
Abstract
Intensive care units (ICUs) are challenging environments for healthcare professionals (HCPs), patients, and families. Up to 75% of HCPs experience psychosomatic symptoms and 30% intend to leave their job. To address this, a German ICU implemented an integrated psychosocial care model. Its implementation and evaluation are described. In a quasi-experimental design, a psychologist was integrated part-time into an ICU team for 7 months (June 2022-January 2023), tasked to deliver low-threshold psychosocial support to HCPs. Additional components were one-on-one interactions, clinical supervisions, a feedback survey and health circles. Pre- and post-measures from a voluntary sample of the intervention ward (N = 65) and a control ward receiving usual psychosocial care (N = 33) were taken via online surveys assessing the psychosocial safety climate (PSC), emotional and cognitive irritation and intention to leave. Groups were compared using linear mixed-effect models. The intervention was implemented as planned, and HCPs expressed satisfaction with the changes experienced on the ward. Statistical testing revealed no significant interaction effects between point of measurement and group allocation on irritation and intention to leave (P > .01). The PSC interaction effect did not reach the significance (α = .01, P = .02) but indicated a trend towards improvement in the intervention group. The intervention successfully provided accessible psychosocial support and fostered a more positive PSC within the ICU team. Statistical effects were limited, likely due to the quasi-experimental study design, small sample size and group imbalances, highlighting the need for larger, more controlled studies.
Keywords
Introduction
There is broad evidence supporting the observation of rough and stressful working conditions in intensive care units (ICUs) since decades. About 28% of ICU nurses from 23 countries worldwide intend to leave their job. 1 Chronic work stress among ICU healthcare professionals (HCPs) are linked to burnout, 2 second victim traumatisation, 3 depression, addiction and suicidality, 4 all of them being connected to the workplace which some even perceive as a “hostile environment.” 5 In addition to health related problems, psychosocial phenomena such as compassion fatigue or moral distress result from it; the latter substantially influencing job turnover intention. 6 These consequences are not only an individual problem but also a public health matter: burnout is associated with reduced productivity, 7 early retirement 8 and compromised patient safety.9-11
There are currently no nationwide structures in Germany to support ICU teams. Only about 20% of surveyed HCPs reported access to psychosocial support measures such as counselling, case discussions and supervision.12,13 Although more and more hospitals are offering clinical supervision for HCPs, these programmes are limited in spontaneity and frequency and may be hindered by time, space and trust barriers. 14
Support strategies targeting individuals may only be moderately effective in reducing psychological distress, 15 as HCP stressors arise at a team or organisational level as well. Team-level stressors include for example, challenging relationships with team members, 16 whereas organisational stressors encompass issues such as poor policy guidance on end-of-life decision making. 17 Consequently, experts increasingly call for low-threshold acute psychosocial care18,19 implemented through organisational interventions. 20 Such ratio-preventative measures may help strengthen team cohesion and foster social support 15 to combat the aforementioned stressors.
The Psychosocial Safety Climate (PSC) 21 theory provides a framework which links organisational culture with employee well-being. PSC describes how employees feel about whether their organisation considers their mental health in decision-making.
High PSC can act as a preventive stress measure for employees through the commitment of senior managers, 22 enhancing employees’ physical health. 23 Organisational factors such as positive leadership can also reduce nurse turnover. 24 PSC can predict the persistence of depressive symptoms 25 and has a positive influence on job burnout 26 and work safety. 27 PSC is therefore increasingly used to measure the effects of workplace interventions. 28
Despite growing awareness, organisational approaches to psychosocial support remain scarce in German ICUs. Our experiences at the University Hospital in Ulm and at the Charité in Berlin during the Corona pandemic29,30 showed that integrating psychologists into ICU teams on a permanent basis can be beneficial. 31
In 2022, reacting to the need for psychosocial support identified by the chief physician of a neurosurgical ICU, we developed a rapid-response intervention to address these issues. Building on previous experiences and guided by PSC theory, we developed a complex intervention centred on the prolonged integration of a psychologist into the ICU team, complemented by system-level measures.
Over the following weeks, this model was adapted to the new ICU’s needs through ongoing feedback. To evaluate the intervention’s effects, a pre-post quasi-experimental design was applied. Our research question was: (1) Will a 7-month integrated psychosocial intervention on an ICU improve the team’s wellbeing, measured by PSC, workplace-related stress (irritation) and turnover intention, compared to a control group?
Methods
Study Design
We used a longitudinal quasi-experimental design, as the control and intervention group could not be assigned randomly due to prior agreements. Consequently, potential baseline differences between groups cannot be ruled out. For drafting and editing this manuscript, the SQUIRE reporting checklist 32 was used, see Supplemental Appendix 1.
The intervention unit was a neurosurgical ICU of a district hospital in the south of Germany (NC: 12 beds). It consisted of 2 subgroups: staff of the NC unit (Subgroup A) and anaesthesiology department (Subgroup B). Subgroup B works closely with Subgroup A and experiences very similar conditions, thus they were analysed together. The control unit was a neighbouring neurological ICU (NL;12 beds + 2 emergency care beds), selected for similar structure and size. The control group was granted the opportunity to receive the intervention after the end of the study. They were aware that the intervention group received an intervention; blinding was not possible. Occupational health services and human resources were available as usual for both groups. Employment on the intervention or control ward was the only inclusion criterion administered.
The intervention was implemented from June 2022 until January 2023. Initially planned for 5 months, it was extended to 7 months upon request. For an overview of the study timeline and components, see Figure 1.

Study design and timeline.
We enrolled a survey to evaluate intervention effects at 2 measurement points. Active participation in the intervention (eg, talks with the study therapist) was not required for survey participation, and vice versa.
Intervention
The intervention was installed quickly due to the acute circumstances and refined iteratively.
The development team comprised SN (study psychologist (SP) and advanced trainee psychotherapist), HG (senior physician and head of the group) and KH (senior psychotherapist and supervisor).
The intervention aimed to evaluate, clarify and address the psychosocial needs of HCPs. Five intervention components were used to achieve this goal (see Figure 2): The central element was the presence of a SP in the unit, working as a psychological professional and contact person for HCPs, accompanied by clinical supervision groups, an initial exploratory survey, and team meetings (health circles; German “Gesundheitszirkel”) with all team members.

Components of the intervention.
The intervention started with the introduction of the SP to the team, followed by weekly visits over the course of 7 months.
Presence of a Psychologist
Presence of the SP was administered on the intervention ward between 08/06/22 and 11/01/23. During this time, the SP visited the ICU once a week for 3 to 5 h, occasionally more often upon request, and was available by phone. For the means of hygiene and as a symbol of integration, she wore the same scrubs as the HCPs. The psychologist’s role was defined as providing psychosocial care on the ward, emphasing organisational and systemic team support. Any issues that fell outside this remit, such as evident mental health conditions, were referred to other professionals. Regular supervision of the SP with a senior clinical psychologist (KH) ensured governance. The SP had 2 main roles: (a) participatory observation and (b) in-situ coaching. A: Becoming a team member, the SP gained insight into unit dynamics and identified team issues through immersion, facilitating understanding of the atmosphere and its challenges. These observations were later shared within the health circle in a processed form, adapting Bion’s33,34 method of containing. Containing is a therapist’s ability to receive, process and return the client’s overwhelming emotions in a more manageable form, for example by summarising and non-judgmentally reframing staff concerns to support shared understanding.
B: The second role involved informal activities that we referred to as “in-situ coaching” or, in more colloquial terms, “clinical supervision over a cup of coffee,” highlighting the low-threshold, trust-based nature of these supportive and reflective conversations with HCPs. These encounters can be considered as “therapeutic priming” 35 while introducing a therapeutic attitude and evidence-based techniques such as resource activation, problem actualisation, and motivational clarification. 36 Unlike traditional psychotherapy, this approach was proactive, by reaching out to staff the SP perceived as stressed. Confidentiality was a key factor in combining both roles in 1 person. HCPs were informed that participation in all intervention components was voluntary and that they could decline pro-active offers or withdraw from them at any time without consequences. The SP was bound by professional confidentiality, so all disclosed information was only ever shared in an aggregated and anonymous way, unless otherwise agreed on. The SP’s close integration into the team enabled the mirroring of perceptions and emotions with authenticity and credibility that facilitated acceptance and created a feeling of cohesion. We also assumed that, as Colville, 37 (p. 107) put it, “even where the psychologist is not providing formal staff input, their very presence in a team serves as a reminder that there is a psychological dimension to care.”
One-On-One Interactions
Sometimes, interactions between single team members and the SP exceeded the form of brief catch-ups on the ward as they required more time or space. They could then be transferred to a quiet place on the ward or be scheduled to a longer session outside the ward.
Clinical Supervision
N = 3 scheduled clinical group supervision sessions were administered separately for the team (26/07/22), the ward management team (18/10/22) and for the senior physicians’ team (01/12/2022), as requested. The sessions were led by KH, assisted by SN and consisted of 3 to 15 participants. They lasted 90 min. Participation was voluntary.
Feedback Survey
The two-point evaluation survey served 2 purposes: (1) Examining the unit’s needs to objectively substantiate and communicate them. Further, to shape the intervention accordingly by reaching a consensus on the changes the unit wants to work on. And (2) Measuring cues for effectiveness of the intervention (see section 2.4.).
Health Circle (“Gesundheitszirkel”)
A health circle is a group consisting of members from different professions and hierarchies on the ward, brought together with the goal of implementing “workplace-related organisational changes [..] with the participation of employees” 38 (p. 259). The health circle met 4 times in total, every 2 to 3 months for 90 to120 min. It consisted of 4 to 20 members from the unit as well as the psychosomatic team. During these meetings, information collected to date was presented and discussed. The psychosomatic team’s role was to support, moderate, and help the ICU team develop actionable measures. The circles also promoted communication among all members of the unit. Decisions resulting from these discussions were then communicated uniformly. The first health circle took place on 01/06/2022 as a “kick-off” meeting for brainstorming issues. The following health circles took place on 13/07/2022 to discuss feedback survey results. The subsequent circle took place on 20/09/2022. In October, a new senior physician working model was implemented, based on decisions made by the health circle. The final health circle took place on 15/12/2022. The meeting protocols were sent to all participants by email afterwards.
Measures
We used the online survey tool Unipark 39 to conduct a 40-item questionnaire (see Supplemental Appendix 2) among the members of the intervention and control unit. It included 7 demographic items and 5 questionnaires totalling 30 items, as well as 3 open questions. These invited participants to comment on areas of concern, ideas for improvement, and anything else important to them. Two questionnaires – the Workability Index 40 and Healthy Work 41 – were applied solely for situational analysis and to provide feedback during the health circles, they are therefore not included in the analyses in this paper.
Approval was obtained from the ethics committee of the University of Ulm (No. 70/22-FSt/Sta) and the staff council. Informed consent for survey participation was obtained from all study participants, digitally via the survey tool. All data was handled as per the EU General Data Protection Regulation (GDPR) and the German Federal Data Protection Act (BDSG), with the goal of best possible data protection and preservation of anonymity.
The T0 and T1 surveys were distributed via E-Mail and QR-code on the ward. The same survey was administered at T0 and T1. At T1, 1 filter item was added to identify prior T0 participation, after which the demographics section was skipped. Missing data were not imputed. The baseline measures for T0 were collected prior to the intervention over a period of 4 months, from February-June 2022. T1 measure took place post-intervention from end of January-May 2023.
Psychosocial Safety Climate (PSC)
PSC was measured using the German 4-item scale. 42 This reliable, validated scale 43 correlates with psychological stress, emotional exhaustion, and engagement. Items are for example, “Psychological well-being of staff is a priority for this organisation.” They are rated on a five-point Likert scale, (1 = strongly disagree, 5 = strongly agree). For calculation and subsequent classification, a sum variable was formed (range 4;20). Based on a Swedish benchmark study, 44 supported by cross-cultural validation in Germany43,45, three categories can be differentiated: A PSC score of 8 or lower is an indicator of urgent need for action (red risk), a score above 8 and up to 12 indicates that more consideration should be given to regulations (yellow risk), and a score above 12 indicates good existing health and safety practices (green risk).
Irritation Scale
Irritation is a construct to describe a “state between mental fatigue and mental disorder,”46 p. 6. It can be measured using the irritation scale, 47 which is a reliable self-report scale “to economically indicate the potentially damaging effect of critical working conditions.” There are positive correlations with anxiety and emotional exhaustion, as well as physiological stress indicators like systolic blood pressure and cortisol levels. 47 There are negative correlations with life and job satisfaction. 46
The scale consists of 8 items on a seven-point Likert scale (1 = totally disagree − 7 = totally agree); higher scores indicate higher levels of irritation. It contains 2 subscales: the “cognitive irritation” subscale provides an indication of selective, work-related stress (eg, “I find it difficult to unwind after work”); the “emotional irritation” subscale indicates a generalised stress that goes beyond the work context (eg, “I get irritated easily, even if I don’t show it”). We will report the total and subscale values in percentile ranks, according to recent norms from the German population. 48 For statistical modelling in the LMMs, the interval-scaled raw scores will be used to better meet model assumptions.
Job and Career Turnover Intention
Turnover intention (intention to change or leave the current employment) was measured as an indicator for actual job and career turnover. 49 It correlates positively with job demands and negatively with rewards, control, and social support. 50 It was measured using 3 non-validated items from the Nurse’s Early Exit Study. 51 Each item (eg, “How often in the last year have you thought about leaving your job?”) could be answered on a five-point Likert scale, ranging from “never/ a few times a year/ a few times a month/ a few times a week/ everyday.” Higher scores indicate higher Turnover Intention. We used a sum score for analysis (range 5;15).
Statistical Analysis
Due to the mixed comparisons (within- and between-subject) of participants who completed either T0, T1 or both surveys (see Table 1), we will evaluate the effects of group allocation (intervention vs control) and point of measurement (T0 vs T1) as well as their interaction on the dependent variables (PSC, Irritation, Emotional Irritation, Cognitive Irritation and Intention to leave) using linear mixed effects modelling. 52 For the analysis, R 53 and the package lme4 54 will be used. Individual participants will be treated as random effects, group allocation, time of data collection and the interaction of those factors will be included as fixed effects. LMM were estimated using Restricted Maximum Likelihood (REML), which allows inclusion of all available cases, including participants with data from only one measurement point. Missing data were assumed to be missing at random, and no imputation procedures were applied. The results will be interpreted using lmerTest which provides P-value estimates via the Satterthwaite approximation (comparable to a Type III ANOVA). Resulting P-values will be interpreted using a Bonferroni-corrected level of significance of α*<.01 to control for Type I error inflation due to multiple testing across the 5 dependent variables.
Size and Demographic Data of Analysed Sample.

Note. For participants completing both surveys, only demographic data at T0 was examined.
Results
Participants
N = 120 voluntary survey responses from N = 98 participants across all groups were collected (see Table 1). Based on the pseudonym codes assigned at T0, only N = 22 participants could be reliably matched across both survey time points. However, N = 32 participants self-reported that they had participated in T0 and T1. The reason for this discrepancy remains unclear. We analysed the data of all participants, but only treated confirmed matches as repeated participations. N = 76 participants responded solely to the T0 or T1 survey. N = 3 participants relocated between the subgroups of the intervention group during the intervention.
The ratio of female to male participants was higher in the control group than in the intervention group (3.43:1 vs 1.95:1). The ratio of gender-distribution also varied between times of data collection (T0: 2.63:1 vs T1: 1.58:1). The ratio of nurses to physicians was far greater in the intervention group than the control group (1:1 vs 30:1).
Survey Results
Due to the small sample size, reliability was calculated across both time points. All reliability indices showed good internal consistency, except for the non-validated Intention to Leave items (see Table 2).
Reliability Indices for T0 and T1 Combined.

Table 3 shows the means and standard deviations of the dependent variables examined in this study, differentiated by group allocation and point of measurement, as well as the estimated interaction resulting from linear mixed-effects modelling. We analysed the full sample of N = 98 participants from both groups using LMM to account for both within- and between-subject effects. Contrary to our hypothesis, none of the interactions were significant on the basis of the Bonferroni-corrected significance level of α*<.01.
Mean Sum Scores (SS), Percentile Ranks (PR), Standard Deviations (SD, in Brackets) and Sample Size (N) per Subgroup of the Dependent Variables by Group Allocation and Point of Measurement along with the Resulting Test Statistic, P-Values and 99% Confidence Intervals of the Interaction Effects.

Regarding Irritation Scale, there were no significant main effects of group allocation or time of data collection. We categorised the irritation scores using Stanine 55 and percentile ranks 48 into the 3 categories unobtrusive (Stanine <7, PR <77), threshold (Stanine = 7, PR = 77-89) and noticeable (Stanine ≥8, PR >89). All mean percentile ranks fall within the normal range, with the exception of the subscale cognitive irritation (work-related stress) of the intervention group, which is in the threshold category at T0, but in the normal category at T1. Irritation was overall lower within the control group.
For the non-validated Intention to Leave scale, the LMM suggested a trend towards a main effect of time with overall lower scores at T1 (F(1, 74.14) = 6.01, P = .02). This effect, however, did not reach the Bonferroni-adjusted significance level (α* <.01).
The interaction of group allocation and time of data collection on PSC did not reach the significance level (P = .02) but indicated a trend towards improved PSC scores in the intervention group over time in accordance with our hypothesis. Figure 3 presents the distribution of PSC sum scores across the risk-categories proposed by Berthelsen et al. 44 Descriptively, responses in the intervention group shifted towards the low risk category, while the control group showed an opposite trend with more high risk responses over time.
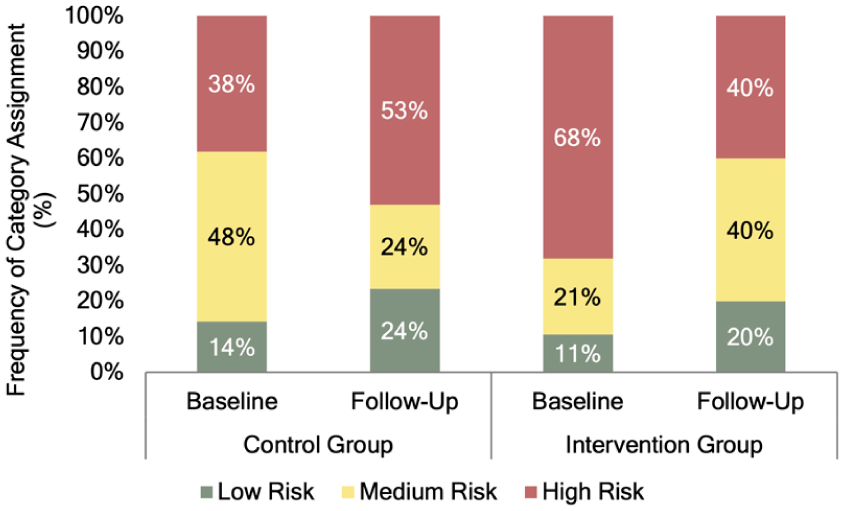
Distribution of PSC sum scores among the low, medium and risk categories by group allocation and point of measurement.
Open Question Answers and Observations Throughout the Study Course
Open responses and observations were summarised thematically to highlight common patterns and support interpretation of the quantitative data. All intervention components (presence of a psychologist, one-on-one interactions, clinical supervisions, health circle, survey) came to use.
In line with quantitative results, the free-text field answers indicated an initially high need for support at T0. For example, 1 respondent wrote; “I have always been able to switch off [of work]. The current situation no longer allows this and is placing an enormous strain on my everyday life.”
Based on the T0 survey and health circle discussions, the ward identified and prioritised its most pressing work issues. The 5 most important issues were: Cooperation with other departments, appreciation of employees’ performance, working without interruptions and disruptions, cooperation between professional groups and having to make difficult decisions. Within the health circles, they were summarised into 3 categories: appreciation, cooperation and workflow. Regarding workflow, a working group of senior physicians as well as a working group comprising nurses and assistant physicians was set up to tackle it. During the intervention, the senior physician structure changed, improving daily availability and clarifying responsibilities – a change welcomed by all HCPs on the ward. Although this was planned earlier, the process was refined and encouraged by the health circle and implemented during the intervention period by the newly formed working group. Appreciation and cooperation were issues that were discussed a lot and brought to the attention of management (physician and nurse).
Concerns about nursing ward management emerged within open surveys responses and one-on-one talks, (eg, experienced lack of cooperation and care towards the nursing staff). With consent, the SP shared these with management, who were motivated to make changes. Despite the concerns, HCPs expressed hope for improved interdisciplinary cooperation. They showed appreciation for the survey, as it made them feel heard and valued.
In supervision and one-to-one meetings, HCPs showed satisfaction with the effects of the intervention, as they perceived an improved team atmosphere and management interest. One team member told the SP that, since the new work model for senior physicians was introduced, time pressure had been “eliminated” and working on the ward had become much more enjoyable. They appreciated being able to focus on important tasks. Another team member said that the nursing staff felt more valued because they were more involved in treatment, their opinions were sought, and they had better access to information. This is also reflected in the positive trends within cognitive irritation and PSC.
To our knowledge, both wards did not use any regular psychosocial services during the time of the intervention. When the control ward was later on offered to receive the same intervention, they declined.
Discussion
In this study, we implemented and evaluated a 7-month ad-hoc integrated psychosocial intervention in an ICU and compared it with a control unit, measuring both groups pre- and post-intervention. All planned components were used and, after an acclimatisation period, accepted and appreciated by the unit. While the quasi-experimental design (with no randomisation) and the small, imbalanced sample size entail serious methodological limitations, discussed later, the findings provide important first insight into the feasibility and acceptability of such an approach. The health circles revealed issues related to appreciation, cooperation and workflow, leading to team-level changes during the intervention. The observations throughout the study period indicated that the intervention fostered a more open and supportive work environment.
Statistical analysis indicated that our hypothesis was rejected, as no significant group-and-time interaction effects were found.
Descriptively, cognitive irritation improved slightly within the intervention group, in line with our hypothesis. We also observed a baseline difference suggesting that the intervention group was more irritated initially – consistent with their expressed need for support. Nevertheless, this imbalance restricts validity of statistical analysis.
A non-significant trend towards reduced Intention to leave was observed in both wards. As the scale was non-validated with moderate internal consistency, reliability of this outcome is limited. The results are not in line with the changes within the other measures, yet it may be attributable to a general post-pandemic easing of stress amongst HCPs. 56
Although not statistically significant, the observed trend towards improved PSC in the intervention group may nevertheless indicate a clinically relevant change, especially as PSC slightly worsened in the control group. These outcomes must be interpreted very cautiously due to the non-randomised design, baseline differences, unequal group sizes and sample imbalances regarding gender and occupation. While some literature indicates effects of gender or occupation on PSC, 44 no robust effects are known. 57 As covariate analysis wasn’t included in our hypotheses, we refrained from conducting it a posteriori.
In the literature, PSC correlates negatively with psychological distress 58 and shows similar patterns to work-related strain. 59 However, findings are inconsistent, as some studies reported no link between PSC improvement and well-being or work-related outcomes. 60 Overall, interventions designed to enhance PSC generally appear to succeed in this goal.59,60 Against this background, the direction of the observed change in PSC in the present study may reflect a meaningful intervention signal. However, this must be interpreted in light of the methodological limitations.
From a theoretical perspective, the observed PSC improvement may relate to psychosocial care being implemented at management’s request, potentially perceived as a sign of management care. Additionally, the intervention may have improved social connections, leadership, trust, workplace values and healthy coping strategies, 61 all of which are embedded within PSC. This interpretation is supported by HCPs reports of workplace improvement. Given the non-blinded nature of the study, a confounding Hawthorne effect cannot be ruled out. The opposite development in the control group could reflect contrast effects, as they may have felt disadvantaged. Alternatively, working conditions may have worsened organisation-wide, but were mitigated by the intervention.
Limitations
As a quasi-experimental field study, this research was subject to significant methodological constraints. Participants were neither randomised nor blinded, and the sample was small and imbalanced. Expectations, hope or floor effects may have influenced the outcomes. Owing to the limited sample size, longitudinal matching (only N = 22 matches) or advanced bias-reduction approaches (eg, propensity score matching) were not feasible, leaving possible residual confounding.
Responses at T1 may have been influenced by the intervention group being informed of the T0 results at the second health circle. Sample size and group imbalances (by gender and profession) did not cause convergence issues within the formulated LMMs, 62 yet they still influence statistical power and increase the risk of type-II errors. 63 In particular, these differences may have influenced the baseline levels, responsiveness to the intervention, and outcomes. Some mismatch of participant codes between T0 and T1, likely due to spelling mistakes, complicated longitudinal analysis and indicate caution. While unplanned, the modest extension of the study duration by 2 months is unlikely to have affected its statistical power or internal and external validity, given the quasi-experimental design and the fact that no formal power calculation was conducted a priori.
The intervention supported a major structural change increasing the availability of senior physicians. As this change overlaps with key intervention components, particularly management engagement and improvements at the ward level, intervention-specific effects cannot be clearly disentangled from it. Integrating a psychological professional into the team posed some challenges. The unfamiliarity came with barriers of incomprehension and occasional rejection. It required sensitivity to group dynamics and awareness of individual and collective motives as well as hierarchies. Uncertainty in acute medical teams about the role of the SP has been well documented, 64 highlighting the need for clear role definitions.
It remains unclear whether a dose-response effect exists. With an intervention lasting only 3 to 5 h per week, the level of intensity was limited, but the approach was cost-effective.
Conclusions
Although beneficial in practice, the statistical results of our study were weak. As this was a quasi-experimental study design, these effects were to be expected. Future studies require larger samples and a more controlled experimental design which allows for example, matched longitudinal data. Further methodological refinements like stronger intervention definitions, blinding or variation of intervention dose could increase statistical power, yet they limit complexity and freedom of this adaptive approach. To advance psychosocial care in ICUs, the field needs a precise evaluation of the needs and resources of ICU staff and other affected groups. There seem to be shared needs between the different affected groups on ICUs, 65 which emphasises the need for a broader and holistic cross-group perspective. Ideally, health intervention development should follow stages from a model or theory of the problem to a model of change, programme design, production, and finally implementation and evaluation. 66 Our work continues in the ongoing “IPS-Pilot” project; refining the intervention and evaluating its feasibility in a pilot RCT in 8 German ICUs. 67
Supplemental Material
sj-pdf-1-inq-10.1177_00469580261428687 – Supplemental material for Impact of an Integrated Psychosocial Intervention for Health Care Professionals in an Intensive Care Unit: Controlled Quasi-Experimental Trial
Supplemental material, sj-pdf-1-inq-10.1177_00469580261428687 for Impact of an Integrated Psychosocial Intervention for Health Care Professionals in an Intensive Care Unit: Controlled Quasi-Experimental Trial by Sophie Felicitas Nickel, Simone Korger, Karl Christian Hirning, Klaus Hönig, Christian Rainer Wirtz, Ferdinand Keller and Harald Otto Gündel in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-2-inq-10.1177_00469580261428687 – Supplemental material for Impact of an Integrated Psychosocial Intervention for Health Care Professionals in an Intensive Care Unit: Controlled Quasi-Experimental Trial
Supplemental material, sj-pdf-2-inq-10.1177_00469580261428687 for Impact of an Integrated Psychosocial Intervention for Health Care Professionals in an Intensive Care Unit: Controlled Quasi-Experimental Trial by Sophie Felicitas Nickel, Simone Korger, Karl Christian Hirning, Klaus Hönig, Christian Rainer Wirtz, Ferdinand Keller and Harald Otto Gündel in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
I acknowledge the use of DeepL Translate (DeepL.com) and ChatGPT-5 (chatgpt.com) as writing assistance to generate better translations from my first language in the preparation of this manuscript.
ORCID iDs
Ethical Considerations
Ethics committee approval of the university of Ulm was obtained on 16/05/2022 (No. 70/22-FSt/Sta), approval of the staff council on 31/03/2022.
Consent to Participate
Informed consent for survey participation was obtained from all participants of the study. The consent form was integrated digitally into the survey tool.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The intervention was funded by the Clinic for Neurosurgery BKH Günzburg, which operates the intensive care unit that received the intervention. No funding was received for conducting this study and preparing the manuscript.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The study allowed for a result in both directions. The study therapist is also the author of this paper. However, the analysis was predominantly carried out by SK and FK, who were not involved in the intervention.
Data Availability Statement
Data is available on request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.