
Abstract
This scoping review examined barriers and facilitators influencing dental care access among adolescents (ages 10-19) using a multilevel health disparities framework to capture behavioral, social, and structural determinants. Following the Arksey and O’Malley framework and Joanna Briggs Institute methodology, 6 databases and gray literature were searched for English-language studies (2011-present) on dental care access among adolescents. Data were categorized at individual, interpersonal, community, and societal levels. Fifty-eight studies met inclusion criteria. Common barriers included dental anxiety, minority status, low parental education, limited income, weak peer support, geographic disparities, unstable insurance, and provider shortages. Facilitators included public insurance programs, school-based dental clinics, culturally tailored education, caregiver modeling, and community engagement. An ecomap illustrated multilevel predictors and research gaps, identifying strategies such as peer-led programs, safety-net investment, patient navigation, and policy reforms to strengthen access. Adolescent dental access is shaped by intersecting determinants at behavioral, social, and systemic levels. Coordinated efforts integrating infrastructure, health education, and policy interventions are essential to reduce oral health disparities and inform future research directions. The multilevel ecomap presented in this review provides an adaptable, evidence-based foundation for developing actionable strategies to improve adolescent oral health across different social backgrounds and geographic regions.
Introduction
Adolescents from low-income families (Families with incomes below 200% of the federal poverty threshold—$64 300 for 2 adults and 2 related children in 2025—are often classified as “low-income.” Families fall into “deep poverty” if their income is below 50% of FPL (≤ $16 075) for a family of 4. Source: U.S. Department of Health and Human Services. (2025, January 17). Annual update of the HHS poverty guidelines. Federal Register, 90(12), 3271 to 3272. https://www.federalregister.gov/documents/2025/01/17/2025-01377/annual-update-of-the-hhs-poverty-guidelines.) are disproportionately affected by untreated dental caries and face significant challenges in accessing dental care compared with their more affluent peers.1,2 This disparity highlights the urgent need to prioritize the oral and general health of adolescents, a stage of life that is often overlooked in health research. Adolescents are particularly vulnerable to negative influences from parental attitudes and peer behaviors, which can lead to high-risk practices that negatively affect their oral and overall health, both immediately and in the future.3,4
The Centers for Disease Control and Prevention’s Oral Health Surveillance Reports indicate a troubling trend: although the prevalence of untreated tooth decay among children aged 2 to 11 years decreased by approximately 5% between 1999-2004 and 2011-2016, adolescents experienced a 2% significant increase in the rate of untreated tooth decay. 5 This age-based disparity is particularly pronounced among non-Hispanic Black adolescents from low-income families. Furthermore, the utilization of dental care services has significantly declined among lower-income families, with a lower number of youth across all income levels receiving preventive dental care in the last 5 years. 6 This decline is concerning, as the latest proportion of low-income youths receiving preventive dental visits was 68.7%, significantly below the Healthy People 2030 target of 79.9% for preventive dental visits among youth. 7
The expansion of Medicaid in the late 1990s and subsequent related legislation, such as the Omnibus Budget Reconciliation Act of 1990 (OBRA 1990), aimed to improve access to dental care for children of all ages living in families with incomes at or below 100% of the federal poverty level (FPL); however, challenges remain.8,9 Public dental coverage was expanded after the State Children’s Health Insurance Program allowed states to expand eligibility for public insurance for uninsured children aged <19 years in families with incomes up to 200% of the FPL or 50% points above the Medicaid threshold in March 1997.8,9
The tragic death of a 12-year-old boy from Maryland, United States (U.S.), in 2007, caused by complications from an untreated dental infection, dramatically highlighted the challenges Medicaid-enrolled children experience in finding dental providers. 10 This case, wide publicized in the U.S., demonstrated how limited dental coverage and the low participation of dentists in Medicaid can have fatal consequences. The incident sparked advocacy leading to key legislative reforms, including the Children’s Health Insurance Program (CHIP) Reauthorization Act of 2009, which required all U.S. states to provide dental coverage since 2010. 11 . This example underscores the broader importance of addressing dental care disparities globally, as similar gaps in coverage, provider participation, and care coordination may exist in other countries and warrant critical re-examination of how dental care is organized and financed.
This scoping review summarizes the main factors related to dental care access among adolescents across the U.S., shedding light on the complexities of this critical issue and identifying areas for policy or programmatic intervention. By applying the National Institute on Minority Health and Health Disparities (NIMHD) Research Framework 12 and focusing specifically on adolescents, this review offers a novel, multilevel perspective that extends beyond service utilization to capture the broader determinants of access.13,14
Materials and Methods
This scoping review followed the methodological framework suggested by Arksey and O’Malley 15 and the Joanna Briggs Institute (JBI) methodology for scoping review. 16 The protocol was prospectively registered on the Open Science Framework. 17 Link is provided with Supplemental File S1. Reporting adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines to ensure comprehensive and transparent reporting of methods and results. 18
Search Strategy
An electronic search for hindrances to dental care access among U.S. adolescents was conducted in 6 information resources by a health science librarian (ES) between December 15-19, 2023. Databases included PubMed (https://pubmed.ncbi.nlm.nih.gov/), Embase (via Elsevier, including Embase Classic and Medline), and the Cochrane Central Register of Controlled Trials (via Ovid). Gray literature was searched in ProQuest Dissertation and Theses Global, Clinicaltrials.gov, and NIH RePORTER. Searches were limited to English-language records from 2011 onward. A date limit of 2011 to present was utilized as it was not until 2010 when the implementation of the Affordable Care Act required all states to cover children up to age 19 with family incomes below 133% of the Federal Poverty Level through the Medicaid program, thus facilitating more possible access to dental care across individuals of all socioeconomic background. 9 PubMed and Embase utilized a validated U.S. search hedge, 19 and a modified pediatric hedge 20 was applied across PubMed, Embase, Cochrane Central, and ProQuest. Only U.S.-registered trials were included from ClinicalTrials.gov. The exact searches used in all information resources are documented and available via the Open Science Framework. Link is provided with Supplemental File S1.
The searches were updated on August 16, 2024. Results were exported to EndNote 21, 21 de-duplicated using the Systematic Review Accelerator De-duplicator, 22 and uploaded to Covidence 23 for screening.
Inclusion Criteria: Population and Concept
The target population was adolescents, defined as individuals aged 10 to 19 years. The aim was to identify studies that specifically addressed hurdles and facilitators of dental care access among adolescents from different backgrounds.
The concept was informed by the NIMHD Research Framework, 12 a comprehensive, ecological model that identifies individual, interpersonal, community, and societal determinants of health disparities. Furthermore, it broadens the focus of the NIMHD framework beyond the utilization of dental services to include a wider range of domains that affect overall care access.
Exclusion Criteria
Studies were excluded if they provided only general child data without adolescent-specific information. We also excluded theses, abstracts, incomplete trials, surveillance/trend reports, and studies from non-US populations.
Study Screening
Two independent reviewers (RCGO and HK) screened titles and abstracts, resolving discrepancies through discussion and consulting a third reviewer (SS) when needed. Full-text screening was conducted by RCGO and SS, with disagreements resolved by consensus discussion. Study methodological quality was assessed for all included studies using the JBI critical appraisal checklist, with reviewers independently evaluating studies via a web-based tool based on each study’s design. Summary appraisals were compared using the JBI SUMARI database to produce a final critical appraisal. 24 Screening and appraisal continued until a 95% reviewer agreement was achieved. The PRISMA-ScR flowchart (Figure 1) outlines the process; out of 312 full texts reviewed, 254 were excluded, resulting in 58 studies.

Preferred reporting items for systematic reviews and meta-analyses extension for scoping reviews (PRISMA-ScR) flowchart.
Data Extraction and Charting
Data extraction was performed using a customized Covidence spreadsheet 23 that captured study design, population, setting, outcomes, predictors, sample characteristics, frameworks applied, and key findings (Supplemental Table 1).
The extraction tool was pilot tested on 15% of the studies by 3 reviewers (RCGO, HK, and SS), with iterative refinement to ensure completeness. A random 10% subset of studies was independently double extracted to very consistency, yielding a high inter-rater reliability (κ = .95). Any discrepancies were resolved via consensus or third-party adjudication.
Data Synthesis and Analysis
Extracted data were collaboratively analyzed to identify key themes, representing barriers and facilitators of adolescent dental care access. These themes, informed by target predictors form the included studies, encompassed parental and adolescent behaviors, attitudes toward dental health, demographic characteristics of parents and adolescents, geographic variations, insurance coverage, workforce availability, and vulnerable groups.
Themes were categorized across individual, interpersonal, community, and societal levels consistent with the NIMHD Research Framework. The qualitative synthesis was visually represented using an ecomap to illustrate multilevel determinants and their interconnections. Additionally, a summary table integrated these findings, highlighting actionable interventions and research gaps. By mapping the evidence landscape, this scoping review proposes targeted interventions and a structured approach to addressing the complex factors that shape dental care access for adolescents.
Results
Study Selection
In total, 2904 records were identified in the databases and registers. An additional 44 records were identified through the gray literature. After removing 711 duplicates, 2237 records were screened. Three additional duplicates were discovered during the screening process, resulting in a total of 714 duplicates removed and 2234 records screened. Of these, 1922 were excluded, and 312 full-text articles were assessed. Another 254 were excluded for reasons including wrong design (n = 106), population (n = 74), no age breakdown (n = 19), or other criteria (Figure 1). In total, 58 studies were included in this review25 -82 (Table 1 and Supplemental Table 1).
Summary of Evidence on Adolescent Dental Access Barriers and Facilitators.

AEC = ambulatory emergency care; AHRF = area health resources file; aRR = adjusted relative risk; BRFSS = behavioral risk factor surveillance system; CHIP = children’s health insurance program; CPCS = community paramedicine and community support services; DDW = disability-disabled worker; DDIA = delta dental of Iowa; CT DSS = Connecticut department of social services; DRC = data resource center; FC = foster care; IHHS = child and family household health survey; IOR = interval odds ratios; KFF = Kaiser family foundation; MEPS = medical expenditure panel survey; MOR = median odds ratios; NHANES = national health and nutrition examination survey; NHIS = national health interview survey; NSCAW, Wave II = national survey of child and adolescent well-being; NSCH = National survey of children’s health; SBHC = school-based health center; SCHIP = state children’s health insurance program; YRBSS = youth risk behavior surveillance survey.
Behavior and Habits of Parents and Adolescents Toward Dental Health Experience
Adolescence is a critical stage in life that is affected by parental and peer attitudes, which can lead to high-risk behaviors that are detrimental to oral and general health, both in the present and future.1,4 Qualitative and quantitative research has contributed to understanding the complex interplay of beliefs, limitations, and behaviors that shape dental health experiences among youths25 -29 (Table 1 and Supplemental Table 1). One renowned study found that children were at a greater risk of missing dental visits, lacking insurance coverage, and deferring care due to costs, reflecting their parents’ experiences. 26 Key risk factors for children included older age and minority status, whereas protective factors included public insurance, higher parental education, and female-led households. 26
Moreover, social influences were significant, with 71% of individuals indicating that peers and family affected their dental care decisions in a study of Mexican American teenagers in urban Indiana. 25 The same study revealed that 77% believed they needed urgent dental treatment, and 94% preferred seeking private dentists over emergency rooms. Despite recognizing the importance of preventive care, many teenagers reported barriers including dental anxiety, perceived high costs, and practical limitations, such as constrained office hours and conflicting schedules. In a study of African American and Hispanic/Latinx adolescents, regular flossing was associated with better access to dental supplies. Notably, among non-flossers, sex, grade level, and school-based instruction were significant predictors of adopting preventive health behaviors, highlighting the need for targeted oral health education. 27
The financial aspects of dental care affect parental behavior in postponing or avoiding dental appointments for children. Adolescents aged 10 to 19 years often incurred higher costs for dental services than adults. 28 In addition, many parents or caregivers encountered difficulties related to costs, appointment wait times, and a lack of clarity about which healthcare providers accept their insurance, 29 emphasizing the economic challenges faced by families seeking dental care and the effects of such difficulties on their decisions on what should be prioritized. Taken together, these findings highlight the disconnection between perceived needs and health behaviors, which may present major hurdles.
Demographics
Race and Ethnicity
Recent studies have revealed significant disparities in adolescent dental health in the U.S., which are primarily affected by race and socioeconomic status30 -45 (Table 1 and Supplemental Table 1). Black, African-American, and Mexican-American adolescents were more likely to experience untreated tooth decay in both primary and permanent teeth compared to adolescents from other racial or ethnic backgrounds. 5 More worrisome is that these groups are less likely to have dental visits, as shown by various studies across different states.32,35,37,38 Non-white, non-native English-speaking, undocumented children were disproportionately affected by missed opportunities for preventive care. 40
Children in states offering public insurance, regardless of documentation status, were more likely to have health insurance and access preventive medical and dental care. 40 Among immigrant populations, those from non-citizen households living in the U.S. for less than 5 years had language barriers associated with a lower prevalence of pit and fissure sealants, compared to children who were U.S. citizens at the time of the survey. 45
Socioeconomic Status (SES)
SES, a composite measure that typically includes income, education, and occupation, has long been associated with disparities in access to healthcare, including dental care. Multiple studies in the U.S. consistently showed that children from low-income families were more likely to experience untreated tooth decay and other oral health problems83 -88 (Table 1 and Supplemental Table 1). In addition, the effect of SES on dental health varies with age, with adolescents being the most affected.30,31 For instance, the income gradient for untreated decay was reduced among children aged 9 to 11 years but re-emerged in older children aged 12 to 17 years.
Low-income families were less likely to have access to dental insurance and preventive care. 36 Furthermore, uninsured children were less likely to visit the dentist, and parental education could influence whether children receive regular dental care. Specifically, caregivers with higher educational levels were more likely to ensure that their children regularly visited dentists.
Associations between family income and oral health outcomes were frequently diminished when adjustments were made for factors such as dental insurance coverage, parental education, and occupation.39,43 This attenuation suggests that although SES was a critical factor influencing access to dental care, it was not the sole determinant of oral health. For example, a study found that even with a higher family income, there were persistent racial and ethnic disparities in dental care access, indicating the effect of other structural factors within the oral healthcare system that mediate the availability of preventive care services. 39 The complexity of SES-related disparities was further demonstrated by another study that introduced a cumulative risk index incorporating social factors beyond income. 43 Elements such as lower parental education levels and poor maternal mental health have been shown to increase the risk of poor oral health outcomes, thus demonstrating that the effects of SES on dental care access are multidimensional and interconnected with other social determinants of health.
Several studies have examined the impact of parental education on children’s oral health outcomes.33,41,42 One study reported that parental education level had a direct and positive association with income and insurance status in models for Hispanic and non-Hispanic Black children. 41 Similarly, a parental education level of eighth grade or lower was associated with poor oral health outcomes. 33 Earlier research has reinforced these disparities among less-acculturated Latinos. 42
Encouragingly, more recent findings suggest progress in reducing these gaps, with some studies reporting no significant racial differences in rates of preventive care use and an increased proportion of non-white youths accessing care from public health dental hygiene practitioners.34,44
Geographic Variations
Adolescent dental care remains low and is influenced by place of residence. 47 Geographic factors significantly affected access to care, as shown in multiple US-based studies46 -56 (Table 1 and Supplemental Table 1). These studies used various proxies for geographic disparity, including ZIP code-level poverty, 46 urban-rural strata,48,49,52 -54 neighborhood support and attributes, fluoridated water access, 50 dentist availability,50,52,53,55 and other ZIP or state-level indicators.47,51
Adolescents living in urban areas were generally more likely to receive preventive dental care than those living in rural areas.46,48,49,54 Moreover, children in rural areas were more likely to report their oral health as fair or poor. 48 Beyond self-reported poor dental conditions, a Wisconsin-based study highlighted a higher frequency of restorative, endodontic, and extraction procedures among youths in rural areas, in contrast to a greater number of preventive care procedures in urban areas. 46
A series of studies in Iowa identified regions with particularly low rates of dental care utilization, often corresponding to areas with limited dentist availability and longer travel distances for preventive annual visits.53,54 In contrast, a different analysis of orthodontic service utilization among Medicaid-enrolled youth aged 10 to 13 years found an opposite trend: areas with lower population density and greater average travel distances to orthodontic providers had higher utilization rates than smaller, more densely populated regions. 52 Similarly, another study found that lower population density was an important geographical factor associated with higher utilization of dental sealants on permanent first molars in Wisconsin. 55
State-level variation accounted for a small but notable proportion of the overall disparity in dental care access, suggesting that state policies and local healthcare infrastructure played a substantial role in shaping service delivery. 51 Given that access to dental care varies across states (intraclass correlation coefficients [ICC] = 3.66%), state-level planning must account for these factors to improve access to preventive care, particularly for children in regions with inadequate dental services.
State-level variability was even more concerning in remote regions such as Alaska, 56 where there was limited access to formal healthcare infrastructure. Alternative dental workforce models, such as primary dental health aides (PDHAs) and dental health therapists (DHATs), helped mitigate some of the challenges to care but also required supportive administrative frameworks for effectiveness.
Dental Insurance
Several studies have explored the impact of Medicaid and CHIP policies on children’s access to dental care, highlighting the role of insurance coverage, Medicaid reimbursement rates, provider fees, and broader social, economic, and demographic factors that affected dental insurance enrollment.57 -71 Despite differences in design and geography, the findings consistently showed that Medicaid policies strongly influence dental care use and reveal persistent disparities.
A consistent finding across studies was that Medicaid and CHIP policies directly affected children’s access to dental care. Most observational studies included in this review found a significant increase in dental care usage among children and adolescents enrolled in Medicaid compared to their uninsured counterparts.57-59,61
However, 3 studies found no significant link between Medicaid coverage and preventive visits or improved oral health outcomes.63,70,71 Medicaid enrollment may not have had a significant effect on preventive dental visits due to low Medicaid reimbursement rates and limited provider availability. These findings highlight the importance of financial incentives and adequate provider networks, beyond simply expanding Medicaid eligibility. Higher reimbursement rates have been linked to increased dental visits and reduced unmet needs.57,61,68 More generous Medicaid payments modestly increased preventive dental visits and improved outcomes, particularly among Hispanic children, emphasizing the critical role of Medicaid’s financial structure in ensuring access to care. 66
Several studies found that Medicaid adult dental coverage improved children’s oral health outcomes after 1 year of coverage, particularly among non-Hispanic Black children.64,66,67 However, some studies have failed to find an association between expanding adult Medicaid dental coverage and improved access for children. For instance, a study on the effects of Medicaid expansion under the Affordable Care Act found no significant change in children’s receipt of preventive dental care associated with Medicaid expansion between states with and without coverage for preventive dental services for adults. 63
Children in families with mixed Medicaid and CHIP eligibility were found to be more likely to be uninsured and miss preventive dental visits than those in families where all siblings were eligible for the same program. 62 This suggests that a mixed eligibility status reduced healthcare access, although the effect was contingent on the specifics of eligibility across siblings. Similarly, Medicaid policy changes that allowed non-dentists to become certified providers and bills for sealants in public health settings have led to increased sealant use. However, non-Hispanic Black children remained underserved despite these improvements. 69
Overall, while Medicaid expands availability, it may not ensure quality and fails to address broader social determinants. Benefit expansions and improved provider reimbursement rates can improve overall access; however, other factors, such as parental coverage, provider participation, and socioeconomic obstacles, must also be addressed.
Workforce Shortage
One common finding across studies was that access to dental care for adolescents, particularly those from low-income families or minority groups, is often hindered by workforce shortages72 -77 (Table 1 and Supplemental Table 1). A recent study highlighted that children who lacked access to a “medical home,” including regular access to dental care providers, were less likely to receive preventive dental services. 72 They noted that lack of coordinated care, insufficient providers, and gaps in healthcare access were key contributors to unmet dental needs.
This finding was validated by another study that identified school-based health centers as promising models for improving dental access. 73 However, these centers often face workforce shortages, particularly in rural areas where the demand for dental services exceeds the availability of qualified providers. Similarly, earlier research on the “Miles of Smiles” school-based program showed that while it effectively reached children in need of preventive care, transitioning them to restorative care was often hindered by a lack of available providers in the community, especially for more complex treatments. 77
Expanded evening hours were shown to reduce no-show rates and improve access for working parents. However, the study acknowledged that this model was not a comprehensive solution. 75 The expanded hours were limited by the availability of healthcare providers, and adolescents in regions with fewer dental professionals had inadequate dental services. Similarly, school-based dental clinics staffed with dental students could improve oral health outcomes. 74 However, reliance on less experienced providers could lead to delayed or less efficient care, especially when more complex procedures were needed. In all cases, workforce availability directly affected the effectiveness of access-improving interventions.
The importance of Medicaid reimbursement to primary care providers for oral health has been explored as a strategy for increasing access to preventive dental care. 76 However, the study found that dental insurance alone did not guarantee access to care for all children and adolescents, particularly those in lower-income households, suggesting that although insurance coverage may be crucial, it cannot overcome structural limitations such as workforce availability and scarcity of providers in certain areas.
Vulnerable Adolescent Groups
Foster Care
Studies78,82 have explored challenges in dental care access among foster youth, emphasizing the role of dental insurance and placement type (eg, kinship care). Youth without dental insurance were 93.5% less likely to meet their dental needs. 78 Another study36,79 reported that children with nonbiological caregivers (eg, foster parents, grandparents) had lower odds of a past-year dental visit than those with biological parents.
Sexual Minority
A study 80 examined access to dental care among sexually diverse adolescents in the U.S. Bisexual boys (adjusted relative risk [aRR] = 2.50), boys with a “not sure” about their sexuality response (aRR = 3.55), and girls with a “not sure” response (aRR = 2.32) were more likely to avoid dental visits than heterosexual peers. Their findings suggested significant limitations in dental care due to factors such as stigma or lack of support.
Ambulatory Care for Dental-Related Emergency Department Visits
A study 81 analyzed Medicaid and CHIP data from Florida and Texas on caries-related emergency department (ED) visits and follow-up dental care. Visit rates ranged from 6.90 to 30.68 per 100 000-member months. Follow-up dental visits were limited, with only 22% to 39% of patients seen within 7 days and 34% to 49% within 30 days. Adolescents aged 14 and older had the highest rates of ED visits but the lowest follow-up rates, indicating poor care coordination between emergency and dental services. This left older adolescents vulnerable to unresolved dental issues, underscoring the need to integrate emergency and dental services for this high-risk group (Table 1 and Supplemental Table 1).
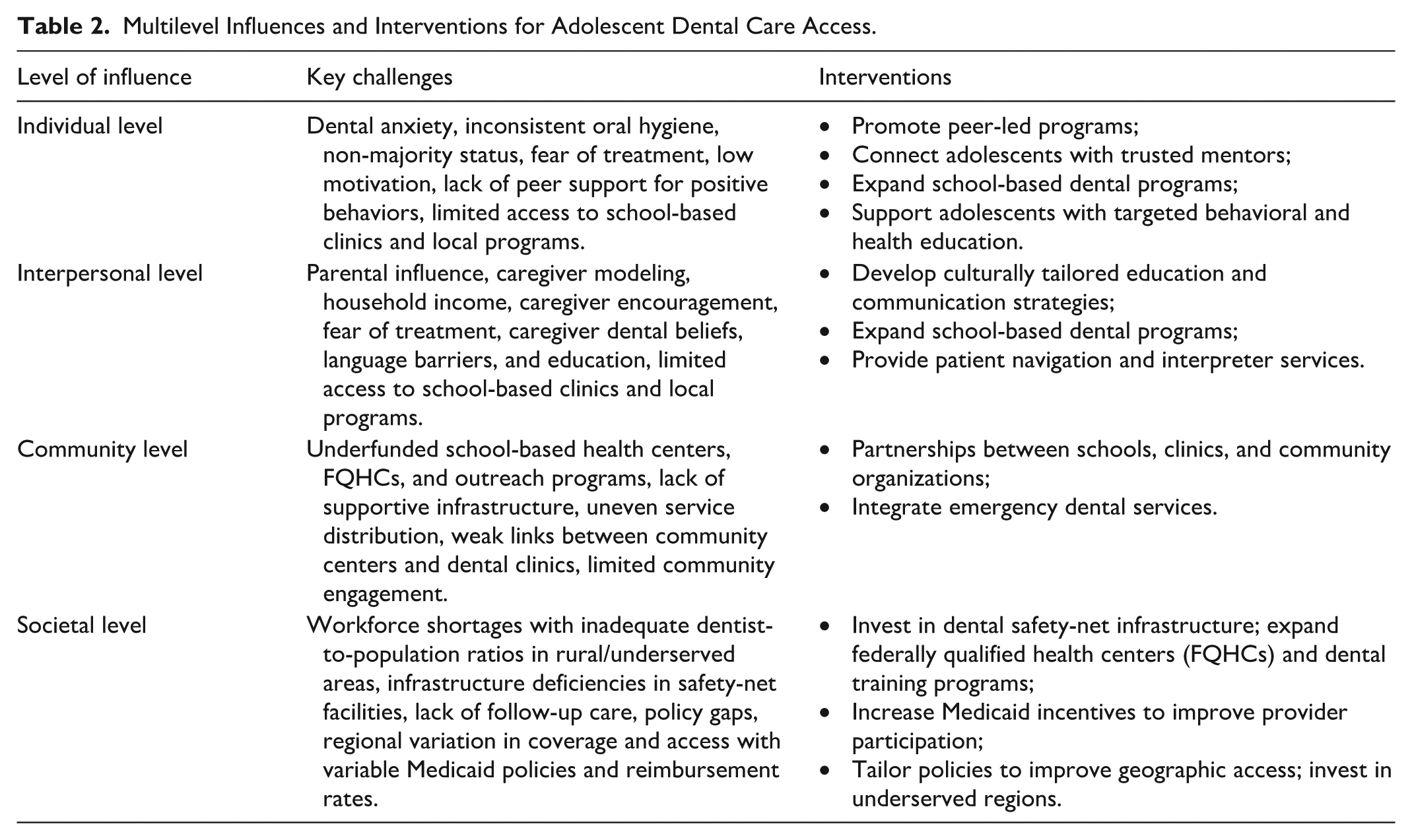
To summarize the findings, we consensually organized the key factors identified across the selected studies into an ecomap (Figure 2), illustrating how adolescent dental care access is shaped by individual, interpersonal, community, and societal influences. The symbols between each factor and the central node (adolescents) indicate the strength and nature of the relationship, whether it acts as a barrier or facilitator, and highlight areas where evidence is emerging or gaps remain. In parallel, we developed a summary table (Table 2) outlining multilevel influences. Together, the ecomap and Table 2 offer a comprehensive overview of the complex factors affecting adolescent dental care and provide actionable guidance for future research, policy, and practice.

Multilevel determinants of adolescent dental care access.
Multilevel Influences and Interventions for Adolescent Dental Care Access.
Discussion
This scoping review highlights the complex, multilevel factors that influence adolescents’ access to dental care in the U.S., guided by the NIMHD Research Framework, and emphasizes that barriers and facilitators persist across the individual, interpersonal, community, and societal levels. The discussion that follows explores these multilevel determinants in greater depth and identifies opportunities for intervention, structural reform, and future research to improve dental care access for this priority population.
Individual Level
Adolescence is a high-risk period for poor oral health and inconsistent preventive dental care.4,5 Contributing factors include minority demographic status, dental anxiety, fear, peer influence, and irregular oral hygiene habits25 -27,78,82 (Figure 2).
Interventions at the individual level can be limited because some obstacles are based on genetics and cannot be overcome. Our review shows that interventions should prioritize continuous oral health counseling and education to improve awareness and motivation.26,27 This includes integrating oral health topics into school curricula, improving access to hygiene supplies, and supporting adolescent engagement through peer-led programs and trusted mentors.25,27,38
Interpersonal Level
Adolescents rely on their parents or caregivers for dental care. Parental behavior and attitudes toward oral and overall health care influence their children’s health-related attitudes. Additionally, social influence can cause teenagers to engage in high-risk behaviors that are detrimental to their health. In our study, parental role modeling, household income, and household demographic characteristics were closely related to the dental care of adolescents. Factors like parental education and language limitations can create additional challenges, making it more stressful for families to navigate dental care and ensure that their children receive the treatment they need (Figure 2).
Some strategies include educating parents on the importance of modeling positive oral health habits for their children32,41 and ensuring that interpreter services are crucial for improving outcomes among linguistically and culturally diverse families.35,37,38,45 Peer support, improved awareness of preventive services and insurance coverage, access to oral hygiene supplies, and financial assistance programs can also help.40,48,60,68
Community Level
At the community level, limited access to school-based clinics, weak links between dental providers and community organizations, and underfunded safety net programs have been frequently reported (Table 2, Figure 2). Supportive environments can be fostered by connecting dental clinics, schools, and community centers. 26 Enhancing culturally competent communication and partnerships with safety net dental clinics can improve care in underserved regions.33 -35,38,42,44,45 Preventive care efforts should target adolescents in rural and under-resourced communities through culturally tailored outreach, incentives for community health workers, appointment reminders, and support in navigating the healthcare system.25 -27,29
However, it is important to acknowledge that improvements in access—such as those created by school-based clinics or community programs—sometimes rely on trainees or less experienced providers. 89 This can lead to delays or less efficient care for more complex procedures and may inadvertently reinforce a “two-tier” system, whereby the most vulnerable populations receive lower-quality care or have limited provider choice. While such community-based interventions are valuable and help mitigate disparities in the short to medium term, they must be complemented by long-term strategies that address workforce shortages and ensure equitable, high-quality care for all adolescents.
Societal Level
Addressing socioeconomic factors at the societal level can help to reduce the limitations of dental care in underserved populations. Along with state policies, neighborhood conditions such as safety, social support, transportation infrastructure, and proximity to providers critically affect access to dental care. State-level differences in dental care availability underscore the need for stronger enforcement of federal regulations and expanded Medicaid dental coverage for children, including foster care alumni. Our findings indicate that although Medicaid policies can improve access to care, the benefits are not consistently experienced across racial and ethnic minority groups. Significant racial disparities exist in terms of the types of dental procedures received by children despite being enrolled in private dental insurance, which can be viewed as an example of “othering”—a process where certain groups are marginalized through assumptions and differential treatment. 90 While no studies explicitly investigated discrimination experiences in dental care, several highlighted persistent structural factors—such as race/ethnicity, income, and geography—that contribute to oral health disparities.32,37,48,73 Whether expanded insurance ensures equitable access to preventive and emergency services remains unclear.55,62 -66,69 This debate may stem from differences in regional coverage, reimbursement rates for dentists, and variations in mandatory benefits across the states.
To address these challenges, policy efforts could include standardizing core Medicaid dental benefits across states, increasing reimbursement to providers to incentivize broader participation, and investing in dental workforce distribution programs in under-resourced areas. Integrating oral health equity goals into broader public health initiatives, such as housing policy, transportation access, and education, can further address the structural determinants that limit access. More granular and county-level research is needed to guide these strategies and identify the most affected communities.
Limitations
This review included studies from 2011 onward. As a result, some potentially valuable data may have been missed because of these restrictions.
Conclusion
This review reveals a systemic issue: mechanisms to improve dental care access through insurance policies or school-based clinics are often undermined by workforce shortages and limited provider participation. This is particularly concerning for adolescents whose dental needs grow more complex with age, especially in under-resourced areas.
State policy interventions should be tailored to address areas with low dentist-to-population ratios by improving physical access, increasing the availability of providers, enhancing affordability, ensuring cultural acceptability, and raising awareness and education regarding available services. Investment in infrastructure is also needed, including the expansion of dental safety net facilities, such as federally qualified health centers, school-based health centers, and academic dental institutions, along with efforts to grow the dental workforce and strengthen referral systems.
Thus, a multifaceted system-level approach is necessary to address the complex factors that affect adolescents’ access to dental care. Future research should examine regional disparities and assess how specific policies impact dental care utilization and overall healthcare access.
Supplemental Material
sj-docx-1-inq-10.1177_00469580261427669 – Supplemental material for Multilevel Determinants of Adolescent Dental Care Access: A Scoping Review Using a Health Disparities Framework
Supplemental material, sj-docx-1-inq-10.1177_00469580261427669 for Multilevel Determinants of Adolescent Dental Care Access: A Scoping Review Using a Health Disparities Framework by Rubelisa C.G. de Oliveira, Sarah Shafik, Hassan Khalid, Elizabeth Stellrecht and Susan C. McKernan in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580261427669 – Supplemental material for Multilevel Determinants of Adolescent Dental Care Access: A Scoping Review Using a Health Disparities Framework
Supplemental material, sj-docx-2-inq-10.1177_00469580261427669 for Multilevel Determinants of Adolescent Dental Care Access: A Scoping Review Using a Health Disparities Framework by Rubelisa C.G. de Oliveira, Sarah Shafik, Hassan Khalid, Elizabeth Stellrecht and Susan C. McKernan in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-3-inq-10.1177_00469580261427669 – Supplemental material for Multilevel Determinants of Adolescent Dental Care Access: A Scoping Review Using a Health Disparities Framework
Supplemental material, sj-pdf-3-inq-10.1177_00469580261427669 for Multilevel Determinants of Adolescent Dental Care Access: A Scoping Review Using a Health Disparities Framework by Rubelisa C.G. de Oliveira, Sarah Shafik, Hassan Khalid, Elizabeth Stellrecht and Susan C. McKernan in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors thank the invaluable contributions of the UB Dental Liaison Librarian Jessica Hollister for her consistent support. We also thank Professor Robert Schifferle for his assistance with language review.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded by the Robert Wood Johnson Foundation (RWJF Fund ID: 80733).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All relevant data are within the paper and its Supporting Information files.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.