
Abstract
The Affordable Care Act (ACA) allowed states to expand Medicaid eligibility, potentially improving access to care and reducing psychological distress among lower-income adults. However, evidence on population-level mental health effects remains mixed, and conventional two-way fixed-effects difference-in-differences (DiD) estimates can be biased under staggered adoption. This study estimates the effect of Medicaid expansion on frequent mental distress (FMD) among non-elderly adults, with emphasis on lower-income adults. We used Behavioral Risk Factor Surveillance System (BRFSS) data from 2011 to 2024 and restricted the sample to adults aged 18 to 64 years. FMD was defined as ≥14 days of poor mental health in the past 30 days. Medicaid expansion was assigned by state implementation year. For transparent weighting and computational feasibility, we collapsed microdata to state-year prevalence using BRFSS survey weights and applied prespecified minimum cell-size and effective-sample screens (lower-income panel: unweighted N ≥ 150 and Kish n_eff ≥ 50; pooled and higher-income panels: n_eff ≥ 200). We estimated group-time average treatment effects using the Callaway–Sant’Anna staggered DiD framework (csdid), clustered standard errors at the state level, and used pair-balanced observations when panels were unbalanced. Income strata were defined using BRFSS household income categories (lower-income: inc_cat = 1; higher-income: inc_cat ∈ {7,8}) and are interpreted as economic-status proxies rather than Medicaid eligibility. In the lower-income state-year panel (353 state-years), Medicaid expansion was not associated with a statistically significant change in FMD (ATT −0.0125; 95% CI −0.0521 to 0.0271; P = .54). Estimates in the higher-income (656 state-years) and pooled (709 state-years) panels were similarly small and not statistically significant. Event-time estimates indicated modest heterogeneity at selected leads/lags without a consistent post-expansion pattern. Medicaid expansion was not associated with significant reductions in population-level frequent mental distress during 2011 to 2024. Any mental health effects appear modest and heterogeneous across cohorts and follow-up periods, suggesting that insurance expansion alone may be insufficient to shift population psychological distress without complementary behavioral health capacity and upstream social supports.
Plain Language Summary
Medicaid expansion under the Affordable Care Act increased health insurance coverage for many low-income adults, which could improve mental health by reducing financial stress and improving access to care. We studied whether Medicaid expansion changed the share of adults reporting “frequent mental distress,” defined as 14 or more days of poor mental health in the past 30 days. Using BRFSS data from 2011–2024, we compared changes in frequent mental distress in states that expanded Medicaid to changes in states that had not yet expanded at the same time. Because states expanded in different years, we used an approach designed for staggered policy adoption and estimated effects separately for low-income, high-income, and all adults aged 18–64. Overall, average effects were small and not statistically distinguishable from zero, although some expansion cohorts showed statistically significant changes in certain years after expansion. These results suggest that Medicaid expansion alone may have limited population-level effects on frequent mental distress.
Keywords
Introduction
Mental health conditions are a major source of disability and impaired functioning and carry substantial economic consequences. Prior work has argued that commonly used burden-of-disease frameworks understate the population burden attributable to mental illness, and U.S. cost-of-illness estimates for major depressive disorder indicate large and growing economic impacts over time.1,2 In the United States, psychological distress is also closely tied to labor market outcomes, household finances, and health care use, channels that may be affected by health insurance coverage and affordability.
The Affordable Care Act (ACA) Medicaid expansion was designed to increase coverage for lower-income adults, reduce out-of-pocket spending, and improve access to care. These mechanisms could influence mental health by reducing financial strain, improving access to behavioral health services, and enhancing continuity of care. However, Medicaid expansion was implemented at different times across states, resulting in a staggered policy rollout. This staggered timing matters because standard two-way fixed-effects difference-in-differences (TWFE DiD) estimators can be difficult to interpret when treatment effects vary across cohorts or over time, both plausible for mental health outcomes under a multi-year rollout.
Evidence and Gap
Prior studies have examined Medicaid expansion and patient-reported mental health using BRFSS and other surveys, but inference can be sensitive to estimator choice under staggered adoption and treatment-effect heterogeneity. 3 A meaningful share of the prior literature relies on TWFE DiD specifications that can be sensitive to staggered timing and heterogeneous effects. In addition, less work has used a consistent public health surveillance outcome over an extended time horizon while also applying estimators designed for staggered adoption. Frequent mental distress (FMD), defined as reporting ≥14 days of poor mental health in the past 30 days, offers a standardized surveillance outcome that can capture population-level changes, including subclinical distress.
Contribution
This study evaluates the association between Medicaid expansion and FMD using (1) the Callaway–Sant’Anna staggered DiD framework (implemented via csdid), designed for staggered adoption; (2) pooled estimates for adults aged 18 to 64 and income-stratified estimates using BRFSS income categories (economic-status proxies, not eligibility-defined groups), aligned with the analytic panels used in the replication workflow; and (3) BRFSS-based FMD as the primary outcome over 2011 to 2024.
Objective
To estimate the effect of state Medicaid expansion on the prevalence of frequent mental distress among non-elderly adults, with emphasis on lower-income adults, and to compare results against higher-income and pooled 18 to 64 panels.
Hypotheses
• Primary (lower-income): Medicaid expansion reduces frequent mental distress among lower-income adults (ATT < 0).
• Secondary: Effects are smaller (closer to zero) among higher-income adults and in pooled analyses.
• Heterogeneity: Effects vary across expansion cohorts and time since expansion.
Methods
Study Design, Setting, and Reporting Guidelines
We conducted a retrospective repeated cross-sectional observational study using BRFSS survey microdata aggregated into a state-year panel. The study setting was the United States (50 states and participating territories), and the analytic period spanned 2011 to 2024. This manuscript was prepared in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline for cross-sectional studies; the completed STROBE checklist is provided as a Supplemental File. 4
Data Source and Analytic Sample
We used Behavioral Risk Factor Surveillance System (BRFSS) microdata from 2011 to 2024, a nationally representative, state-based survey of U.S. adults. 5 We restricted analyses to adults aged 18 to 64 years. We excluded observations with missing outcome data or with survey weights that were missing or nonpositive. BRFSS weighting procedures follow established national methods.
Sample Size Justification (and Power)
We used all available BRFSS respondents who met the eligibility criteria for 2011 to 2024 to maximize precision and generalizability, rather than selecting a subset. Because this is a secondary analysis of an existing surveillance system with a very large sample, a formal a priori power/sample-size calculation was not performed; we note this as a limitation in the Discussion. Precision was additionally managed using prespecified effective-sample-size screens at the state-year level (see below).
Outcome: Frequent Mental Distress
The primary outcome was frequent mental distress (FMD), defined as reporting ≥ 14 days in the past 30 days when mental health was “not good” (eg, stress, depression, or emotional problems). We aggregated the outcome to the state-year level as the survey-weighted prevalence.
Exposure: Medicaid Expansion Timing
The exposure was Medicaid expansion implementation, defined using each state’s expansion year (expand_year). States were treated beginning in their year of expansion and in all subsequent years. State-years with expand_year =
Income Stratification (Economic-Status Proxy, Not Eligibility)
Income strata were constructed using BRFSS household income categories (inc_cat) as proxies for economic status, not Medicaid eligibility. Constructing the percent of the federal poverty level (%FPL) would require combining income with household size and year-specific poverty thresholds; this was not implemented in the main specification.
For the primary income-stratified analyses, the lower-income panel included respondents with non-missing income in the lowest category (inc_cat = 1; <$15 000). The higher-income panel included respondents with non-missing income in the highest categories (inc_cat
Covariates and Missing-Data Handling
Because estimation was conducted on state-year panels, covariates were entered as state-year survey-weighted shares: female, Black, Hispanic, less than high school education, employed, and married. To match the replication workflow, covariate values were zero-imputed when missing, and corresponding missingness shares (state-year weighted proportions missing for each covariate) were included as controls. In pooled 18 to 64 models, we additionally controlled for (i) the share in the lowest income category among respondents with non-missing income and (ii) the share with missing income to mitigate confounding from time-varying sample composition.
Panel Construction and Precision Screens
For computational feasibility and transparent weighting, we collapsed microdata to the state-year level using BRFSS survey weights.5,6 For each state-year, we computed the Kish effective sample size,
To reduce instability from sparse cells, we applied prespecified screening thresholds: in the lower-income panel, we required an unweighted N ≥ 150 and
Statistical Analysis
We used a staggered difference-in-differences design that leverages variation in Medicaid expansion timing across states, estimating group–time average treatment effects and aggregating these effects across cohorts and time. 8 To avoid known interpretational issues with conventional two-way fixed effects under staggered adoption and treatment-effect heterogeneity, 9 we implemented the Callaway–Sant’Anna estimator using csdid in Stata. 10
Identification relies on a conditional parallel trends assumption given the included covariates. 11 We reported the overall average treatment effect on the treated (ATT) and examined dynamic patterns using event-time (event-study) estimates. Under staggered adoption, event-time coefficients represent weighted averages of cohort-specific effects, and the contributing cohorts can vary across event times in unbalanced panels; we therefore interpret event-time plots as summaries of identified ATT(g,t) patterns rather than a single common dynamic effect.
Inference and Unbalanced Panels
Standard errors were clustered at the state level to account for within-state serial correlation. When panels were unbalanced, csdid used pair-balanced observations in its implementation.
Dynamic and Cohort-Specific Effects
We summarized results using the overall average treatment effect on the treated (ATT) and examined dynamic (event-time) patterns using csdid event-study outputs. Under staggered adoption, event-time coefficients are weighted averages of cohort-specific effects at each relative time, and the set of contributing cohorts can vary across event times when panels are unbalanced.12,13 We therefore interpret event-study and cohort figures as summaries of identified ATT(g,t) patterns rather than as a single common dynamic effect. 14
Robustness and Placebo
As robustness checks, we re-estimated the ATT under alternative specifications that (i) omit all covariates (“unadjusted”), (ii) exclude state-years with high covariate missingness (any covariate missingness share > 50% based on the analysis screen), and (iii) implement a placebo design assigning a pseudo-adoption year of 2014 to ever-treated states (0 for never-treated), holding the estimator and clustering constant.
Ethics and Informed Consent Statement
All procedures were reviewed by the Institutional Review Board (IRB) at New York Medical College (IRB #29761). BRFSS obtained informed consent from participants during survey administration. The present study is a secondary analysis of de-identified, publicly available BRFSS data and involved no direct interaction with participants and no access to identifiable information; therefore, no additional written informed consent was obtained for this secondary analysis.
Software
All analyses were conducted in Stata (StataCorp LLC, College Station, TX). Staggered DiD estimates were implemented using the csdid package; all data management and panel construction were performed in Stata.
Results
Analytic Panels and Coverage
After constructing state-year panels from BRFSS microdata and applying the prespecified sample-size/effective-sample screens, the final estimation samples included 353 state-years in the low-income panel, 656 state-years in the high-income panel, and 709 state-years in the pooled ages 18 to 64 panel. In each panel, states contributed observations as “treated” beginning in their Medicaid expansion year and thereafter; state-years with expand_year = 0 served as the never-expanded comparison group within the study window. Because income was missing for all observations in 2022 in our analytic extract, the income-stratified panels exclude 2022 by construction.
Panel definitions: lower-income = inc_cat=1; higher-income = inc_cat ∈ {7,8}; pooled = all respondents aged 18 to 64 with additional controls for income composition and income missingness.
Pooled Average Effects (Overall ATT)
Across panels, the pooled average treatment effect on the treated (ATT) was small and not statistically indistinguishable from zero (Tables 1 and 2 and Appendix Table A1): In the lower-income panel, the estimated ATT was −0.0125 (95% CI −0.0521 to 0.0271; P = .54). Estimates were similarly near zero in the higher-income panel (0.0006, P = .86) and pooled panel (0.0020, P = .67). Interpreted in percentage-point units, the pooled estimate corresponds to an approximately 0.2 percentage-point change in FMD after expansion, with the confidence interval spanning small decreases and small increases.
Overall Average Treatment Effect on the Treated (ATT) of Medicaid Expansion on Frequent Mental Distress (FMD), by Analytic Panel.

Note. Outcome is state-year FMD prevalence (≥14 mentally unhealthy days in the past 30 days), constructed from BRFSS microdata using survey weights and collapsed to the state-year level. Effects are reported in percentage-point units. Interpretation: In the pooled 18 to 64 analysis, the point estimate indicates an increase of approximately 0.2 percentage points in FMD following expansion, but the confidence interval includes both small decreases and small increases. Higher-income defined as inc_cat∈{7,8}.
Compact Event-Study Estimates of Medicaid Expansion Effects on Frequent Mental Distress (FMD), Selected Event Times, by Analytic Panel.
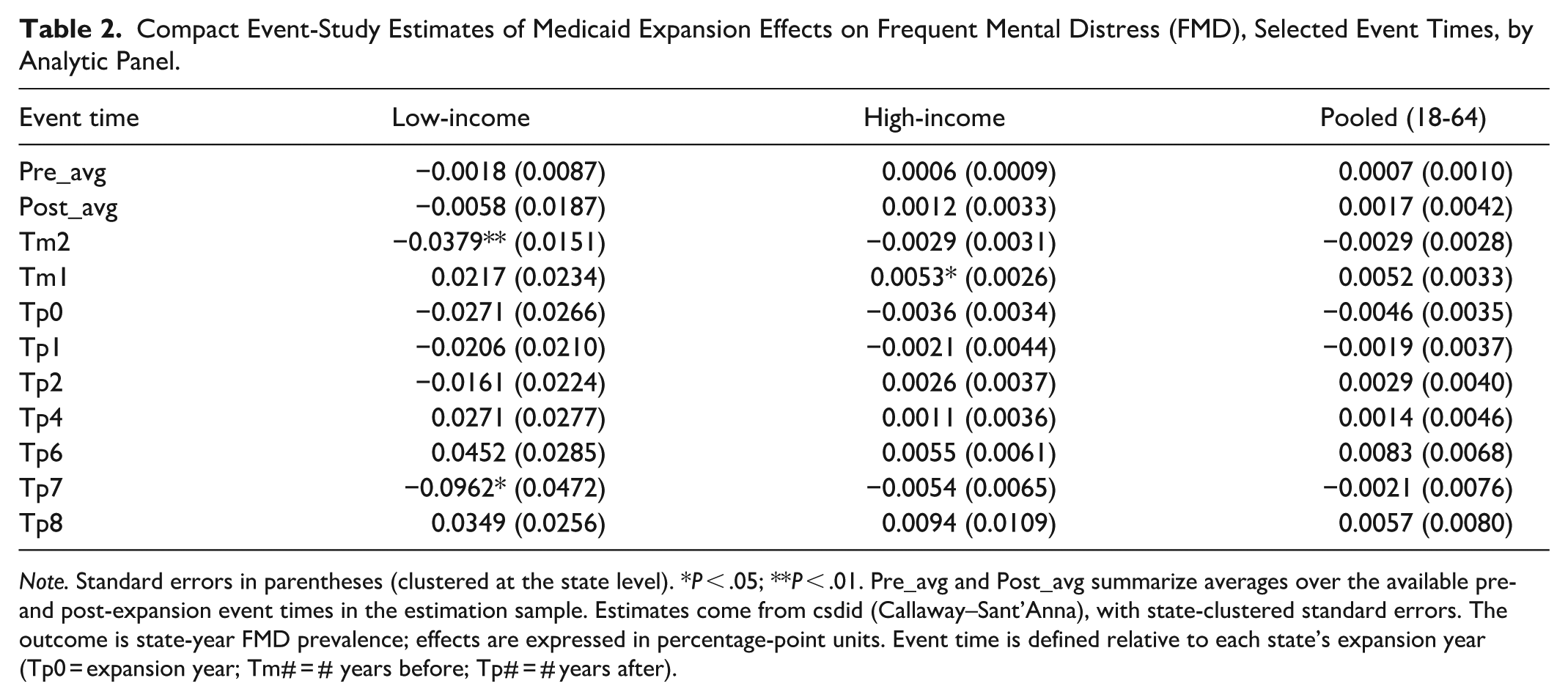
Note. Standard errors in parentheses (clustered at the state level). *P < .05; **P < .01. Pre_avg and Post_avg summarize averages over the available pre- and post-expansion event times in the estimation sample. Estimates come from csdid (Callaway–Sant’Anna), with state-clustered standard errors. The outcome is state-year FMD prevalence; effects are expressed in percentage-point units. Event time is defined relative to each state’s expansion year (Tp0 = expansion year; Tm# = # years before; Tp# = # years after).
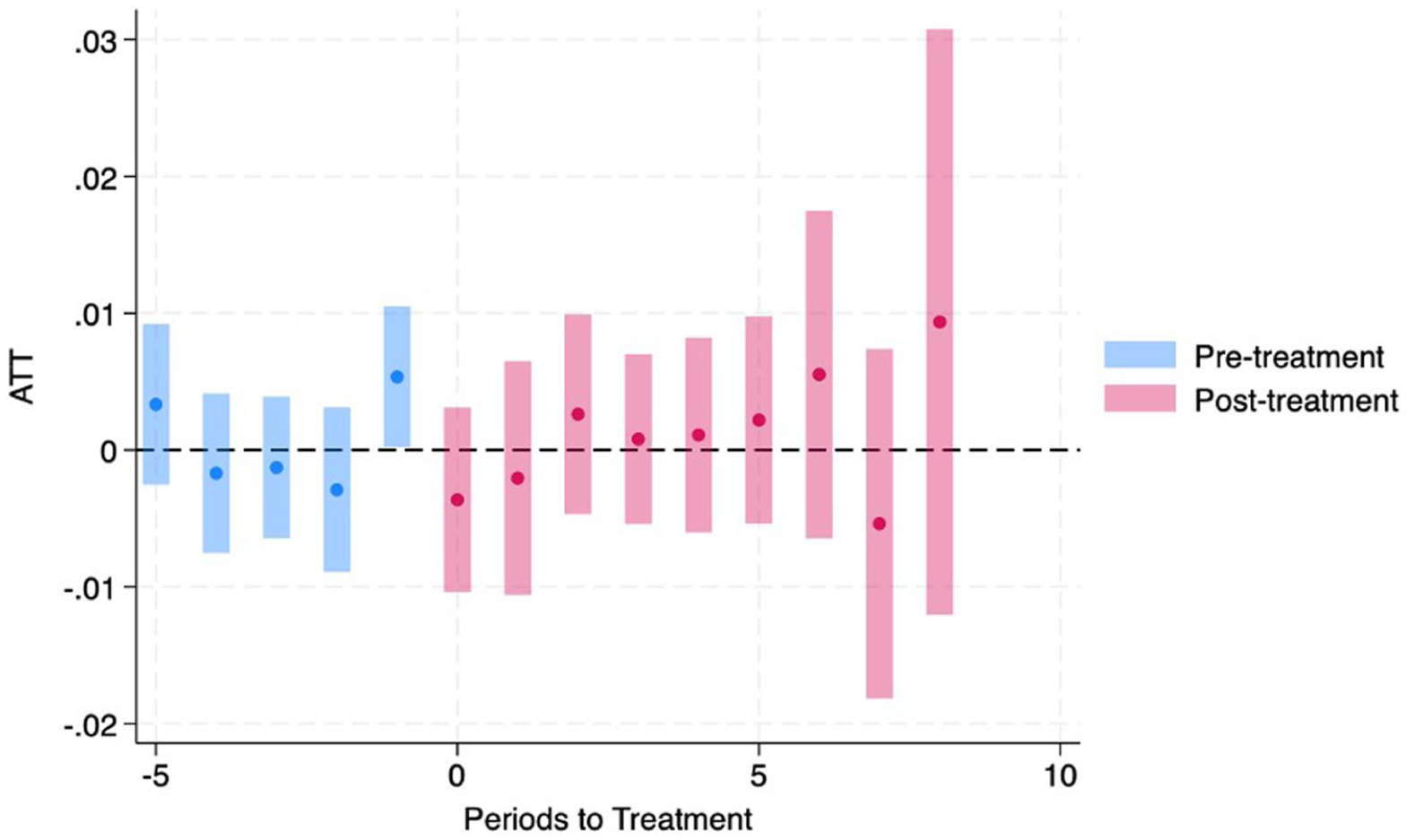
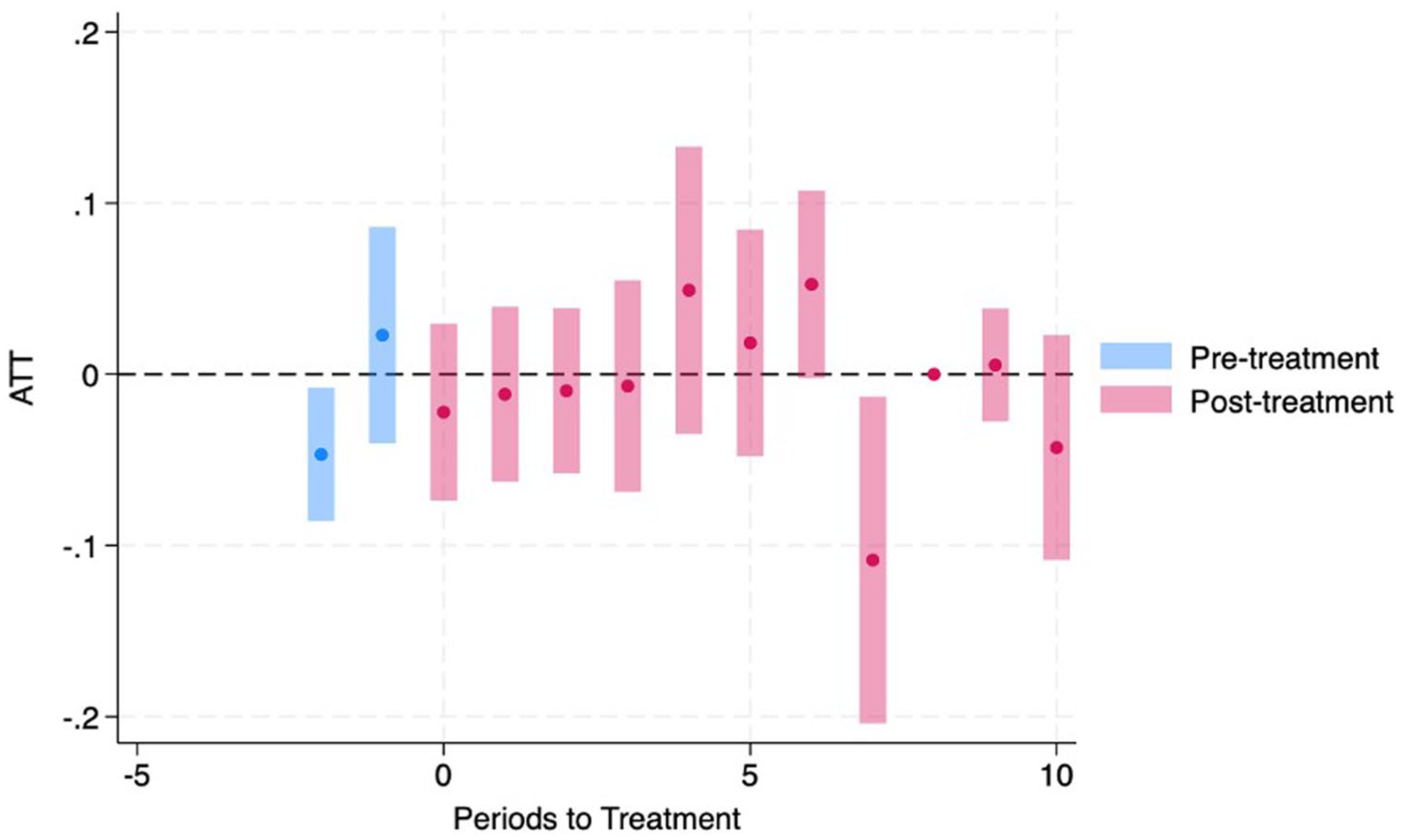
Dynamic (Event-Time) Effects
Event-study estimates did not show a consistent post-expansion pattern in any panel (Figures 1-3 and Table 2). In the lower-income panel, the pre-period average was near zero, and the post-period average was also near zero; some individual event-time coefficients were statistically significant (eg, t − 2 and t + 7), but signs were not consistently sustained across post-expansion years. In the higher-income and pooled panels, event-time estimates were generally small, with only isolated coefficients reaching conventional significance.

Dynamic effects of Medicaid expansion on frequent mental distress (FMD), pooled adults aged 18 to 64 (BRFSS 2011-2024).

Dynamic effects of Medicaid expansion on frequent mental distress (FMD), low-income adults (BRFSS 2011-2024).
Dynamic effects of Medicaid expansion on frequent mental distress (FMD), high-income adults (BRFSS 2011-2024).
Cohort-Specific Heterogeneity
We also examined cohort-by-time effects (ATT(g,t)) for expansion cohorts observed in the estimation sample (Figures 4-6). These cohort-specific estimates are best interpreted as heterogeneity in effects across adoption cohorts and follow-up periods, rather than a single uniform dynamic treatment effect. Across cohorts, estimates varied in magnitude and statistical significance at selected times, but the overall pattern remained consistent with small average effects and non-uniform dynamics.
Cohort-specific effects of Medicaid expansion on FMD: 2014 expansion cohort, low-income panel (BRFSS 2011-2024).

Cohort-specific effects of Medicaid expansion on FMD: 2016 expansion cohort, low-income panel (BRFSS 2011-2024).

Cohort-specific effects of Medicaid expansion on FMD: 2014 expansion cohort, pooled adults aged 18 to 64 (BRFSS 2011-2024).
Overall, pooled estimates were close to zero, while cohort- and event-time estimates showed modest variation across expansion cohorts and time since expansion. This pattern aligns with prior evidence suggesting that Medicaid coverage expansions can reduce distress for some low-income groups, but that population-average mental health effects are often small and not uniform across settings, outcomes, or follow-up windows.15-18
Robustness check, in the pooled 18 to 64 panel, omitting all covariates yields an ATT estimate nearly identical to the baseline specification (ATT = 0.0020, SE = 0.0046). Dropping state-years with high covariate missingness produces a modestly larger pooled estimate (ATT = 0.0053, SE = 0.0049) with a substantially reduced sample (N = 250). In the placebo specification (pseudo-adoption year = 2014), the estimated ATT is near zero (ATT = 0.0008, SE = 0.0050). Appendix Table A2 summarizes these checks.
Discussion
Principal Findings
Using a staggered difference-in-differences design aligned with variation in Medicaid expansion timing, we found near-zero pooled average effects of expansion on frequent mental distress (FMD) among adults aged 18 to 64 and similarly small effects in income-stratified panels. Event-time and cohort-specific estimates showed variability at selected leads/lags, but these differences were not consistently sustained across post-expansion years. Overall, the results suggest that population-average changes in FMD attributable to expansion are small and heterogeneous when assessed using a threshold-based surveillance outcome.
Relationship to Prior Evidence and Contribution
A substantial literature examines Medicaid expansion and patient-reported mental health using BRFSS and other survey data.15-25 Our contribution is therefore not that patient-reported mental health has been overlooked. Rather, we extend existing evidence by combining (1) an extended BRFSS window (2011-2024), (2) a standardized public health surveillance measure (FMD), and (3) a staggered-adoption estimator that is interpretable under treatment-effect heterogeneity across cohorts and time since adoption.8,9 This approach addresses concerns that conventional two-way fixed-effects DiD can yield hard-to-interpret averages under staggered adoption and heterogeneous effects.
Results in Context
The pattern of small average effects is consistent with evidence that Medicaid expansion improves coverage, access, and affordability, while mental health responses are often mixed or modest and depend on the population, outcome definition, and follow-up period.19-21 Evidence from Oregon’s randomized Medicaid expansion showed improvements in some self-reported mental health–related measures, but effects were context-dependent and not uniformly large across endpoints. 17 Studies focused on mental health treatment and utilization similarly document changes in access and service use that may not translate into stable reductions in population distress, particularly when outcomes reflect more persistent symptom burden.22,23 Other work suggests heterogeneity by subgroup and setting, including differences by race/ethnicity and among college populations.24,25 Taken together, prior evidence supports plausible pathways from coverage to improved mental health (eg, reduced financial strain), yet downstream effects on a population prevalence measure of frequent distress may remain limited. 18
Interpretation and Plausible Mechanisms
Several factors could generate modest average effects on FMD even if expansion improves access and reduces financial strain:
Distance from mechanism to outcome: Coverage can reduce out-of-pocket risk and improve access, but distress is also shaped by labor markets, housing instability, and other social risks that may dominate variation in state-year prevalence. 18
Behavioral health capacity constraints: Coverage gains may not translate into effective care when provider supply is limited or nonfinancial barriers persist (eg, network adequacy, wait times, stigma).22,23
Outcome sensitivity: FMD (≥14 “not good” mental health days) captures relatively frequent distress; expansion may affect milder symptoms, treatment initiation, or access measures without shifting this threshold indicator.22,23
Robustness and Interpretation Under Staggered Adoption
Across panels, robustness checks (covariate omission, excluding state-years with high covariate missingness, and placebo timing) did not suggest that pooled null findings hinge on a single modeling decision, although these checks do not replace formal sensitivity analyses for violations of (conditional) parallel trends. 11 Event-time estimates should be interpreted as weighted averages of cohort-specific effects at each relative time; in unbalanced panels, the set of cohorts contributing to each event time can vary, so apparent fluctuations do not necessarily reflect a uniform dynamic effect.8,9
Policy Implications
The findings are most consistent with the conclusion that Medicaid expansion is necessary but not sufficient to generate large reductions in population-level frequent distress. Expansion can improve affordability and financial security 18 and may influence access to and utilization of mental health care22,23; however, meaningful shifts in FMD likely require complementary investments, particularly in behavioral health capacity, the integration of behavioral health into primary care, and upstream social supports. 18 Key strengths include a long BRFSS time horizon and an estimator appropriate for staggered adoption, with results reported in pooled and income-stratified panels consistent with the replication workflow.
Limitations
• Income classification and eligibility mismeasurement: Defining “low-income” as inc_cat = 1 (<$15 000) is an imperfect proxy for <138% FPL and does not account for household size; the comparison group (non-lowest-income with observed income) can include individuals also affected by Medicaid expansion or marketplace subsidies. This misclassification can attenuate estimated contrasts toward the null. A preferred approach constructs %FPL using BRFSS income categories and household size following established methods. 26
• Income missingness in 2022: In our analytic extract, income was missing for all observations in 2022, so income-stratified panels exclude 2022 by construction; pooled analyses retain 2022 because they do not condition on non-missing income.
• State-year aggregation: Collapsing microdata to state-year prevalence can dilute subgroup-specific effects and mask within-state heterogeneity.
• Time-varying shocks and survey context: COVID-era disruptions and evolving social conditions may affect distress and sample composition in ways not fully captured by covariate shares.
• Policy intensity and heterogeneity: A single expansion-year indicator does not capture waiver design, benefit generosity, provider payment, or implementation intensity, which may attenuate average effects.
• Sample size calculation/justification: This study is a secondary analysis of BRFSS surveillance data using all eligible respondents (2011-2024); we did not conduct an a priori power/sample-size calculation. 27
Future Research
Future work should extend this analysis in several directions. First, as a sensitivity analysis, researchers can construct percent of the federal poverty level (%FPL) using BRFSS income categories, household size, and year-specific poverty thresholds to more directly target the <138% FPL population. 26 Second, replicating the main specifications at the individual level (using BRFSS microdata with appropriate survey-weighted methods) would help assess whether state-year aggregation attenuates effects or masks subgroup heterogeneity. Third, effect heterogeneity should be evaluated across baseline distress and key sociodemographic strata (sex, race/ethnicity, education), as well as across timing/context (pre- vs post-2020). Fourth, mechanisms should be tested explicitly using intermediate outcomes available in BRFSS (eg, insurance coverage, cost-related care avoidance, usual source of care, and indicators of mental health treatment access where available). Finally, richer policy measurement, capturing waiver type, eligibility thresholds, benefit design, managed care penetration, and behavioral health capacity, may clarify whether impacts depend on implementation intensity and local treatment supply constraints.
Conclusion
Using BRFSS data from 2011 to 2024 and a staggered difference-in-differences design that accounts for variation in Medicaid expansion timing, we find little evidence of a large population-wide effect of Medicaid expansion on the prevalence of frequent mental distress among adults aged 18 to 64. Pooled estimates are near zero, and income-stratified results are similarly modest, although some cohort- and event-time estimates vary across follow-up years. Overall, the results suggest that insurance expansion alone may be insufficient to shift population frequent mental distress without complementary behavioral health capacity and broader social support interventions.
Supplemental Material
sj-docx-1-inq-10.1177_00469580261441768 – Supplemental material for Medicaid Expansion and Frequent Mental Distress Among U.S. Adults: Staggered DiD Using BRFSS, 2011 to 2024
Supplemental material, sj-docx-1-inq-10.1177_00469580261441768 for Medicaid Expansion and Frequent Mental Distress Among U.S. Adults: Staggered DiD Using BRFSS, 2011 to 2024 by Abimbola Adegoke, Kola Adegoke, Olajide Alfred Durojaye, Deborah Dawodu, Abiodun Isola Aluko, Akorede Adekoya and Kenneth A. Knapp in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Appendix
Robustness and Placebo Checks (csdid Estimator; Standard Errors Clustered by State).

| Panel | Specification | ATT | SE | N |
|---|---|---|---|---|
| Low-income | Baseline (main covariates) | −0.0125 | 0.0202 | 400 |
| Low-income | No covariates | −0.0125 | 0.0202 | 400 |
| Low-income | Drop high covariate missingness (>50%) | −0.0468 | 0.0365 | 159 |
| Pooled (18-64) | Baseline (main covariates) | 0.0020 | 0.0046 | 709 |
| Pooled (18-64) | No covariates | 0.0020 | 0.0046 | 709 |
| Pooled (18-64) | Drop high covariate missingness (>50%) | 0.0053 | 0.0049 | 250 |
| Pooled (18-64) | Placebo: pseudo-adoption year = 2014 for ever-treated | 0.0008 | 0.0050 | 709 |
Note. “Drop high covariate missingness” removes state-year observations where any available covariate exceeds 50% missingness, based on screening criteria defined in the analysis code. The placebo assigns 2014 as a pseudo-treatment year for ever-treated states and 0 for never-treated states; estimation otherwise matches the pooled baseline specification. N denotes observations used in each estimation sample (state-years).
Acknowledgements
We acknowledge the Centers for Disease Control and Prevention (CDC) and state health departments for collecting and making the Behavioral Risk Factor Surveillance System (BRFSS) data publicly available. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the CDC.
Author Note
All authors read and approved the final manuscript.
Ethical Considerations
All recruitment and study procedures were approved by the Institutional Review Board (IRB) at New York Medical College (IRB number 29761).
Consent to Participate
Participant-informed consent was obtained by BRFSS during data collection and survey procedures. The present analysis involved no direct interaction with participants and no access to identifiable information; therefore, no additional written informed consent was obtained for this secondary analysis.
Author Contributions
Conceptualization: Kola Adegoke Methodology: Abimbola Adegoke Data Curation: Abimbola Adegoke; Deborah Dawodu Formal Analysis: Kola Adegoke Software: Kola Adegoke Validation: Abimbola Adegoke; Abiodun Isola Aluko Investigation: Abimbola Adegoke; Olajide Alfred Durojaye; Deborah Dawodu; Abiodun Isola Aluko Interpretation: Abimbola Adegoke, Olajide Alfred Durojaye; Deborah Dawodu; Abiodun Isola Aluko. Writing – Original Draft: Kola Adegoke Writing – Review & Editing: Abimbola Adegoke; Olajide Alfred Durojaye; Deborah Dawodu; Abiodun Isola Aluko; Kenneth A. Knapp. Supervision: Kola Adegoke Project Administration: Deborah Dawodu Resources/Clinical/Program Context Input: Olajide Alfred Durojaye; Abiodun Isola Aluko.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.