation retained 3 factors with eigenvalues >1, explaining 72.44% of the total variance. The factor loading pattern supported the consolidation of the originally theorized 5 dimensions into 3 empirically derived governance capacities (Supplementary Table S1).
Descriptive Statistics of Governance Capacities and HSTP Goals.

Data Analysis
Data were analyzed using SPSS software (version 22). Descriptive statistics were computed to describe participants’ demographic, professional, and organizational characteristics, as well as overall patterns in perceptions of PPP dimensions and HSTP outcomes. Categorical variables were reported as frequencies and percentages, while continuous variables were reported using means and standard deviations.
To examine differences in PPP perceptions across stakeholder characteristics, independent sample t-tests and 1-way analysis of variance (ANOVA) were conducted. Given the ordinal nature of Likert-scale data and the exploratory aim of identifying initial associations, Spearman’s rank-order correlation analysis was performed to assess the direction and strength of relationships between PPP dimensions and HSTP objectives.
Subsequently, multiple linear regression analysis was employed to determine the independent predictive contribution of the PPP dimensions to each HSTP outcome. Although the individual questionnaire items were ordinal, composite scores for each dimension were calculated as means, justifying their treatment as continuous interval-level variables for regression analysis—a standard practice in social science research.
This combined approach allowed for the simultaneous evaluation of multiple predictors while controlling for their interrelationships. Model fit was evaluated using R2 values, and standardized regression coefficients (β) were reported to facilitate the comparison of effect sizes across predictors. Statistical significance was assessed using a 2-tailed P value threshold of P < .05. Only completed questionnaires were included in the final analysis. Missing item responses were minimal and were therefore not imputed.
Results
Participant characteristics are summarized in Supplementary Table S2. The study sample was predominantly from the public health sector (69.1%), with the remaining 30.9% representing private-sector stakeholders. This public-sector weighting is consistent with the broader Saudi health system context, in which public institutions continue to play a leading role in healthcare provision and oversight despite increasing private-sector participation under Vision 2030. 29
Most participants held a bachelor’s degree or lower (76.6%) and were Saudi nationals (88.7%). Approximately two-thirds were employed in health-related roles (65.5%), with the majority occupying middle management positions (65.3%). A high proportion reported prior experience with PPP arrangements (60.0%), and more than two-thirds had participated in at least 1 PPP project, indicating that the sample comprised sufficiently experienced stakeholders to provide informed assessments of partnerships’ role in supporting health system transformation.
As detailed in the methodology, an Exploratory Factor Analysis consolidated the originally theorized 5 PPP dimensions into 3 derived governance capacities: regulatory financial governance, technical capacity, and institutional risk climate. Participants’ overall perceptions of these capacities and the HSTP objectives are presented in Table 1. Stakeholders evaluated the institutional risk climate (M = 4.12, SD = 0.71) and regulatory financial governance (M = 3.98, SD = 0.82) positively, indicating generally favorable assessments of oversight, risk management, and financial structuring within the Saudi health sector. In contrast, the technical capacity dimension received a substantially lower mean score (M = 2.75, SD = 1.24), reflecting more cautious perceptions regarding PPPs’ current contribution to technological innovation and skills development. Participants also reported strong agreement that PPPs contribute to the achievement of overall HSTP objectives (M = 4.08, SD = 0.75).
Differences in perceptions across stakeholder characteristics are presented in Supplementary Table S3. Overall, the findings indicate a high degree of convergence between public and private sector participants, with no substantive sectoral divergence observed for either regulatory-financial governance or institutional risk climate. However, significant differences emerged across levels of professional experience and prior PPP project exposure. Notably, stakeholder ratings of the technical capacity dimension showed a counterintuitive gradient by level of PPP exposure: respondents involved in more than 3 projects reported substantially lower technical ratings (M = 1.93, SD = 0.88) compared to those involved in 1 to 3 projects (M = 2.94, SD = 1.22) or those with no prior experience (M = 2.54, SD = 1.23). This pattern aligns with the statistically significant negative association between years of professional experience and technical capacity perceptions (r = −0.225, P < .001), suggesting that repeated hands-on project involvement may foster more critical evaluations as practitioners gain direct exposure to the operational limitations of current PPP contracts, which tend to prioritize service delivery over structured technical upgrading and knowledge transfer.
Spearman’s rank-order correlation analysis, presented in Table 2, further clarifies these associations. Both institutional risk climate (r = 0.838, P < .001) and regulatory-financial governance (r = 0.819, P < .001) demonstrated strong, positive, and statistically significant associations with overall HSTP objectives, and were also highly correlated with each other (r = 0.858, P < .001), reflecting their conceptual and practical alignment within the broader governance structure. In contrast, the technical capacity dimension exhibited a weak and non-significant negative correlation with the overall achievement of HSTP objectives (r = −0.037, P = .402), suggesting that current technical arrangements operate largely independently of the principal institutional and financial determinants of perceived health system transformation.
Spearman’s Rank-Order Correlations Between PPP Governance Capacities and Overall HSTP Goal Achievement.
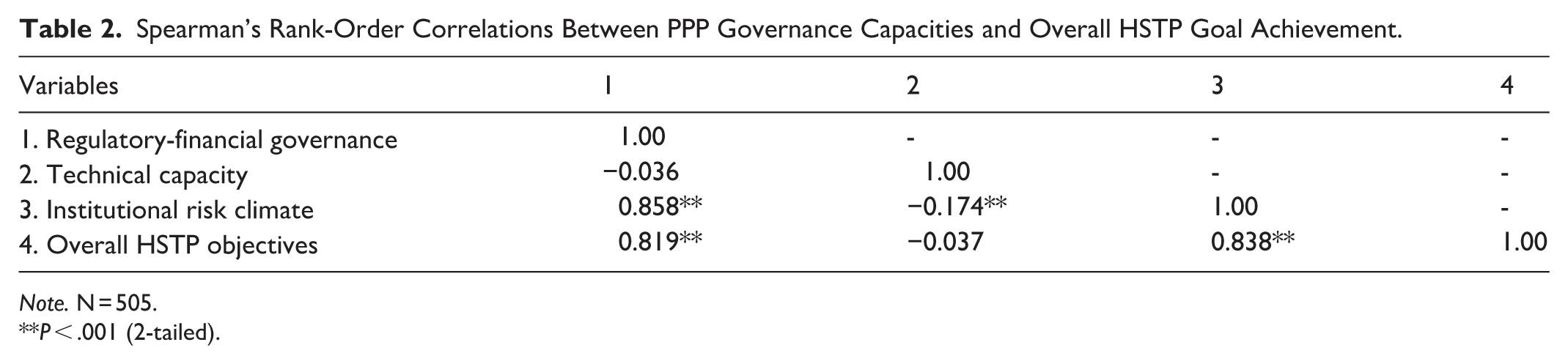
Note. N = 505.
P < .001 (2-tailed).
To determine the independent predictive contribution of the 3 governance capacities, a multiple linear regression analysis was conducted (Table 3). Prior to interpretation, diagnostic tests confirmed that multicollinearity was not a significant concern, with variance inflation factor (VIF) values ranging from 1.06 to 3.34, well below the standard threshold of 5. The overall regression model was statistically significant (F (3, 501) = 469.48, P < .001) and explained a substantial proportion (73.8%) of the variance in perceived HSTP goal achievement (R2 = 0.738, adjusted R2 = 0.736). Institutional risk climate emerged as the strongest and most significant predictor (beta = .795, P < .001), followed by technical capacity (beta = .092, P < .001) and regulatory-financial governance (beta = .083, P = .045). While all 3 dimensions achieved statistical significance, the standardized coefficients indicate that the practical contribution of technical capacity and regulatory-financial governance was substantially smaller relative to institutional risk climate, reinforcing the primacy of governance quality and oversight coherence as the principal determinants of perceived PPP implementation in the Saudi health reform context.
Standardized Regression Coefficients (β) for the Predictive Effects of PPP Governance Dimensions on HSTP Goal Achievement.

Note. N = 505, dependent variable: overall HSTP objectives. R2 = 0.738; adjusted R2 = 0.736; F (3, 501) = 469.48, (P < .001).
B = , unstandardized coefficient; SE = standard error; β = standardized coefficient; VIF = variance inflation factor.
P < .05. **P < .001.
Finally, Supplementary Table S4 presents key enablers, barriers, and preferred application areas for PPPs in the Saudi health sector. The presence of a stable regulatory environment (75.2%) and strong institutional governance (74.2%) were perceived as the most critical enablers of partnership success. Conversely, the absence of clear and standardized contracts (62.5%) and the limited availability of specialized healthcare expertise (56.6%) were identified as the primary implementation barriers. Regarding preferred application areas, stakeholders expressed the strongest preference for PPPs oriented toward primary health care provision (73.0%) and hospital operations management (68.7%), while technology and innovation-focused models were rated comparatively less favorably, a finding that resonates with the broader pattern of lower technical capacity scores observed across the analytical results.
Discussion
The findings of this study suggest that, at the level of stakeholder perceptions, the implementation of public-private partnerships (PPPs) in the Saudi health sector is conceptualized primarily as a function of institutional governance rather than financial structuring or operational outsourcing. Among the 3 PPP governance dimensions examined, institutional risk climate demonstrated the strongest association with perceived achievement of HSTP objectives and the largest independent contribution in the multivariate models. This pattern indicates that respondents chiefly link PPP performance to regulatory stability, clarity of roles, coordinated public stewardship, and structured risk governance, rather than to contractual form or funding modality alone.
This governance‑centered interpretation is consistent with PPP scholarship that conceptualizes partnerships as complex institutional arrangements whose perceived performance depends on their capacity to generate public value and support policy objectives, rather than merely mobilize capital or transfer risk.1,3,6 Comparable perception‑based patterns have been documented in institutionally anchored systems such as Canada, Denmark, and the United Arab Emirates, where PPPs operate within structured public oversight frameworks and are directed toward system‑level integration rather than market substitution.12,22,38 Furthermore, within the Saudi context, these findings build upon recent evaluations 39 by quantitatively demonstrating that perceived institutional strength in coordinating actors and managing operational risks is the primary perceptual anchor for stakeholders evaluating PPPs under Vision 2030.
Collectively, these findings indicate that institutional risk climate constitutes the main platform through which PPPs are understood to safeguard continuity, accountability, and public value.
In contrast, technical capacity exhibits a comparatively limited association with perceived reform achievement in the Saudi health PPP context. Respondents assigned this dimension the lowest overall evaluation, and it did not show a significant bivariate correlation with HSTP objectives, although it retained a statistically significant but substantively small independent contribution in the multivariate models. Substantively, these results suggest that existing PPP arrangements are perceived primarily as instruments of operational stabilization and service delivery rather than as vehicles for technological transformation or structured knowledge transfer.3,25,37,40 This perception is heavily reinforced by the counterintuitive gradient observed among respondents: stakeholders with the most extensive practical exposure to PPPs (involvement in more than 3 projects) rated the technical dimension substantially lower than those with less experience. This divergence suggests that while less-exposed observers may hold aspirational expectations about private sector innovation, repeated hands-on involvement exposes the operational reality that current contracts lack structured technical capacity-building.1,39,40
This perception is consistent with established PPP literature, which emphasizes that technical upgrading and innovation do not arise automatically from private sector participation but depend on contractual architectures that explicitly embed measurable innovation targets, performance‑based digital indicators, and enforceable mechanisms for skills transfer.1,34,38 Comparative evidence from Iran, Pakistan, Malaysia, and Turkey similarly reports operational improvements without substantive technological upgrading where contracts lacked explicit technology‑transfer commitments.11,14,41 Stakeholders’ identification of “limited specialized expertise” and “contract ambiguity” as primary implementation barriers reinforces the interpretation that technical transformation within Saudi health PPPs should be viewed as a contingent outcome requiring deliberate policy intent and future contract design.
The regulatory-financial governance dimension demonstrated a statistically significant yet comparatively modest independent effect in the multivariate analysis, despite exhibiting a stronger bivariate association with perceived HSTP achievement. This suggests that the perceived contribution of financial structuring and regulatory frameworks is closely intertwined with broader governance capacities. In other words, stakeholders appear to regard finance and regulation as essential enabling conditions for PPP implementation, but not as autonomous engines of reform once institutional risk climate is taken into account.1,6 Within this integrated perspective, financial arrangements are interpreted less as mechanisms for short-term cost reduction and more as instruments for resource mobilization, long-term fiscal planning, and continuity of service provision under structured oversight.9,15 Regulatory architecture, in turn, appears to contribute through predictability and procedural clarity, yet regulation alone does not seem to generate reform momentum unless embedded within a coherent institutional structure.19,20
Taken together, these perception-based results help explain the differentiated pattern of perceived contributions across HSTP objectives. Institutional risk climate appears most closely aligned with system‑level objectives related to coordination, accountability, continuity of care, and long‑term sustainability. Regulatory-financial governance is perceived to support resource mobilization and fiscal continuity, while the comparatively modest contribution of technical capacity suggests that innovation‑oriented ambitions remain contingent upon future contractual development. This configuration is broadly consistent with international patterns in which health PPPs initially contribute to access expansion and operational consolidation before deeper technological upgrading emerges.1,3,12 Within this comparative landscape, the Saudi case appears to follow a governance‑sequenced reform trajectory in which institutional consolidation and fiscal stabilization precede deeper technological transformation.
The findings of this study, viewed through the lens of international best practices, offer 3 actionable policy implications for the design and execution of future health PPPs in Saudi Arabia. First, embedding technical capacity and knowledge transfer into contracts, the persistent underperformance of the technical dimension necessitates a strategic shift in PPP contract design. Policymakers should transition from generic service-level agreements to incorporating mandatory, measurable key performance indicators (KPIs) linked to technology localization, digital health integration, and joint workforce training.3,39,40 As demonstrated in successful models and advocated by international development agencies, specific contractual mechanisms such as “knowledge transfer clauses,” explicit technology deployment quotas, and structured penalties for failing to upskill the local workforce are essential to convert private sector operational expertise into sustainable public sector capacity.
Second, strengthening institutional oversight and contractual flexibility, the predictive dominance of the institutional risk climate underscores the necessity for robust public stewardship. The Ministry of Health and related commissioning entities must ensure that “payment security” mechanisms and clear risk-sharing protocols are explicitly defined to maintain long-term private sector confidence. 23 Furthermore, adopting “contractual flexibility,” a critical success factor identified in World Bank evaluations, will allow long-term PPP agreements to be reviewed and adjusted periodically. 16 This adaptability is vital to mitigate the risks of rigid regulatory constraints that this study found to occasionally hinder implementation agility.
Finally, enhancing monitoring and evaluation for equity and quality, to move beyond operational outputs, the Saudi health sector must develop comprehensive monitoring and evaluation systems that track the long-term impact of PPPs on clinical outcomes and health equity. 18 While this study captured perceptions largely from Riyadh-based stakeholders reflecting the administrative and commercial hub where PPP implementation is currently concentrated, national policy frameworks should explicitly safeguard equitable access. Future governance frameworks should mandate that PPP operators report on service accessibility and coverage for underserved and non-urban populations, ensuring that the drive for private investment does not compromise the HSTP’s core objective of universal, equitable health coverage across all geographic regions.23,42
This study has several limitations that inform directions for future research. First, the reliance on perceptual data from a purposive sample of predominantly Riyadh-based stakeholders may introduce geographic bias, limiting the direct generalizability of the findings to rural or peripheral health clusters where PPP infrastructure and equity challenges differ significantly. Second, while the integration of Exploratory Factor Analysis and regression modeling effectively addressed structural overlap and multicollinearity among the governance dimensions, the cross-sectional nature of the data precludes causal inferences. Future longitudinal research should move beyond perceptual metrics by triangulating stakeholder assessments with objective performance indicators such as cost-efficiency ratios, clinical quality metrics, and spatial access rates to comprehensively evaluate the transformative impact and geographic equity of PPPs over time.
Conclusion
This study provides evidence that the perceived implementation of PPPs in advancing Saudi Arabia’s HSTP is fundamentally contingent upon institutional governance rather than solely on financial outsourcing mechanisms. Stakeholders consistently identify the institutional risk climate encompassing regulatory stability, clear risk allocation, and structured public stewardship as the primary driver of PPP success. Rather than being perceived solely as market-based instruments, PPPs are understood as coordinated public-private governance arrangements operating within a centrally steered agenda. To fully realize Vision 2030s ambitions, future PPP configurations must extend beyond operational stabilization to explicitly mandate technological innovation through actionable contract design, while ensuring that robust oversight mechanisms safeguard geographic equity in healthcare access.
Supplemental Material
sj-doc-3-inq-10.1177_00469580261444278 – Supplemental material for Public-Private Partnership Governance in Health System Transformation: Stakeholder Evidence From Saudi Arabia’s Vision 2030
Supplemental material, sj-doc-3-inq-10.1177_00469580261444278 for Public-Private Partnership Governance in Health System Transformation: Stakeholder Evidence From Saudi Arabia’s Vision 2030 by Nada Abdullah Alsubki and Saad Abdullah Alghanim in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580261444278 – Supplemental material for Public-Private Partnership Governance in Health System Transformation: Stakeholder Evidence From Saudi Arabia’s Vision 2030
Supplemental material, sj-docx-2-inq-10.1177_00469580261444278 for Public-Private Partnership Governance in Health System Transformation: Stakeholder Evidence From Saudi Arabia’s Vision 2030 by Nada Abdullah Alsubki and Saad Abdullah Alghanim in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-1-inq-10.1177_00469580261444278 – Supplemental material for Public-Private Partnership Governance in Health System Transformation: Stakeholder Evidence From Saudi Arabia’s Vision 2030
Supplemental material, sj-pdf-1-inq-10.1177_00469580261444278 for Public-Private Partnership Governance in Health System Transformation: Stakeholder Evidence From Saudi Arabia’s Vision 2030 by Nada Abdullah Alsubki and Saad Abdullah Alghanim in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors thank the participating institutions and stakeholders for their time and valuable insights, and acknowledge the support of King Saud University in facilitating this research.
Ethical Considerations
This study was approved by the Institutional Review Board of King Saud University (approval number KSU-HE-23-947) on October 10, 2023.
Author Contributions
Nada Abdullah Alsubki: conceptualization, study design, data collection, data analysis and interpretation, drafting of the manuscript, and critical revision for important intellectual content. Saad Abdullah Alghanim: methodological guidance, supervision, interpretation of findings, and critical revision of the manuscript for important intellectual content.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.