
Abstract
Barriers to accessing healthcare are significant obstacles to achieving full immunization coverage, yet their impact remains underexplored in existing literature. Therefore, we assessed the effect of barriers to accessing healthcare on full immunization coverage in East African countries. This study used a cross-sectional design, using pooled demographic and health survey data (2015-2023) from 11 East African countries. After removing observations with missing data, the final weighted sample included 48 351 children aged 12 to 35 months, all born within 5 years of each country’s survey period. The outcome variable was full immunization coverage, whereas the treatment variable was barriers to accessing healthcare. We used propensity score-matching to estimate the average treatment effect of barriers to healthcare access on vaccination coverage, comparing children who faced these barriers (treated) with those who did not (untreated). Approximately two-thirds of children aged 12 to 35 months in East Africa (65.5%; 95% CI: 65.1-65.9) were from mothers who reported at least 1 barrier to accessing healthcare. The average treatment effect on the treated (ATT) estimate revealed that facing at least 1 barrier to accessing healthcare reduced the probability of completing the recommended vaccination by 3.8 percentage points (ATT = −0.038, 95% CI: −0.063, −0.014). Among the assessed barriers, challenges obtaining permission to visit health facilities, lack of companionship when seeking care, distance to the health facility, and difficulty obtaining money for treatment reduced full vaccination coverage by 12.1, 10.2, 8.2, and 2.2 percentage points, respectively. This study revealed that barriers to accessing healthcare, including geographical inaccessibility, lack of companionship, financial constraints, and the need for permission to seek care, negatively affect childhood vaccination coverage. Therefore, our findings underscore the need for public health interventions that address these barriers to enhance childhood vaccination coverage.
Keywords
Introduction
Childhood vaccination is among the most impactful and cost-effective public health strategies to protect the health and well-being of children under the age of five.1,2 Its effective implementation averted an estimated 4.4 million deaths from vaccine-preventable diseases (VPDs) such as tuberculosis, influenza, polio, diphtheria, tetanus, pertussis, and measles each year globally. 3 Despite these successes, immunization efforts are often disrupted, and many children are still not getting the protection they need against VPDs in many regions globally.4,5
In 2023, 14.5 million children missed their first dose of the diphtheria-tetanus-pertussis (DTP) vaccine, indicating inadequate access to immunization and healthcare. 6 This happened due to challenges that include reductions in immunization funding, combined with ongoing regional conflicts, instability, and population displacement; inequitable access to and fragility of primary healthcare systems; increasing vaccine hesitancy; and disruptions to routine childhood vaccination related to the COVID-19 pandemic.7-11
These setbacks have worsened existing inequities, particularly in sub-Saharan Africa, where health systems are often fragile and under-resourced. 12 In East African countries such as Ethiopia, Kenya, Tanzania, and Uganda, progress in childhood immunization has occurred. For instance, in Ethiopia, full vaccination rates among children aged 12 to 23 months rose from 14.3% in 2000 to 44.1% by 2019. 13 However, coverage remains inconsistent and stagnates below the WHO’s global target of 90%, disproportionately impacting rural and marginalized communities.14-16
Barriers to accessing routine immunization services are among the main challenges to achieving full immunization coverage.17,18 These obstacles include poor institutional infrastructure, geographic remoteness, financial constraints, and socio-cultural factors.4,18 Efforts to address these barriers, such as establishing community-based vaccination interventions, mobile health clinics, and public awareness campaigns, are critical to reducing inequities in immunization services and ultimately saving children’s lives.19-21 The Kenyan community health strategy, for example, has used community health workers to increase immunization coverage in inaccessible areas. 19
Similarly, immunization services in Ethiopia were integrated with the health extension program along with other primary healthcare interventions. 22 Despite these initiatives, progress has been inconsistent, with important gaps remaining. The persistence of these problems provides an opportunity to better understand the specific barriers to care and their impact on immunization coverage. Previous studies have shown that access to care is a key determinant of immunization coverage, but many relied on observational data, which are prone to selection bias because healthcare use is non-random.17,23 This study employs propensity score matching (PSM) to mitigate such bias, providing a more robust analysis of the impact of access barriers.
Methods and Materials
Study Design, Setting and Data Source
This study employed a retrospective cross-sectional design using data from the Demographic and Health Surveys (DHS) in East African countries. According to the United Nations (UN) Statistics Division, the East African region includes 19 countries (Burundi, Comoros, Djibouti, Ethiopia, Eritrea, Kenya, Madagascar, Malawi, Mauritius, Mozambique, Reunion, Rwanda, Seychelles, Somalia, Somaliland, Tanzania, Uganda, Zambia, and Zimbabwe). 24 Our analysis included 11 East African countries (Burundi, Ethiopia, Kenya, Madagascar, Malawi, Mozambique, Rwanda, Tanzania, Uganda, Zambia, and Zimbabwe) that had recent DHS datasets between 2015 and 2022/23. Other East African countries either had no DHS during this period (eg, Eritrea, Djibouti, Somalia, Seychelles, and Comoros) or their most recent survey was conducted outside of this timeframe.
The survey was carried out by each country’s Ministry of Health, National Statistics Office, or a designated government research institution, with technical support from ICF International and funding by the USAID. The DHS program employs validated tools and standardized methods, which ensure reliability, nationally representative data, and comparability across different countries. 25 These surveys used large samples and provided high-quality data on population, health, and nutrition to facilitate their use for planning, policymaking, and program management. The data is publicly available on the Measure DHS website: https://www.dhsprogram.com/data/. This study adheres to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for cross-sectional studies (Supplemental File 1)
Population and Sampling
The survey employs a 2-stage stratified cluster sampling design to select participants. Initially, a pre-existing sample frame, usually drawn from the most recent census, is stratified by region and by urban-rural location. Within each stratum, primary sampling units (PSUs) are selected in proportion to the population size. In the second stage, households within each PSU are systematically selected after a thorough household listing. Apart from ensuring representativeness at the national and subnational levels, and the urban and rural divide, sampling weights are used to account for the selection probabilities of certain units. More details about the DHS methodology are provided at https://dhsprogram.com/Methodology/index.cfm. 26
This study utilized immunization data extracted from the DHS children’s recode files (KR) across 11 East African countries. The study population consisted of all children aged 12 to 35 months who were alive at the time of each country’s DHS survey, drawn from births occurring within the 5 years preceding each survey period. We used pooled DHS data (2015-2023) from 11 East African countries. After removing observations with missing data, the final study included a total weighted sample of 48 351 children aged 12 to 35 months, all born within 5 years of each country’s survey period. Children under 12 months were not included in this study because they are not yet eligible to complete the recommended vaccination schedule.
Variables and Measurements
Outcome Variable
In this study, the outcome variable was the immunization status of the most recent child aged 12 to 35 months. It was measured by maternal interview responses and the vaccination card report. Mothers were requested to provide their child’s vaccination card, from which data collectors collected the dates and doses of immunizations received.
If the vaccination card was unavailable, maternal recall was used to determine the child’s immunization status. The children were classified into 3 categories: full immunized, partially immunized, and unvaccinated. The fully immunized children were those who received all recommended vaccines, including 1 dose of BCG, 3 doses of Pentavalent, pneumococcal conjugate vaccine (PCV), 2 doses of Rotavirus, oral polio vaccines (OPV), and a single dose of measles vaccine. Children who received at least 1, but not all of the recommended doses (missed any one of the recommended vaccines) were considered to have incomplete immunization, while children who failed to receive any routine immunizations were considered to have zero doses. For the main analysis, the outcome variable was dichotomized as “fully immunized” (coded 1) and “not fully immunized” (incomplete or zero-dose, coded 0). 27
Treated Variable
The treatment variable in this study was barriers to accessing healthcare services. It is a composite variable computed from 4 standardized questions asked to women about barriers to care by type of problem. These were (i) difficulty in getting money for treatment (money), (ii) difficulty with distance to health facility (distance), (iii) difficulty in not wanting to go for medical help alone (companionship), and (iv) difficulty with getting permission from their husband or household head to visit the health facility (permission). These indicators, often used in DHS-based studies, align with the WHO healthcare access framework, which emphasizes availability, accessibility, affordability, and acceptability dimensions as key determinants of service utilization.28,29
Based on the aforementioned 4 problems, barriers to care were recoded as “a big problem, coded as 1” and “not a big problem, coded as 0.” Then a composite binary variable (barriers to care) was created, coded “Yes” if a woman reported any one of these barriers (money, distance, companionship, and permission) and “No” if none of the barriers posed a challenge.30,31 This binary treatment variable (access barriers: yes = 1, no = 0) was used in the PSM analysis to assess the effect of barriers to care on full childhood immunization coverage, using “not fully immunized” (incomplete or zero-dose) as the reference category.
Covariates
A list of covariates was selected from the prior literature and based on theoretical relevance as potential determinants of risk and confounding variables for the relationship between barriers to care and full immunization coverage.32-35 Then, variables for confounder adjustment were selected for matching based on their statistical significance (P ≤ .05) in chi-square tests. Accordingly, maternal age, child’s sex, marital status, religion, residence, number of living children, media exposure, mother’s working status, wealth index, sex of household head, and birth order were included.
Data Processing and Statistical Analysis
The analysis was performed using STATA 17.0. The propensity score matching (PSM) method was used to analyze the impact of barriers to care on full immunization coverage. The treatment group included respondents who were classified as having “a big problem” in accessing healthcare services, while those classified as having “no big problem” were represented in the control group. PSM was chosen to simulate randomization through matching participants based on their vaccination status (eg, fully vaccinated or partially vaccinated) across relevant variables. This approach minimizes bias in the treatment effect and enhances the reliability of the estimate compared to other methods.36,37
To estimate propensity scores, logistic regression was used as the estimation algorithm and radius caliper matching with the tolerance level of 0.05 as the matching approach after testing several matching approaches (nearest neighbor, kernel, and radius within calipers ranging from 0.01 to 0.05), based on 2 key assumptions: common support and no confounding. Following matching, balance in covariates between the treatment and control groups was assessed to confirm the similarity of the matched samples, with higher matching quality attained by utilizing the common support option.
Propensity scores were generated by the pscore command, while matching and treatment effect estimation such as Average Treatment Effect on the entire population (ATE), Average Treatment Effect on the Treated (ATT), and Average Treatment Effect on the Untreated (ATU), were performed with the psmatch2 command. The quality of the matches was checked using the pstest command and investigating standardized biases before and after matching. The percentage difference in standardized bias was used to assess balance between the treatment and control groups, with a differences of less than 10% indicating balance. 38 Additionally, the joint significance of covariates in the estimation of conditional probability of treatment before and after matching was assessed using pseudo-R2 and likelihood ratio tests.
Finally, to ensure the robustness of the findings against possible hidden biases, a sensitivity analysis was performed using the bounding approach via the mhbounds command. The analysis was conducted across gamma values from 1 to 2 with increments of 0.05, yielding informative results on the possible effect of unmeasured confounders on the findings. 39
Results
Socio-Demographic Characteristics of Mothers
A total of 48 351 weighted samples of children aged 12 to 35 months who were born alive and were included in the survey years were included in the study. The majority of mothers were aged 25 to 34 years (46.05%), and more than half of their children were aged 12 to 24 months (54.79%). The majorities of respondents were married (83.60%) and resided in rural areas (75.52%). More than 49.66% of respondents had attended primary school, and most of them were lower wealth status (45.98%) (Table 1).
Background Characteristics of Study Participants in East African Countries, 2015 to 2023 DHS (n = 48, 351).

Reproductive and Child Health Related Factors
Most East African women had their first child at 20 years of age or younger (68.52%), and nearly half had received the recommended 4 or more ANC visits (50.41%). The majority of women had 1 or less children under the age of 5 (43.60%), and more than half had 2 to 4 total live births (51.69%) (Table 2).
Reproductive and Child Health Related Factors of Study Participants in East African Countries, 2015 to 2023 DHS (n = 48, 351).

Vaccination Coverage by Country
This study shows significant differences in full vaccination coverage across East African countries, with the highest coverage in Rwanda (89.84%) followed by Burundi (67.97%) and Malawi (53.23%). Ethiopia (23.61%) and Zimbabwe (27.26%) have lower full vaccination coverage rates. Incomplete vaccination is common in most countries, particularly high in Zimbabwe (63.59%) and Tanzania (59.29%). Zero vaccine dose percentage is highest in Ethiopia (29.13%), Madagascar (21.45%), and Mozambique (11.35%) (Figure 1).
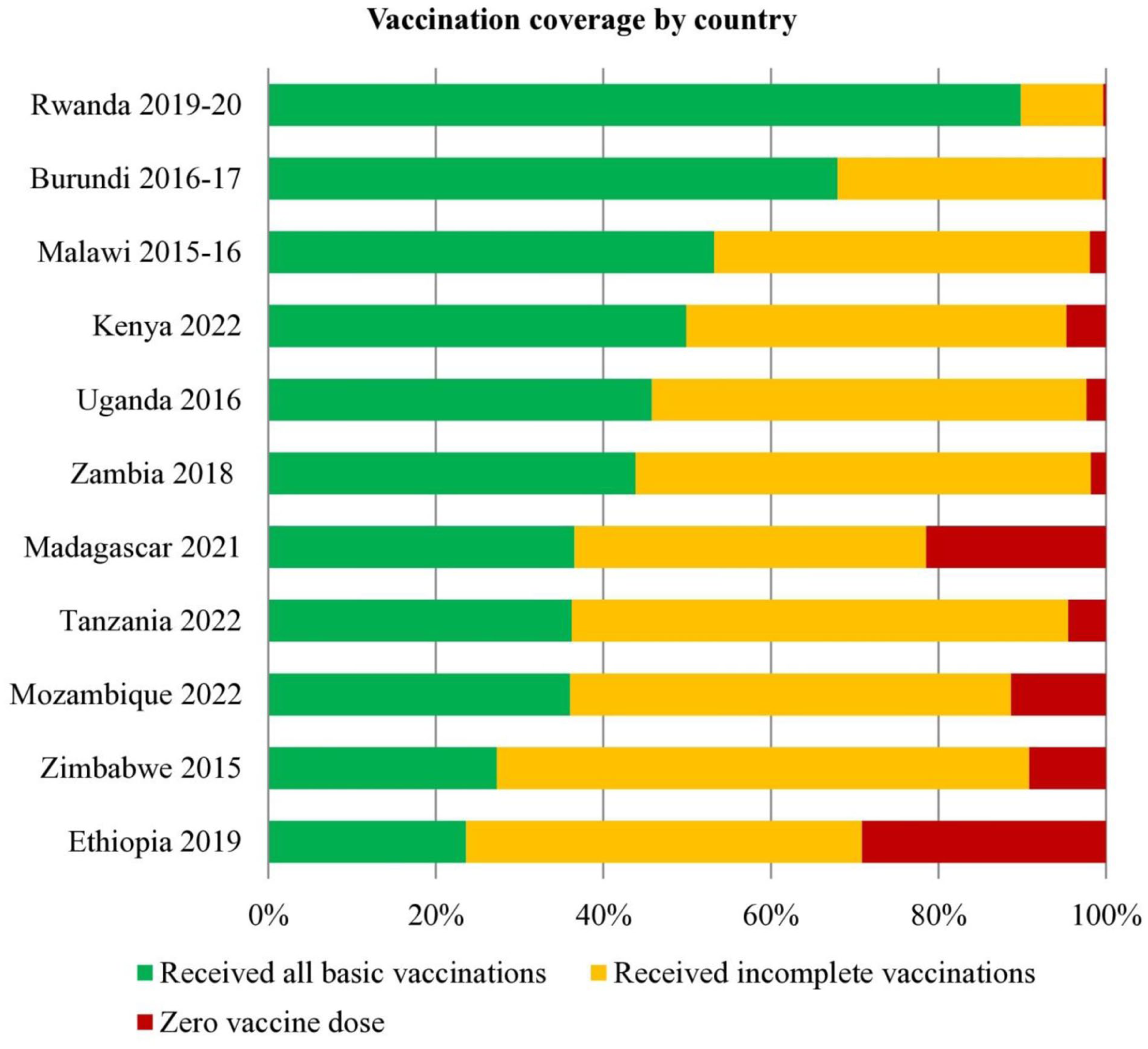
Vaccination coverage among children aged 12 to 35 months in 11 East African countries by country (DHS 2015-2023) (n = 48 351).
In East African countries, initial doses of vaccines such as BCG (91.89%), DTP1 (91.51%), and Polio1 (89.78%) demonstrated high coverage rates; however, coverage declined for subsequent doses (eg, DTP3 at 83.52% and Polio3 at 73.27%). Measles coverage was moderate at 83.85%, while only 53.35% (95% CI: 52.90, 53.79) of children were fully vaccinated. A significant proportion, 40.08% (95% CI: 38.89, 41.78), were incompletely vaccinated, and 6.57% (95% CI: 6.22, 6.98) had not received any of the recommended vaccine doses (Figure 2).

Coverage of routinely recommended vaccines among children aged 12 to 35 months in 11 East African countries (DHS 2015-2023) (n = 48 351).
Barriers to Accessing Healthcare Among Women in East Africa
In this study, 65.5% (95% CI, 65.1%-65.9 %) of women with children aged 12 to 35 months reported at least one barrier to accessing healthcare. Among the types of barriers included, getting money for treatment (53.9%) and distance to a health facility (45.5%) were the major barriers hindering access to care (Figure 3).

Percentage of women of children aged 12 to 35 months who reported having barriers in accessing healthcare in East Africa (DHS 2015-2023) (n = 48 351).
Estimations of Propensity Score and Common Support
The propensity score was estimated using logistic regression to predict the probability of being in the treatment group (barriers to care) compared to the control group (no barriers to care), based on selected covariates in the study population. The mean propensity score difference between barriers to care and full vaccination coverage was 0.65 (standard deviation = 0.12), indicating minimal variability between the treatment and control groups.
The common support assumptions assessed graphically using a histogram (Supplemental Figure 1). The distributions of propensity scores for the treated and untreated groups showed substantial overlap, indicating that the common support assumption of propensity score matching was satisfied.
The region of common support ranges from 0.41 to 0.82 and the number of blocks was 16. All observations from both the treated (n = 31 673) and untreated (n = 16 678) groups lie within the region of common support, with no cases falling outside this range. This result demonstrates that the PSM analysis retained the entire study sample and ensured comparability between the groups (Supplemental Table 1).
The Impact of Access Barriers to Care on Vaccination Coverage
The PSM analysis indicates that barriers to accessing healthcare were associated with statistically significant reductions in the likelihood of full immunization coverage among children in East Africa (P < .001 for all estimates). The average treatment effect on the treated (ATT) indicates that children whose mothers reported at least 1 barrier to accessing healthcare had a 3.8 percentage-point lower probability of completing the recommended vaccination schedule than children without such barriers (ATT = −0.038, 95% CI: −0.063, −0.014).
Among the types of barriers included, those related to companionship and permission showed the strongest effects: children whose mothers required permission to visit a health facility were 12.1 percentage points less likely to complete the recommended vaccination schedule (ATT = −0.121, 95% CI: −0.134, −0.108), and those mothers who reported difficulty in going alone were 10.2 percentage points less likely to be fully vaccinated (ATT = −0.102, 95% CI: −0.113, −0.091), compared with their matched counterparts. Similarly, children whose mothers facing problems to reach to the health facility were 8.2 percentage points less likely to complete the recommended full vaccination (ATT = −0.082, 95% CI: −0.093, −0.071), while those children of mothers experiencing barriers in getting money for treatment were 2.2 percentage points less likely to complete the full vaccination (ATT = −0.022, 95% CI: −0.033, −0.011), than their matched counterparts (Table 3).
The Propensity Score Matched Analysis of the Impact of Barriers to Care on Full Immunization Coverage in East Africa (2015-2023) (n = 48 351).

Note. ATT = average treatment effect on treated; ATU = average treatment effect on the untreated; ATE = average treatment effect on the entire population.
Women who have at least 1 barrier in accessing healthcare from lists in this table.
Quality of Matching
Balancing Test, Standardized Bias, and Model Significance
A covariate balancing test was conducted to evaluate the effectiveness of propensity score matching in reducing differences between the treated and control groups in terms of mean bias, median bias, mean standard bias, and a pseudo-R2. After matching, the treated and control groups showed substantial improvement in balance. Accordingly, the mean bias decreased from 13.8 to 2.2, the median bias decreased from 2.5 to 1.2, and the mean standard bias (B) decreased from 54.4 to 7.7. Furthermore, the T-test results showed that the pseudo-R2 after matching decreased from 0.050 to 0.001, and most selected covariates had P-values > .05 after matching, indicating better model fit and more reliable estimation of treatment effects (Supplemental Table 2). Moreover, the standardized percentage bias for covariates after matching was close to zero, as shown in Figure 4. These indicate good matching quality and low explanatory power of each covariate after matching.

Standardized percentage bias across covariates before and after matching to access barriers on childhood immunization in East Africa (2015-2023).
Sensitivity Analysis Using Mantel-Hansel-Bounds
The Mantel-Haenszel test statistic was used to investigate whether PSM estimates were sensitive to hidden bias. The sensitivity analysis results show that our matching techniques are robust to hidden bias. Accordingly, the overestimation (p_mh+) and underestimation (p_mh−) of hidden bias were similar at gamma equal to 1 and became significant as gamma increased to 2 (Supplemental Table 3).
Discussion
This study provides critical information on the effect of access barriers to healthcare on childhood immunization coverage in East African countries, a region where many children still die and health inequities continue to challenge progress toward the Sustainable Development Goals. Specifically, we analyzed the impact of selected barriers to care, such as distance to health facility, financial constraints, lack of companionship, and the need for permission to seek care, on full immunization coverage among children aged 12 to 35 months.
The findings of this study indicate that approximately two-thirds of children aged 12 to 35 months faced at least 1 barrier to accessing healthcare in East Africa. In our analysis, full immunization coverage among children in this age group dropped by 3.8 percentage points, when at least 1 access barrier was present. While this effect size seems small, it is significant given the large population and its cumulative impact over time. In addition, this relatively small effect size may be due to the implementation of extensive community outreach and mobile immunization programs in many East African countries over recent decades, which could have mitigated the expected negative effect of access barriers on vaccination coverage. It is also important to note that this study focused on individual and household-level access barriers, which are measurable using DHS data.
Importantly, this study found that children whose mothers faced challenges obtaining permission to visit health facilities, difficulty going alone, and problems reaching health facilities had the greatest negative effects on completing the recommended vaccination schedules. These barriers reduced the probability of full vaccination coverage by 12.1, 10.2, and 8.2 percentage points, respectively.
This finding was supported by previous reports from studies conducted in different parts of Africa, which found that a significant proportion of children aged 12 to 35 months faced barriers to accessing healthcare, primarily due to geographical inaccessibility, and financial constraints.18,40,41 For instance, a systematic review conducted in sub-Saharan Africa showed that distance to access point, financial deprivation, lack of partners’ support, and cultural beliefs were the main barriers to accessing child immunization programs. 32
Studies in Ethiopia, Kenya, and Nigeria also revealed that transportation challenges, financial constraints, obtaining permission to receive treatment, and reluctance to travel alone were the primary barriers to accessing vaccination services at health facilities.18,40,41 This implies the need for collaborative efforts, such as door-to-door campaigns and mobile clinics, as well as addressing sociocultural challenges, to ensure access to immunization services. In addition, government policies need to address indirect costs, such as transportation, opportunity costs, and informal fees, to ensure that vaccination services are really affordable and accessible.
While we controlled for key confounders, there are other supply-side and demand-side barriers that are not available in the DHS dataset, such as poor infrastructure, workforce shortages, communication gaps between providers and caregivers, vaccine and supply stockouts, and outreach coverage gaps that influence vaccine uptake and immunization programs. Evidence in different East African countries, such as Madagascar, Ethiopia, and Kenya, reported socioeconomic status, household size, maternal and paternal education, supply chain disruptions, geographic location, and media access as key obstacles.42-44 Although these variables overlap with our adjusted confounders, they indicate the necessity of integrated strategic responses.
This finding aligns with evidence from DHS-based and facility level studies worldwide, which show that barriers to care consistently decrease uptake and non-completion of immunization series.16-18,45-47 This is because barriers to care, such as distance from health facilities, financial constraints, the need for companionship and difficulties in obtaining permission to visit health facilities, impose a significant burden on families and often delay the provision of care to children. For example, Bangura et al and Burnett et al found that distance to healthcare facilities, difficulties with transportation, and availability of services are key predictors of incomplete vaccination in sub-Saharan Africa.32,34 Likewise, Simegn et al and Debie et al emphasized the importance of having companionship for the full utilization of the vaccination program.48,49
Regarding vaccination coverage, our study revealed that only 53.4% of children aged 12 to 35 months in East Africa had completed the recommended vaccination schedule. This result is far from the WHO 90% target of 2030. This might be attributed to several interlinked factors contributing to the low vaccination rate in this area. Examples include political instability, limited community participation, inefficient health systems, and financial constraints.50,51 At the same time, entrenched social norms, cultural and religious beliefs continue to hinder the uptake of vaccination across these regions. 52
Furthermore, the finding of this study fall short of the coverage reported in similar low and middle-income settings. For example, a study in sub-Saharan Africa reported 59.4%, 53 West Africa has reported 56.45% in Ghana, 54 Malaysia documented (86.4%), 55 Nigeria reported 74.2%, 56 Lao People’s Democratic Republic documented 67.6%, 57 and South Asian countries such as India, Bangladesh and Nepal have achieved 85% coverage. 58 This disparity may be due to fragmented health systems, 59 insufficient funding for health in East Africa compared to other countries, 60 and persistent inequalities in service delivery between rural and urban setting. 61
In this study, Rwanda demonstrated remarkably high coverage, with 89.84% of children receiving full vaccination, thereby attaining global targets. This might be attributed to sustained political commitment, strong decentralized immunization programs, and digital immunization registers. Rwanda’s experience suggests that consistent funding for local health systems, data-driven monitoring, and community engagement can improve vaccination rates and health equity, offering replicable strategies for neighboring countries. 62
Strength and Limitations
This study was based on nationally representative DHS data collected using standardized questionnaires across all 11 countries, ensuring data comparability. Importantly, the study used propensity score matching to adjust for confounding variables, providing a more accurate estimate of the impact of barriers to care on full immunization coverage. However, this study has limitations inherent to the DHS survey methodology. As DHS surveys are household-based and intended to represent the permanently resident population; nomadic, displaced, and other marginalized groups may be underrepresented or excluded. Since vaccination status was based on vaccination cards or maternal recall, this may introduce recall bias. Moreover, the matching process used observed variables to balance the treatment and control groups; unmeasured confounders may still affect the results and lead to residual confounding.
The study also did not contain broader health system barriers. These include poor health infrastructure, workforce shortages, suboptimal communication between healthcare workers and caregivers, and vaccine and supply stock-outs. Such barriers play a significant role in vaccination access, and future studies should therefore incorporate them to provide a more comprehensive picture.
Another limitation is that the DHS surveys were conducted in different years across the included countries, potentially introducing temporal variability. Furthermore, the analysis combined children aged 12 to 23 months and 24 to 35 months into a single group to enhance comparability and increase the sample size. However, barriers to care may influence these age groups in distinct ways. Finally, we had no control over the quality of the secondary data collected during the DHS, which could have influenced the findings.
Conclusions
This study revealed that about two-thirds of children aged 12 to 35 months in East Africa have faced at least 1 barrier to accessing healthcare. Barriers such as geographic inaccessibility, financial constraints, a lack of companionship, and the need for permission to seek care significantly reduce childhood vaccine coverage. Therefore, countries in East Africa should enhance their efforts by improving women’s financial empowerment, facilitating women’s companionship, and strengthening immunization programs to reach underserved areas. These measures would significantly increase full childhood immunization coverage and reduce child mortality from vaccine-preventable diseases.
Supplemental Material
sj-docx-1-inq-10.1177_00469580261441758 – Supplemental material for Access Barriers to Healthcare and Full Childhood Immunization Coverage in East Africa (2015-2023): A Propensity Score Matched Analysis
Supplemental material, sj-docx-1-inq-10.1177_00469580261441758 for Access Barriers to Healthcare and Full Childhood Immunization Coverage in East Africa (2015-2023): A Propensity Score Matched Analysis by Endalkachew Dellie, Chalie Tadie Tsehay, Getachew Teshale, Andualem Yalew Aschalew, Asebe Hagos, Tesfahun Zemene Tafere, Nebebe Demis Baykemagn and Nigusu Worku in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580261441758 – Supplemental material for Access Barriers to Healthcare and Full Childhood Immunization Coverage in East Africa (2015-2023): A Propensity Score Matched Analysis
Supplemental material, sj-docx-2-inq-10.1177_00469580261441758 for Access Barriers to Healthcare and Full Childhood Immunization Coverage in East Africa (2015-2023): A Propensity Score Matched Analysis by Endalkachew Dellie, Chalie Tadie Tsehay, Getachew Teshale, Andualem Yalew Aschalew, Asebe Hagos, Tesfahun Zemene Tafere, Nebebe Demis Baykemagn and Nigusu Worku in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-3-inq-10.1177_00469580261441758 – Supplemental material for Access Barriers to Healthcare and Full Childhood Immunization Coverage in East Africa (2015-2023): A Propensity Score Matched Analysis
Supplemental material, sj-docx-3-inq-10.1177_00469580261441758 for Access Barriers to Healthcare and Full Childhood Immunization Coverage in East Africa (2015-2023): A Propensity Score Matched Analysis by Endalkachew Dellie, Chalie Tadie Tsehay, Getachew Teshale, Andualem Yalew Aschalew, Asebe Hagos, Tesfahun Zemene Tafere, Nebebe Demis Baykemagn and Nigusu Worku in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-4-inq-10.1177_00469580261441758 – Supplemental material for Access Barriers to Healthcare and Full Childhood Immunization Coverage in East Africa (2015-2023): A Propensity Score Matched Analysis
Supplemental material, sj-docx-4-inq-10.1177_00469580261441758 for Access Barriers to Healthcare and Full Childhood Immunization Coverage in East Africa (2015-2023): A Propensity Score Matched Analysis by Endalkachew Dellie, Chalie Tadie Tsehay, Getachew Teshale, Andualem Yalew Aschalew, Asebe Hagos, Tesfahun Zemene Tafere, Nebebe Demis Baykemagn and Nigusu Worku in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-5-inq-10.1177_00469580261441758 – Supplemental material for Access Barriers to Healthcare and Full Childhood Immunization Coverage in East Africa (2015-2023): A Propensity Score Matched Analysis
Supplemental material, sj-docx-5-inq-10.1177_00469580261441758 for Access Barriers to Healthcare and Full Childhood Immunization Coverage in East Africa (2015-2023): A Propensity Score Matched Analysis by Endalkachew Dellie, Chalie Tadie Tsehay, Getachew Teshale, Andualem Yalew Aschalew, Asebe Hagos, Tesfahun Zemene Tafere, Nebebe Demis Baykemagn and Nigusu Worku in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The author would like to acknowledge the Demographic and Health Surveys Program for granting access to the dataset used in this study, which made this analysis possible.
Abbreviation
ATE: Average Treatment effect on the Entire population; ATT: Average Treatment Effect on the Treated; ATU: Average Treatment effect on the Untreated; CI: Confidence Interval; DHS: Demographic and Health Survey; PSM: Propensity score matching; VPDs: Vaccine Preventable Diseases
Ethical Considerations
The MEASURE DHS (available at ![]() Data and accessed on 16 December 2024) provided the ethical approval and authorization of the data after submission of a brief study concept. Since the data used are secondary and publicly available, the consent of the participants was not required. This study is not a clinical trial; thus, no clinical trial registration applies. All procedures have been conducted in accordance with the Helsinki Declaration.
Data and accessed on 16 December 2024) provided the ethical approval and authorization of the data after submission of a brief study concept. Since the data used are secondary and publicly available, the consent of the participants was not required. This study is not a clinical trial; thus, no clinical trial registration applies. All procedures have been conducted in accordance with the Helsinki Declaration.
Author Contributions
ED conceived the study and was involved in the data extraction and data analysis. NW, AYA, CTT, GT, TZT, AH, and NDB participated in the editing and revising of the manuscript. All authors have read and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.