
Abstract
Early Childhood Caries (ECC) is considered one of the most prevalent chronic diseases globally, particularly affecting children in socially vulnerable situations. Its significance goes beyond oral health, undermining overall development and quality of life and placing a considerable economic burden on health systems. Given the inadequacy of conventional curative approaches, this manuscript proposes a preventive model based on primary care, structured around an interdisciplinary approach and family-based communication strategies. It analyzes, based on scientific evidence, the fundamental pillars of controlling dental caries in children: promoting health from pregnancy, early education in oral hygiene, and motivational interviews, particularly relevant in contexts with structural and cultural barriers. The role of non-dental health personnel takes center stage in early detection, education, and timely referral. The proposal promotes equitable, sustainable care based on prevention from early childhood, seeking to transform oral health care into a more efficient, inclusive, and long-term oriented paradigm.
Background
Early childhood caries (ECC) is an aggressive form of dental caries with high prevalence and incidence, affecting approximately 1.76 billion children with primary dentition worldwide. With a global prevalence of 48%, its distribution is not homogeneous across regions: 30% in Africa, 48% in the Americas, 52% in Asia, 43% in Europe, and 82% in Oceania. 1 According to the Global Burden of Disease study, Decayed, Missing, and Filled Teeth (DMFT) has multiple consequences for the pediatric population, including pain, odontogenic infections, reduced quality of life, and school absenteeism. This condition is the 12th most prevalent disease worldwide.2,3
In addition to its impact on health, DMFT represents a considerable economic burden. In 2010, the global costs associated with dental diseases amounted to $442 billion, of which $298 billion corresponded to direct treatment costs, representing 4.6% of global health expenditure. Indirect costs, related to lost productivity due to caries, periodontitis, and tooth loss, totaled $144 billion. 4 Children from low socioeconomic backgrounds are the most affected, with a higher risk of developing DMFT. This has a negative impact on their overall development and quality of life, perpetuating the cycle of health inequality. 5
Traditional curative approaches to caries treatment have multiple limitations that reduce their long-term effectiveness. First, they involve high costs that, in many low-income countries, exceed the total budget allocated to medical care. Furthermore, these approaches lack sustainability, as they do not address the underlying causes of the disease, which perpetuates the emergence of new cases, especially among vulnerable populations. 6 It is therefore important to prioritize prevention strategies from the eruption of the first tooth, that is, during the first year of life. To achieve this, it is essential to rely on primary health care centers, since through oral health literacy interventions among parents and caregivers by health professionals, early childhood caries can truly be addressed at its source, curbing excessive sugar consumption and promoting exposure to fluoride, thereby preventing it at both the individual and community levels. 7
Within this framework, the purpose of this article is to highlight the importance of preventing ECC at the primary care level, emphasizing the fundamental role of addressing this disease from an interdisciplinary approach, through continuous training and the implementation of tools such as motivational interviewing. Through a thorough review of the literature and analysis of innovative experiences at the international level, strategic routes are suggested to strengthen children’s oral health through preventive interventions that are culturally adapted to improve the community and family environment.
Search Methodology
This narrative review was developed using a structured methodological strategy to ensure a comprehensive, transparent, and evidence-based selection of the available literature. The search was conducted in the Scopus, PubMed, and Web of Science databases, considering research published over the last 20 years (2004-2024). Original articles, meta-analyses, systematic reviews, and official guidelines were included, with experimental, observational, or mixed designs that evaluated ECC prevention in primary health care. Priority was given to studies that analyzed family education, interdisciplinary approaches, motivational interviewing, and community or digital prevention programs. The search strategy implemented Boolean operators and various combinations of keywords, such as early childhood caries, primary health care, ECC prevention, oral health promotion, motivational interviewing, health education, digital health, interdisciplinary approach, and caregiver communication. Studies that did not reflect scientific rigor or did not directly address interdisciplinary or preventive aspects of ECC were discarded. The included literature was critically examined, analyzed, and synthesized to identify the key elements of determinants, preventive strategies, and innovations aimed at promoting children’s oral health in the primary care setting.
Fundamentals for the Prevention of ECC
Primary teeth are particularly susceptible to caries compared to permanent teeth. This is because deciduous teeth are smaller, have thinner, more porous enamel, and a higher organic content, which makes them up to 1.5 times more vulnerable to developing caries. 8 During the first year of life, when primary teeth erupt in the oral cavity, factors such as early consumption of sugars and fermentable carbohydrates, together with inadequate oral hygiene, further promote the development of carious lesions. In addition, lack of information and the misconception that primary teeth do not require care because they will eventually be replaced contribute to this problem. 9 ECC seriously affects the overall health of children under 6 years of age, interfering with growth and development by compromising chewing, affecting their self-esteem, and causing school absenteeism due to oral infections, with a negative impact on their quality of life.3,10 The role of parents or caregivers is fundamental, as tooth brushing should begin with the eruption of the first tooth and continue until the age of 8, when the child has acquired the necessary skills to brush effectively. 11
Preventive interventions should begin during pregnancy. It is crucial to inform pregnant women about the importance of their own and their baby’s oral health, recommending dental consultations to diagnose and treat conditions such as caries, gingivitis, or periodontitis, without additional risk during any stage of pregnancy. If necessary, periapical radiographs and local anesthetics can be used without additional risk to the mother or fetus. Brushing with fluoride toothpaste twice a day, flossing, and limiting the consumption of sugars and fermentable carbohydrates are recommended. In the event of vomiting, rinsing with water and baking soda is suggested to neutralize gastric acid remnants in the oral cavity. 12
After birth, exclusive breastfeeding should be promoted for the first 6 months and along with complementary feeding until 2 years of age or older, highlighting its benefits for oral health. It is advisable to prevent the exchange of saliva through the sharing of cutlery, cups, pacifiers, or bottles to avoid the transmission of acidogenic bacteria to the infant. The first visit to the dentist should take place during the first year of life to receive guidance on oral health care, the application of sodium fluoride varnish (depending on the individual risk of developing caries), and to detect and treat any defects in enamel development that may be present.13,14 Breast milk provides immunoglobulin A, lysozyme, casein, calcium, and phosphorus, which help remineralize enamel and do not alter oral pH. Breast milk alone is not cariogenic, but when combined with a diet rich in sugars, it can promote the development of ECC.15,16 In addition, prolonged use of bottles containing sugary liquids, especially at night, increases the risk of developing caries lesions, as does frequent consumption of added sugars and fermentable carbohydrates during the day, which is the main etiological factor in tooth enamel demineralization. 17
Likewise, foods and beverages with added sugars should be avoided in children under 2 years of age, not only to prevent the development of caries lesions, but also to reduce the risk of cardiovascular disease in adulthood.2,12,18,19 In addition, fluoride varnish applications are recommended every 6 or 4 months to reduce the risk of ECC.14,26
Fluoride is a key tool in the prevention of ECC. It strengthens tooth enamel by converting hydroxyapatite to fluorohydroxyapatite, which is more resistant to pH drops of up to 4.5. 20 The use of fluoridated toothpaste is recommended, using an amount equivalent to the size of a grain of rice in infants under 3 years of age and the size of a pea after this age. Do not rinse with water after brushing to maximize the anticariogenic effect of fluoride.18,21 Brush at least twice a day and lift the lip to fully expose the front surfaces of the upper teeth and lower the lip to fully expose the front surfaces of the lower teeth.12,22 The Bass technique is recommended for its effectiveness. On the chewing surfaces, use back-and-forth strokes; on the front surfaces, place the brush at a 45° angle at the junction between the tooth and gum, brushing from bottom to top on the lower teeth and from top to bottom on the upper teeth; and on the inner surfaces of the teeth, repeat the procedure with the same angle.23,24
First Level of Care as a Strategic Platform
Primary care represents a fundamental strategic platform for both the prevention and early detection of ECC.25 -28 Thanks to its proximity to the community and its role as the first point of contact with the health system, it is ideally positioned to implement timely and effective actions and interventions that have a tangible impact on children’s oral health in the early stages of life. 26
Adequate prevention of ECC requires an interdisciplinary approach that encompasses the knowledge, skills, and experience of multiple health professionals. This approach allows for addressing the etiological and social complexity of ECC, supporting more comprehensive and family-centered interventions.26,29 The participation of physicians, dentists, nutritionists, nurses, and social workers ensures the management of both the biological factors and the social determinants of the condition. Each of these professionals performs specific functions.26,30,31 Medical and nursing staff can perform early detection during well-child visits, apply fluoride varnish, and provide oral hygiene education, as well as refer patients to dental care when warning signs are identified. 29 On the other hand, dentists focus on clinical evaluation, preventive and corrective treatment, and technical guidance on brushing and fluoride use. In addition, nutritionists can play a key role in modifying cariogenic diets to reduce the consumption of fermentable sugars. For their part, social workers can intervene in conditions related to the family environment and barriers to access to services.30,32
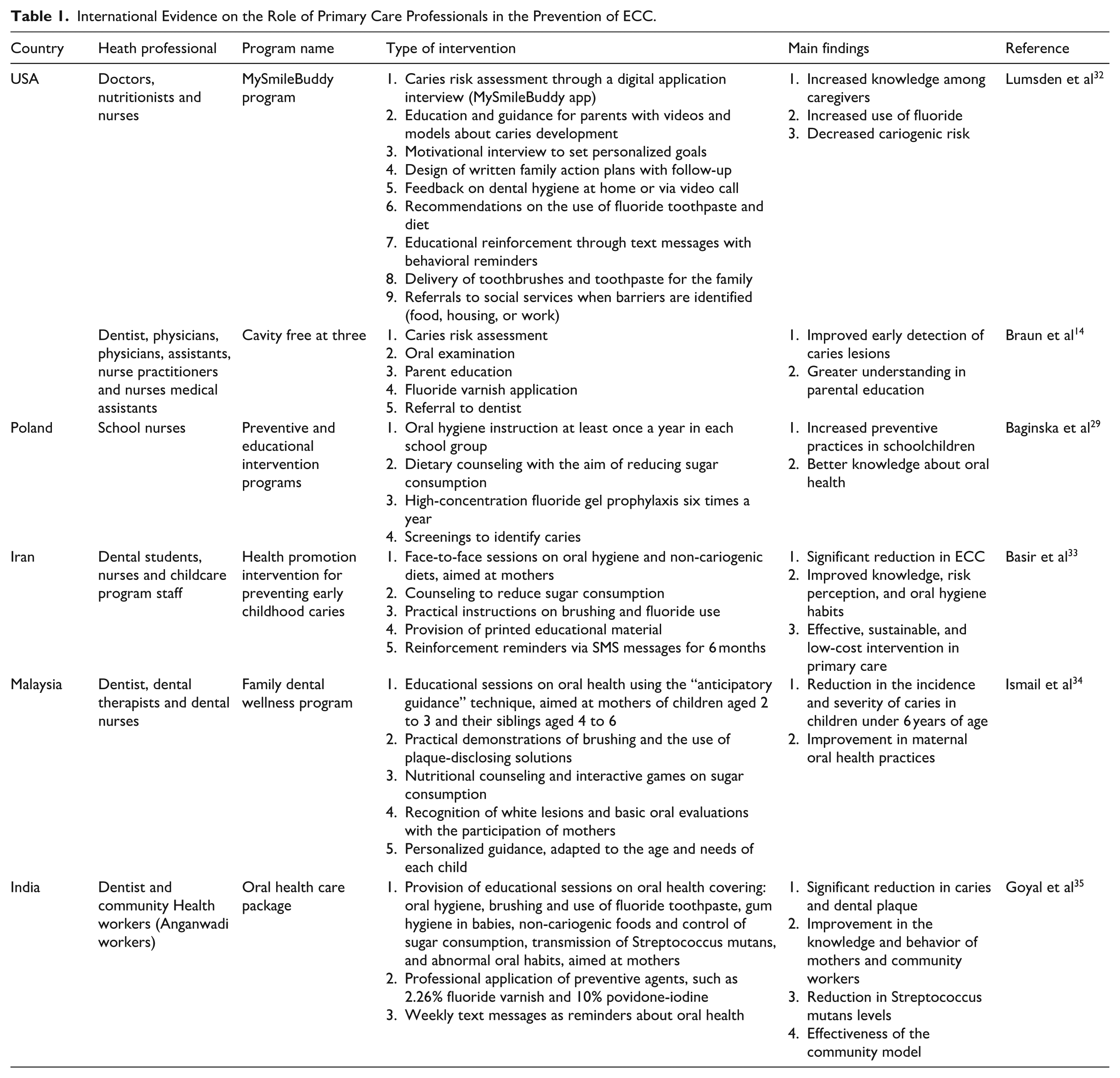
International evidence on the role of primary care professionals in preventing ECC is presented in Table 1. In the United States, 2 programs stand out for their interdisciplinary approach. In the first, “Cavity Free at Three,” the research group led by Braun et al brought together doctors, nurses, and medical assistants from health centers to perform cariogenic risk assessment, basic oral examinations, preventive education for parents, fluoride varnish application, and referrals to dental care, achieving early identification of caries in children with 4 or more applications before the age of 3 and greater understanding in parental education. 14 In parallel, the “MySmileBuddy” program incorporated nutritionists, doctors, and nurses through a digital intervention based on structured interviews in a mobile application, combined with educational videos, personalized goals, motivational sessions, and text message reminders. This model increased caregivers’ knowledge promoted the use of fluoride and helped reduce the risk of caries in the participants’ families. 32 On the other hand, in Poland, the study by Baginska et al evaluated school nurses who were assigned to provide oral hygiene education, dietary counseling to reduce sugar consumption, and supervised fluoride prophylaxis. screening for the identification of dental caries, showing that training and collaboration with dentists increases the effectiveness of preventive interventions aimed at children and adolescents. 29 In Iran, Basir et al describe a “health promotion intervention to prevent early childhood caries,” structured according to Nutbeam’s 4-level model. This intervention was implemented in health centers, where health personnel offered group sessions to mothers on oral hygiene and nutrition, increasing risk awareness, health literacy, and reducing the frequency of ECC. 33 The Family Dental Wellness Program, coordinated by dentists, therapists, and dental nurses in Malaysia, developed the anticipatory guidance technique, implementing various practical demoatinstrons, educational sessions, and nutritional counseling aimed at mothers of young children, significantly reducing the incidence and severity of caries and strengthening maternal oral hygiene practices. 34 Finally, in India, through the community model within the framework of the Integrated Child Development Scheme, Goyal et al implemented training for community workers (Anganwadi workers) to provide oral health education to mothers and children aged 1 to 6 years, showing an improvement in maternal knowledge and behavior and a projected decrease in the prevalence of caries, supporting the role of community public health. 35
International Evidence on the Role of Primary Care Professionals in the Prevention of ECC.
Continuous training is an essential tool to ensure effective interdisciplinary collaboration. This training for health personnel should be updated, systematic, and aimed at strengthening skills related to the prevention and detection of ECC. It is important to recognize that it is not enough for dental personnel to have a thorough knowledge of the clinical field; it is essential that general practitioners, nutritionists, nurses, and social workers are trained in the fundamental principles of children’s oral health, including the early signs of ECC, its multifactorial etiology, the importance of proper brushing techniques, and the use of fluoride according to each particular case. In addition, this training should include the development of effective, family-centered communication skills, integrating methodologies such as Motivational Interviewing, which has proven to be highly effective in achieving sustainable behavior change. This training tool will not only improve oral health education but also build trust with caregivers, promoting their active role in preventive actions.26,32
An interesting component of ongoing training is collaborative and interprofessional work. Simultaneous training in various shared learning spaces promotes understanding and awareness of the importance of each professional role, strengthens coordination in care, and reduces segmentation in the management of children and their family environment. 26 International studies on the integration of oral health into primary care sample successful results in which structured training protocols are implemented to raise awareness among professionals to identify oral risks from their respective disciplines and promote timely interventions, integrating timely referral to the dental area when warning signs are identified.26,32 Furthermore, this training should always be linked to evaluation and continuous feedback mechanisms, so that the impact of learning on community and clinical practice can be assessed and training content can be updated in line with advances in scientific knowledge and local epidemiological requirements. In this way, we could ensure an up to date, sensitized, and committed health team with a truly interdisciplinary approach that recognizes the prevention of ECC as one of the main priorities in primary care. 26
This model in primary care is supported by international experience. The systematic review by Christian et al 26 analyzed 49 studies from different countries and found that strategies characterized by interprofessional training, adjustments to health policies, and standardized risk analysis tools significantly improve referral processes by increasing preventive treatments and, therefore, reducing the prevalence of caries in children. The MySmileBuddy program developed in the United States is a notable prototype of this type of approach, which incorporates digital technology, motivational interviewing, and the active collaboration of various health professionals. These professionals, trained to accompany families at risk, not only provide information and management, but also set behavioral goals and personalized action plans adapted to the cultural and social context of each family environment. Preliminary findings from this model show an increase in caregivers’ knowledge, greater adherence to fluoride use, and a decrease in childhood caries risk in the most vulnerable populations. 32
Therefore, the first level of care is a strategic platform that allows risk factors to be identified from an early age and also operates as a system for coordinating clinical, educational, and community actions. Its optimal functioning requires staff training, the establishment of standardized protocols, and the promotion of intersectoral collaboration, fostering timely and sustained intervention in the prevention of ECC.
There are structural and operational barriers that effectively limit the various interdisciplinary preventive interventions aimed at children’s oral health. Among the most significant obstacles is the insufficient continuing education of non-dental health personnel, which prevents the proper implementation of techniques for promoting and early detection of DMFT. 29 Various studies have shown that although doctors, nurses, nutritionists, and community workers play a fundamental role in the prevention of oral diseases, the lack of training in the field of dentistry and poor interprofessional collaboration reduce the effectiveness of programs implemented at the primary care level. 14 In addition, the scarcity of human and material resources, together with the excessive workload of nursing and medical staff, makes it difficult to sustain preventive actions, particularly in rural areas and vulnerable communities. 32 In turn, limited coordination between dental and general medical services hinders early referral and regular follow-up of patients, while structural and socioeconomic inequalities deepen the gaps in access to oral care.33,34 Taking together, these limitations highlight the urgent need to promote interprofessional skills, optimize the availability of resources in primary care centers, and promote continuing education on oral health through collaborative models that incorporate dentists, physicians, nurses, therapists, and community agents within a structured and sustainable preventive network.
Motivational Interviewing in Pediatric Dentistry: An Essential Tool
Motivational interviewing is a person-centered communication tool that seeks to bring about behavioral change for improvement, in this case oral health.36 -39 This communication technique has proven highly beneficial in the field of health, seeking to strengthen commitment and motivation to achieve a goal, while always respecting the autonomy of the caregivers. Pediatric dentistry has implemented this tool to guide parents and caregivers in promoting the adoption of preventive oral measures and practices to prevent ECC.32,38
The 4 principles on which motivational interviewing is based are: resisting the urge to correct, knowing and understanding the person’s motivations, listening with empathy, and empowering the patient or caregiver.6,36 The principle of resisting the urge to correct consists of getting the person to discover the reasons for change on their own. During this intervention, the person is encouraged to explore their internal motives and reasons for change. On the other hand, listening with empathy involves prioritizing active listening in order to understand and comprehend the person’s various perspectives. Finally, empowering the person is a principle that promotes and encourages oral health care while considering the person’s autonomy.37,38
This approach has been found to be quite effective, particularly in vulnerable populations characterized by cultural and structural barriers that hinder adherence to healthy practices. The implementation of motivational interviewing is organized into 4 phases: connection, focus, evocation, and planning. 37 During the bonding phase, a relationship of trust and harmony is developed between parents or caregivers and the dentist. At this stage, it is essential that the professional pays genuine attention to their concerns and values their qualities and efforts without expressing opinions or judgments, to generate a connection and develop a bond of trust.36 -38 In the focus phase, the professional guides the caregiver in recognizing and defining the priority objectives for change in oral care. To improve understanding in this phase, it is essential to use visual tools that can be presented to caregivers, explaining in detail how to implement the recommendations for the oral care of the children in their care. An interesting example is the use of a bubble diagram that samples various topics, including sugar consumption control, regular visits to the dentist, tooth brushing with fluoride toothpaste, and caries prevention during pregnancy and breastfeeding.36 -38 On the other hand, in the evocation phase, the internal motivations for caregivers to adopt new habits are analyzed, reiterating their internal commitment. At this stage, the aim is to identify their own reasons for change, always respecting their autonomy. 36 Finally, in the planning phase, a clear, specific, measurable, and achievable plan is established, tailored to the actual conditions of the family environment based on their own motivations and goals. Future follow-up appointments are also agreed upon to evaluate progress and provide feedback on strategies if necessary.36,38,39
Various international studies have demonstrated the implementation of motivational interviewing as a patient-centered educational strategy aimed at promoting sustainable changes in behaviors associated with oral health. Recently, in a systematic review and meta-analysis, Manek et al analyzed 6 studies involving 2663 participants under the age of 6 and determined that motivational interviewing leads to a significant decrease in the incidence of new cavities compared to traditional dental education, with an average reduction of 3.64 (−5.77, −1.51) in favor of motivational interviewing after sensitivity analysis. This comprehensive study, which considered trials conducted in Brazil, Australia, Canada, and the United States, demonstrated the benefits in terms of changes in habits, behavior, and maternal knowledge; however, it emphasized the relevance of standardizing protocols and extending follow-up. 40 Complementarily, in a randomized clinical trial in an indigenous American population with 579 mother-child pairs, Batliner et al implemented 4 sessions of motivational interviewing combined with community services versus traditional services. Although there was a significant improvement in maternal understanding of oral health, there were no differences in the incidence of caries or oral hygiene practices after 3 years of follow-up. We could therefore suggest that the exclusive use of motivational interviewing does not have a sufficient impact in highly socially vulnerable environments. 41 On the other hand, in a pediatric hospital setting, Falahinia et al conducted a quasi-experimental study with mothers of children under 6 years of age diagnosed with leukemia. They found that motivational interviewing significantly improved the dental plaque index of infants, as well as the mothers’ attitudes, knowledge, motivation, and practices associated with oral health. This study highlights the potential of this motivational intervention even in high-risk clinical populations, as a more effective educational tool than conventional instruction based on informational brochures. 42 As an innovative proposal for the digital implementation of motivational interviewing, the MySmileBuddy program was proposed by Lumsden et al as a motivational interviewing-guided family educational intervention model. It was the protocol for a randomized clinical trial conducted at Columbia University to analyze the effectiveness of this tool in reducing the progression of DMFT in at-risk children aged 24 to 71 months. This program is based on training community health workers to use a digital application that includes risk assessment, motivational counseling, goal setting, and follow-up via text messages, with the aim of optimizing fluoride brushing and promoting non-cariogenic diets. It is important to note that this study is a study protocol and not a report of findings, making it impossible to draw definitive conclusions about its effectiveness. 32 Taken together, these studies show that motivational interviewing is a promising strategy for promoting oral health behaviors when implemented by trained professionals; however, they also highlight the need to define standardized protocols, determine the appropriate timing of intervention, and consider the patient’s social environment.
In addition to the classic interview, proposals are suggested to incorporate some elements of health literacy, shared intercultural communication, and an approach based on social determinants. The combination of the motivational interview with complementary strategies such as structured counseling, health coaching, or home visits has been shown to increase the impact in marginalized communities. 26
Integrating motivational interviewing into primary care services will allow for better communication between families and health personnel, as well as promoting parental empowerment, generating greater adherence to preventive programs, and encouraging a personalized care model, which are fundamental for reducing inequalities in children’s oral health.
The barriers to implementing motivational interviewing in primary care are diverse and highlight both structural limitations in the healthcare system and factors related to staff training. First, limited consultation time tends to be one of the main obstacles, as healthcare demands and the burden of patient care make it difficult to devote additional time to establishing a reflective and empathetic dialog with caregivers. Second, the lack of adequate training in patient communication techniques, as most primary care professionals do not receive formal training in motivational interviewing during their academic training. Third, the frequent turnover of health personnel is a significant barrier, as it interrupts follow-up and hinders the consolidation of communication skills among interdisciplinary groups. In addition, there have been institutional and logistical limitations, such as a lack of specialized human resources, a lack of administrative support to integrate behavioral strategies, and a lack of digital support tools adapted to the primary care context. 32
Strategic Pillars for an Interdisciplinary Preventive Model for ECC
Comprehensive management of ECC from the first level of care represents a promising opportunity to transform children’s oral health systems. 26 Future lines of action need to be based on 5 strategic pillars: systemic integration of oral health into primary care, consolidation of interdisciplinary training, integration of digital technologies, cultural adaptation of interventions, and continuous evaluation of community impact.
First, it is essential to institutionalize oral health as a core component of primary care, which will allow its role in overall health to be recognized. 43 Regulatory frameworks need to be established that include ECC prevention as a key indicator for monitoring child development. This integration will secure dedicated funding, standardize protocols, and commit health professionals to engage and train in these objectives.26,43
Second, it is a priority to establish a structured, interdisciplinary model of continuing education that trains primary care personnel in the basic principles of pediatric oral health, diagnosis of early signs, family-centered communication, and effective strategies such as motivational interviewing.36 -38 This training promotes a collaborative, child-centered approach, integrating not only dentists but also nurses, general practitioners, nutritionists, and social workers.36 -38
Third, the integration of digital technologies creates opportunities to promote and strengthen the prevention of ECC. Educational mobile applications, automated text messages, interactive platforms for caries risk analysis (such as Cariogram), and community electronic records are some of the tools that provide continuous support to families, strengthening the follow-up of preventive programs.44,45 Additionally, to achieve adequate staff training and dental follow-up in areas with limited access, telehealth systems could be considered. 45
A fundamental pillar for the functioning of the various proposals by the primary care level is the cultural adaptation of interventions. The success of different programs such as MySmileBuddy depends largely on their adaptation to the sociocultural characteristics of the communities. Because of this, it is essential that the design and implementation of future strategies and interventions be considered in accordance with health literacy levels, access barriers, local beliefs, and nutritional practices.32,46
Finally, the evolution and improvement of preventive interventions depend on continuous evaluation of their impact on the community. This calls for longitudinal studies that evaluate various relevant parameters, including reduction in the prevalence of ECC, adherence to oral hygiene measures, changes in parental behavior, and the monetary benefits associated with the reduction in restorative treatments. It is also extremely important to strengthen child oral health information systems, ensuring follow-up and continuous feedback on the interventions implemented.47,48
These 5 strategic areas aim to consolidate a robust, innovative, interdisciplinary, culturally adapted, and evidence-based primary care model capable of transforming the child oral health paradigm toward an equitable and preventive approach (Figure 1).

Strategic axes for a comprehensive approach to early childhood caries (ECC) at the primary care level. The strategy is based on systemic integration, interdisciplinary training, the use of digital technologies, cultural adaptation of interventions, and continuous evaluation of the impact on the community.
Conclusion
Globally, ECC continues to represent a public health problem of considerable prevalence, especially among the most vulnerable sectors. Its effective management requires moving beyond the therapeutic model and integrating preventive strategies from the early stages of life. The first level of care represents a strategic platform for implementing early, community-based, and sustainable actions and interventions, with the participation of families and interdisciplinary health teams.
A preventive approach should not only consider the implementation of clinical techniques, but also the continuous training of health personnel in communication skills with families through motivational interviewing. Similarly, the integration of digital technologies and the adaptation of various interventions to the sociocultural context increases adherence to oral health recommendations and reduces the cariogenic risk in the population.
A true transformation of the paradigm of children’s oral health care requires integrated policies, interdisciplinary training, and innovative strategies that establish effective prevention from the earliest years of life. In this way, it will be possible to reduce the prevalence of DMFT and ensure an adequate quality of life for future generations.
Footnotes
Abbreviations
ECC Early childhood caries
DMFT Decayed, Missing, and Filled Teeth
ORCID iDs
Author Contributions
Conceptualization: M.C.-G., M.M.-N., G.E.G.-A., M.A.A.-S., L.S.E.-V., A.H., and S.M.L.-M.
Formal analysis: M.C.-G., M.M.-N., G.E.G.-A., M.A.A.-S., L.S.E.-V., A.H., and S.M.L.-M.
Writing—original draft: M.C.-G., M.M.-N., G.E.G.-A., M.A.A.-S., L.S.E.-V., A.H., and S.M.L.-M.
Writing—review & editing: M.A.A.-S., A.H., and S.M.L.-M.
Supervision: A.H. and S.M.L.-M.
Approval of final manuscript: All authors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting this study’s findings are available from the corresponding author upon reasonable request.