
Abstract
Physicians play a central role in medical innovation, bridging scientific discovery and clinical application. Underpinned by Social Cognitive Theory, this study examines the associations among organizational factors, psychological factors, and physician innovation performance, within the distinct setting of public hospitals. A cross-sectional survey was conducted among 1859 physicians from 22 tertiary municipal hospitals in Beijing. Multilevel structural equation modeling (MSEM) was employed to examine the relationships between organizational-level and individual-level variables. The hospital organizational innovation climate was positively associated with both physicians’ creative self-efficacy (β = .255, P < .001) and their innovation performance (β = .501, P < .001). Creative self-efficacy was positively associated with innovation performance (β = .646, P < .001) and partially mediated the climate-performance relationship (indirect effect = 0.217). These results highlight the importance of the hospital innovation climate—integrated with robust resource systems and scientific incentives—as it relates to physicians’ creative self-efficacy and their innovation performance in public healthcare institutions.
Keywords
Introduction
Science and Technology Innovation (STI) has become a critical driver of global health progress and a key pathway for achieving the United Nations’ Sustainable Development Goals (SDGs). 1 The COVID-19 pandemic period vividly demonstrated how STI’ s transformative role in healthcare, such as artificial intelligence (AI), big data analytics, and telemedicine, rapidly improved diagnostic efficiency, expanded access to quality medical resources in remote areas, and strengthened health system resilience.2,3 These developments underscore that STI is not only a response to crisis but also a catalyst for sustainable improvements in healthcare delivery, particularly in developing and emerging economies (DEEs). 4
China has strategically positioned the health sector STI as a national priority through the “Healthy China 2030” initiative, which established a comprehensive national medical innovation ecosystem framework. 5 Public hospitals, as pivotal nodes in this ecosystem, are increasingly performance-evaluated through innovation-related metrics. For instance, The Operational Manual for Performance Assessment of National Tertiary Public Hospitals (2024 Edition) mandated a progressive increase in both the “scientific research funding per 100 healthcare workers” and the “scientific research output conversion per 100 healthcare workers,” with these indicators quantitatively incorporated into the annual performance assessment criteria, with some designated as national monitoring indicators. These measures underscore that innovation performance has become not only a benchmark for Chinese hospital competitiveness but also a strategic priority in the governance of China’s public healthcare system. 6
Defined as the capacity of employees to adapt to dynamic environments by continuously updating knowledge and transforming innovative behaviors into tangible outcomes, innovation performance is closely associated with individual professional growth and organizational value creation. 7 Despite the recognized importance of healthcare innovation, empirical research has predominantly focused on nursing personnel innovation, with limited attention to physician innovation performance.8 -10 This phenomenon is noteworthy given that physician innovation encompasses distinct complexities. While nursing innovation typically addresses care process optimization and service delivery enhancement—such as developing patient care protocols, improving medication administration procedures—physician innovation operates at the intersection of scientific discovery and clinical implementation including pioneering minimally invasive surgical techniques, creating innovative treatment protocols, and translating basic science discoveries into clinical applications. As a core driving force behind the advancement of medical technology, the optimization of clinical workflows, and the ultimate improvement of population health outcomes, physician innovation directly shapes healthcare standards and constitutes a source of institutional competitive advantage.
Unlike enterprise employees whose innovation behaviors are primarily driven by profit maximization and market competition, physicians in public hospitals prioritize patient welfare over financial returns, creating fundamentally different innovation incentives. Physicians occupy a distinctive position within healthcare organizations, engaging in basic research, clinical application, and strategic decision-making. Their innovations—spanning novel surgical techniques, diagnostic protocols, and therapeutic interventions—directly influence care standards and constitute core technological competencies for healthcare institutions. 11 Nevertheless, studies examining physicians in public hospitals remain scarce, and the organizational factors associated with their innovation performance remain underexplored.
Existing research indicates that employee innovation performance is associated with multifaceted factors, which can be broadly categorized into individual- and organizational-level dimensions.12 -16 Multilevel studies have demonstrated significant positive correlations between individual innovation performance and organizational-level variables, including team boundary-crossing behaviors, leadership styles, and spiritual leadership.17 -19 These findings underscore the necessity of adopting multilevel analytical frameworks to elucidate the complex relationships underlying physician innovation performance. However, much of the current research in healthcare management primarily focuses on simplistic linear correlations between variables, which inadequately capture the complex interdependent relationships between individual characteristics and organizational contexts.20,21 This reductionist approach limits understanding of the multifaceted pathways associated with innovation performance, particularly in complex professional environments such as public hospitals. Consequently, a comprehensive theoretical framework integrating both internal psychological states and external environmental factors is imperative to elucidate these complex relationships.
Social cognitive theory (SCT) provides a robust theoretical framework for examining individual-environment interactions, positing that behaviors and outcomes emerge from dynamic relationships between cognitive processes and environmental factors. However, SCT applications to physician populations remain relatively scarce, despite physicians’ central role in healthcare innovation. Within this framework, creative self-efficacy has emerged as a key psychological construct associated with both organizational innovation climate and individual innovation performance. 22
Therefore, this study is grounded in Social Cognitive Theory, focuses on physicians, and examines how hospital innovation climate influences physicians’ innovation performance through the mediating role of creative self-efficacy.
Literature Review and Research Hypothesis
As a significant theoretical paradigm in modern psychology, SCT provides a comprehensive framework for examining the dynamic interplay between environmental conditions, cognitive factors, and behavioral outcomes. 22 According to SCT, human behavior is not interpreted as a sole product of internal traits or external forces; instead, it emerges from the reciprocal associations among personal cognition, environmental factors, and behavioral responses. Within this framework, organizational contexts are pivotal environmental factors associated with individual psychological states and performance outcomes.
This study examines organizational innovation climate as a key environmental factor. Organizational innovation climate represents employees’ shared perceptions of the extent to which their organization supports and encourages innovation activities. 23 As an organizational-level construct, it encompasses 3 defining characteristics: (1) it represents a collective cognitive phenomenon shared among organizational members; (2) it functions as an environmental variable interrelated with members’ psychological states and behavioral performance; and (3) it reflects members’ holistic perceptions of organizational systems rather than discrete events. 24
Empirical evidence demonstrates a positive relationship between organizational innovation climate and individual innovation performance. For example, Woodman et al identified organizational innovation climate as a key antecedent variable for explaining innovation performance, suggesting that is positively and significantly associated with innovation outcomes. 25 Similarly, Ramazan’s research demonstrated a significant positive correlation between the nursing work environment and nurses’ ultimate innovation output. 26 Moreover, a meta-analysis by Cui et al revealed a robust positive correlation between organizational innovation climate and innovation performance. 27 Accordingly, we propose Hypothesis 1:
Self-efficacy, a core construct of social cognitive theory, represents a critical factor of behavioral initiation and maintenance. 28 As social cognitive theory continues to evolve, scholars have contextualized self-efficacy, giving rise to creative self-efficacy—an individual’s subjective evaluation of their confidence and ability to complete innovative tasks during the innovation process.
The empirical studies have shown that employees’ creative self-efficacy is positively correlated with their innovation performance. 29 Stajkovic and Luthans, in their meta-analysis, reported a correlation coefficient as high as .38 between self-efficacy and performance, underscoring the strong link between these 2 variables. 30 Similarly, Dan et al demonstrated that nurses with elevated self-efficacy were more likely to implement innovative practices successfully. 31 Furthermore, Tierney et al found that the relationship between creative self-efficacy and innovation performance exceeded that of general self-efficacy. 32 These findings emphasize creative self-efficacy as a critical correlate of innovation outcomes.
SCT posits that creative self-efficacy, similar to general self-efficacy, is closely related to the interaction between personal and environmental factors.33,34 As environmental variable, the organizational innovation climate s closely associated with employees’ psychological processes and their corresponding innovative behaviors. Isaksen argued that an organizational climate supportive of innovation links to individual innovative performance via underlying psychological processes. 35
Furthermore, Mitchell and Gist’s theoretical model proposes that domain-specific self-efficacy is interrelated with analyzing task requirements, evaluating personal and environmental resources, and identifying limiting factors. 36 Importantly, the evaluation of personal and environmental resources and constraints aligns closely with the core concept of an organizational innovation climate. Specifically, a supportive organizational innovation climate is associated with heightened creative self-efficacy among employees, as it aligns with the availability of environmental resources and the mitigation of perceived constraints, which are consistent with higher innovation performance. Based on these theoretical foundations, we propose the following hypothesis:
In conclusion, this study proposes the following hypotheses (The flow chart is shown in Figure 1):

The conceptual framework of research hypotheses.
Methods
Study Design, Participants, and Procedures
Employing a cross-sectional design, this study focuses on practicing physicians from 22 hospitals in Beijing as research subjects. Beijing has the most abundant medical resources in the country, with a total of 138 tertiary hospitals. The 22 hospitals under the Beijing Municipality are all tertiary hospitals, comprising 16.94% of the city’s total. They provide over one-third of the city’s healthcare services and serve as representative institutions for delivering comprehensive care, advancing healthcare reforms, and driving innovations in the medical field.
The inclusion criteria for this study were as follows: (1) Participants were employed at municipal public hospitals in Beijing; (2) Participants were engaged in clinical medical practice; (3) Participants had been continuously employed at their current hospital for at least 1 year. Exclusion criteria were as follows: (1) Individuals with a tenure of less than 1 year at the current hospital; (2) Individuals who were on long-term leave, absent from their post, or on secondment during the survey period.
A stratified sampling method was employed to ensure the representativeness and balance of the sample. This approach accounted for the differences in functional positioning and resource allocation between key and non-key clinical departments and the potential variations in innovation willingness and behavior among physicians with different professional titles. Sampling within each hospital was stratified by key and non-key clinical departments, with 15% of practicing physicians selected from the 3 professional title levels: senior, intermediate, and junior. This method reduces sampling bias caused by uneven sample distribution, ensuring that the findings comprehensively capture the characteristics and disparities among professional groups. The Beijing Statistical Yearbook 2020 provided data on the number of licensed physicians in each municipal hospital.
Sample Size Calculation
The sample size was calculated using the formula for cross-sectional studies:
Data Collection and Quality Control
The questionnaire survey was conducted between October and November 2022. This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Capital Medical University (Approval No. Z2022SY090). All procedures adhered to relevant ethical guidelines and institutional regulations. Before beginning the formal questionnaire, all participants were required to answer an informed consent question: “Are you willing to participate in this questionnaire survey?.” Only participants who selected “Yes” could proceed to the questionnaire, indicating their voluntary participation.
We had established a minimum completion time of 70 s to ensure data reliability as an exclusion criterion during the data cleaning process. This threshold was determined based on the questionnaire’s length and the estimated time necessary for respondents to read, comprehend, and thoughtfully answer all items. Responses completed in less than 70 s were deemed likely to reflect inattentive reading or random/mechanical answering. Additionally, we excluded questionnaires exhibiting apparent logical inconsistencies to enhance data quality and ensure the robustness of subsequent analyses. A total of 2178 questionnaires were distributed, of which 1859 were deemed valid, resulting in a valid response rate of 85.35%.
Measurements
The questionnaire comprised 4 components: (a) demographic information, (b) physicians’ innovation performance scale, (c) hospital organizational innovation climate scale, and (d) physicians’ creative self-efficacy scale.
This study utilized a modified scale developed and validated by other scholars. To ensure contextual relevance, we adjusted the subject of the scale, replacing references to the “unit” with “hospital.” This approach of adapting the reference subject is a well-established and widely accepted practice in organizational behavior research.
Demographic Information of the Characteristics
The survey included 11 items covering demographic and professional characteristics, such as gender, age, educational background, years of work experience, professional title, administrative position, and department type.
Innovation Performance
This study adopted the Employee Innovation Performance Scale developed by Han et al which consists of 8 items. 7 A 7-point Likert scale was used, ranging from 1 (“strongly disagree”) to 7 (“strongly agree”), with higher scores reflecting a greater level of employees’ personal innovation performance. The scale exhibited high internal consistency reliability in its original validation, with a Cronbach’s alpha of .904.
Organizational Innovation Climate
This study adopted the Organizational Innovation Climate Scale developed by Zheng et al 38 The scale comprises 7 dimensions with a total of 24 items: 4 items for incentive mechanisms, 3 items for leadership by example, 3 items for teamwork, 4 items for support from superiors, 3 items for resource assurance, 3 items for organizational facilitation, and 4 items for autonomous work. A 5-point Likert scale was used, ranging from 1 (“strongly disagree”) to 5 (“strongly agree”). The original scale demonstrated good internal consistency reliability with a Cronbach’s alpha coefficient of .920.
Creative Self-Efficacy
This study employed the Employee Creative Self-efficacy Scale developed by Gu and Peng, which was localized to the specific context of China. 39 This adaptation aimed to ensure the scale’s accuracy and effectiveness in measuring the innovation self-efficacy of Chinese employees. The scale consists of 8 items rated on a 5-point Likert scale, ranging from 1 (“completely inconsistent”) to 5 (“completely consistent”), with high internal consistency (Cronbach’s α = .886). Higher scores indicate a greater level of employees’ innovation self-efficacy.
Aggregation Appropriateness Test
In this study, the hospital organizational innovation climate was analyzed as an organizational-level construct. This aggregation approach reflects the institutional reality that strategic orientations and essential innovation-related factors in tertiary hospitals—including performance-based incentive schemes, professional promotion pathways, and institutional resource allocation—are predominantly established and coordinated at the hospital level rather than by individual departments. Moreover, the hospital’s overarching organizational culture permeates the organization and is accessible to physicians regardless of their departmental affiliations. Although departmental climates exist, they operate within the broader parameters of the hospital’s integrated strategic objectives, ensuring a degree of structural alignment across the organization. Therefore, the study aggregates the organizational innovation climate at the hospital level.
To justify aggregating individual-level data to the organizational level, we examined both within-group consistency and between-group differences. For within-group consistency, the Rwg values for all secondary dimensions of the hospital’s organizational innovation climate ranged from 0.73 to 0.90, exceeding the threshold of 0.7. This result indicated a high level of consistency in employees’ perceptions of organizational innovation behavior within the same hospital. For between-group differences, the ICC (1) values for the hospital’s organizational innovation climate ranged from 0.14 to 0.28, surpassing the standard value of 0.12. Additionally, the ICC (2) values, representing intra-group variability, ranged from 0.75 to 0.88, exceeding the threshold of 0.7. These results support the appropriateness of aggregating individual-level perceptions to the hospital level.
Statistical Analysis
Given that the theoretical model of this study includes variables at both the individual and organizational levels and exhibits a clear nested data structure, we identified MSEM as the most suitable analytical approach. Additionally, considering the complex relationships between the latent variables under investigation, MSEM offers unique advantages. It effectively decomposes the variance of variables, distinguishing between-group and within-group variations, and independently models these variations by constructing structural and measurement models. Compared to traditional methods, MSEM presents several advantages. First, it simultaneously accounts for the complex interrelationships between individual- and organizational-level variables, reducing the risk of confounding effects caused by cross-level interactions. Second, by precisely controlling for variations at each level, MSEM significantly reduces bias in estimating mediating effects, thereby enhancing the model’s structural validity and the accuracy of the analytical results. 40 MSEM was employed to test the research hypotheses. Additionally, the Markov Chain Monte Carlo (MCMC) method was introduced to evaluate the mediating effects within the model SPSS 26.0, which was used to calculate the means and standard deviations of the variables. 41 At the same time, Mplus 8.3 was employed to perform the model testing.
Testing for Common Method Bias
This study collected data through self-reports from a single source—physicians in Beijing municipal hospitals—which may introduce common method bias (CMB). To control CMB and mitigate its potential impact on research results, we employed several procedural controls: utilizing anonymous questionnaire administration, incorporating reverse-scored items within the scales, and implementing Likert scales with diverse response levels. In addition, the study followed the recommendations of Podsakoff et al and Organ to assess CMB using Harman’s single-factor test. 42 If the variance explained by the largest factor is below 40% or 50%, and if more than 1 factor has an eigenvalue greater than 1, it indicates the absence of significant CMB. This study extracted 6 common factors with eigenvalues greater than 1, with the first factor explaining 38.479% of the variance, suggesting no severe CMB. This study further employed the unmeasured latent method factor approach. The baseline model (MODEL1) loaded all items onto their respective theoretical dimensions, while an alternative model (MODEL2) incorporated an additional common method factor. 43 The fit of MODEL2 was then compared with MODEL1 to determine whether the inclusion of the common method factor significantly improved the model fit (MODEL2-MODEL1). The comparison revealed △CFI = −0.121, △TLI = −0.132, △RMSEA = 0.076, and △SRMR = 0.346, indicating that the model fit worsened after adding the common method factor. Therefore, this study does not suffer from significant common method bias.
Results
Basic Characteristics of the Study Participants
Among the 1859 surveyed physicians, a substantial proportion were female (1089, 58.58%). The majority were aged 31 to 40 years (811, 43.63%) and predominantly married (1582, 85.10%). Nearly half of the respondents held a doctoral degree or higher (912, 49.06%). Regarding professional titles, the largest group comprised physicians with intermediate titles (611, 32.87%). Regarding employment status, the vast majority were regular, tenured employees (1741, 93.65%). The majority had 11 to 20 years of work experience (602, 32.38%). Most participants were in general staff positions (1585, 85.26%). Additionally, many respondents worked in non-clinical key departments (1086, 58.42%).
Descriptive Statistics and Correlation Analysis
Table 1 presents the main variables’ means, standard deviations, and correlation coefficients. As shown in Table 1, the hospital’s organizational innovation climate is positively correlated with physicians’ creative self-efficacy and innovation performance (P < .01). Additionally, physicians’ creative self-efficacy positively correlates with innovation performance (P < .01). Furthermore, gender, education, and professional title influence physicians’ creative self-efficacy; age influences innovation performance. Therefore, these demographic variables were included as control variables in the data analysis to mitigate the impact of spurious effects on the research results.
Results of Descriptive Statistics and Correlations.

OIC = organizational innovation climate; CSE = creative self-efficacy; IP = innovation performance; SD = standard deviation.
**P < .01. *P < .05.
Reliability and Validity Testing
All scales utilized in this study demonstrated high internal consistency, with Cronbach’s alpha coefficients exceeding .8 for all variables. Specifically, Cronbach’s alpha coefficient was .974 for the physicians’ innovation performance scale, .968 for the hospital organizational innovation climate scale, and .965 for the physicians’ creative self-efficacy scale.
Convergent validity reflects the degree to which different items of the same construct converge on a common latent variable. It is typically assessed using the Average Variance Extracted (AVE) value, Composite Reliability (CR) value, factor loadings, and their statistical significance. In this study, the AVE values exceeded 0.5, and the square roots of these values were greater than the correlation coefficients among variables. The CR values were all above 0.9, and the factor loadings of all items were greater than 0.7 with corresponding P values below .001. These results indicate robust convergent validity in this study.
A series of nested confirmatory factor analyses (CFA) were conducted to assess the discriminant validity of the constructs. The results presented in Table 2 indicate that the 3-factor model exhibited the best model fit. This finding indicated satisfactory discriminant validity across all constructs and further suggested that common method bias was not a serious concern in this study.
Results of Confirmatory Factor Analyses.

OIC = organizational innovation climate; CSE = creative self-efficacy; IP = innovation performance; CFI = comparative fit index; TLI = Tucker-Lewis index; SRMR = standardized root mean square residual.
OIC = CSE + IP.
CSE = IP + CSE.
IP = CSE + OIC.
P < .001.
Hypothesis Testing Results
The MSEM and Monte Carlo confidence interval estimation methods were employed to test the hypotheses proposed in this study (As shown in Tables 3 and 4). Model 2 of Table 3 shows that the hospital’s organizational innovation climate is positively associated with physicians’ innovation performance (β = .501, P < .001), supporting H1. Model 1 demonstrates a significant positive association between the hospital’s organizational innovation climate and physicians’ creative self-efficacy (β = .255, P < .001), confirming H2. Furthermore, Model 3 reveals that physicians’ creative self-efficacy is positively associated with innovation performance (β = .664, P < .001), supporting H3. In Model 4, physicians’ creative self-efficacy remains a significant correlate of innovation performance (β = .646, P < .001). Additionally, the coefficient representing the association between the hospital’s organizational innovation climate and physicians’ innovation performance was decreased from β = .501 (P < .001) to β = .286 (P < .001) after including physicians’ creative self-efficacy in the model. This reduction suggests that creative self-efficacy serves as a partial mediator of this relationship.
Results of MSEM Analysis.
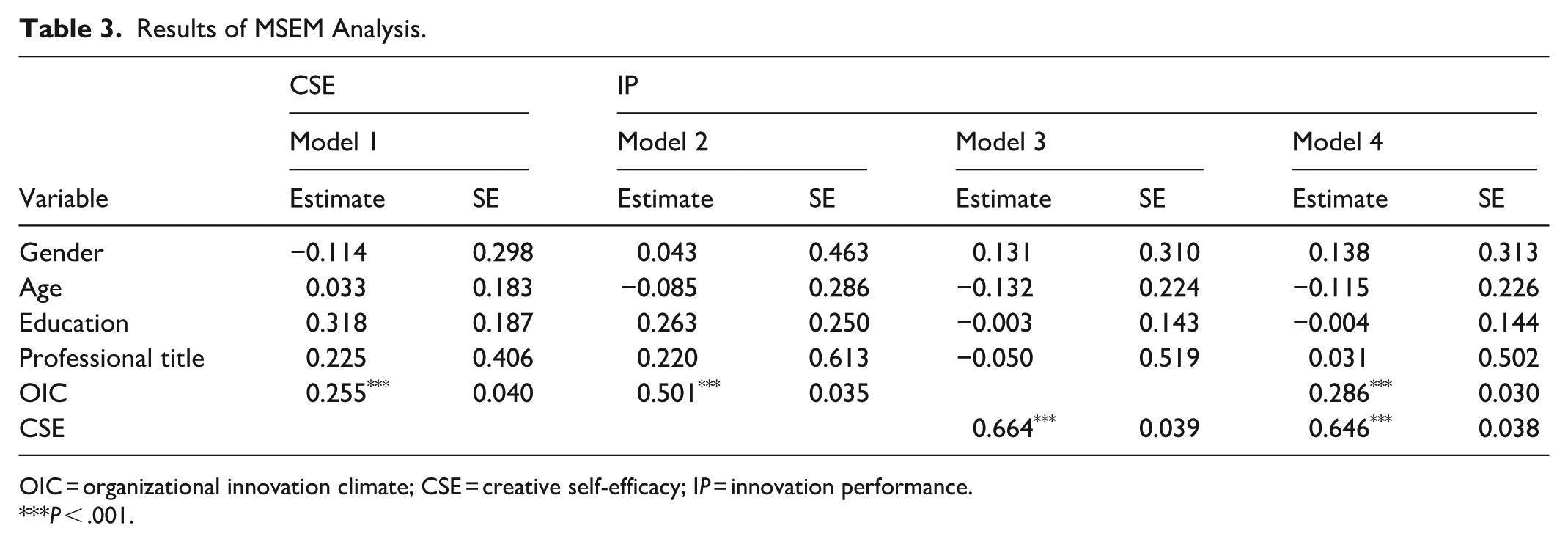
OIC = organizational innovation climate; CSE = creative self-efficacy; IP = innovation performance.
P < .001.
Results of Mediating Effect Test.
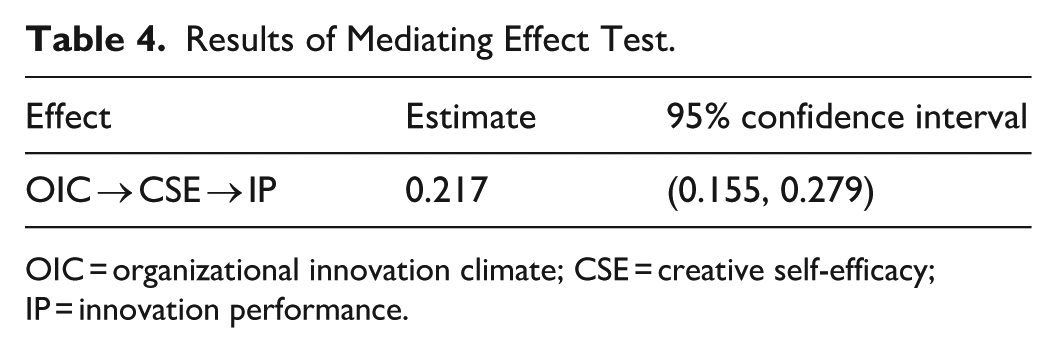
OIC = organizational innovation climate; CSE = creative self-efficacy; IP = innovation performance.
Moreover, as presented in Table 4, the estimated indirect effect is 0.217, with a 95% confidence interval of (0.155, 0.279), which does not include 0. This further corroborates H4, suggesting that the mediating role of creative self-efficacy is statistically significant.
Robustness Test
In general, key departments are allocated more resources than non-key, which may influence their innovation performance. This study classified the entire sample into 2 groups based on department type to ensure the robustness of the results: key departments and non-key departments. Separate analyses were then conducted for each group (As shown in Table 5). The results indicate that the estimated coefficients’ signs and significance for the research hypotheses are consistent across the 2 groups and the entire sample, demonstrating strong robustness.
Results of the Robustness Test.

OIC = organizational innovation climate; CSE = creative self-efficacy; IP = innovation performance.
P < .001. *P < .05.
Discussion
This study employed an MSEM to investigate the relationships among organizational innovation climate, physicians’ creative self-efficacy, and innovation performance in public hospitals. The results align with our theoretical framework, confirming that organizational innovation climate in public hospitals, as a key organizational-level factor, is significantly and positively associated with both physicians’ creative self-efficacy and innovation performance at the individual doctor level. Additionally, creative self-efficacy serves as a partial mediator of this relationship. These findings provide valuable theoretical insights into the mechanisms underlying physician innovation and offer empirical evidence for developing effective innovation management strategies in public hospitals.
The findings indicate that the organizational innovation climate in public hospitals is positively associated with physicians’ creative self-efficacy and innovation performance, aligning with results reported in the existing literature and underscoring the strategic role of the organizational environment in facilitating innovative practices.44 -46 This findings hold significant implications for “Healthy China 2030” initiative, which prioritizes scientific and technological innovation in healthcare as a national strategic objective. By fostering robust innovation climates, public hospitals can fulfill their roles as drivers of medical advancement and contribute to building an innovation-driven healthcare system at the national level. As highly institutionalized entities, public hospitals develop organizational climates that are extensively associated with clinicians’ motivation and behavioral patterns. Healthcare administrators can integrate incentive policies with cultural guidance and cultivate an innovation-friendly organizational atmosphere. 15 Specifically, hospitals’ organizational culture should emphasize openness, inclusiveness, and psychological safety for innovation failure, fostering conditions that support professional innovation.47,48 Moreover, hospitals can integrate innovation-oriented indicators into performance evaluation, scientific research, and quality improvement frameworks, ensuring that innovation becomes a visible and rewarded component of daily medical practice.
Additionally, this study revealed that physicians’ creative self-efficacy partially mediates the relationship between a hospital’s organizational innovation climate and physicians’ innovation performance. This mediation role may relate to elements within the hospital’s innovation climate, such as resource availability, superior support, and organizational facilitation, which create favorable conditions for physicians’ innovative practices. 49 Moreover, physicians with higher levels of creative self-efficacy are more likely to proactively explore novel approaches, tackle complex challenges, and engage in interdisciplinary collaboration, ultimately generating higher-value innovative outcomes in their professional practice.50,51 These findings carry important practical implications for hospital administrators. While transforming an organization’s macro-level innovation climate requires substantial resources and extended timeframes, targeted interventions designed to enhance creative self-efficacy represent a more agile and cost-effective strategy. Hospitals are advised to implement a diversified innovation incentive system that combines material and non-material rewards to boost medical staff’s creative self-efficacy effectively.52,53 Supporting infrastructure should include targeted innovation training, adequate resource allocation, cross-departmental collaboration mechanisms, and knowledge-sharing platforms to strengthen the foundation for innovation.54,55 In the era of “Internet+,” hospitals can amplify physicians’ innovation efforts by harnessing big data technologies, including big data analytics, specialized online training, and AI-enabled collaboration platforms, providing specialized training opportunities, and utilizing artificial intelligence to establish online collaboration platforms.
Theoretical Contributions
Our study makes 3 main contributions to the prior literature. First, it focuses on physicians within China’s distinct healthcare context—a population often overlooked in medical innovation research. While social cognitive theory and organizational climate models have been extensively validated in business and nursing contexts, their applicability to physicians—who uniquely combine clinical decision-making with research responsibilities—remains empirically unexamined. By empirically examining, our study enriches the theoretical understanding of physicians’ innovation performance from a social cognitive perspective.
Second, by examining their relevance within China’s distinctive healthcare context, refines the explanatory scope of social cognitive theory and related frameworks, including self-efficacy theory and the stimulus–organism–response (S–O–R) model. 56 Although these theories posit broadly applicable cognition–behavior mechanisms, China’s healthcare system—shaped by state-led innovation policies and hierarchical administrative structures—presents institutional systems that diverge markedly from those observed in Western settings. Our findings demonstrate that creative self-efficacy is a key psychological pathway linking organizational climate and innovation performance. 57 By contextualizing this pathway within China’s post-pandemic healthcare reforms, our work illustrated that these classical theories are generalizable and contextually adaptive and enrich cross-level behavioral research in healthcare organizations.
Third, while most prior research has relied on cross-sectional descriptive analyses or basic Ordinary Least Squares (OLS) regression, our study employs Multilevel Structural Equation Modeling (MSEM). This represents a methodological advancement, as MSEM is specifically designed to handle nested data structures inherent in hierarchical organizational settings. By partitioning variance across individual and organizational levels, MSEM provides unbiased cross-level parameter estimates. This approach helps elucidate the underlying relationships in our study.
Limitations
This study has several limitations. First, this study employed cross-sectional data. Although our model is theoretically grounded in Social Cognitive Theory, the observed associations do not confirm causal relationships. Future research should employ longitudinal or time-lagged designs to examine causal relationships between organizational climate and physician innovation. Furthermore, while statistical indices justified the aggregation of data to the hospital level, this approach may not fully capture the potential heterogeneity across clinical departments. Individual perceptions might be influenced by specific environments within different clinical departments that were not differentiated in the current study. Subsequent research could explore the contributions of departmental-level climates to provide a better understanding of the relationships underlying physician innovation performance.
Third, this study is subject to potential endogeneity and omitted variable bias. While we controlled for several key covariates, unobserved confounders at both the individual level (eg, innate ability, research motivation) and the institutional level (eg, research resources, university affiliation) may bias the estimated associations. These omitted variables could be simultaneously associated with both organizational innovation climate and physician innovation performance, potentially confounding the observed relationships. Although controlling for all potential confounders is impossible in observational research, we acknowledge this limitation. Future research should employ longitudinal or quasi-experimental designs to better identify causal mechanisms and mitigate concerns regarding unobserved heterogeneity. Fourth, our study relying on self-reported data from a single source may introduce CMB. Although procedural controls and statistical tests were performed, they cannot fully eliminate the risk of CMB. Future research should incorporate multi-source ratings or objective metrics to validate these findings more rigorously. Finally, this study employed a general employee scale rather than a physician-specific instrument, which may limit its ability to fully capture the unique characteristics and contextual nuances of physicians’ innovation performance. Future research should develop or adopt healthcare-specific measures to more accurately assess innovation within medical settings.
Conclusion
This cross-sectional study of 1859 physicians in Beijing tertiary hospitals used multilevel structural equation modeling to examine relationships between organizational innovation climate, creative self-efficacy, and innovation performance. Organizational innovation climate was significantly and positively associated with both physicians’ creative self-efficacy and innovation performance. Creative self-efficacy was positively associated with innovation performance and served as a significant indirect link between organizational climate and performance outcomes. These findings demonstrate the pathways through which organizational factors are associated with physician innovation, emphasizing the pivotal role of self-efficacy beliefs. Hospital administrators may strengthen innovation climate through targeted interventions: securing innovation resources, developing incentive structures, and establishing collaborative platforms. Such initiatives may enhance physicians’ creative self-efficacy and improve medical service quality.
Supplemental Material
sj-pdf-1-inq-10.1177_00469580261433833 – Supplemental material for Relationships Between Organizational Innovation Climate, Creative Self-Efficacy, and Innovation Performance: A Cross-Sectional Study in Public Hospitals
Supplemental material, sj-pdf-1-inq-10.1177_00469580261433833 for Relationships Between Organizational Innovation Climate, Creative Self-Efficacy, and Innovation Performance: A Cross-Sectional Study in Public Hospitals by Ruizhe Wu, Xingmiao Feng, Ziyan Zhai, Xinyue Sun, Zhen Wang, Zhaoyang Wang and Kai Meng in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-2-inq-10.1177_00469580261433833 – Supplemental material for Relationships Between Organizational Innovation Climate, Creative Self-Efficacy, and Innovation Performance: A Cross-Sectional Study in Public Hospitals
Supplemental material, sj-pdf-2-inq-10.1177_00469580261433833 for Relationships Between Organizational Innovation Climate, Creative Self-Efficacy, and Innovation Performance: A Cross-Sectional Study in Public Hospitals by Ruizhe Wu, Xingmiao Feng, Ziyan Zhai, Xinyue Sun, Zhen Wang, Zhaoyang Wang and Kai Meng in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors thank all participants in this study, the doctors who contributed to the investigation, and the 22 municipal hospitals in Beijing for their collaborative support.
Ethical Considerations
This study was conducted in accordance with the principles of the Declaration of Helsinki. This study is based on a research study approved by the ethics committee of Capital Medical University (No. Z2022SY090) on October 14, 2022.
Consent to Participate
All the participants signed written informed consent forms prior to participating in the study.
Consent for Publications
All authors are aware of and agree to the publication.
Author Contributions
RW contributed to the data curation, software, formal analysis, and writing of the original draft. XF contributed to the questionnaire design and investigation. ZZ contributed to software analysis and writing-review, and editing. XS, ZW, and Z-yW contributed to supervise the project. KM contributed to conceptualization, methodology, writing-review, editing, supervision, project administration, and funding acquisition. All authors contributed substantially to the article revisions.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by National Natural Science Foundation of China (grant number 72074160). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration of AI Use
This study did not use any Artificial Intelligence (AI) tools in the generation, analysis, or interpretation of data, nor in the creation of figures, tables, or other scientific content. All aspects of the study were conducted by the authors, who take full responsibility for the accuracy, originality, and integrity of the submitted work.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.* E-mail:
Supplemental Material
Supplemental material for this article is available online.