
Abstract
This study examined how multidimensional poverty—combining income deprivation and time poverty (working >52 paid hours per week)—is associated with metabolic syndrome (MetS), and whether these associations vary after accounting for employment structure and behavioral risk factors. We conducted a pooled cross-sectional analysis of the Korea National Health and Nutrition Examination Survey data (2013-2023), including 34 650 economically active adults aged ≥19 years. Sex-stratified hierarchical logistic regression models sequentially adjusted for employment type and behavioral risk factors. Among men, time poverty was associated with a higher probability of metabolic syndrome in partially adjusted models (+3.22 pp, P = .009), but this association attenuated after full adjustment (+1.86 pp, P = .125). Among women, dual poverty (+4.53 pp, P = .001) and income-poverty-only (+2.73 pp, P < .001) remained significantly associated with metabolic syndrome in fully adjusted models, whereas time poverty was attenuated (+2.79 pp, P = .065). Self-employment was independently associated with metabolic syndrome in both sexes (P < .001). Associations between poverty type and metabolic syndrome differed by sex and varied across levels of adjustment. The findings indicate that employment structure and behavioral factors are important in interpreting observed associations between multidimensional poverty and metabolic risk.
Keywords
Introduction
Poverty is widely recognized as a fundamental social determinant of health that reflects structural inequality beyond material deprivation. 1 Within this framework, poverty arises from unequal access to power, money, and resources across the conditions in which people are born, grow, live, and age. Although poverty is increasingly described as multidimensional, policy and empirical research have largely operationalized it in economic terms—typically as insufficient income or material resources to meet basic needs. 2
Time is a finite and unequally distributed resource that shapes opportunities for rest, care, and health-promoting activities.3,4 “Time poverty,” refers to an insufficient discretionary time remaining after paid and unpaid work obligations are fulfilled. Research in time-use epidemiology demonstrates that limited discretionary time constrains health-supportive behaviors and contributes to physiological stress.3,5 When poverty is defined solely in material terms, such temporal constraints may remain overlooked, increasing the likelihood that behavioral differences are attributed to individual choice rather than unequal access to resources. 5
Metabolic syndrome (MetS) represents a relevant health outcome for examining how income and time constraints may be linked to chronic metabolic risk. As a cluster of interrelated conditions—abdominal obesity, hypertension, insulin resistance, and dyslipidemia—MetS greatly increases the risk of cardiovascular disease, type 2 diabetes, and premature mortality. 6 Globally, its prevalence among adults ranges from 14% to 39%, accounting for a substantial portion of the global burden of noncommunicable diseases. 7 Because MetS is closely linked to diet, physical activity, alcohol use, and smoking—behaviors shaped by access to material and temporal resources—it provides a lens for examining how resource inequalities may become physiologically embodied.
While traditional models emphasize modifiable behavioral risk factors, these behaviors are socially patterned rather than purely individual choices. Access to material resources and discretionary time shapes the opportunity to exercise, prepare healthy meals, or avoid harmful coping behaviors such as smoking or binge drinking. Without considering such resource constraints, health behaviors may be misinterpreted as individual failures rather than patterned responses to unequal conditions. Accordingly, behavioral practices partially account for the association between multidimensional resource deprivation and metabolic outcomes.
Resource constraints, however, do not operate in isolation. Income and time are organized within broader institutional contexts, including employment structures that shape working hours, employment stability, income security, and schedules control. These institutional arrangements influence not only the quantity of resources individuals possess but also their predictability and usability in everyday life. In this way, structural conditions may affect material and temporal deprivation, which are experienced and translated into behavioral and physiological risk.
Gender further differentiates these processes. Rather than assuming uniform vulnerability, it is plausible that men and women experience distinct linkages between resource deprivation and metabolic risk. Women’s disproportionate responsibility for unpaid care and concentration in flexible or precarious employment may intensify the interaction between time scarcity and material constraints. 8 Men, conversely, experience intense work demands and long hours under the normative pressures of the breadwinner role and influence health-related practices, including alcohol use or reduced self-care. These gendered arrangements suggest that the association between multidimensional poverty and MetS may operate through partially different behavioral and structural configurations for men and women.
Despite increasing recognition of these dynamics, empirical research simultaneously examining income deprivation, time poverty, structural labor market context, and MetS remains limited. Identifying how a combination of income and time constraints clusters within the employment structure is relevant for informing labor, social protection, and health policy. South Korea provides a pertinent context for such an investigation. Among the Organization for Economic Cooperation and Development (OECD) nations, Korea has consistently recorded some of the longest average working hours and one of the most pronounced gender gaps in unpaid care work.9,10 These conditions make Korea a useful case for examining how income and time resources intersect within structured institutional environments to shape metabolic health.
Building on this context, the present study develops a sex-specific explanatory model linking multidimensional poverty—including both income and time deprivation—to metabolic syndrome. Rather than predicting individual risk, the study disentangles the structural and behavioral pathways through which resource scarcity is translated into metabolic outcomes and evaluates the relative contribution of each pathway by sequentially modeling structural conditions and behavioral factors. Using nationally representative data from the Korea National Health and Nutrition Examination Survey (KNHANES), we examine how income and time resources, institutional context, and health-related behaviors jointly shape sex-differentiated patterns of MetS.
By clarifying whether structural constraints or behavioral practices account for a greater share of metabolic risk—and whether these mechanisms differ by sex—the model identifies actionable entry points for policy intervention. Given the rising burden of metabolic disorders and persistent gender disparities in labor and time allocation, distinguishing these pathways is essential for designing targeted, gender-responsive strategies in labor, social protection, and chronic disease prevention. By situating metabolic risk within broader resource and structural conditions, this study contributes to policy discussions on equitable and gender-responsive approaches aligned with the Sustainable Development Goals (SDGs 3, 5, 8, and 10).
Methods
Database Information and Study Population
The Korea National Health and Nutrition Examination Survey (KNHANES) is a nationally representative cross-sectional survey conducted by the Korean Disease Control and Prevention Agency (KDCA). It was designed to assess the health and nutritional status of the Korean population. It comprises health interviews, health examinations, and nutrition surveys using a stratified multistage probability sampling method.
This study utilized secondary data from the sixth (2013-2015), seventh (2016-2018), eighth (2019-2021), and ninth (2022-2023) waves of the KNHANES spanning 11 years. Data from health interviews and examination surveys were integrated to create a pooled dataset.
The study size reflects the number of eligible participants available in the pooled KNHANES dataset after applying predefined inclusion and exclusion criteria. From the pooled sample of 82 970 individuals, participants younger than 19 years were excluded to ensure consistency with adult metabolic syndrome criteria. Because time poverty and employment type were defined based on labor market participation and weekly working hours, individuals who were not economically active were also excluded. Additional exclusions were applied for missing poverty variables (household income or weekly working hours) and missing outcome data. For covariates, missing responses were retained as separate categories in the regression models.
The final analytic sample comprised 34 650 economically active adults aged 19 years and older. The number of participants by year ranged from 2813 in 2023 to 2981 in 2013, with an approximately uniform distribution over time. The same analytic sample was used for all regression analyses to maintain comparability across models and to minimize bias arising from differential missing. A detailed flow diagram of the sample selection process is presented in Figure 1.

Flow of study sample selection from pooled KNHANES 2013-2023 data. The initial pooled sample included 82 970 individuals. Participants younger than 19 years and those not economically active were excluded. Additional exclusions were applied for missing poverty variables (household income or weekly working hours) and missing outcome. The final analytic sample (N = 34 650) was used consistently for the interaction analysis and hierarchical regression models.
Data Collection and Variables
The KNHANES data were collected annually by trained field staff using standardized procedures. Health interviews were conducted face-to-face or via self-administered questionnaires, and health examinations were performed by medical professionals using mobile examination centers equipped with clinical diagnostic instruments. Data collection quality was ensured through ongoing training, supervision, and quality control protocols managed by the KDCA.
All questionnaire-based variables used in this study were derived from the standardized KNHANES, administered by the KDCA. The survey instruments and measurement protocols are nationally standardized and publicly documented. No newly developed or modified questionnaires were used in this analysis.
Metabolic Syndrome (MetS)
The dependent variable was MetS, which was defined according to the International Diabetes Federation (IDF) criteria. 11 Participants were classified as having MetS if they met the criterion for abdominal obesity (waist circumference ≥90 cm for men and ≥80 cm for women) and at least 2 of the following additional risk factors: elevated triglycerides (≥150 mg/dL), low HDL cholesterol (men < 40 mg/dL, women < 50 mg/dL), elevated blood pressure (≥130/85 mmHg), or elevated fasting glucose (≥100 mg/dL). These thresholds represent cardiometabolic risk-factor cut-offs used to identify clustered abnormalities and do not correspond to clinical diagnostic criteria for hypertension or diabetes. All indicators were derived from health examination survey data, including anthropometric measurements of waist circumference and blood test results for triglyceride, HDL cholesterol, and fasting glucose levels. Individuals who did not meet these criteria were classified as having no MetS. This variable was coded as binary (yes or no).
Poverty Type
The primary independent variable was the type of poverty. Rather than analyzing income and time poverty separately, a categorical variable was constructed that combined both dimensions. This approach integrates the income and time dimensions and facilitates the identification of intersecting poverty types. This categorization produced 4 groups: dual poverty (both income and time poverty), income poverty only, time poverty only, and no poverty.
Income poverty was defined based on household income adjusted for household size using equivalized income calculated by dividing total household income by household members. The threshold distinguishing income poverty was set at the 50th percentile of the sample distribution, which is consistent with the lower bound of relative poverty defined in Korea and the OECD statistical frameworks.
Time poverty was operationalized as working more than 52 h/week. This threshold reflects Korea’s statutory ceiling on weekly working hours and captures prolonged working exposure beyond regulated full-time employment. South Korea has historically exhibited comparatively long average working hours among OECD countries, and the 52-h ceiling was introduced to regulate excessive overtime. 12 By adopting this benchmark, the present study situates time poverty within the institutional labor context of Korea and emphasizes structural exposure to extended paid work rather than routine employment duration. To assess robustness, additional sensitivity analyses were conducted using alternative thresholds of 40 and 60 h/week (see Supplemental Tables S1-S4).
All data required to construct the poverty type variable, including household income, size, and average weekly working hours, were obtained from the health interview survey data.
Covariates
Employment type was included as a structural explanatory factor within the institutional pathway linking multidimensional poverty to MetS. Employment conditions are closely tied to socioeconomic disadvantages (eg, income and time poverty) and health outcomes.1,13 -15 Failure to account for employment type could lead to biased estimates by attributing health disparities solely to resource deprivation, which may also reflect differences in institutional resource arrangements and related exposures. Employment type captures the institutional organization of income security, working hours, schedule control, and access to social protection, which shape not only the quantity of resources available but also their predictability and usability in everyday life.16 -18 For example, precarious employment conditions such as irregular work, self-employment without security, or unpaid family labor are disproportionately experienced by socioeconomically disadvantaged groups and are associated with elevated stress and reduced access to health-promoting resources.18,19 Employment type was categorized as regular wage employment, irregular employment, self-employment, and unpaid family work.
Behavioral risk factors for MetS were included as a downstream behavioral pathway through which structural resource constraints may be translated into metabolic risk. Prior research has consistently identified behavioral factors such as physical inactivity, excessive alcohol consumption, and smoking as major risk factors for MetS.20 -23 Furthermore, these behaviors are socially patterned and shaped by individuals’ socioeconomic conditions.16,24 -26 Rather than conceptualizing them solely as individual choices, they are understood as patterned responses to structural conditions. This pathway was operationalized using 3 binary variables: physical activity, monthly binge drinking, and current smoking status. Participants were considered physically active if they engaged in at least 150 min of moderate-intensity physical activity, 75 min of vigorous-intensity activity, or an equivalent combination of both per week. This classification followed the global physical activity guidelines recommended by the World Health Organization (2010) as applied to the KNHANES dataset by the KDCA. 27 Monthly binge drinking was defined as the consumption of 7 or more drinks for men and 5 or more drinks for women on a single occasion, at least once a month during the past year. This definition was based on the criteria adopted by the KDCA in its national health statistics reporting and is widely recognized as the standard definition of binge drinking in Korean public health research, including the KNHANES and the Youth Health Behavior Survey. 9
Sex was also included both as an effect modifier and as a stratification variable, consistent with the study’s sex-specific explanatory framework. Numerous studies have shown that men and women may exhibit different vulnerability profiles to both poverty and MetS, reflecting gendered exposure to social determinants such as employment conditions, caregiving burdens, and behavioral norms.10,28 -31
Age and family history of chronic disease were treated as control variables representing non-modifiable physiological factors.6,32 Family history was categorized as yes, no, or don’t know. Age was coded as a continuous variable, with those aged 80 years or older grouped as 80, following the coding scheme provided in the original KNHANES dataset.
Statistical Analysis
All analyses were conducted using STATA/MP version 18.0 (StataCorp, College Station, TX, USA), applying sampling weights to account for the complex survey design of the KNHANES and ensure national representativeness. Because multiple survey waves (2013-2023) were pooled, the original sampling weights were divided by the number of pooled survey years in accordance with the KNHANES analytic guidelines to maintain appropriate population representation in the combined dataset. Standard errors were estimated using survey design–based methods appropriate for the KNHANES multistage sampling structure. This study was reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for cross-sectional studies. 33
A 3-stage analytical strategy was implemented. Descriptive statistics were used to summarize participant characteristics, and chi-square and Mann–Whitney U tests were employed to assess subgroup differences. Second, we included a sex-by-poverty interaction term in the logistic regression models to evaluate the sex-based differences in the association between poverty and MetS. Third, sex-stratified hierarchical logistic regression models were fitted to examine explanatory pathways. Model 1 included poverty type, age, and family history; Model 2 additionally included employment type to assess its structural contribution; and Model 3 further incorporated behavioral risk factors to evaluate behavioral effects. All regression models were adjusted for survey-year fixed effects to account for temporal variation across the study period.
Because these hierarchical models were compared sequentially, results were presented as Average Marginal Effects (AMEs), expressed as absolute changes in predicted probability. In nonlinear models such as logistic regression, odds ratios may vary across models due to rescaling when additional covariates are introduced, making direct comparison difficult. AMEs are less sensitive to this issue and provide more interpretable estimates of effect size. Statistical significance was set at P < .05.
To assess the robustness of the hierarchical modeling results with respect to the operational definition of time poverty, additional models were estimated using alternative thresholds of 40 and 60 h per week. In addition, perceived stress (self-reported high vs low) was included in supplementary models as an additional covariate to examine potential psychosocial confounding.
Results
Table 1 presents the descriptive characteristics of the study population, including unweighted sample sizes (n) and sampling-weight-adjusted percentages (%). Among the 34 650 economically active adults included in the final analytic sample, 51.6% were men (n = 17 885) and 48.4% were women (n = 16 765). The weighted median age was 49 years (IQR 37-60), with a statistically significant but modest difference between men and women (P = .006). Significant sex differences were observed in employment type, weekly working hours, and income distribution (all P < .001). Men were more likely to be regularly employed, self-employed, and to report longer working hours (≥41 h), whereas women were more frequently engaged in irregular employment and shorter working hours (<30 h). Women were also more represented in the lowest income quartile. The distribution of poverty type differed significantly by sex (P < .001). Dual poverty and time-poverty-only were more prevalent among men (25.6% and 28.1%, respectively), whereas women were more likely to experience income-poverty-only (34.3%) and no poverty (33.5%). Behavioral risk factors also showed significant sex differences (all P < .001). Men reported a higher prevalence of monthly binge drinking and current smoking, whereas women were more likely to be physically inactive. The overall prevalence of metabolic syndrome was 21.1%, with a significantly higher prevalence among men than women (22.8% vs 18.7%, P < .001).
Weighted Characteristics of the Study Population by Sex.

Values are presented as weighted percentages (%) with unweighted sample sizes (n) in parentheses; age is presented as weighted median.
P-values for categorical variables were obtained using survey-adjusted chi-square tests.
Age was compared using survey-adjusted Wilcoxon rank-sum tests.
Table 2 summarizes the results of the weighted logistic regression analysis examining the interaction between sex and multidimensional poverty in relation to MetS. The model was adjusted for age, family history and survey year. Using men with no poverty as the reference group, time-poverty-only was associated with higher odds of MetS among men (OR = 1.16, 95% CI: 1.02-1.33), whereas dual poverty and income-poverty-only were not statistically significant. Women in the no-poverty group had significantly lower odds of MetS compared with men (OR = 0.58, 95% CI: 0.53-0.64). Significant interaction effects were observed, indicating that the association between poverty type and MetS differed by sex. Specifically, the interaction terms indicate the additional effect for women beyond the main effects estimated for men (with men with no poverty as the reference). The significant positive interaction terms for dual poverty (OR = 1.92, 95% CI: 1.56-2.37), income-poverty-only (OR = 1.60, 95% CI: 1.40-1.83), and time-poverty-only (OR = 1.28, 95% CI: 1.01-1.63) indicate that, relative to men with no poverty, women in these poverty categories experienced a greater increase in odds.
Survey-Weighted Logistic Regression of Interaction Effects Between Sex and Multidimensional Poverty on Metabolic Syndrome. e

Odds ratio and 95% confidence intervals from survey-weighted logistic regression models.
The reference group was men with no poverty. Main effects of poverty type reflect associations among men, and interaction terms represent additional effects among women relative to men.
Poverty type was defined as 4-category variable combining income and time poverty.
Model adjusted for age, family history, and survey year fixed effects.
Overall model significance was assessed using a survey-adjusted Wald test: F(20, 1781) = 58.76, P < .001.
Figure 2 presents the predicted probabilities of MetS according to sex and poverty type. Among men, the highest predicted probability of MetS was observed in the time-poverty-only group, while the probabilities for dual poverty and income-poverty-only were closer to those of the no-poverty group. In contrast, among women, the highest predicted probability was observed in the dual-poverty group, followed by income-poverty-only and time-poverty-only, with the lowest probability in the no-poverty group. Although absolute predicted probabilities remained higher among men across most poverty categories, the relative ordering of poverty types differed by sex. These patterns visually illustrate the statistically significant interaction identified in Table 2, indicating that the distribution of metabolic risk across poverty types differs between men and women. Increasing age and a positive family history were independently associated with higher odds of MetS.

Predicted probabilities of metabolic syndrome by sex and poverty type. Predicted probabilities were estimated from survey-weighted logistic regression models including a sex-by-poverty interaction term and adjusting for age, family history, and survey year fixed effects. Solid lines represent men and dashed lines represent women. Among men, the highest predicted probability was observed in the time-poverty-only group. In contrast, among women, the highest predicted probability was observed in the dual-poverty group, followed by income-poverty-only and time-poverty-only, with the lowest probability in the no-poverty group. These patterns visually reflect the significant interaction between sex and poverty type reported in Table 2.
Table 3 presents the results of the hierarchical logistic regression models for men, illustrating the structural and behavioral pathways through which multidimensional poverty is linked to metabolic syndrome. Sequential adjustments were made for employment type (structural factor) and behavioral risk factors, and the results are presented as AMEs.
Hierarchical Logistic Regression Models Predicting Metabolic Syndrome Among Men. f

Model 1: adjusted for age and family history; Model 2: additionally adjusted for employment type; Model 3: further adjusted for lifestyle behaviors. AMEs are estimated using survey-weighted logistic regression models. All models additionally adjusted for survey year fixed effects.
AME = Average Marginal Effect; values indicate percentage-point change in the predicted probability of metabolic syndrome.
Bold values indicate statistical significance at P < .05.
Reference groups: No poverty, regular employment, no physical activity, no binge drinking, no smoking, and no family history.
N reflects complete-case observations for each model.
Overall model significance was assessed using survey-adjusted Wald tests: Model 1, F(16, 1779) = 17.54; Model 2, F(20, 1775) = 16.07; Model 3, F(26, 1769) = 16.51 (all P < .001).
In the Model 1 (adjusted for age, family history, and survey years), the time-poverty-only group had a significantly higher predicted probability of MetS (AME = +3.22pp, P = .009), whereas dual poverty and income-poverty-only were not statistically significant.
After additionally adjusting for employment type in Model 2, the association between time-poverty-only and MetS was attenuated but remained statistically significant (AME = +2.48pp, P = .042). In this model, employment conditions emerged as important correlates. The self-employment had a higher predicted probability of MetS (AME = +3.55pp, P < .001), whereas irregular employment showed a significantly lower probability (AME = −2.35pp, P = .009) compared with regularly employed counterparts. As shown in Supplemental Table S5, more than half of irregularly employed men were engaged in physically demanding occupations such as machine operation (28.95%) and elementary labor (23.08%). This occupational distribution may account for their lower predicted probability of MetS compared with regular workers, reflecting higher levels of occupational physical activity despite employment instability.
In the fully adjusted Model 3, which incorporated behavioral risk factors, the association between time-poverty-only and MetS was further attenuated and no longer significant (AME = 1.86pp, P = .125). Self-employment remained positively associated with MetS (AME = +3.27pp, P < .001), and irregular employment continued to show a negative association (AME = −2.06pp, P = .021). Among behavioral risk factors, physical activity was associated with a 4.31 percentage point lower probability of MetS (P < .001), monthly binge drinking with a 7.02 percentage point higher probability (P < .001), and current smoking with a 2.30 percentage point higher probability (P = .002). Across all models, age and family history consistently predicted higher MetS risk.
Table 4 presents the hierarchical logistic regression models for women, showing the AMEs after sequential adjustments for employment type and behavioral risk factors. In Model 1 (adjusted for age, family history, and survey years), dual poverty and income-poverty-only were significantly associated with higher predicted probability of MetS (AME = +5.88pp and +3.16pp, respectively; both P < .001). Time-poverty-only was also positively associated (AME =+4.00pp, P = .009).
Hierarchical Logistic Regression Models Predicting Metabolic Syndrome Among Women.
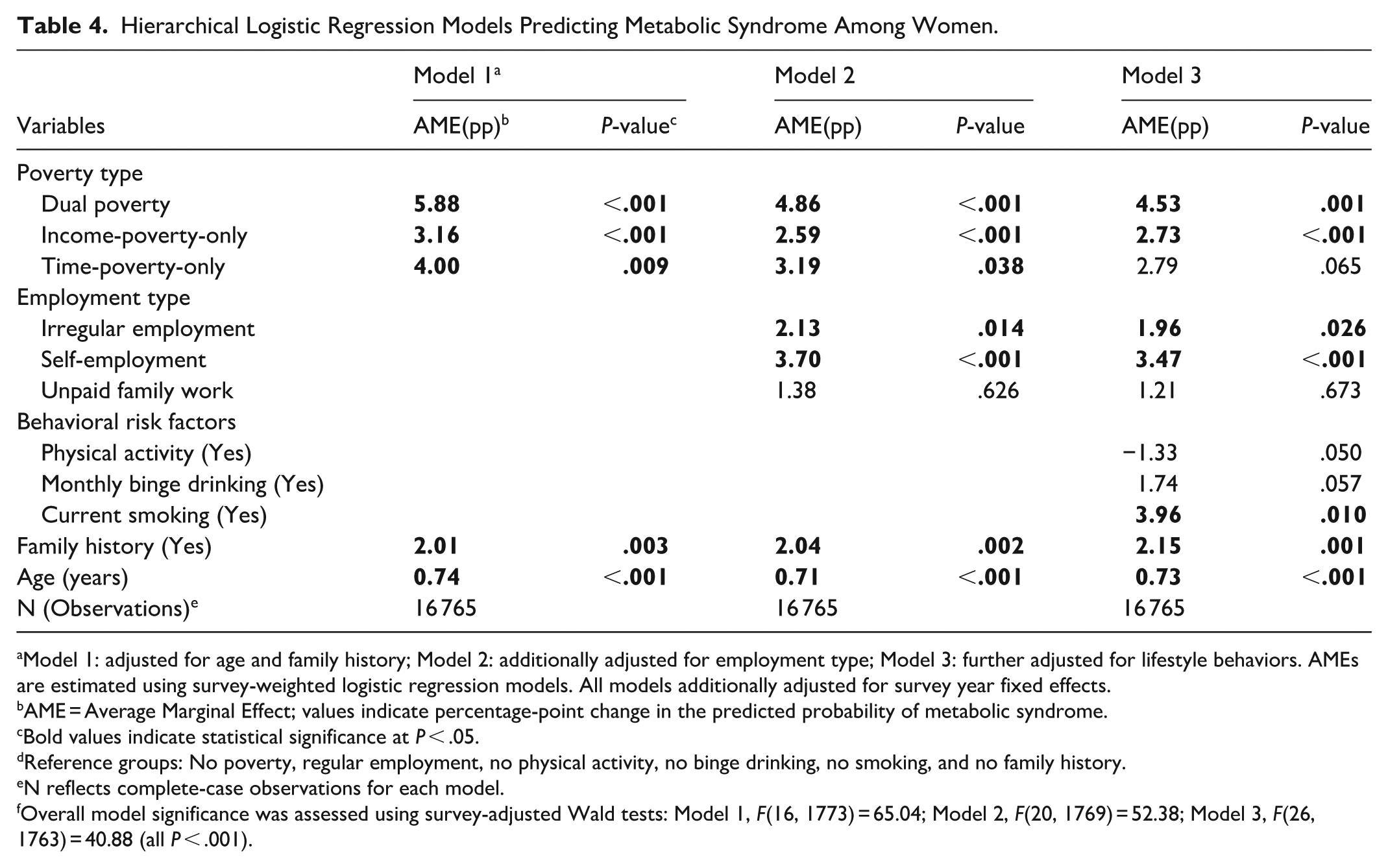
Model 1: adjusted for age and family history; Model 2: additionally adjusted for employment type; Model 3: further adjusted for lifestyle behaviors. AMEs are estimated using survey-weighted logistic regression models. All models additionally adjusted for survey year fixed effects.
AME = Average Marginal Effect; values indicate percentage-point change in the predicted probability of metabolic syndrome.
Bold values indicate statistical significance at P < .05.
Reference groups: No poverty, regular employment, no physical activity, no binge drinking, no smoking, and no family history.
N reflects complete-case observations for each model.
Overall model significance was assessed using survey-adjusted Wald tests: Model 1, F(16, 1773) = 65.04; Model 2, F(20, 1769) = 52.38; Model 3, F(26, 1763) = 40.88 (all P < .001).
After additionally adjusting for employment type in Model 2, the associations for dual poverty (AME = +4.86pp, P < .001), income-poverty-only (AME = +2.59pp, P < .001), and time-poverty-only (AME = +3.19pp, P = .038) remained statistically significant. Self-employment was associated with a higher predicted probability of MetS (AME = +3.70pp, P < .001), and irregular employment also showed a positive association (AME = +2.13pp, P = .014), whereas unpaid family work was not significant.
In the fully adjusted Model 3, incorporating behavioral risk factors, dual poverty (AME = +4.53pp, P = .001) and income-poverty-only (AME = +2.73pp, P < .001) remained significantly associated with higher MetS probability. The association for time-poverty-only was attenuated and became marginally significant (AME = +2.79pp, P = .065). Among employment types, self-employment (AME = +3.47pp, P < .001) and irregular employment (AME = +1.96pp, P = .026) remained positively associated with MetS. Among behavioral risk factors, current smoking was significantly associated with higher MetS probability (AME = +3.96pp, P = .010), whereas physical activity (AME = −1.33pp, P = .050) and monthly binge drinking (AME = +1.74pp, P = .057) showed borderline associations. Across all models, age and family history of chronic disease were consistently associated with increased MetS risk.
Taken together, the sex-stratified hierarchical models indicate that attenuation patterns differed between men and women. Among men, the association between time-poverty-only and MetS was attenuated after adjustment for employment and behavioral factors, whereas among women, dual poverty and income-poverty-only remained significantly associated with MetS even in the fully adjusted models.
Sensitivity analyses were conducted to examine the robustness of the findings to alternative specifications. Using alternative thresholds to define time poverty (40-h and 60-h cutoffs) yielded comparable directions of association, although the statistical significance of time-poverty effects varied by threshold (Supplemental Tables S1-S4). Among women, dual poverty and income-poverty-only remained consistently associated with higher MetS probability across alternative definitions, whereas time-poverty-only was not significant under the 40-h definition but showed positive associations under the 60-h definition. Among men, time-poverty-only was not statistically significant under either alternative threshold, and dual poverty was significant only in the age-adjusted model under the 60-h definition. In addition, perceived stress was included as an additional covariate to assess potential psychosocial confounding. Although higher perceived stress was independently associated with MetS, the associations of poverty type and employment remained largely unchanged (Supplemental Table S6).
Discussion
This study examined how multidimensional poverty—including income deprivation and time scarcity—is associated with metabolic syndrome (MetS) within a nationally representative Korean sample. Consistent with the conceptual framework of social determinants of health, poverty was operationalized as resource deprivation across income and time dimensions, while employment type was incorporated to capture the institutional context through which these resources are structured within the labor market.1,3 The findings indicate that the relationship between resource deprivation and metabolic syndrome varies by sex and across levels of structural and behavioral adjustment.
Among men, time poverty was associated with a higher predicted probability of MetS in partially adjusted models. This aligns with prior research linking long working hours to adverse cardiometabolic outcomes and constrained health-related behaviors.13,19,34 The attenuation of this association after behavioral adjustment suggests that temporal constraints may operate through socially patterned behaviors rather than exerting an independent physiological effect. This pattern is consistent with studies showing that socioeconomic gradients in metabolic syndrome are partially mediated by health behaviors.24,25
Among women, time poverty was also associated with MetS in partially adjusted models, but this association was attenuated after adjustment for behavioral factors. In contrast, income poverty and dual poverty remained significantly associated with MetS even in fully adjusted models. These findings correspond with evidence that material deprivation contributes to cardiometabolic risk in sex-specific ways.28,31,35 Income-related disadvantage remained statistically significant after adjustment for employment and health behaviors, indicating that its association with metabolic syndrome is not fully explained by employment classification or behavioral factors alone.14,15,36
Employment structure was also associated with metabolic risk, although patterns varied by sex. Self-employment remained positively associated with MetS after full adjustment, consistent with prior Korean studies reporting differences in cardiometabolic risk across employment types.14,15 The association for irregular employment differed between men and women. Supplementary analyses (Supplemental Table S5) indicated that the occupational distribution within irregular employment categories varied by sex, suggesting that observed differences may partly reflect labor market segmentation rather than employment status alone. These residual associations may therefore reflect broader occupational conditions, such as income instability or limited institutional protection. 37
A critical limitation concerns the operationalization of time poverty. In this study, time poverty was defined using paid weekly working hours and did not include unpaid domestic or caregiving labor. Time-use research demonstrates that unpaid labor disproportionately affects women’s total workload.8,38,39 Because unpaid labor was not incorporated into the present measure, the observed associations for women may not fully capture total temporal burden. Accordingly, estimates of time-related deprivation may be subject to measurement constraints that could influence the interpretation of sex-specific patterns. This limitation underscores the need for more comprehensive time-use indicators in future epidemiologic research.
The findings also highlight the importance of distinguishing between resource-based deprivation and behavioral correlates. Behavioral risk factors—including physical inactivity, smoking, and alcohol use—were significantly associated with metabolic syndrome, consistent with global evidence.20 -23,27 These behaviors are socially patterned and frequently clustered with socioeconomic disadvantage.26,40 The attenuation of time poverty after adjustment for behavioral factors suggests that part of its association with metabolic syndrome may be related to health-related behaviors. In contrast, income-related associations persisted after behavioral adjustment, indicating that multidimensional resource deprivation cannot be fully accounted for by behavioral factors alone. Taken together, these findings are consistent with a framework in which resource constraints and health behaviors are related but analytically separable dimensions of metabolic syndrome.
In addition to behavioral factors, psychosocial processes may also contribute to sex-differentiated patterns of metabolic health. Perceived stress was independently associated with metabolic syndrome; however, its inclusion in supplementary analyses (Supplemental Table S6) did not materially alter the observed associations between multidimensional poverty, employment type, and metabolic syndrome. This suggests that while psychosocial stress represents an important dimension of health inequality, the structural and resource-based associations identified in this study were not fully explained by perceived stress within the present analytic framework.18,41
Several limitations warrant consideration. First, the cross-sectional design precludes causal inference. Second, behavioral measures were self-reported and subject to potential misclassification. Third, detailed dietary modeling was not incorporated. Although diet is a recognized contributor to metabolic syndrome, available dietary data in the KNHANES are based on short-term recall and may not adequately reflect habitual intake patterns. 32 Fourth, time poverty was measured solely using paid work hours, potentially underestimating women’s total workload. Finally, occupational characteristics such as job control or preventive care access were not directly assessed.
Although this study is situated in the Korean context—characterized by long working hours and pronounced gender differences in unpaid labor participation—these structural configurations are not unique to Korea.13,42 Patterns of labor market flexibilization, employment precarity, and unequal time allocation are observed across many high-income economies.35,43 At the same time, institutional and welfare regime differences may influence the magnitude and expression of these associations, and direct extrapolation should be made cautiously.
Overall, the findings suggest that multidimensional poverty is associated with differences in metabolic syndrome across configurations of income constraints, time allocation, and employment context. Rather than functioning as a singular exposure, poverty appears situated within broader labor market structures, while remaining analytically distinct from employment classification.
Conclusion
In a nationally representative Korean sample, multidimensional poverty—encompassing income deprivation and time scarcity—was associated with metabolic syndrome in sex-differentiated patterns. Time poverty was more strongly attenuated after behavioral adjustment, whereas income-related deprivation demonstrated more persistent associations, particularly among women. Employment structure, especially self-employment, remained independently associated with metabolic syndrome.
These findings underscore the importance of considering income, time, and employment context together when examining metabolic health disparities. Policy efforts addressing excessive working hours and employment instability may contribute to reducing socially patterned metabolic risk. Longitudinal research incorporating comprehensive time-use and occupational measures is warranted to clarify causal pathways.
Supplemental Material
sj-docx-1-inq-10.1177_00469580261439103 – Supplemental material for Income and Time Poverty and Metabolic Syndrome in Korea: Sex-Specific Patterns After Hierarchical Adjustment
Supplemental material, sj-docx-1-inq-10.1177_00469580261439103 for Income and Time Poverty and Metabolic Syndrome in Korea: Sex-Specific Patterns After Hierarchical Adjustment by Ji In Lee, Kyung Hee Kim and Jae Wook Choi in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580261439103 – Supplemental material for Income and Time Poverty and Metabolic Syndrome in Korea: Sex-Specific Patterns After Hierarchical Adjustment
Supplemental material, sj-docx-2-inq-10.1177_00469580261439103 for Income and Time Poverty and Metabolic Syndrome in Korea: Sex-Specific Patterns After Hierarchical Adjustment by Ji In Lee, Kyung Hee Kim and Jae Wook Choi in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-3-inq-10.1177_00469580261439103 – Supplemental material for Income and Time Poverty and Metabolic Syndrome in Korea: Sex-Specific Patterns After Hierarchical Adjustment
Supplemental material, sj-docx-3-inq-10.1177_00469580261439103 for Income and Time Poverty and Metabolic Syndrome in Korea: Sex-Specific Patterns After Hierarchical Adjustment by Ji In Lee, Kyung Hee Kim and Jae Wook Choi in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-4-inq-10.1177_00469580261439103 – Supplemental material for Income and Time Poverty and Metabolic Syndrome in Korea: Sex-Specific Patterns After Hierarchical Adjustment
Supplemental material, sj-docx-4-inq-10.1177_00469580261439103 for Income and Time Poverty and Metabolic Syndrome in Korea: Sex-Specific Patterns After Hierarchical Adjustment by Ji In Lee, Kyung Hee Kim and Jae Wook Choi in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-5-inq-10.1177_00469580261439103 – Supplemental material for Income and Time Poverty and Metabolic Syndrome in Korea: Sex-Specific Patterns After Hierarchical Adjustment
Supplemental material, sj-docx-5-inq-10.1177_00469580261439103 for Income and Time Poverty and Metabolic Syndrome in Korea: Sex-Specific Patterns After Hierarchical Adjustment by Ji In Lee, Kyung Hee Kim and Jae Wook Choi in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-6-inq-10.1177_00469580261439103 – Supplemental material for Income and Time Poverty and Metabolic Syndrome in Korea: Sex-Specific Patterns After Hierarchical Adjustment
Supplemental material, sj-docx-6-inq-10.1177_00469580261439103 for Income and Time Poverty and Metabolic Syndrome in Korea: Sex-Specific Patterns After Hierarchical Adjustment by Ji In Lee, Kyung Hee Kim and Jae Wook Choi in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-7-inq-10.1177_00469580261439103 – Supplemental material for Income and Time Poverty and Metabolic Syndrome in Korea: Sex-Specific Patterns After Hierarchical Adjustment
Supplemental material, sj-docx-7-inq-10.1177_00469580261439103 for Income and Time Poverty and Metabolic Syndrome in Korea: Sex-Specific Patterns After Hierarchical Adjustment by Ji In Lee, Kyung Hee Kim and Jae Wook Choi in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
Ethical Considerations
This study was conducted using secondary anonymized data from KNHANES 2013 to 2024 and was exempt from ethical review by the Korea University Institutional Review Board (approval number: KUIRB-2025-0178-01).
Consent to Participate
Informed consent was not required due to the use of publicly available de-identified data. This study does not involve a clinical trial. Clinical trial registration: not applicable.
Author Contributions
The first authors (Ji In, Lee) designed the study, conducted analyses, and drafted the manuscript. The corresponding authors (Kyong Hee, Kim) provided critical feedback and guidance during the writing. All the authors read and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.