
Abstract
Cleaning industry is the place where the labor intensive, and high prevalence of ergonomic hazard exposures (EHE) were reported among hospital cleaners particularly in low-middle income countries. However, only few studies were conducted in eastern Ethiopia on preventive implication of EHE and its associated factors among hospital cleaners, which was the aim of this study. A hospital based cross section study design was conducted on 741 hospital cleaners from May to August 2023 in Ethiopia. Face-to-face interview was conducted. The study outcome, EHE was assessed by Nordic Questionaries. Data was coded, double-entered, checked, and cleaned using Epi-Data 3.1. After that, Stata 17MP was used to analysis data. Binary and multivariable logistic regression were applied to explore the relationship between EHE and predictors. The cut-point for multivariable analysis was p-value of .20 at a binary analysis. The crude odds ratio (COR) and adjusted odds ratio (AOR) with a 95% confidence interval (95% CI) was statistically declared. The current study found that self-reported EHE among hospitals cleaners was 40.35% (95% CI: 36.64-44.15). The main 5 leading causes of EHE among cleaners were pushing cleaning materials (55.79%), pulling cleaning materials (65.40%), lifting cleaning materials (58.50%), pushing waste materials (65.90%) and standing more than 4 h (57.60%). The model found that those have poor knowledge about EHE (AOR: 6.68; 95% CI: 2.83-15.76), those having greater than 6 years working services (AOR: 1.90; 95% CI: 1.12-3.21) and having workload (AOR: 2.98; 95% CI: 1.58-5.60) were more likely to exposed with ergonomic hazards. The concludes that nearly 4 out of 10 (roughly 40%) hospital cleaners in government hospitals in eastern Ethiopia experience EHE has significant, multifaceted implications for worker health, operational efficiency, and the healthcare system. It was found that poor knowledge about EHE, increasing in working service, working more than 8 h/day and workload were significantly associated with it.
Introduction
The cleaning services industry is vital because it maintains safe, effective, and healthy work environments. 1 Routine cleaning extends the life of supplies and equipment, which eventually improves business operations and employee morale. Cleaners consider the job labor intensive, and that workload is increasing in recent years. 2 Hospitals cleaners face ergonomic hazards from repetitive motions, awkward postures, heavy lifting, and prolonged exertion, which can lead to musculoskeletal disorders (MSDs) like back, shoulder, and hand injuries, such as tendinitis and carpal tunnel syndrome. 3 Other hazards include poor workstation design that forces excessive reaching and non-adjustable equipment, as well as psychosocial factors like high work rates, lack of rest breaks, and shift work that contribute to muscle tension and fatigue. 4
Ergonomic and work-related MSDs represent a significant and growing global health burden, providing strong justification for further study. The global prevalence of MSDs among sanitary workers including cleaners is high, with a major 2024 meta-analysis finding an overall rate of 40.52%, affecting over two-fifths of workers, with higher rates in high-income countries (43.32%) and in low-income countries (38.58%). These disorders stem from poor ergonomics, job design, repetitive motions (lifting, pushing, standing), and job strain, often impacting the lower back, neck, and shoulders. 5 The cleaning tasks and locations, and the tools used vary in a shift, only through field assessments can the true physical exposure of the occupation be better understood. The choice of assessment methods is therefore important to evaluate tasks to a better fidelity. 6
While there are various methods, observational methods were considered over direct measurement in a cleaners work setting due to its non-invasive, non-disruptive, and easy-to-apply nature in a field environment. 7 For maids and housekeeping cleaners, the rate was 415, about 3.5 times higher than the average. 8 Due to the nature of the cleaning tasks, hand/wrist, shoulder, and low back are the most affected body parts among the janitorial population. 9 Workplace conditions that lead to physical wear and tear on the body, such as uncomfortable postures (like bending and twisting), strong exertions (like heavy lifting), and repetitive motions, are the source of ergonomic hazard exposures in cleaning activities. 10 Contact stress from hard surfaces, vibration from equipment, poorly designed workstations, high-stress workplaces, and personal health variables including specific medical disorders can all enhance susceptibility. 11 The primary consequences of hospital cleaners’ exposure to ergonomic hazards are high incidence of MSDs, chronic pain, and occupational injuries. These conditions have a significant impact on the workers’ productivity, standard of living, and physical health. 3
Additionally, cleaning the workplace carries a number of biological, chemical, and physical hazards. Workers may encounter bacteria, viruses, fungi, and mold from contaminated surfaces, bodily fluids, or waste materials. Cleaning agents often contain corrosive acids, alkaline agents, and volatile organic compounds, which can cause respiratory irritation, chemical burns, or other health issues. Also physical hazards include slips, trips, and falls on wet floors or from using ladders/scaffolding, ergonomic injuries from repetitive motion or heavy lifting, and cuts or punctures from sharp objects or broken equipment. 12 Work-related ergonomic exposures factors and individual-related variables are the 2 main categories into which associated ergonomics factors may be divided. Forceful exertions, repeated actions, uncomfortable or static postures, direct pressure, vibration, and extremely high or low temperatures are all examples of ergonomic exposures factors that can cause strain and injury. How a person interacts with their surroundings and the hazards that come with it can be influenced by a variety of individual aspects, including physical attributes (body size, strength, and fitness), cognitive abilities, skills, and even attitude.13,14 Furthermore, cleaning and sanitation practices in developing countries are typified by the preponderance of physical labor. The working conditions and characteristics of cleaning expose those who work in the cleaning industry to a variety of hazard exposures that may go untreated because of restricted access to medical services. 15
Furthermore, the key gaps in the study of ergonomics among hospital cleaners include a lack of consistent ergonomic applications, a need for more research in developing countries. While studies identify high rates of work-related ergonomic, there is a significant gap in research evaluating the effectiveness of widespread implementation strategies for ergonomic principles, tools, and training programs within hospital settings. 12 There is limited information available on the prevalence and contributing factors of ergonomical hazard exposure among cleaners in many developing countries, indicating a major geographical knowledge gap. Research highlights that current cleaning tools and equipment often contribute to awkward postures and heavy lifting. 16 There is a gap in studies that involve cleaners in the co-design of more ergonomic tools and hospital interiors to improve usability and comfort. Therefore, studying ergonomical problems among cleaners fill small of gap found in developing countries. Thus, the goal of the current study was to assess ergonomic hazard exposures and associated factors among hospitals cleaners in eastern Ethiopia.
Methods
Settings and Period
The study was conducted from May 2023 to August 2023 in 8 government hospitals in eastern Ethiopia. The eastern part of Ethiopia along study settings were selected based on the proximity and resources availability of the author. In this study, eastern Ethiopia included the entire Harar area, the Dire Dawa federal administrative city, the Oromia region, and a portion of the Somali region. These hospitals are restricted to general hospitals, referral hospitals, and university teaching hospitals. They were selected among other health care settings based on service providing, patient load and human power that influence the cleaning tasks on cleaners. Accordingly, 8 public hospitals were selected at random from a total of 14, with each region having an equal chance. Two of hospitals were designed select from 1 region in order to ensure the sample is representative of the locations and to maximize the response rate, adapted from Banerjee and Duflo. 17 In 8 hospitals, the mean and standard deviation (Mean ± SD) by bed occupancy were 269.5 ± 132.6 per day, according to the liaison’s report. In the meantime, the mean ± SD for inpatients and outpatient flow in these chosen hospitals were 233.9 ± 125.4 and 154.4 ± 67.4, respectively. Consequently, in 8 hospitals, there are 388.3 ± 190 both inpatients and outpatient. 18
Study Design
Hospital based cross section study design was applied.
Study Population
All hospital cleaners working in general to referral hospitals in Eastern Ethiopia served as study population.
Study Target
All hospital cleaners employed by chosen governmental hospital facilities from general to referral hospital in eastern Ethiopia were studied.
Inclusion and Exclusion Criteria
All hospital cleaners who worked in selected public hospitals were included. Consequently, cleaners maintain the cleanliness of the patient wards and restrooms were included in this study. The survey also selected individuals who were employed for a year, whether they were contracted, permanent working as cleaners, garbage collectors, or emptier. However, cleaners who worked in the administration building, cafeteria, and gardens, as well as those on yearly, sick, or maternal leave, were excluded from the study. Also, the other workers with musculoskeletal disorders outside of work were excluded from the study.
Sample Size Determination
The sample size required for the study was calculated using a single population proportion formula by considering an estimated prevalence of work-related stress to be 45.2%, 19 from the study conducted in Bahir Dar Textile Factory north-west Ethiopia, a 5% margin of error, a 95% confidence interval, and 10% non-response rate which was became 381. To get sufficient and representative of each region by using design effect size of 2.0, the final 762, which was close to the overall hospital cleaners actively working in 8 hospitals (n = 741). So that the final sample size was 741 hospital cleaners, which were recruited for the study.
Sampling Procedures
Eight public hospitals were randomly selected using lottery methods from 14 public hospitals of 4 locations/regions of eastern Ethiopia. Two of hospitals were designed select from 1 region in order to ensure the sample is representative of the locations and to maximize the response rate, adapted from Banerjee and Duflo. 17 Accordingly, 176 of SWs were included from Haramaya University Hiwot fana Specialized Comprehensive Specialized hospitals, 41 from Jogula general hospital, 32 from Sabian general hospital, 34 from Bisidimo general hospital, 42 from Chiro general hospital, 128 from Dilchora Referal hospital, 225 from Jigjiga University Sheik Hassen Yabre Referral hospital, and 63 from Karamara general hospital
Study Variables
Dependent variable was ergonomic hazard exposures for last 12 months due to working conditions within the hospitals the measurement tool was rated by Nordic Questionaries pursued to has YES [1] and NO [0], adapted.20,21 While, the independent variables were socio-demographic variables (age [>18years], sex, educational status, work experience, job rotation ([shift 1, morning], shift 2, day & Shift 3, night]), marital status [married, single/separated], and monthly income). The individual variables (Knowledge and attitude). The representative questions about knowledge of on ergonomics hazard exposure was assessed using Boolean Logical question by YES/NO and using mean, it converted into poor (<mean), fair (mean) and good (>mean), adapted from previous study. 22 The 1 generalized question about attitude on ergonomics hazard exposure was assessed using 3 Likert scale (Disagree, Neutral, and Agree) and using median, then converted into negative (<median), neutral (equals median) and positive (>median). The other variable is institutional variables (ergonomical/workplace training and supervision), behavioral variables (alcohol consumption, cigarette smoking, chewing khat (Green leaf consider as substance in use in Ethiopia), job stress, and sleeping disorder). These all questions were asked using Boolean Logical question by YES/NO, adapted from the previous study. 23 Working environment variables (Environmental and job satisfaction, working hours, workload, and social recognition). These all variables measured by Boolean Logical question and answer YES [1] and NO [0], adapted from the previous study. 24
Data Collection Tools
Ergonomical hazard exposures was measured using Boolean logic (YES [1]/NO [0], adapted from previous study. 20 The validated alpha Cronbach on this study for item of ergonomical hazard exposures was 0.83. Behavioral factors such as sleep disorders, heavy alcohol consumption, chewing Khat and smoke cigarette were assessed using Boolean Logic (YES [1]/NO [0], adapted from Manzar et al. 23 The safety factors such as occupational health and safety, working hour per a day, workload. 25 The physical indicators such as muscular pains, tremors, palpitations, diarrhea, sweating, respiratory distress, dizziness, indigestion, headaches, backache, poor sleep, loss of libido, increased heart rate, raised blood pressure, and dry mouth and throat were evaluated using Boolean Logic (YES [1]/NO [0]).
Data Collectors and Supervisors
Face-to-face interview was demonstrated. Eight data collectors participated in data collection. Four (4) MSc in environmental health and Occupational health, 4 MPH in public health were recruited for data collections. Meanwhile, 4 supervisors were recruited for 8 selected public hospitals to supervise the data collection procedures. Before data collections, all data collectors and supervisors were received proper training how to collect data, handle the participants as well as how to handle the challenges while they collect data within daily bases.
Data Collection Procedures
Following study approval from public hospitals, 8 data collectors and 4 supervisors were assigned to the collection sites. Data collectors were informed about 3-shifts for the cleaners in hospitals. Through the year, the duration and continuity of the shifts among the cleaners are varied (ranges a month to 3 months) from hospitals to hospitals. But, within 24 h, the time for each shift for their work assignment is similar. Accordingly, the first shift starts at 7:00am and ends at 12:00am. The second shift starts at 1:00pm and ends at 5:00pm. The third shift starts at 12:00pm to 6:00am. This group works on schedule for two consecutive days and then rests for 2 days. By considering this, the questionnaires were administered (Morning: 9:00am-10:00am) for shift 1. For shift 2, the interview was done (Afternoon: 3:00pm-4:00pm]. The same method was done for shift 3 on 2 days because they don’t do for 24 h if they work at night.
Data Quality
For quality management, at the beginning, after a review of the literature on work stress or job stress, the questionnaires were created. Then, standard, structured English questionnaires with both closed-ended and open-ended questions were created for each goal in order to ensure the quality of the data. After that, the text was translated into 3 regional languages according to local tastes. Second, 8 supervisors and data collectors were assigned from related professions. Third, supervisors and data collectors received enough training on how to handle participants and complete surveys, especially those that focused awareness of occupational or job-related stress. Using appropriate terminology, concepts, and statistical models, the fourth objective is to finish the reliability and validity study of quantitative data.26,27 In order to guarantee the usefulness and lucidity of the questionnaires and to prevent misunderstandings in the data collecting measuring tools, a pretest study (5%) was carried out among the employees of Haramaya general hospital. Sixth, information from those whose data quality was subpar was immediately eliminated throughout the screening phase.
Ethical Statement
The Institutional Health Research Ethics Review Committee [IHRERC] at Haramaya University College of Health and Medical Sciences (CHMS) gave its approval to the study (Ref: IHRERC/064/2023). Every participant and hospital administration gave their informed, voluntary, signed, and written consent. Therefore, in accordance with Helsinki protocol, all of the information provided was kept confidential and secure. It indicates that no information exists that would allow for the participants’ precise identification. The results of the study are not specific to any 1 person; rather, they apply to the entire study group. To avoid names showing up, the questionnaire was coded.
Data Analysis
After data collection finalized, the data management and processing were the other activities. Accordingly, Coded quantitative data was double-entered, checked, and cleaned using Epi-Data 3.1. After that, Stata 17MP was used to export the data. Two statistical analyses were used. Initially, descriptive statistics were applied to determine the frequencies, proportions, and percentages (categorical variables) and mean, median, and standard deviations (continuous variables). The missing variables were imputed by mean of the variables across the column. To ascertain the relationship between independent factors and dependent variables, a second analytical statistical analysis was conducted. Because the data for dependent variable was binomial, binary logistic regression was applied during the bivariate and multivariate phases of the research. Fourteen variables were the candidates for the multivariate analysis at binary logistic regression analysis with the P-value of .20.
The crude odds ratio (COR) and adjusted odds ratio (AOR) with a 95% confidence interval (CI) were presented. Then, determinants having an AOR with a P-value of .05 were reported (95% CI). The variance inflation factor (VIF), which measures how an independent variable’s variance is associated with the others with a cut-off point of less than 10, 28 was used to test for multicollinearity. In addition, Hosmer and Lemeshow (HL) goodness of fit test was employed for regression model fit, where HL with a small chi-square value with a P-value more than .05) was approved according to Hosmer et al. 28 interpretation.
Result
Sociodemographic Characteristics
In the current study 679 (91.63%) of the 741 public hospital cleaners replied. About 9% (62 cleaners) did not respond, despite efforts to reduce non-response bias by developing a smooth approach, keeping questions brief, and closing the loop (The reason is explained discussion). Nearly 99% of these were female, and 97% were permanents. Of them, roughly 48% were in the 24- to 35-year-old age range, 69% were married, and 50% worked the first shift (morning). These mean ± standard deviation (SD) were 34.28 ± 7.46 years, 6.72 ± 6.52 grade, 6.80 ± 2.50, and 35.50 ± 6.17 Unites state dollar (1967 ± 342 Ethiopian currency) for age, work experience, education, and monthly income compensation, respectively (Table 1).
Sociodemographic Status of Selected Public Hospitals’ Cleaners in Eastern Ethiopia, 2023.

Note. Level salary I*($21.35 = 1100ETB); Level V** ($43.80 = 2344ETB), Levels of civil service salary based on national Job Evaluation and Grading [JEG], 2019 (Where 1Dollar ($) = 55.45 ETB, September, 2023).
Prevalence of Ergonomics’ Exposures
The current study found that self-reported ergonomic exposures among cleaners in public hospitals was 40.35% (95% CI: 36.64-44.15). The main 5 leading causes of ergonomic exposures among cleaners were overstretching while pushing cleaning materials (55.79%), overstretching while pulling cleaning materials (65.40%), lifting cleaning materials and others (58.50%), pushing waste materials (65.90%) and standing more than 4 h during the cleaning (57.60%; Table 2).
Descriptive Information for Self-Reported Ergonomic Exposures, Causes and Symptom Among Cleaners in Public Hospitals, 2023.

Binary Logistic Regression Analysis
Binary logistic regression found that male cleaners were more likely to exposed to ergonomically hazard (AOR: 9.04; 95% CI: 1.45-34.69) as compared to female cleaners. In the same analysis, hospital leaners those worked in the morning (shift 1; AOR: 1.70; 95% CI: 1.25-2.32), more than 35 years old (AOR: 1.55; 95% CI: 1.12-3.45), having working experience more than 6 years (AOR: 2.46; 95% CI: 1.55-3.90) were more likely to exposed to ergonomically hazard as compared to their counterparts. In addition, those have poor knowledge about ergonomic exposures (AOR: 4.16; 95% CI: 1.88-9.18), negative about ergonomic exposures (AOR: 1.43; 95% CI: 1.04-1.97) were more likely to exposed to ergonomically hazard as compared to their counterparts. Besides, those having behavioral characteristic such as sleeping disorders (AOR: 1.27; 95% CI: 1.02-3.45), heavy consumption of alcohol (AOR: 2.50; 95% CI: 1.41-4.43) and smoking cigarettes (AOR: 2.89; 95% CI: 1.67-4.99) were more likely to exposed to ergonomically hazard. Furthermore, those haven’t conducive environmental, namely presence of workload (AOR: 4.32; 2.96-6.30), having job stress (AOR: 3.17; 2.25-4.46) and have poor social recognition and work based violated (AOR: 1.97; 95% CI: 1.43-2.70) were more likely to exposed to ergonomically hazard while they are working within the hospitals. As contrasts, those have regular supervision (AOR: 0.44; 95% CI: 0.31-0.64) and working less than or equals to 8 h per a day (AOR: 0.44; 95% CI: 0.31-0.62) were reduce the chance of ergonomically hazard exposures as compared to those haven’t daily supervision and worked more than 8 h per a day (Table 3).
Binary Logistic Regression Analysis Model for Predictors of Ergonomic Hazard Exposures Among Hospital Cleaners, 2023.
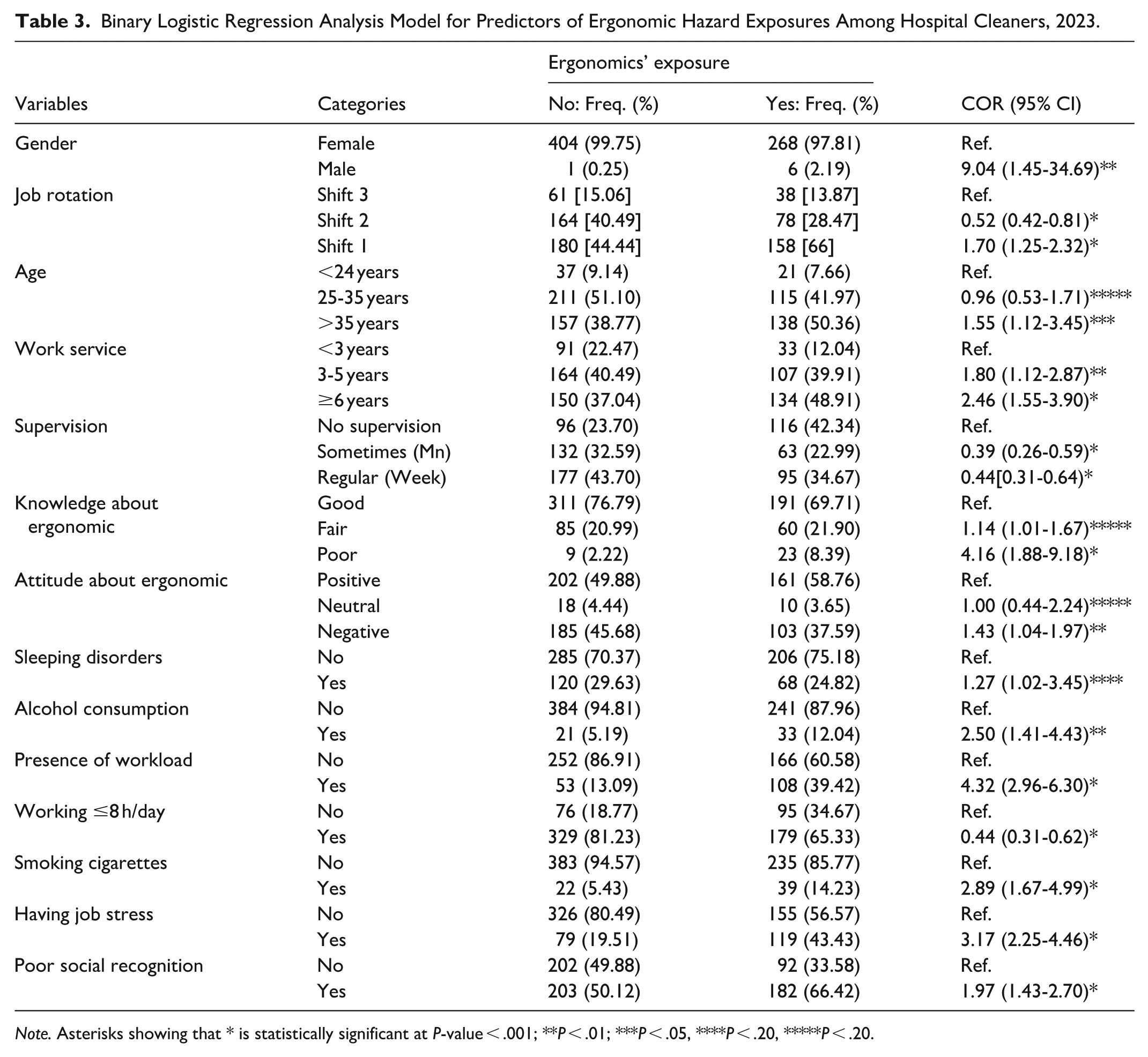
Note. Asterisks showing that * is statistically significant at P-value < .001; **P < .01; ***P < .05, ****P < .20, *****P < .20.
Multi-Variable Logistic Regression Analysis
The multi-variable logistic regression analysis model found that hospital cleaners those have greater than 6 years working experiences (AOR: 1.90; 95% CI: 1.12-3.21), those have poor knowledge about ergonomic (AOR: 6.68; 95% CI: 2.83-15.76) and having workload (AOR: 2.98; 95% CI: 1.58-5.60) were more likely to expose with ergonomic hazards as compared to their counter parts. On other hands, the mode found that hospital cleaners those worked afternoon (AOR: 0.60; 95% CI: 0.40-0.89) were reduce the chance of ergonomically hazard exposures by 40% as compared to those worked in night (shift 3). In same analysis, have sometimes supervision (day-week; AOR: 0.36; 95% CI: 0.21-0.65) were reduce the chance of ergonomically hazard exposures by 64% as compared to those haven’t supervision during their cleaning time. Moreover, hospital cleaners those worked less than 8 h per a day (AOR: 0.63; 0.21-0.92) were reduce the chance of ergonomically hazard exposures by 64% as compared to those have greater than 8 h per day (Table 4).
Multi-variable Logistic Regression Analysis Model for Predictors of Ergonomic Hazard Exposures Among Hospital Cleaners, 2023.

Note. Asterisks showing that * is statistically significant at P < .001; **P < .05; ***P > .05.
Discussion
The aim of the present study was to assess prevalence of ergonomic hazard exposures and association among public hospitals’ cleaners in eastern Ethiopia. In this study, out of 741 hospital cleaners, 679 people responded the questionnaires. The remaining, 9.13% (62 cleaners) did not respond, despite efforts to reduce non-response bias by developing a smooth approach, keeping questions brief, and closing the loop. The following were the main causes: 33% of them said the study would not provide a wage raise, 17% said there was no time for the interview, and 12% said we shouldn’t reveal our hospitals that seemed to be complaint institutions.
The current study highlighted that nearly 4 out of 10 hospital cleaners in Eastern Ethiopia experience ergonomic hazard exposure—such as heavy lifting, awkward postures, and repetitive tasks—implies a critical need for targeted, immediate, and systemic preventive measures. This high prevalence of ergonomic risks is strongly linked to work-related musculoskeletal disorders high workload, long working hours, and lack of training. When it compares with previous, it is slightly similar to 42.8% reported from India, Joseph et al, 29 ; and lower than 19% in Texas, reported by Salwe et al, 30 and 32% reported from Taiwan. 7 However, it is lower than 52% 31 ; and lower than 57.2% 32 reported from Ethiopia’s hospitals, 77%—Nigeria hospitals Adebusoye et al, 33 56%—Norway’s hospitals Lasrado et al, 34 82%—Thailand’s hospitals Laithaisong et al, 35 74%—UK hospitals, 36 and 77%—Malaysia hospitals. 37
This does not imply that the current study units are getting adequate ergonomics principle, well work design or adequate occupational health and safety services. But the discrepancy might be due to socio-economic of low and high-income countries due to factors like occupational differences and access to ergonomic interventions.38 -42 Because effectiveness of ergonomic interventions, where previous research has demonstrated the potential of ergonomic interventions to reduce risk of ergonomic.42,43 The other discrepancies could be due to safety factors such as PPE compliance and OHS training, where adherence to safety regulations and awareness of ergonomic principles have reduced risk of ergonomic in comparison to those who did not comply with safety protections.44 -46
The overall the current finding indicates that there is lack of ergonomic principles and presence of improper work design among the public hospitals where cleaners are working. In addition, this percentage showed that it raised the risk of infection since cleaners are more susceptible to biological dangers while handling hospital trash due to ergonomic strain and inadequate, dangerous methods, which is also indicated by previous study. 47 The implication of this result can cause pain, disability, increased absenteeism, and lower productivity. 3 As the result, this suggests that policy ramifications of ergonomic exposures among cleaners requiring the use of controls like task rotation and ergonomic equipment, developing training programs on safe practices and symptom reporting, enforcing laws regarding load limits and breaks, and requiring employers to maintain records of these procedures. 48 The other policy implication of this finding, it necessitates the regulations mandating ergonomic exposures assessments and controls like adjustable tools and job rotation, which was also explained by previous study. 49 Therefore, it is important to ensuring workers receive training on ergonomics prevention, promoting early reporting of symptoms, and establishing systems for continuous evaluation and improvement of safety programs to prevent its health outcomes. 16
In this study the main leading causes of ergonomic exposures among cleaners were overstretching while pushing cleaning materials and overstretching while pulling cleaning materials. Because it is accurate to say that overstretching when pushing and pulling cleaning supplies was the primary source of ergonomic hazards for cleaners. Out reaching, extending, and pushing and dragging large, heavy objects are all recognized as important risk factors for developing musculoskeletal diseases among the workers. 50 Moreover, standing more than 4 h during cleaning was one of the main leading causes of ergonomic exposures among hospitals cleaners because it poses risks like foot pain, varicose veins, back pain, and joint strain due to prolonged pressure and blood pooling. 51 Furthermore, awkward postures also reported among the current hospital cleaners, which is consistence with previous study. The causes are awkward postures, repetitive motions, and the force needed to complete a task are examples of ergonomic hazard exposures, which are working circumstances that raise the risk of musculoskeletal disorders among workers. 50 According to this study found that the common ergonomic exposures are awkward postures, heavy lifting, repetitive motions, and inadequate work design, resulting in symptoms like chronic back and neck pain, which can significantly impact a cleaner’s quality of life. 52
Multi-variable logistic regression analysis model found that hospital cleaners those have greater than 6 years working experiences were more likely to increase ergonomic exposures nearly by 2 times as compared to those have less than 3 years working experiences. This finding consistence with previous study where the longer working service among the workers could increase the risks of ergonomic, which is directly associated with musculoskeletal disorders. 53 The other study also revealed that longer service often involves prolonged exposure to tasks like repetitive motions, awkward postures, heavy lifting, and prolonged static positions. 54 According to this study all studies, there are a lot of significant factors of ergonomic hazard exposures that directly contribute to the development of work-related musculoskeletal disorders affecting the low back pain, upper back pain, neck, elbow, shoulders, and other body parts.
The model also found that hospital cleaners those were poor knowledge about principle, rule as well as application of ergonomics were more exposed as compared to those have good understanding about it. Because they can’t understand, adapt to, and avoid ergonomic hazard exposures factors such unpleasant postures, repetitive motions, and excessive force, workers without ergonomics competence are more likely to suffer from work-related impairments. 55 The other study also confirmed this hypothesis as it stated, misinformation, people are more likely to lift things incorrectly or sit in hazardous positions, which increases their risk of musculoskeletal disorders, chronic pain, and accidents. 56
Preventive Implication of the Study
The study highlights this study has certain preventive implications for national policy and proclamation, future research, future initiative of ergonomic principle and occupational health and safety and the subject matter across the national level including study eastern part of Ethiopia. Therefore, the main domain of preventive implication of this study will be illustrated as below.
Implication of the Study for the Hospitals
The current finding revealed that there was high magnitude of ergonomic exposures that there is an indication of high tendency of the cleaners’ potential to develop musculoskeletal disorders risks while working in a hospital setting. This suggests that hospitals would be expected to implement interventions through education and training in order to reduce, avoid, and manage occupational dangers in the future.
Implication of the Study for Policy
The current study has a valuable policy implication because it offers relevant information on unsafe workplace, improper work design, poor occupational health and safety measures practice at hospitals’ workplace. These type of workplace apparently contradicted national Article 92, in which it states that an employer’s fundamental duties include implementing all necessary measures to ensure that workplaces healthy and safety, and free from hazards to employees’ well-being. 57 Also, the study has an implication on the national proclamations practice about ergonomical and occupational health and safety management. This study indicated revealed that there is no management of ergonomical outcomes, no guidelines for safeguarding and preventing risks among cleaner in hospitals. It means that these conditions are not put into practice at hospital levels and as a result, future policy enforcement is required to ensure the health and safety of these staff members, which may also apply to the other hospital staffs. But Ethiopia has been ratified occupational injuries management treatment proclamation (Article 47), provided safety measures (Article 48), compensation principles, and types of disabilities (Articles 49–53). 57
For the Data Records and Future Initiatives
Even in the absence of clinical data on reporting ergonomic hazard exposures from the hospitals and absence of labor statistics from the regions are the indication of policy gap that should be considered for the future.
For the Subject Matter
Assessing occupational related ergonomic hazard exposures are the thematic works of occupational health and safety, environmental health and public health fields. Consequently, the results provide valuable insights for education and training programs as well as it serves as a foundation for the future ergonomic principle, rules and occupational health and safety (OHS) studies on these areas.
For the Future Study
As the current findings rely on self-reported data, the future research modality will incorporate clinical data records and/or longitudinal data to provide more definite evidence than what is currently available. As closed, the preventive implications and interventions are implementation of ergonomic training; workplace redesign and engineering controls (assistive equipment and task modification); administrative controls and job design (job rotation and workload management); strengthening occupational health policies (supervision and safety policies); and health and wellness programs.
Limitations of the Study
Though the current study has important findings, but it has following limitations, which would be expected to address in the next future studies. The first one is the current findings only obtained from self-report of hospital cleaners in the selected public hospitals over a year—this might be lead recall or memory bias. There are no reported data or clinical data from the health care settings as well as from regional bureau of labor statistics—these factors made limitations on the findings to triangulate the information and to bring more supportive evidences. The second, body mass index of the participant is expecting the main causes of ergonomics exposures among cleaners, therefore the current study couldn’t assess this factor, in which the future study would be considered. The third, evaluating the variables with a single item (Yes/No) may result in a greater or narrower range of likely outcomes—which in turn reduces the validity and accuracy of the values. The fourth the study’s scope was confined to the outcomes among hospital cleaners in a specific public hospital—that didn’t guaranty for other occupational health outcomes among hospital cleaners. The fifth, it’s possible that the hospital cleaners withheld the outcomes of their answer out of concern that it would harm the reputation and competitiveness of the hospitals they work with—this would be affecting future decision for the correction of poor work-related stress management misconduct. The sixth the study was cross sectional nature that prevented the establishment of a causal relationship between variables. Therefore, longitudinal studies be conducted in the future
Conclusion
This study concludes that nearly 4 out of 10 hospital cleaners were experienced with ergonomical hazard exposures. These working groups are at serious exposures for ergonomic hazards, which mostly result in musculoskeletal conditions like arm, back, and neck discomfort and strains at the long run. This study found that awkward bodily postures (bending, kneeling, squatting), heavy lifting, repetitive actions, and extended static positions are the causes of these dangers, which are sometimes made worse by time constraints and demanding workloads. The probability and severity of these work-related problems might be raised by elements such as non-ergonomic equipment use, poor workstation design, and insufficient training. The current study identified that poor knowledge about ergonomics’ exposures, sedentary working experience, working more than 8 h per a day and presence of workload were significantly associated with exposures of ergonomically hazards among hospitals cleaners. Thus, the findings advised that a comprehensive strategy from both policy makers and hospital is very vital to address the root causes of ergonomic exposures, promote cleaner’s retention, and improve the quality of their well-being of cleaners.
Footnotes
Acknowledgements
I acknowledged Institutional Health Research Ethics Review Committee [IHRERC] at Haramaya University College of Health and Medical Sciences for ethical approval for the targeted study.
Ethical Considerations
The study was approved by the Haramaya University College of Health and Medical Sciences, Institutional Health Research Ethics Review Committee (Ref ID: IHRERC/064/2023). Each Hospital were communicated about the study requesting their cooperation through a formal letter from the college. Each hospital has also given institutional consent for collecting health facility related data. All study participants were asked for their consent and sign on the consent form for their agreement to be part of the study (ie, written type of consent). The confidentiality of the individuals was upheld in compliance with the Helsinki Protocol.
Author Contributions
STT conceived of the presented idea and conceptualized the proposal, collected data, STT developed the theory and performed the computations. STT verified the analytical methods and write the manuscript and revise the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
I consent the data deposit in a public repository that meets appropriate standards of archiving, citation, and supplement information files under alongside of the manuscript. The data can provide an explanation and details of any restrictions on access if data are not freely available, and acceptable justifications for restricting access may include legal and ethical concerns.