
Abstract
To examine whether previous Affordable Care Act (ACA) Medicaid expansions had an added effect on the mental health of low-income adults during the COVID-19 pandemic in 2020 and 2021. We use the 2017-2021 Behavioral Risk Factor Surveillance System (BRFSS) data. We use an event study difference-in-differences model to compare the number of days in poor mental health in the past 30 days and the likelihood of frequent mental distress among 18 to 64 year old individuals with household incomes below 100% of the federal poverty level who participated in BRFSS in one of the surveys from 2017 to 2021 and who resided in states that expanded Medicaid by 2016 or states that had not expanded by 2021. We also examine the heterogeneity of the expansion effects across subpopulation groups. We find some evidence that the Medicaid expansion was associated with better mental health during the pandemic for adults younger than 45, females, and non-Hispanic Black and other non-Hispanic non-White individuals. There is some evidence of an added benefit to mental health from Medicaid expansion status during the pandemic for some subgroups among low-income adults, suggesting potential health benefits from Medicaid eligibility during public health and economic crises.
The COVID-19 pandemic brought unprecedented economic, social, and health challenges. Previous Medicaid expansions have been associated with increased access to coverage and health services among low-income population.
This study examines if prior Medicaid expansions affected the mental health of adults below 100% of the federal poverty level in the COVID-19 pandemic-era and finds some evidence that the expansion is associated with better mental health, especially among adults younger than 45 years, females, and non-Hispanic Black and other non-Hispanic non-White individuals.
The findings add some evidence to the potential health benefits of Medicaid eligibility for low-income adults, especially benefits to mental health during public health and economic crises.
Introduction
The novel coronavirus disease 2019 (COVID-19) pandemic and some of the policies implemented to slow down its spread brought unprecedented economic, social, and health challenges that likely had major impacts on mental health. Millions of Americans reported loss of work and income, or reduced work hours because of the pandemic. 1 Low-income individuals, women, and racial and ethnic minorities were particularly impacted as they experienced greater job loss.2,3 Unemployment can increase stress and financial insecurity and reduce self-esteem, which could worsen mental health. 4 Compounding and exacerbating the pandemic impacts on mental health were the fears and worries surrounding COVID-19 risk of infection and related restrictions of social distancing, business and school closures, quarantines, and isolation, all of which have had profound social and mental health effects.5-7
Mental health disorders affect over 20% of adults and are disproportionally more prevalent among low-income individuals. 8 Prior to the implementation of the Affordable Care Act (ACA) and its related Medicaid expansions, the uninsured rate was markedly higher among individuals with mental health disorders (20%) compared with the general population (15%), and less than 50% of people with mental health disorders received treatment.9-11 Health insurance coverage is critical to accessing mental health services, particularly among low-income populations. The ACA Medicaid expansions beginning in 2014 and continuing with additional states expanding in subsequent years have increased coverage among adults with household income below 138% of the federal poverty level (FPL). Evidence on effects of the ACA Medicaid expansions before the pandemic suggests improved access and utilization of mental and other health care services,12,13 and improved mental health14-22 particularly in the early years of the expansions as take-up of Medicaid coverage significantly increased. 23 However, whether there was an added benefit from the prior expansions to mental health during the pandemic is not well understood. With added shocks to mental health during the pandemic and disruptions to insurance coverage and access to essential mental health care services, one hypothesis is that Medicaid coverage for low-income individuals in expansion states may have buffered against some of the adverse impacts on mental health by providing greater access to needed mental health services (such as access to prescription drugs or mental health care providers providing psychotherapy via telehealth) compared to similar income individuals without Medicaid coverage in non-expansion states. Furthermore, Medicaid coverage during the pandemic may have conferred additional financial security in the event of losing a job or employer-sponsored coverage24,25 or illness, which has been associated with higher rates of anxiety, depression, and substance abuse. 26 Therefore, in this study, we examine whether the prior ACA Medicaid expansions provided an added benefit to the mental health of low-income individuals compared to non-expansion states during the pandemic.
Studies report an increase in adverse mental health conditions during the pandemic.27,28 These conditions worsened among younger adults due to school closures, employment loss, and increased feelings of social isolation.29,30 Furthermore, women were more likely than men to reduce work hours, leave their jobs to homeschool or take care of other family activities.31,32 Studies report a greater increase in depression and anxiety rates among women compared to men as their burden of responsibilities disproportionately increased during the pandemic. 33 Hispanic and non-Hispanic Black populations had a greater increase in self-reported depression and anxiety rates.34,35 In addition to disproportionally experiencing economic hardship from the pandemic, Black populations also had higher COVID-19 hospitalizations and mortality.36,37
As mentioned above, the ACA Medicaid expansions before the pandemic may have an incremental effect on mental health of low-income individuals during the pandemic in two main ways. The first possible mechanism is through access to mental health services for individuals who needed them, which may include care for newly onset or worsening prior mental health conditions during the pandemic. Without coverage, low-income individuals would have little access to such needed services. The second plausible mechanism is by providing additional financial security from Medicaid coverage38-41 after (potential) loss of employer-sponsored coverage as a result of the pandemic-related unemployment or underemployment, which might reduce stress and improve mental wellbeing. 42 This second pathway might be especially important during a global pandemic when most people become keenly attentive to their own and their family’s health. The reduction in stress with insurance coverage and financial protection from illness might be more salient during such time.
In addition, in March 2020, Congress passed the Families First Coronavirus Response Act (FFCRA), providing states with an additional 6.2 percentage-point increase in federal matching assistance percentage (FMAP) to provide continuous coverage for Medicaid.43-45 This provision may have increased coverage, reduced churning in Medicaid and interruption in access to health care services among covered individuals that may occur over time and further enhanced the expansion effect on financial security and access to mental health services. The Centers for Medicare & Medicaid Services (CMS) report an increase of 25% nationally in the population covered by Medicaid between February 2020 and January 2022. 46 Therefore, we also examine whether there was an added effect of the ACA Medicaid expansion on coverage in 2020-2021.
There is emerging evidence of the effects of the previous ACA Medicaid expansions on the mental health of low-income individuals during the COVID-19 pandemic. Two studies report that Medicaid expansion nullified the negative effect of loss of work on mental health.25,42 Another study reported no statistically significant difference in changes in days not in good mental health in the past 30 days during 2020 between expansion and non-expansion states overall, although the study found a statistically significant decline in this outcome for non-Hispanic Black individuals. 47 That study, however, included individuals up to 138% of the FPL and did not examine the effect separately for individuals below 100% of the FPL. In non-expansion states, individuals within 100-138% of the FPL are eligible for insurance marketplace subsidies, so including them in the sample may attenuate the effect of the Medicaid expansion. Furthermore, that study did not evaluate the effect on frequent mental distress characterized as experiencing 14 or more days of poor mental health in the past month, an indicator of diagnosable depressive and anxiety disorder. 48 Employing nationally representative data, we focus on individuals below 100% FPL who are expected to benefit most from the Medicaid expansions (consider the eligibility of those at 100%-138% FPL for subsidized marketplace insurance coverage). We also evaluate potential heterogeneity across age, sex, race/ethnicity, and whether children lived in the household.
Study Data and Methods
Data and Sample
We use data from the Behavioral Risk Factor Surveillance System (BRFSS), a nationally representative cross-sectional telephone survey conducted annually by the Centers for Disease Control and Prevention and state governments. The survey is conducted in all states and the District of Columbia, and it is designed to represent the non-institutionalized adult population in the United States. For this study, we include BRFSS data from 2017 to 2021, from states that expanded Medicaid by 2016 and states that had not expanded by 2021 to compare them on changes in mental health over time, including from 2019 to 2021. We exclude states that expanded Medicaid after 2016 (Idaho, Maine, Missouri, Nebraska, Oklahoma, Utah, and Virginia). Medicaid expansions by 2016 (including 4 states and the District of Columbia that had full or near full expansions before 2014 but also adopted the ACA expansion in 2014) comprise the treated group. We restrict the sample to low-income adults aged 18 to 64 with household incomes below 100% of the FPL; as a reference, for a single individual in 2021, this income was below $12 880. 49 As income is reported in ranges in the BRFSS, we use the midpoints of the income ranges and then assign to each individual income as a percentage of the FPL considering household structure.50,51 We exclude from the sample respondents whose income is between 100% and 138% FPL since, as noted above, they receive subsidies in non-expansion states to obtain insurance through the health insurance marketplace. The analytical sample consisted of 128 074 adults surveyed between 2017 and 2021, with household incomes less than 100% FPL. There were 92 061 adults in Medicaid expansion states and 36 013 adults in non-expansion states.
Outcomes
BRFSS asks respondents about the number of days in the past 30 during which their mental health was not good, including experiencing stress, depression, and emotional problems. We use this measure of mental health as the main outcome. In addition, we construct a binary indicator for frequent mental distress equal to 1 if the respondent had 14 or more days in poor mental health and 0 otherwise. 52
We also examine whether coverage changed differentially in 2020 and 2021 (compared to 2019) between previously expanded states and non-expansion states as a potential mechanism affecting mental health. As noted above, an added (incremental) effect from the earlier Medicaid expansions on mental health during the pandemic may develop without a greater increase in new enrollment in expansion states. However, if expansion states had greater enrollment during the pandemic, this may also contribute to an incremental effect on mental health among the population of income-eligible adults. BRFSS asks whether respondents have any form of health care coverage but does not ask about insurance type in all years. Therefore, in addition to the BRFSS data, we use data from the American Community Survey (ACS), 53 and Medicaid enrollment data reported by states through the Medicaid Budget and Expenditures System (MBES). 54
Research Design and Statistical Analysis
To investigate the incremental effect of Medicaid expansion, we estimate difference-in-differences models that compare changes in the outcomes in the Medicaid expansion states to changes in outcomes in the non-expansion states. Because we are interested in how the effect varied over time from 2017 to 2021, we estimate event study models. The event study allows us to examine the effects of the expansions relative to the base year of 2019, and to also test the parallel trends assumption of similar trends in outcomes between expansion and non-expansion states before the pandemic. The event study DD model is:

where
Medicaid Expansion Effects on Coverage
To investigate the effect of Medicaid expansion on coverage, we estimate a similar model using data on coverage separately from the BRFSS, ACS, and the Medicaid enrollment data. The ACS collects individual level data on insurance status along with other important demographic and socioeconomic characteristics. Using the ACS, we include a sample similar to the BRFSS sample from 2017 through 2021 to examine changes in insurance type. We also use monthly reports of Centers for Medicare & Medicaid Services (CMS) Medicaid enrollment data reported by states through the Medicaid Budget and Expenditures System (MBES) to compare Medicaid enrollment per population 18 to 64-year-old (calculated as the ratio of total Medicaid enrollment and population 18-64-year-old) between expansion and non-expansion states from 2017 through 2021. Data are adjusted using BRFSS weights, ACS weights, and population weights are used for the Medicaid enrollment data.
Results
Medicaid Expansion Effects in Total Sample
Figure 1 shows the descriptive trends in the number of days not in good mental health in the past 30 and the cutoff of 14 days or more for frequent mental distress (without any adjustment for covariates) in Medicaid expansion and non-expansion states from 2017 to 2021. Between 2017 and 2019, there is an increase in the number of days in poor mental health in both expansion and non-expansion states. In contrast, there is a relatively small decline in this outcome in 2020 (slightly more in expansion states) but a sharp increase in 2021 in both expansion and non-expansion states. However, there is less such increase in 2021 in expansion states. The trends for frequent mental distress largely follow those of the days count measure especially during the pandemic.
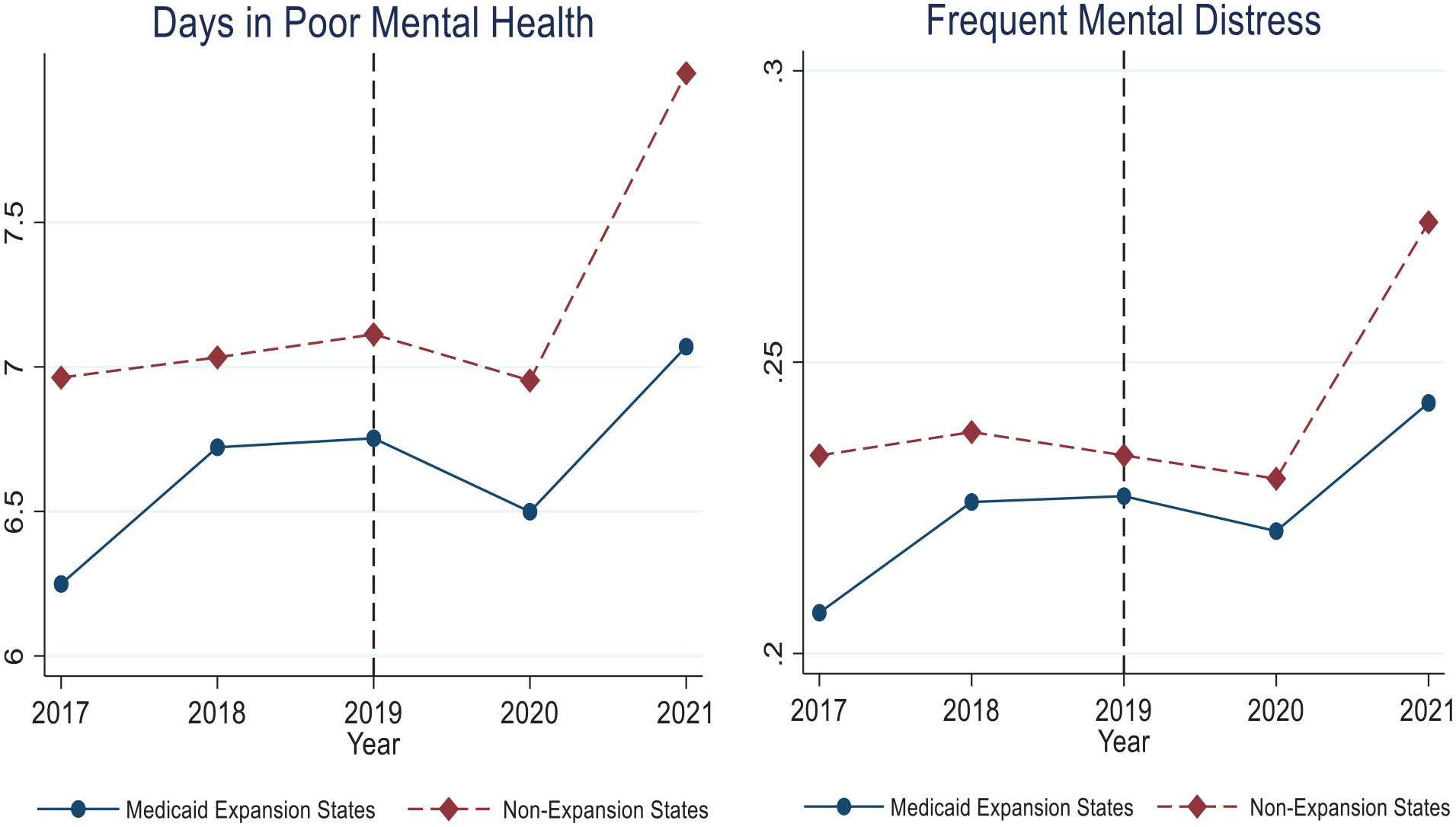
Trends in the number of days in poor mental health and frequent mental distress, Medicaid expansion versus non-expansion states, BRFSS 2017-2021.
Figure 2 presents the event study difference-in-differences graphs for the differences in mental health outcomes—number of days not in good mental health and frequent mental distress between Medicaid expansion states and non-expansion states over the years, with 2019 as the reference period. The detailed estimates are in Supplemental Appendix Tables 2 and 3. There is a decline in both mental health outcomes in 2020 and 2021 relative to 2019 associated with the Medicaid expansion. However, the estimate is not statistically significant for the number of days not in good mental health and marginally significant (P < .1) for frequent mental distress in 2021. For the latter outcome, Medicaid expansion is associated with a 3.5 percentage-point decline in the likelihood of frequent mental distress in 2021 compared to 2019; however, the difference in the 2017-2019 pre-trend between expansion and non-expansion states is marginally significant, although in the opposite direction to the effects in 2020 and 2021. The estimates are similar when excluding observations pre-pandemic in January and February in 2020 (Supplemental Appendix Tables 4 and 5). The unweighted estimates of the Medicaid expansion effect (Supplemental Appendix Tables 6 and 7) are noticeably smaller (in absolute value) and the estimate the day count measure is near null and in the opposite direction. This difference between the weighted and unweighted suggests potential heterogeneity in the effects across states, in which case the unweighted estimate of the average effect may be less generalizable. As noted above, differences between expansion and non-expansion states before 2019 are in the opposite direction in the weighted model and overall not statistically significant.

Event study estimates of the Medicaid expansion effects on the number of days in poor mental health in the past 30 days and frequent mental distress, BRFSS 2017-2021.
Medicaid Expansion Effects Among Demographic Subgroups
Figures 3 to 6 report the event study difference-in-differences estimates for the number of days not in good mental health and frequent mental distress among demographic subgroups by age, race/ethnicity, gender, and having children in the household or not. Supplemental Appendix Tables 2 and 3 show the detailed estimates.
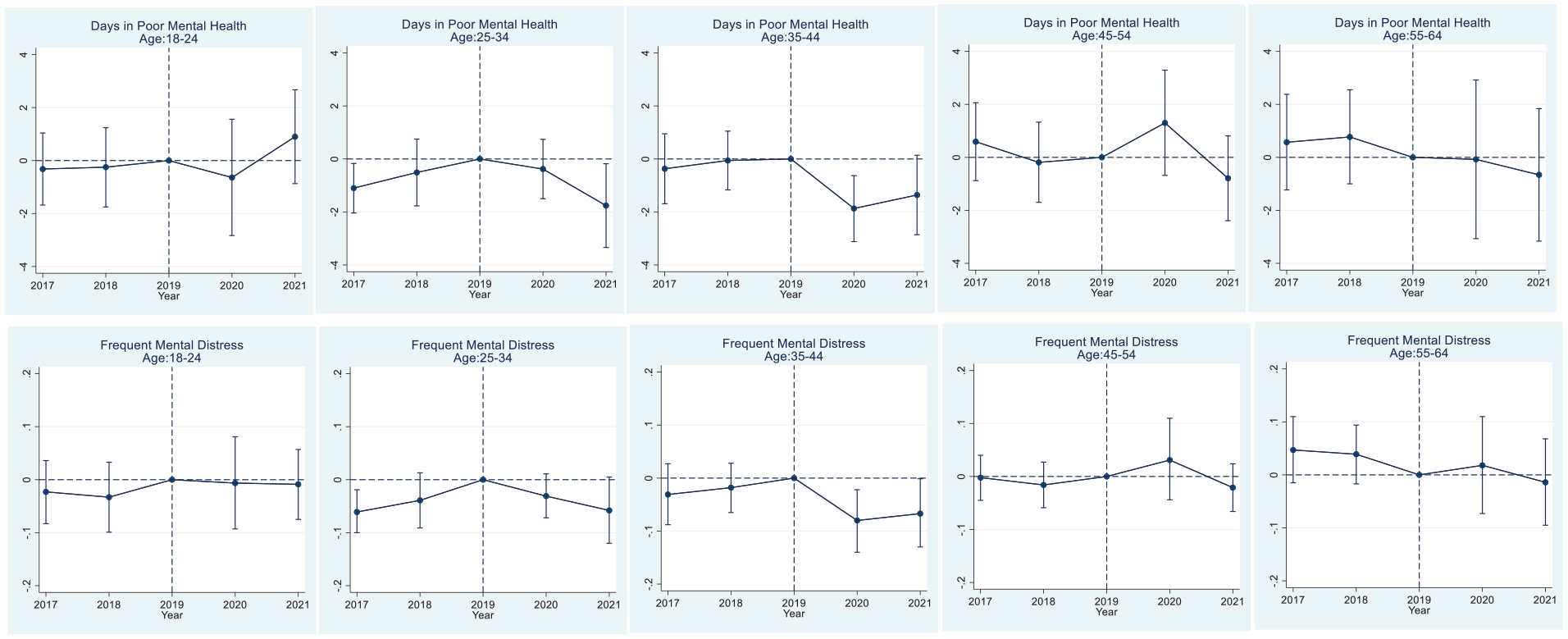
Event study estimates of the Medicaid expansion effects on the number of days in poor mental health in the past 30 days and frequent mental distress by age groups, BRFSS 2017-2021

Event study estimates of the Medicaid expansion effects on the number of days in poor mental health in the past 30 days and frequent mental distress by gender, BRFSS 2017-2021.

Event study estimates of the medicaid expansion effects on the number of days in poor mental health in the past 30 days and frequent mental distress by race/ethnicity, BRFSS 2017-2021.
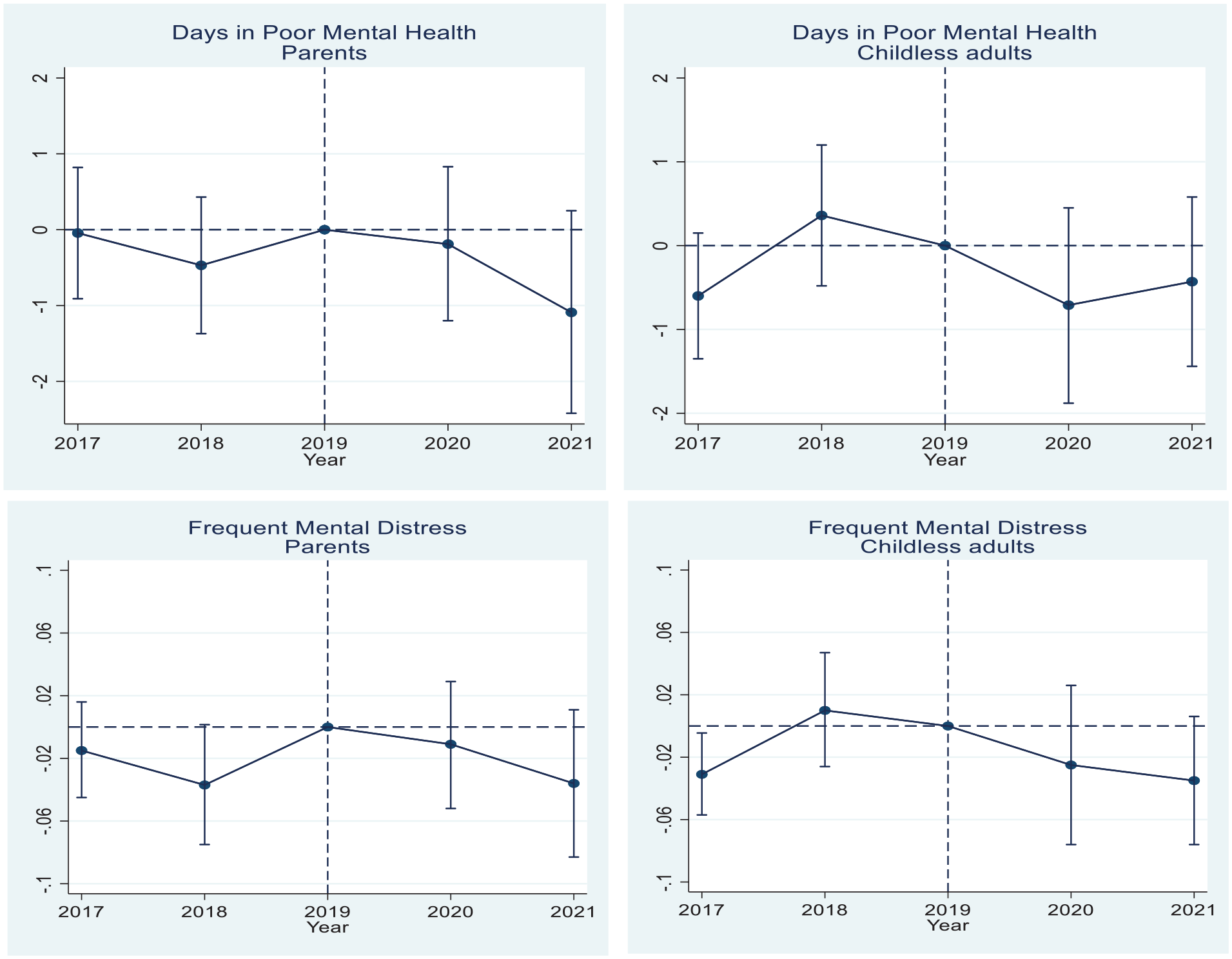
Event study estimates of the Medicaid expansion effects on the number of days in poor mental health in the past 30 days and frequent mental distress by parental status, BRFSS 2017-2021.
Comparing by age (Figure 3), we find that for 25 to 34-year-old, the ACA Medicaid expansion is associated with a 1.8 fewer days not in good mental health (P < .05) and 5.8 percentage point (P < .1) lower likelihood of frequent mental distress in 2021. The pre-trend differences between expansion and non-expansion states are statistically significant for this group, but they are in the opposite direction, suggesting that the Medicaid expansion effect is unlikely to be biased in direction. For 35 to 44-year-old individuals, the expansion is associated with 1.9 (P < .01) and 1.4 (P < .1) fewer days not in good mental health in 2020 and 2021 respectively. During the same period, there is an 8 percentage-point (P < .01) and 7 percentage-point (P < .05) lower likelihood of frequent mental distress in those years, respectively. There are no statistically significant pre-trend differences for this age group. Estimates are smaller and statistically non-significant for the other age groups.
When stratifying by gender (Figure 4), we find that among females the expansion is associated with 0.8 (P < .05) and 0.9 (P < .05) fewer days not in good mental health in 2020 and 2021, and with lower likelihood of frequent mental distress reduced by 3.5 (P < .05) and 3.9 (P < .01) percentage-points, respectively, without statistically significant pre-trend differences. Estimates for males are smaller and statistically non-significant and are of the opposite direction in 2020.
Comparing across race/ethnicity (Figure 5), we find that for non-Hispanic Black individuals, the expansion is associated with 1.8 fewer days not in good mental health (P < .1) in 2020 and with 6.9 percentage-point lower likelihood of frequent mental distress (P < .1) in 2021. Among other non-Hispanic, non-White individuals, there are 2.1 fewer days not in good mental health (P < .05) and 9.3 percentage-point lower likelihood of frequent mental distress (P < .05) in 2021. In this group, there is marginally significant difference in the 2017-2019 pre-trend between expansion and non-expansion states although of the opposite direction to the 2021 effect estimate. The Medicaid expansion effect estimates are smaller for the other groups and statistically non-significant. Finally, the Medicaid expansion is associated with a 3.5 percentage-point lower likelihood of frequent mental distress in households without children in 2021 (P < .1), though the 2017-2019 pre-trend difference is marginally significant and of the opposite direction. This estimate is close although not statistically significant for households with children. (Figure 6). The subgroup estimates are similar excluding observations interviewed in January and February in 2020 (Supplemental Appendix Tables 4 and 5).
The unweighted estimates by the demographic subgroups are reported in Supplemental Appendix Tables 6 and 7. These estimates suggest improvement in mental health for 25 to 34 year-old, non-Hispanic Black, and other non-Hispanic, non-White individuals. However, the unweighted estimates are smaller (in absolute value) for females and are not statistically significant, suggested effect heterogeneity across states.
Medicaid Expansion Effects on Coverage
Supplemental Appendix Table 8 to 13 presents the estimates for the expansion effects on coverage on the full sample and subgroups using the BRFSS, ACS, and CMS Medicaid enrollment data. The results indicate no incremental effects on coverage during the pandemic using the BRFSS and Medicaid enrollment data (Supplemental Appendix Tables 8 and 9). Using the ACS data, there is a 1.4 percentage-point increase in Medicaid coverage in 2020 (Supplemental Appendix Table 8). Across subgroups, there is suggestive evidence of an effect from the expansions on coverage in 2020 or 2021 among individuals aged 25 to 34-year-old, Male, non-Hispanic White and other, and childless adults (Supplemental Appendix Tables 10–13). However, the results using the ACS data should be interpreted cautiously given the concern about non-response bias in the ACS in 2020 associated with the pandemic.57,58
Discussion
This study evaluates whether previous Medicaid expansions had an added effect on mental health during the COVID-19 pandemic in 2020-2021-era. Specifically, the study compares the mental health of low-income adults during those years of the pandemic compared to before between states that had expanded Medicaid by 2016 and those that had not expanded Medicaid by 2021 using an event study difference-in-differences design and data from BRFSS. We find some evidence that the Medicaid expansion is associated with better mental health, particularly among adults younger than 45 years, females, and non-Hispanic Black and other non-Hispanic, non-White individuals. The pandemic and pandemic-related economic hardship had widespread effects on the population, particularly among low-income, Black, women, and young adult populations. The findings suggest that access to Medicaid coverage during an economic and public health crisis may partially offset some of the negative financial and health impacts of the pandemic, in this case, effects on mental health.
The suggested benefit to mental health from higher Medicaid eligibility might result from greater access to needed mental health treatments among those experiencing mental health problems. Before the pandemic, the ACA Medicaid expansions had been associated with an increase in mental health care utilization,13,59 access to care for people with mental distress,60,61 and availability of mental health treatments.12,21 The pandemic created barriers to and disrupted the delivery of mental health care. Overall, outpatient services declined 60% in the early months of the pandemic in 2020 as providers made practice adjustments and deferred non-emergency services. Similarly, studies report a decline in initiation of mental health medications during the pandemic.62,63 However, low-income individuals with Medicaid coverage in expansion states may have had greater access to mental health services during the pandemic than individuals with similar income in non-expansion states, including via telehealth care which some state Medicaid programs expanded during the pandemic. 64 Studies show that the utilization of telehealth for mental health conditions increased during the pandemic, 63 specifically among young adults, 65 females, 66 and individuals with serious mental illness. 67 In addition to greater access to services, there is also the possibility of an added effect on financial security during the pandemic as noted above. Before the pandemic, Medicaid expansion has been associated with a reduction in financial distress, 68 specifically among non-Hispanic Black individuals. 24 Because coverage protects against the financial shocks of unexpected catastrophic medical events, it may confer “feelings of security” that may improve mental health among individuals that are more likely to be impacted.18,22 However, BRFSS does not provide data to investigate these potential mechanisms, which we leave for future research.
A related question is whether there was an incremental effect on Medicaid enrollment in expansion states that would lead to an added benefit on mental health among the income eligible population. Using multiple data sources-BRFSS, ACS, and the Centers for Medicare & Medicaid Services (CMS) Medicaid enrollment data from 2017 to 2021, we find some evidence of an incremental effect on coverage and across some subpopulation groups using the ACS data indicating that some of the added benefit to mental health during the pandemic may have resulted from gains in access to Medicaid coverage in expansion states. However, this result should be interpreted with caution due to concerns about survey quality issues in 2020. 57 CMS reports an increase in Medicaid enrollment nationally during the pandemic, although this appears to be largely driven by the FFCRA maintenance of eligibility and continuous enrollment rather than new applicants.69,70 Also, our study excludes states that expanded after 2016 including those that expanded during the pandemic which may have experienced different effects on coverage.
The temporary FMAP with the continuous eligibility and enrollment provisions are scheduled to end in 2023. Continuous eligibility and enrollment are scheduled to expire on the 31st of March and the temporary FMAP will gradually phase out by December 2023. 71 Reversing these provisions may lead to breaks in or loss of coverage if individuals encounter barriers related to providing required documentation for Medicaid redetermination. 70 Such coverage interruptions may reduce access to needed mental health services. Reforms to facilitate enrollment and limit coverage interruptions for eligible adults are needed not only during the pandemic but also after that, especially if the pandemic has long-term effects on mental health.
This study has limitations. The measures for poor mental health in the BRFSS are self-reported, leaving the possibility for measurement error. However, measurement errors are unlikely to be associated with Medicaid expansion or to bias the estimates. The pandemic may have disrupted data collection processes among states. However, we do not expect that these changes will bias the results unless changes in data collection during this period systematically differed between expansion and non-expansion states. Another caveat is that even though studies using other data report declining mental health conditions in the general population and among subpopulation groups during the pandemic,6,27,35,72 mental health trends before and after the pandemic using the BRFSS data seem to suggest less of an effect from the pandemic on mental health in 2020 than other surveys. Depending on the data source and timing of the survey, estimates of the pandemic’s effects on mental health may differ in magnitude. 73 One study reported an increase in anxiety and depression in 2020 using the Household Pulse Survey (HPS) and the National Health Interview Survey (NHIS) but reported an opposite trend using BRFSS data (consistent with the trends in descriptive Figure 1). 74 However, any potential bias in mental health trends during the pandemic in a given survey would only influence the Medicaid expansion effects if this bias differed between expansion and non-expansion states. Furthermore, there is a sharp increase in days not in good mental health in 2021 in the BRFSS as noted above. In any case, it would be important to replicate this study using other national datasets, including the NHIS (which would require access to the restricted data since state geocodes are not publicly available in that dataset). Since the HPS started during the pandemic, it would not be possible to evaluate pre-trends between expansion and non-expansion states in that dataset; therefore, its value for understanding the Medicaid expansion effects in this particular case is limited.
Conclusion
We find that previous ACA Medicaid expansions are associated with an added benefit to the mental health of individuals below 100% FPL in 2020-2021 during the COVID-19 pandemic. This association does not appear to result from a larger increase in new enrollment in expansion states in that year compared to non-expansion states but rather from prior and continuing coverage. This finding adds to the evidence of the health benefits from the Medicaid expansions to income-eligible individuals, including during public health and economic crises.
Supplemental Material
sj-docx-1-inq-10.1177_00469580231166738 – Supplemental material for Effects of the Affordable Care Act Medicaid Expansions on Mental Health During the COVID-19 Pandemic in 2020-2021
Supplemental material, sj-docx-1-inq-10.1177_00469580231166738 for Effects of the Affordable Care Act Medicaid Expansions on Mental Health During the COVID-19 Pandemic in 2020-2021 by Onyinye Oyeka and George L. Wehby in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Presence of Declarations,and Ethics and Consent statements
Our study does not require an ethical board approval because we use publicly available and deidentified data.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.