
Abstract
Introduction: This study aimed to investigate the factors influencing infection control performance among healthcare workers in long-term care facilities using self-administered questionnaires. Methods: This cross-sectional study included a total of 180 healthcare workers selected from 2 representative medium-to-large long-term care facilities in the Gwangju and Jeonnam regions of the Republic of Korea. Individuals with less than 3 months of work experience were excluded. Results: Statistical analyses showed significant differences in organizational culture for infection control based on educational level (F = 7.414, P < .001), and in the infection prevention environment based on both occupation (F = 3.217, P = .042) and educational level (F = 2.739, P = .045). Multiple regression analysis revealed that perception of standard infection control guidelines (β = .223, P = .001) and organizational culture (β = .479, P < .001) were significant predictors of infection control performance. Conclusion: These findings suggest that strengthening institutional infection prevention systems and fostering a culture of infection safety can improve occupational health outcomes and reduce the risk of healthcare-associated infections in long-term care settings.
Keywords
What is already known about this topic?
Long-term care facilities have high risk of healthcare-associated infections, yet most of the evidence on the determinants of infection control is drawn from acute-care settings, thereby leaving limited understanding of long-term care contexts.
This study provides setting-specific evidence by joint ly examining organizational, environmental, and perceptual factors and identifying key predictors of infection control performance among healthcare workers.
Our findings support multilevel infection control frameworks and underscore the need to strengthen safety culture, environmental support, and standardized training and protocols in long-term care facilities.
Background
The United Nations anticipates that Korea will experience one of the most significant increases in its older population. 1 Long-term care facilities (LTCFs), such as nursing homes (NHs), primarily serve older individuals and patients with chronic illnesses who typically reside in shared living environments for extended periods. These patients often have weakened immune systems, making them highly susceptible to infections. Outbreaks in these settings pose significant risks owing to the potential for rapid transmission.2,3
The COVID-19 pandemic underscored how failures in infection control within LTCFs can contribute to broader transmission of community infection. This has highlighted the need for a systematic analysis of the factors influencing infection control capacities. 4 In response, the Korea Disease Control and Prevention Agency (KDCA), through the Second National Infection Prevention and Control Comprehensive Plan (2023-2027), has expanded its focus to include caregivers and nursing assistants, and environmental service workers. 5 The plan aims to foster a safer healthcare environment by broadening the scope of infection control initiatives. 5
Unlike acute care hospitals, LTCFs predominantly rely on caregivers and nursing assistants, rather than physicians or registered nurses. Because of their frequent and close interactions with patients, these healthcare workers are exposed to increased risks of pathogen exposure and may inadvertently contribute to the spread of infections.6,7 Given their central role in providing daily care, enhancing their understanding of and adherence to infection control practices has become a critical focus for improving patient safety. 8
Recent evidence indicates healthcare-associated infections (HAIs) to be a significant concern in LTCFs. A systematic review and meta-analysis of 123 point-prevalence studies involving 709 860 residents across 33 countries reported an overall HAI prevalence of 3.5% (95% confidence interval [CI] 3.1%-4.0%). 9 Longitudinal surveillance studies in European LTCFs also showed an incidence of approximately 1.8 HAIs per 1000 resident-days, with a substantial proportion resulting in hospitalization or death. 10 These findings highlight HAIs to be prevalent and serious threats in LTCFs, thus underscoring the importance of understanding the factors that influence healthcare workers’ infection control performance in these settings.
The Standard Precautions Guidelines issued by the U.S. Centers for Disease Control and Prevention (CDC) serve as a foundational framework for preventing HAIs and are intended for all healthcare workers, including nurses. 11 Effective infection control in LTCFs depends on strict adherence to such guidelines, and healthcare workers’ compliance directly affects the level of infection prevention in a facility. 12 Therefore, consistent observation of standard precautions by all staff, including caregivers and nursing assistants, is essential for maintaining a safe healthcare environment.
Recent studies on infection control performance in LTCFs have identified several influencing factors, including demographic characteristics such as age, sex, educational attainment, and job position of the healthcare workers. 13 Furthermore, their personal attributes such as prior infection-related education and infection control awareness, 8 as well as organizational factors such as hospital culture,12,14 significantly affect infection control performance. Notably, improving adherence to Infection Prevention and Control (IPC) guidelines requires more than education. Physical and environmental conditions within the facility also significantly influence infection management behaviors.12,13 The infection prevention environment encompasses not only the physical infrastructure and equipment needed to protect healthcare workers but also the administrative support structures, all of which are fundamental to quality patient care.12,15
Organizational culture—consisting of shared norms, behaviors, and expectations—also plays a pivotal role in infection control performance. 16 Infection control culture refers to the shared values, beliefs, behaviors, and expectations among workers regarding adherence to infection management guidelines to ensure patient safety.16 -18 Thus, an organizational culture that supports infection control through environmental safety, administrative support, and sufficient resource allocation serves as a crucial external factor for enhancing infection control performance. However, most previous studies have focused on general hospitals and medical staff, such as doctors and nurses. Notably, research on how the infection prevention environment and organizational culture impact caregivers and nursing assistants in long-term care settings is limited.
This study aimed to examine how perceptions of standard infection control practices, the infection prevention environment, and organizational culture influence infection control performance among healthcare workers in long-term care facilities.
Materials and Methods
Study Design
A cross-sectional observational study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE; Supplemental Material) guidelines 19 to examine factors associated with infection control performance among healthcare workers in LTCFs.
Participants
This study included 180 healthcare workers employed at 2 LTCFs located in the Gwangju and Jeonnam regions of the Republic of Korea. The 2 hospitals were chosen owing to their status as medium-to-large LTCFs that exemplify the typical organizational characteristics of their regions and employ a diverse range of healthcare professionals. Participants were randomly selected; individuals with less than 3 months of work experience were excluded because they typically lack sufficient knowledge of infection control guidelines and have limited familiarity with organizational culture, which may hinder their ability to effectively implement infection control measures. 20 Only individuals who understood the purpose of the study and provided informed consent were included. Data was collected using self-reported questionnaires from March 14 to April 13, 2025.
Sample Size
The required sample size was calculated using the G*Power software (version 3.1.7, Heinrich-Heine-University, Germany). Infection control performance was used as the dependent variable for multiple regression analysis. Based on an effect size of .15, a significance level (⍺) of .05, statistical power (1−β) of .95, and 10 predictors (7 demographic characteristics, perception of standard infection control guidelines, infection prevention environment, and organizational culture for infection control), the minimum required sample size was found to be 172. To account for potential dropouts, questionnaires were distributed to 185 healthcare workers. A total of 180 completed questionnaires were included in the final analysis, reflecting a dropout rate of 2.70%.
Measurements
Perception of Standard Infection Control Guidelines
The perception of standard infection control guidelines was assessed using a tool originally developed based on the CDC’s standard precautions and later revised by Hong et al. 21 This tool consists of 31 items divided into 7 subdomains. The subdomains comprised 10 items on hand hygiene, 9 on personal protective equipment, 3 on respiratory etiquette, 2 on therapeutic equipment and supplies, 2 on environmental management, 2 on linen, and 3 on employee safety. Each item was rated on a 5-point Likert scale ranging from 1 (not important at all) to 5 (very important), with higher scores indicating greater perception of standard infection control guidelines. The tool demonstrated a Cronbach’s α of .95 in the study by Hong et al 21 and .88 in the present study.
Infection Prevention Environment
The infection prevention environment was measured using an instrument originally developed by Han and revised by Ahn et al.14,22 This tool consists of 11 items, each rated on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree), with higher scores indicating a more favorable environment for infection prevention. The reliability of the instrument was Cronbach’s α = .89 in the original study by Han 22 and .87 in the present study.
Organizational Culture for Infection Control
The organizational culture for infection control was assessed using a modified version of the patient safety culture tool developed by the Agency for Healthcare Research and Quality and adapted by Moon.23,24 The tool consists of 10 items rated on a 7-point Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree), with higher scores reflecting a more positive organizational culture regarding infection control performance. The tool demonstrated a Cronbach’s α of .85 in Moon’s 2015 study 23 and .89 in the present study.
Infection Control Performance
Infection control performance was measured using a tool originally developed by Askarian et al 25 and revised by Ko and Park 26 for application among caregivers in small- and medium-sized hospitals. The instrument contains 15 items distributed across 4 subdomains: 5 on hand hygiene, 4 on personal protective equipment, 2 on linen and the environment, and 4 on respiratory etiquette. Each item is rated on a 4-point Likert scale ranging from 1 (never performed) to 4 (always performed), with higher scores indicating better infection control performance. The tool demonstrated a Cronbach’s α of .81 in the study by Ko and Park 26 and .84 in the present study.
Ethical Considerations
This study was conducted after approval from the Institutional Review Board (No. 1040191-202502-HR-002-01). All participants received detailed information about the study’s objectives and procedures prior to participation. Participation was entirely voluntary, and confidentiality and anonymity were assured. Data collected through self-administered questionnaires were anonymized, coded, and securely stored in a database without any personally identifiable information. Participants were compensated for their participation.
Data Analysis
Data analysis was performed using IBM SPSS Statistics for Windows, Version 26. Descriptive statistics and frequency analysis were used to analyze general participant characteristics. Differences in variable scores based on general characteristics were assessed using the t-test. Pearson’s correlation coefficients were used to examine relationships between variables. Multiple linear regression analysis was performed to identify factors affecting infection control performance among healthcare workers in LTCFs. P < .05 was considered to be statistically significant.
Results
Differences in Variables by Demographic Characteristics
The average age of the participants was 46.31 ± 14.58 years; 139 were females (77.2%), and 41 were males (22.8%). Regarding education level, 72 participants (40.0%) had a high school education or less, 58 (32.2%) held a diploma degree, 44 (24.4%) had a bachelor’s degree, and 6 (3.3%) had a master’s degree or higher. In terms of occupation, 60 participants (33.3%) were physicians or nurses, 85 (47.2%) were caregivers or nursing assistants, and 35 (19.4%) were allied health professionals (eg, clinical laboratory technologists, radiologists, physical therapists). Concerning work experience, 32 participants (17.8%) had less than 1 year, 46 (25.6%) had 1 to 5 years, 40 (22.2%) had 5 to 10 years, and 62 (34.4%) had more than 10 years of work experience. A total of 175 participants (97.2%) had completed infection control training, while 5 (2.8%) had not. Additionally, 125 participants (69.4%) reported experience with healthcare accreditation, whereas 55 (30.6%) had no such experience (Table 1).
Differences in Measured Variables by Demographic Characteristics (N = 180).

Note. M = mean; SD = standard deviation; AN = nursing assistants.
Analysis of the measured variables based on demographic characteristics revealed no significant differences in scores based on sex, work experience, or accreditation experience. However, organizational culture for infection control differed significantly by education level (F = 7.414, P < .001). The infection prevention environment showed statistically significant differences based on both occupation (F = 3.217, P = .042) and education level (F = 2.739, P = .045; Table 1).
Levels of Perception of Standard Infection Control Guidelines, Infection Prevention Environment, Organizational Culture for Infection Control, and Infection Control Performance
Participants’ perception of standard infection control guidelines was high, with a mean score of 4.77 ± 0.26 on a 5-point Likert scale. The average scores by subdomain were hand hygiene 4.71 ± 0.34, personal protective equipment 4.77 ± 0.31, respiratory etiquette 4.86 ± 0.29, therapeutic equipment and supplies 4.83 ± 0.33, environmental management 4.80 ± 0.43, linen 4.81 ± 0.35, and employee safety 4.83 ± 0.37. Higher scores indicate a stronger understanding of the importance and necessity of standard infection control guidelines, as well as a more positive attitude toward adhering to them. The infection prevention environment was perceived positively, with a mean score of 4.22 ± 0.45 on a 5-point Likert scale, where higher scores reflect an environment that supports infection prevention, including adequate facilities, equipment, and organizational support. Organizational culture regarding infection control was also perceived positively, with a mean score of 5.73 ± 0.84 on a 7-point Likert scale, where higher scores indicate a culture that encourages and supports infection control practices through leadership, peer support, and institutional norms. Infection control performance was rated highly, with a mean score of 3.74 ± 0.35 on a 4-point Likert scale. The average scores by subdomain were 3.68 ± 0.44 for hand hygiene, 3.74 ± 0.44 for personal protective equipment, 3.73±0.48 for linen and environment, and 3.83 ± 0.34 for respiratory etiquette. Higher scores reflect the extent to which participants consistently implement infection control practices in their daily work (Table 2).
Descriptive Statistics of Measured Variables (N = 180).
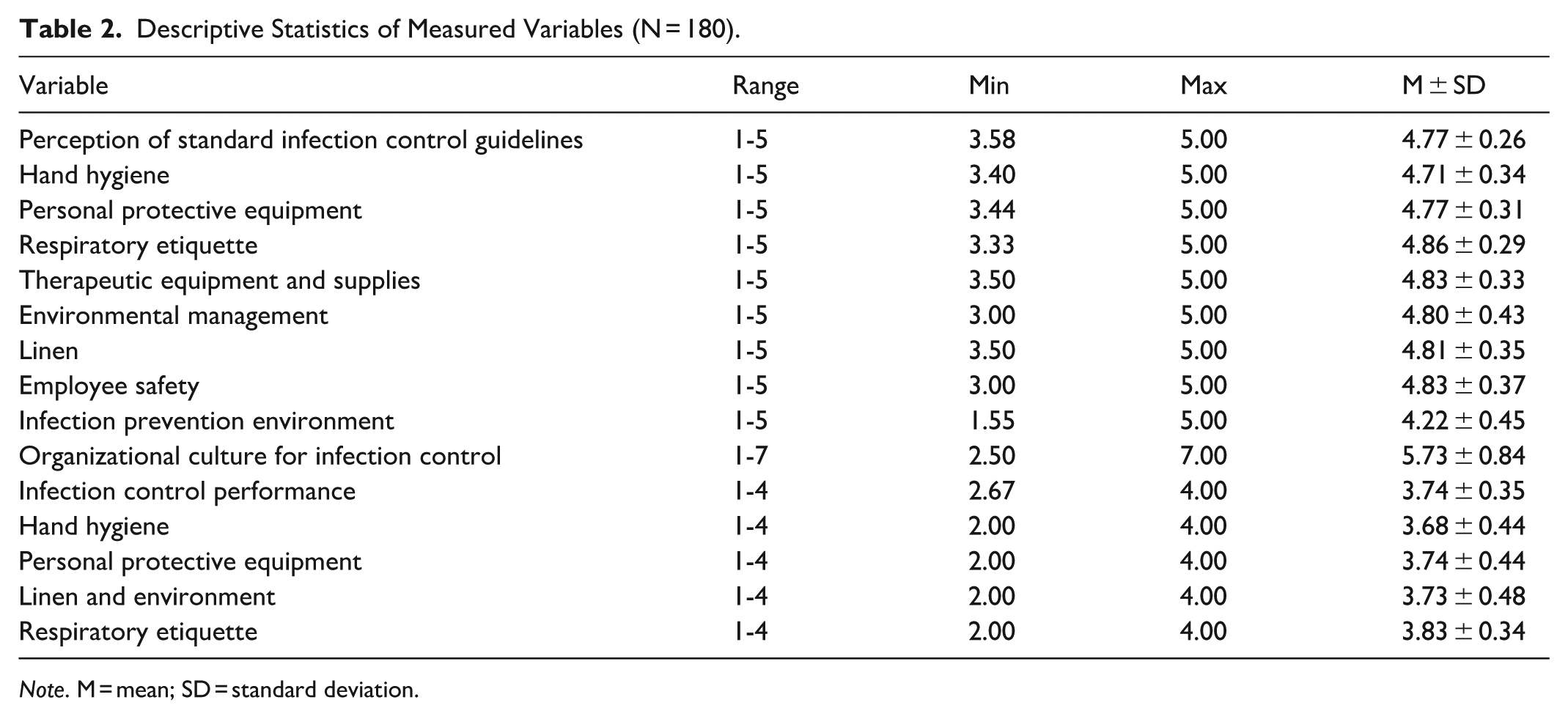
Note. M = mean; SD = standard deviation.
Correlations Between Perception of Standard Infection Control Guidelines, Infection Prevention Environment, Organizational Culture for Infection Control, and Infection Control Performance
The correlations among perception of standard infection control guidelines, infection prevention environment, organizational culture for infection control, and infection control performance are presented in Table 3. Statistically significant positive correlations were found among all measured variables. Perception of standard infection control guidelines was positively correlated with the infection prevention environment (r = .379, P < .001), organizational culture for infection control (r = .448, P < .001), and infection control performance (r = .444, P < .001). The infection prevention environment was significantly correlated with both organizational culture for infection control (r = .665, P < .001) and infection control performance (r = .426, P < .001). Organizational culture for infection control showed a strong positive correlation with infection control performance (r = .599, P < .001).
Correlations Among Measured Variables (N = 180).

Factors Influencing Infection Control Performance
Regression analysis was conducted to examine the effects of education level, occupation, perception of standard infection control guidelines, infection prevention environment, and organizational culture for infection control—variables that showed significant differences in the Analysis of Variance and correlation analysis—on infection control performance. The regression model was statistically significant (F = 19.861, P < 0.001), with an explanatory power of 38.7%. No issues with multicollinearity were observed, as variance inflation factor (VIF) values ranged from 1.156 to 1.958. Additionally, the Durbin–Watson statistic was 1.870, indicating no auto-correlation in the residuals. The results showed that both perception of standard infection control guidelines (β = .223, P = 0.001) and organizational culture for infection control (β = .479, P < .001) significantly influenced infection control performance among healthcare workers in LTCFs. The model had an R2 of .408 and an adjusted R2 of .387 (Table 4).
Factors associated with Infection Control Performance (N = 180).

Note. SE = standard error.
Discussion
This study examined the influence of healthcare workers’ perceptions of standard infection control guidelines, the infection prevention environment, and organizational culture for infection control on infection control performance in LTCFs. Our findings revealed several significant insights with meaningful implications for infection control strategies in these settings.
Among the general characteristics, education level was significantly associated with organizational culture for infection control, while both occupation and education level were significantly associated with perceptions of the infection prevention environment. These results are consistent with findings from a study conducted in India. 13 Occupation and education level influence perceptions of the infection control environment, as different roles, such as nurses, physicians, and allied health professionals, interact with or shape this environment in varied ways. For instance, nurses and other medical staff are more likely to engage directly with infection control practices, which may lead to a stronger perception of the infection prevention environment. Similarly, individuals with higher educational attainment tend to evaluate their surroundings more systematically and critically. This population group is also more likely to possess relevant knowledge, understand the importance of infection control and adhere to professional ethical standards. Consequently, individuals with more advanced education may recognize the significance of organizational culture for infection control and exhibit greater compliance with related policies and procedures. These findings suggest that both professional roles and educational backgrounds influence healthcare workers’ perceptions and integration of infection control policies into daily practice.
Correlation analysis demonstrated significant positive relationships among all key variables. Specifically, perception of standard infection control guidelines was significantly associated with the infection prevention environment, organizational culture for infection control, and overall infection control performance. The infection prevention environment was also positively correlated with both organizational culture and infection control performance. The strongest correlation was observed between organizational culture and infection control performance. These findings support prior research emphasizing the interrelated nature of organizational and behavioral factors in achieving effective infection control.16,27 These findings also reinforce the idea that infection control should not be regarded as an isolated practice, but rather as an integral aspect of an organization’s ethos, attitudes, and behaviors. 28
Multiple regression analysis identified 2 significant predictors of infection control performance: perception of standard infection control guidelines and organizational culture for infection control. These findings indicate that both individual awareness and the organizational infrastructure jointly influence staff performance in infection control.
This aligns with previous studies by Kim and Park and Harb et al, which highlighted the importance of infection control education and an enabling environment for the prevention of HAIs.8,16 Interestingly, neither occupation nor educational level emerged as significant predictors in the regression model. This suggests that although these factors influence perceptions of infection control, they may not directly enhance infection control performance unless mediated by cognitive and cultural factors, such as awareness and shared organizational values. Similarly, while the infection prevention environment showed positive correlations with other variables, it was not a significant predictor in the regression analysis. One plausible explanation is that the environment may exert an indirect influence on infection control performance by enabling or symbolizing organizational commitment, reinforcing professional norms, and supporting the internalization of infection control values among the staff. In other words, the environment may shape behavior primarily through its effect on perceptions and the development of an infection control-oriented organizational culture rather than through a direct behavioral pathway.
Despite these meaningful findings, some limitations of this study should be acknowledged. First, data were collected using self-reported questionnaires, which may be subject to response bias, including social desirability and recall bias; therefore, actual infection control practices may differ from reported behaviors. Second, the study sample was limited to healthcare workers in LTCFs, which may restrict the generalizability of the findings to other healthcare settings, such as acute care hospitals or community-based facilities. Third, unmeasured confounding variables, including leadership style, workload, staffing levels, and institutional resources, were not included in the analysis, which may have influenced infection control performance. These factors should be taken into consideration in future research.
Future studies should further investigate these potential mediating pathways through replication and longitudinal research. In particular, longitudinal and intervention-based studies would be valuable for clarifying causal mechanisms and evaluating the effectiveness of organizational and educational strategies over time. Overall, the findings of the present study underscore the importance of fostering a strong organizational culture focused on infection control, coupled with strategies to enhance healthcare workers’ perceptions of standard precautions. This has particular relevance for non-clinical and frontline care workers in long-term care settings. The results also highlight the need for integrated interventions that extend beyond education alone, incorporating leadership engagement and culture-building initiatives to empower all staff, regardless of their role, to actively participate in infection control efforts.
Conclusion
In summary, our results confirmed that perceptions of standard infection control guidelines and organizational culture for infection control are key determinants of infection control performance among healthcare workers in LTCFs. These findings highlight the need to improve infection control awareness and foster a supportive organizational culture, especially for non-medical staff such as nursing assistants and caregivers, to enhance adherence to infection prevention practices. Practical strategies to achieve this could include implementing leadership “safety walk-rounds” to actively monitor and support staff compliance, establishing peer mentoring programs to reinforce best practices, or integrating infection control metrics into regular staff feedback and recognition systems. Given the study’s cross-sectional design and reliance on self-reported data, causal inferences were limited. Future research should adopt longitudinal approaches to explore how organizational culture and awareness contribute to sustained behavioral change, particularly in settings with diverse healthcare roles.
Supplemental Material
sj-docx-1-inq-10.1177_00469580261432983 – Supplemental material for Factors Influencing Infection Control Performance Among Healthcare Workers in Long-Term Care Facilities: A Cross-Sectional Study
Supplemental material, sj-docx-1-inq-10.1177_00469580261432983 for Factors Influencing Infection Control Performance Among Healthcare Workers in Long-Term Care Facilities: A Cross-Sectional Study by Yon Hee Seo and Kyong Ah Cho in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Ethical Considerations
This study was approved by the Institutional Review Board (1040191-202502-HR-002-01) at Gyeongkuk National University. All methods were conducted in accordance with the relevant guidelines and regulations.
Consent to Participate
Written informed consent was obtained from all the participants.
Author Contributions
KAC contributed to the concept and design of the study, collection, and analysis of data, and drafting of the manuscript. YHS contributed to the concept and design of the study, statistical analysis, and interpretation of results. All the authors have read and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT; IRIS-2025-24533209).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data related to the study is available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.