
Abstract
Health insurance coverage is essential to improving preventative health services and decreasing financial burdens for older immigrants; however, disparities remain among different insurance kinds. This study analyzes the influence of private, public, and uninsured coverage on healthcare access and financial vulnerability among elderly immigrants in the United States, a population disproportionately impacted by socioeconomic and administrative obstacles. This cross-sectional study used data from the National Health Interview Survey (NHIS) covering 2020 to 2023 sourced from IPUMS, focusing on foreign-born persons aged 60 years and older. Weighted logistic regression models and propensity score adjustments were used to assess the associations between insurance type (private, Medicare, Medicaid, or uninsured) and 3 outcomes: access to regular care, financial strain, and unmet need due to cost. Analyses addressed age, sex, education, and economic status as confounding through using survey weights and complex design alterations. Results indicate that people with private insurance had significantly higher chances of having an ongoing source of care (OR = 1.54, 95% CI = 0.98-2.42) and decreased odds of having unmet healthcare demands (OR = 0.59, 95% CI = 0.39-0.90) compared to the uninsured population. Medicare coverage had a positive association with regular medical treatment (OR = 2.21, 95% CI = 1.34-3.64). No significant correlations have been identified between insurance type and financial strain. Gender and age variations persisted, with women showing somewhat reduced odds of receiving regular care. The findings demonstrate that health insurance coverage improves access to preventive care however does not eliminate financial stress among senior immigrants. Policy efforts must enhance fair coverage, address obstacles to Medicaid and Medicare access, and integrate culturally appropriate care for aging immigrant populations.
Keywords
Introduction
Health service scholars, whether they are professionals, administrators, educators, or policymakers, have a commitment to recognizing the different medical requirements as well as experiences of people and organizations in the design and delivery of health care services. This study demonstrates the use of a national database, the National Health Interview Survey (NHIS) in the USA, to identify unique health insurance coverage and health utilization of services patterns among ethnic groups in the USA.
Health insurance significantly impacts immigrants’ access to essential healthcare services and their ability to manage economic burdens in the United States.1,2,3 Older immigrants face unique problems, such language barriers, cultural inequalities, and inadequate understanding of the U.S. healthcare system that increase health inequalities and contribute to significant financial challenges. 4 Considering the increasing number of the aging population in the U.S., it is crucial to evaluate the influence of health insurance coverage on this demographic to develop policies that improve equality in health care and improved public health. Thorough U.S. studies suggests that health insurance improves access and mitigates inequalities in preventive services. Medicaid enhancements for children diminished unmet healthcare requirements, 5 however the Affordable Care Act’s coverage for dependents clause improved availability for young adults.6,7 Subsequently, results from the Oregon Health Insurance Study confirm that joining Medicaid resulted in increased medical consumption, mostly through enhanced emergency room visits. 8
Previous research show that immigrants are somewhat less likely to have health coverage compared to native-born individuals, resulting in decreased access to healthcare services, especially preventive care, and a higher incidence of acute health problems and financial strain.9,10 The literature highlighted the importance of culturally appropriate interventions that reduce these differences, showing that improved healthcare access may significantly enhance the quality of life for immigrant communities. 11
This study attempts to address an important research gap by addressing the question: “To what extent does health insurance coverage promote access to preventive healthcare and alleviate financial hardships amongst elderly immigrants in the U.S.?” The study analyzes the connection between health insurance coverage, preventative medication, and economic outcomes, primarily the objective of improving support for immigrant groups in achieving optimal medical results.
This study complements an important body of U.S. studies that has examined the causal impacts of health insurance on access to healthcare and financial stability. Prior studies, including the RAND Health Insurance Experiment, demonstrated how cost-sharing influences utilization and financial risk. 12 Trials with Medicaid expansion in Oregon have shown significant rises in treatment utilization, yet the consequences on health outcomes remained inconsistent.8,13 Research on public insurance expansion for children 14 and for young adults under the Affordable healthcare Act 6 demonstrated significant enhancements in access to preventative care. However, data addressing elderly immigrants, a minority disadvantaged based on age and citizenship status, remains limited. This study overcomes the gap by emphasizing on elder immigrants’ access to preventive healthcare and financial stability. Despite national gains in insurance coverage, racial, and ethnic disparities in preventive screenings and healthcare access continue to persist. 15
Despite the widely recognized significance of health insurance for promoting healthcare access, there’s a notable shortage of research that specifically examines the impact of different insurance coverage types on the health and financial security of older immigrants in the U.S. This study seeks to fill this significant gap through using data from the National Health Interview Survey (NHIS) from 2020 to 2023, examining the associations between health insurance status, access to preventive medical care, and the economic burden on immigrant communities. This study’s findings can inform policy decisions that promote health equality for immigrants, perhaps that lead to broader social benefits.16,17
Background and Literature Review
Health insurance coverage is essential for enabling healthcare access, especially for senior immigrants in the United States. In the present scenario, “health insurance coverage” indicates the range and features of financial security provided to individuals for medical expenses. “Healthcare access” refers to the capacity of individuals to get required health services, which is essential for maintaining or improving health. “Preventive healthcare” includes medical services intended to avoid illnesses before to the development of significant symptoms, which is vital for elderly populations who are more prone to chronic diseases.
Insurance and Healthcare Access for Immigrants
Elderly immigrants in the United States, particularly those of South Asian descent, frequently encounter significant obstacles in obtaining sufficient health insurance coverage. Barriers such as not sufficient English proficiency, which hampers interaction with healthcare providers and hinders navigating of the complex U.S. healthcare system. In addition, their commonly limited knowledge of the system’s operational mechanisms presents a further obstacle. 11 Socioeconomic problems like lower income levels and unstable employment, accelerate these barriers, limiting these groups’ ability to achieve, and maintain continuous coverage. 9
These factors collectively result in significant variations in the availability and standard of health insurance for older Asian immigrants. Therefore, many people within this group suffer delays getting medical care, which is vital to the prevention and control of chronic diseases. Such delays frequently end in decreased use of important preventative services, including regular checks and early disease screenings, which are crucial for the prompt detection and care of possibly fatal disorders. 18 The absence of suitable preventive care negatively impacts this group, leading to worse long-term health outcomes, particularly increased rates of complications from chronic illnesses and a rise in mortality. 4
Furthermore, the standard of healthcare given to these groups can often be compromised. Insufficient insurance coverage limits access to better medical professionals and specialized services, raising the possibility that elderly immigrants will get care from inferior providers or forego vital medical care entirely. 10 This inadequate care system negatively impacts both physical and mental health, as the stress associated with handling these difficulties can result in increased anxiety and feelings of helplessness among the elderly. 19
A combination of linguistic, structural, and economic barriers significantly limits access to adequate health insurance and excellent medical care for elderly South Asian immigrants, consequently perpetuating disparities in health and affecting their overall health outcomes. These observations emphasize the urgent need for customized actions to tackle specific barriers to increase healthcare accessibility and insurance coverage for this poor population. 4
Economic Barriers and Delayed Healthcare in Elderly Immigrant Adults
Economic challenges offer an important barrier to healthcare access for older immigrant people, with many in this demographic delaying or completely abandoning essential medical care due to financial limitations. This issue is particularly acute among immigrants who frequently experience increased economic vulnerability and lack a safety net of savings or familial support to reduce medical expenses.5,19 The financial challenges are made worse by the increasing price of medical treatment in the United States, that can be overly demanding, particularly for those lacking finish health insurance coverage.
The restricted access to affordable insurance options worsens the problem. Many elderly immigrants particularly those without valid permanent residency are excluded from government insurance programs such as Medicare and Medicaid, increasing their economic vulnerability and delayed access to care. 17 This demographic frequently encounters the challenge of choosing vital healthcare over basic needs like food and housing, leading to delayed medical attention and disregard of chronic illnesses.
Delays in getting medical care can lead to significant repercussions turning manageable problems into serious and expensive health emergencies. Conditions such as hypertension and diabetes, if not regularly monitored and regulated, it may result in serious complications requiring intense and expensive treatment.1,18,20 Moreover, psychological strain linked to economic hardship and lack of access to health care may negatively impact mental health, resulting to a reduced quality of life and possibly aggravate pre-existing medical conditions. 10
The interplay of financial stresses, insufficient insurance, and elevated healthcare costs creates an ongoing pattern of health neglect, leading to insufficient medical care and worsened health outcomes among elderly immigrants. This cycle affects both the health and well-being of those impacted and puts more pressure on the healthcare system via increased emergency care use and increased treatment costs for serious illnesses.4,18 Consequently, reducing the economic barriers to healthcare faced by elderly immigrants is crucial to improving their health outcomes and ensuring accessibility for prompt and suitable medical care. 21
Exceptional Challenges Experienced by Elderly Immigrants
Elderly immigrants have many challenges that significantly impact their access to health and financial well-being in the United States. Citizenship status and ability to speak English are among the most important variables. Limited English proficiency hampers efficient interaction between healthcare personnel and immigrant patients, often leading to misconceptions about symptoms, options for treatment, and prescription directives. The status of non-citizens worsens these issues, as they frequently encounter difficulties in obtaining health insurance programs, particularly Medicaid, due to criteria limitations. These obstacles result in an important percentage of the population being uninsured or underinsured, consequently limiting their access to essential healthcare procedures.17,22
Cultural stigma around the use of public healthcare facilities could discourage elderly Asian immigrants form seeking essential medical care. This stigma often arises from concerns over discrimination or negative assessments from others within their community or from medical professionals lacking cultural awareness. Concerns about potential immigration consequences, particularly impacts on immigration status or anticipation of deportation, greatly impact the situation. These worries are made worse by strict immigration rules, preventing individuals from accessing needed healthcare services, notwithstanding their vital significance for health.21,23
Furthermore, a shortage of culturally suitable medical centers and an absence of healthcare personnel who understand the different cultural and economic status contexts of Asian immigrants could exacerbate these difficulties. Insensitivity to cultural understanding in medical settings negatively affects the quality of care and discourages elderly immigrants from coming for future appointments or following to recommended treatment. 10
The interaction of these factors leads in a hazardous scenario whereby older Asian immigrants frequently face delayed diagnosis and treatment, resulting in poor health outcomes and increased mortality rates. Fighting these challenges requires an extensive plan involving changes to policies that increase access to linguistically and culturally suitable healthcare services, enhanced training for medical personnel in cultural competence, and reforms that would boost health insurance and health accessibility for non-citizens.4,10,18
Preventive Healthcare Utilization and Its Importance
Continuous preventive healthcare is crucial to preventing chronic diseases while improving the quality of life in elderly populations, particularly elderly immigrants who are at a higher risk for chronic ailments.4,18,24 Many older individuals’ Asian immigrants, however, face obstacles in obtaining regular medical care and preventative services due to geographical in nature financial, and language limitations.9,23
Cultural inequalities and fear of discrimination hinder the pursuit of preventive treatment.19,21 Adopting culturally appropriate healthcare policies and outreach to the community can improve access to vital preventive services for this at-risk population.
Although elderly immigrants in the U.S. recognize the importance of preventive healthcare; however, they face economic and structural challenges, like inadequate health insurance coverage, out of pocket cost which limits their ability to get to these services.15,24,25 The present study has not thoroughly examined the effects of various kinds of health insurance coverage upon the use of preventative services and financial stability within these populations.
This gap informs the study’s main study question: How does health insurance coverage influence access to preventative healthcare and financial outcomes for elderly immigrants in the U.S.? Addressing the question could help the identification of specific measures that improve health and financial stability for this at-risk population.
This study employs National Health Interview Survey (NHIS) data from 2020 to 2023 to investigate the impact of health insurance on access to healthcare for elderly immigrants. Logistic regression will be used to look at the data, altering for traits such as age, ethnicity, and socioeconomic position, to clarify the impact of insurance coverage.
This study is fundamentally based in the Social Determinants of Health Theory. The theory argues that health outcomes are greatly influenced through numerous environmental, social, and economic variables. It argues that systemic inequalities, such as inequalities in getting healthcare and economic resources, significantly impact community and personal health outcomes. This perspective is crucial for understanding the challenges faced by older immigrants, particularly with regard to the effect of their social life on their health insurance coverage as well as access to healthcare services. 9 Research findings support this theoretical approach, showing that elderly immigrants frequently face reduced access to wellness services and increased economic pressures due to insufficient health insurance coverage.
This research aims to fill the critical divide concerning the influence of health insurance inequalities on wellness practices and economic outcomes among elderly immigrants through the integration of these concepts and empirical findings. The objective is to share improvements to policies and efforts that strengthen equality in health care, ensuring that older immigrants get adequate assistance for a better quality of life.
Data and Methods
A retrospective study used pooled data from the 2020 to 2023 National Health Interview Survey (NHIS) sourced from IPUMS to examine the use of health services and immigrant status among individuals aged 60 and older. This study defined “older adults” as individuals aged 60 years and older, which is consistent with standards used for gerontological and public health research.10,16,24 The investigation focuses on 2 primary immigrant groups: Asian immigrants and Hispanic immigrants. Asian immigrants were categorized by reported racial categories, and Hispanic immigrants were classified based on self-reported Hispanic ethnicity. A binary “immigrant” variable was developed to combine these groupings into a single categorization. Individuals were regarded as immigrants if they fell into the part of the Asian or Hispanic demographics. Asian immigrants were identified specifically when racenew equals 1, and Hispanic immigrants were identified where hispyn equals 1. An aggregate immigrant variable was established, giving a value of 1 (immigrant) for those who satisfied either criterion, or 0 (non-immigrant) to those who did not. The NHIS lacked accurate national-origin identifiers for all Asian sub-groups; still, initial division revealed slight differences in utilization between South Asian and East Asian respondents. The observed differences failed to reach statistical significance (P > .10), consequently they were not modeled separately in this analysis, but have been identified as a possible area for future research. 4 Inclusion criteria included respondents aged 60 years and over who were foreign-born and gave complete responses for insurance coverage, healthcare access, and financial metrics. The exclusion criteria included U.S.-born individuals, respondents under 60 years of age, and cases with incomplete data on key covariates, like education, gender, or income (fewer than 3% of total observations).
Many possible confounding variables, such as access to healthcare facilities and individual health situation, could influence healthcare utilization but are missing within the National Health Interview Survey dataset. Similar research using experimental or quasi-experimental approaches recognizes similar limitations, showing that unmet health requirements could bias the relationships with coverage and access.26,27 To address this, control variables for age, education, income, and proficiency in English language are included and Propensity Score Matching further reduces observable bias.
The findings showed that from a total of 147 430 pooled NHIS respondents (2020-2023), 48 890 were aged 60+, and 5611 foreign-born adults were included in the analytic sample after exclusions. Cross-tabulations further supported the classification, showing that all people designated as Asian immigrants or Hispanic immigrants were properly integrated into the aggregate immigrant group. This approach ensures a precise depiction of the immigrant population in the study and enables an in-depth investigation of healthcare access, economic strain, and associated health consequences among elderly immigrants in the United States. A flow diagram (Appendix 2) of analytic sample selection from NHIS data, 2020 to 2023.The diagram shows inclusion and exclusion steps leading to the final weighted analytic sample (n = 48 368), with subsequent propensity score matching for immigrant and non-immigrant older adults. The preliminary pooled NHIS sample included roughly 60 000 cases year from 2020 to 2023, totaling to over 240 000 potential respondents. After the application of the criteria for age (≥60) and immigration status, 48 890 viable cases were kept. Observations with missing answers about insurance status or important control variables (less than 3%) have been eliminated to preserve data integrity. The variation in sample size across tables reflects the use of complete-case analysis for each outcome variable. The variables “Age” and “Education” showed a slightly greater rate of missing data (about 9%), leading in a decreased analytic sample in descriptive models, while logistic regressions were limited to 5611 valid observations across all predictors. To improve transparency, a flow diagram (Appendix 2) was added to illustrate the inclusion and exclusion procedures, including total sample derivation, missing data oversight, and the matching sequence.
This research adopts the Behavioral Model of Health Service Utilization28,29 to investigate healthcare access and utilization among elderly immigrants. The framework defines factors that influence as predisposing, enabling, and need factors. Predisposing factors include demographic and social attributes, like age, sex, education, which influence a person’s tendency to seek care. Enabling factors indicate the resources that both enable or impede access to healthcare, such family income, employment status, length of residence in the United States, and health insurance coverage. This paradigm investigates how these factors paired influence access to wellness services and the economic obstacles faced by elderly immigrants.
This study analyzes the effect of health insurance coverage and immigration-related features, particularly citizenship status and years of residence in the U.S., on access to preventive healthcare services and financial challenges faced by elderly immigrants. The dependent variables include engagement in preventive healthcare practices, which includes the existence of an established care provider, yearly exams, the type of health care facility utilized, financial constraints, and medical requirements that remain due to costs. Control variables include socioeconomic and demographic parameters such as age, gender, race, education, work position, and income, in along with linguistic ability and the usage of translation services to tackle obstacles in healthcare access and affordability.
Statistical Analysis
Descriptive statistics have been developed with survey weights that reflected the complex structure of the NHIS. Weighted logistic regression models were used to assess the connections between insurance coverage and healthcare outcomes. Propensity score matching (PSM) was used to reduce selection bias. Model diagnostics included pseudo-R2 values, variance inflation factors (VIF), and standardized mean differences (SMD) for assessing balance and multicollinearity.
Estimation Strategy for Analyzing Health Insurance Impact
This study makes use of logistic regression models to investigate the impact of insurance coverage on access to preventive healthcare and the financial strain associated with medical bills amongst elderly immigrants. The independent variables include various kinds of health insurance, namely private, Medicare, Medicaid, and uninsured status, for assessing their different impacts on healthcare utilization and financial difficulties. To reduce potential confounding variables, propensity score matching (PSM) or stratification is used to create comparison groups that are statistically equivalent based on characteristics such as age, income, and education, thereby reducing selection bias inherent to observational studies. 30 An interaction term between “immigrant” and every kind of insurance has been studied in a broader framework to determine if the effects of coverage varied by immigration status. The results showed a consistent trend toward significance for private insurance, indicating that the safeguarding impact of private coverage on economic hardship is greater for immigrants than for non-immigrants, in addition to the differential access patterns observed in national data. 16
Logistic Regression Models
To assess the impact of health insurance coverage on healthcare access and financial burden, the following logistic regression models were estimated:
Model 1: Access to Regular Care
The likelihood of having regular healthcare access is modeled as:

where P(Has Regular Care = 1) is the probability that an individual has a regular source of healthcare.
Model 2: Financial Burden
The probability of experiencing financial strain due to medical expenses is given by

where P(Financial Burden = 1) indicates the likelihood that an individual experiences financial difficulty paying medical costs.
Model 3: Unmet Need Due to Cost
The likelihood of reporting unmet healthcare needs due to cost is estimated as

where P(Unmet Need = 1) represents the probability of an individual reporting healthcare needs that were unmet due to cost barriers.
P (Y = 1): is the probability of the outcome occurring.
b, α, γ: are coefficients for each independent variable.
Independent variables include health insurance type (Private Insurance, Medicare, Medicaid, Uninsured), demographic factors (Age, Sex), and socioeconomic status (Education).
ϵ represents the error term. The regression models follow the Behavioral Model of Health 28 Service Utilization, with age, sex, and education contributing as predisposing characteristics, insurance coverage as the main enabling factor, and access and affordability indicators indicating actual need. This method enables the empirical analysis of how enabling resources reduce or increase structural barriers to healthcare for elderly immigrants.
Propensity Score Matching (PSM)
To minimize potential selection bias and ensure comparability between insured and uninsured groups, propensity scores were estimated using logistic regression

Here:
P(Treatment = 1) represents the probability of being insured (treatment group).
δ0 is the intercept, and δ1-δ3 are coefficients for covariates such as age, sex, and education.
Matching Methodology
Nearest neighbor matching was applied in this study with a (caliper = 0.05) to make sure balance between treated (insured) and control (uninsured) groups. Balance was measured using standardized mean differences (SMD) to confirm that all covariates achieved balance (SMD < 10%). Matching diagnostics confirmed adequate equivalence between the treatment group and control groups. The average standardized differences for variables before matching exceeded 20% for age and income, but decreased to below <5% post-matching, which is consistent with the quality standards. 30 Visual inspection confirmed common support, showing overlap over the whole range of propensity scores. Matching was carried out with replacement to minimize bias and variance. In this study, the classified treatment group as respondents holding any type of medical insurance (private, Medicare, or Medicaid), while the comparison group included people having no insurance coverage. The binary variables for “insured vs uninsured” was used in matching, while insurance subcategories were further investigated using stratified logistic models. Standardized mean differences (SMDs) were calculated before and after matching to ensure transparency and evaluate balance. Before matching, the average standardized mean difference (SMD) across covariates was 18.7%, which decreased to 4.6% after matching, demonstrating effective covariate balance per Rosenbaum and Rubin criteria. 30
The analysis also examines whether language proficiency modify the relationship between health insurance coverage and access to healthcare, emphasizing the effect of language barriers on healthcare disparities. The cross-sectional approach of the NHIS recognizes limitations in establishing causality. To improve robustness, advanced techniques like PSM and stratification stimulated quasi-experimental conditions, ensuring improving robustness. 31 Propensity scores are determined via logistic regression including covariates such as age, sex, and education. Nearest neighbor matching, using a caliper of 0.05, achieves covariate equilibrium validated through standardized mean variations (SMD) < 10% and acceptable variance ratios. This study followed the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) checklist for cross-sectional studies to ensure transparent and comprehensive reporting of methods and results. 21
Results
Descriptive Statistics
Table 1 provides descriptive statistics for the major variables examined in the study. The sample consist of on the data collected from the Health Interview Survey (NHIS), 2020 to 2023. Based on data from the National Health Interview Survey (NHIS), 2020 to 2023, Table 1 shows descriptive statistics for the main variables studied in this study. Analytic sample is based on 5611 individuals 60 years of age and older who have been born in the country other than United States. Higher educational attainment indicates tertiary or advanced degrees. The NHIS uses an established classification system for educational attainment, with codes 101 to 997 denoting years and higher values indicate postsecondary or advance degrees of schooling. The overall percentage across all insurance coverage categories is slightly higher than 100% (100.2%) because of minor rounding inaccuracies. The uninsured group wasn’t used as the reference group in regression models with the goal to prevent multicollinearity.
Weighted Descriptive Statistics of Study Variables (NHIS 2020-2023).
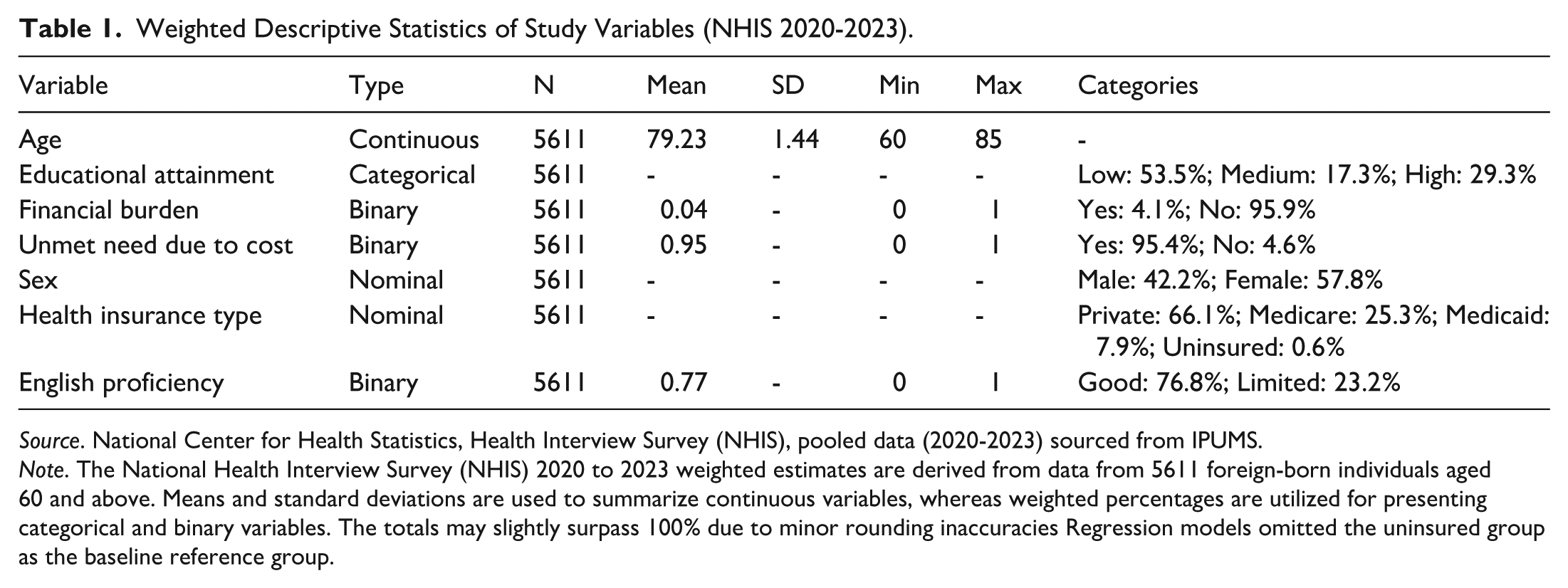
Source. National Center for Health Statistics, Health Interview Survey (NHIS), pooled data (2020-2023) sourced from IPUMS.
Note. The National Health Interview Survey (NHIS) 2020 to 2023 weighted estimates are derived from data from 5611 foreign-born individuals aged 60 and above. Means and standard deviations are used to summarize continuous variables, whereas weighted percentages are utilized for presenting categorical and binary variables. The totals may slightly surpass 100% due to minor rounding inaccuracies Regression models omitted the uninsured group as the baseline reference group.
Age and level of education are continuous variables that are evaluated for each respondent (n = 5611). Participants vary in age from 60 to 85 years old, with an average age of 79.23 years (SD = 1.44). According to respondents’ educational attainment, 29.3% have a high level of education, 17.3% have a medium level, and 53.5% have a low level.
Binary variables include English proficiency, financial burden, and unmet need due to cost. Approximately, 4.1% of respondents reported being unable to pay medical bills. A substantial number of older immigrants may face monetary barriers to accessing healthcare, as seen by the 95.4% of respondents who reported unmet healthcare needs attributed to cost. In terms of language, 23.2% showed limited fluency in English, whereas 76.8% reported excellent proficiency.
Nominal variables include Health Insurance Type and Sex. Men represented 42.2% of the respondents, while women made up 57.8%. Regarding health insurance coverage, only 0.6% immigrants are without insurance, whereas 66.1% had private insurance, 25.3% had coverage provided by Medicare, and 7.9% were covered by Medicaid. These descriptive characteristics illustrate the broad spectrum of healthcare and socioeconomic factors across older immigrants. Table 5 displays the gender distribution among respondents and policy holders, serving as a demographic proxy for household coverage roles. Appendix Tables 1 and 2 offer an in-depth evaluation of insurance coverage patterns by sex, highlighting inequalities among private, public, and uninsured categories for foreign- born individuals aged 60 and above.
Gender Distribution
Table 2 illustrates the gender distribution among participants and policyholders, serving as a substitute indicator of household insurance coverage trends among older immigrants. The sample includes 42.2% male and 57.8% female respondents. In the study of policyholder demographics determined by the gender of the respondent or their spouse/partner men represent a greater proportion of policyholders (64.0%) than women (36.0%). The gender inequality suggests that men are more likely to have primary insurance policies in immigrant households, reflecting broader patterns of gendered economic and career participation among older persons.
Respondent and Policyholder Sex Among Foreign-Born Adults ≥ 60 years.

Source. National Center for Health Statistics, Health Interview Survey (NHIS), pooled data (2020-2023) sourced from IPUMS.
Insurance Type by Sex
Table 3 demonstrates the distribution of insurance coverage categories between male and female respondents. Among men, 64.7% reported private insurance coverage, 73.2% owned Medicare, and 99.1% took part in Medicaid, whereas only 1.8% of male respondents were uninsured. In contrast, all women stated that they had private insurance, 24.7% had enrollment in Medicare, and 9.8% were covered by Medicaid, with a minor uninsured proportion of 0.8%. The information reveals that although private coverage is common among both genders, women are more likely to rely on private or mixed insurance, whereas males demonstrate marginally more involvement in public insurance programs like Medicare and Medicaid.
Insurance Coverage Type by Sex Among Foreign-Born Adults ≥ 60 years.

Source. National Center for Health Statistics, Health Interview Survey (NHIS), pooled data (2020-2023) sourced from IPUMS.
Cross-Tabulation by Sex
Table 4 cross-tabulates types of insurance coverage by sex to show proportional inequalities within each insurance category. Private insurance suggests a distribution of 41.3% male and 58.7% female, while Medicare and Medicaid coverage offer a more balanced representation, with 45.4% and 40.8% male, respectively. Uninsured responders are evenly split by gender (45.5% male; 54.6% female). The results reflect the trends reported in Table 4, suggesting that although women constitute a larger percentage of the insured demographic, men continue to be the main policyholders in multiple immigrant homes. The disparities in gendered coverage are likely caused by overlapping factors, such job background, spousal coverage eligibility, and language or occupational limitations that impact access to employer-based or public insurance programs.
Insurance Type by Sex (Weighted %).

Source. National Center for Health Statistics, Health Interview Survey (NHIS), pooled data (2020-2023) sourced from IPUMS.
Model Building
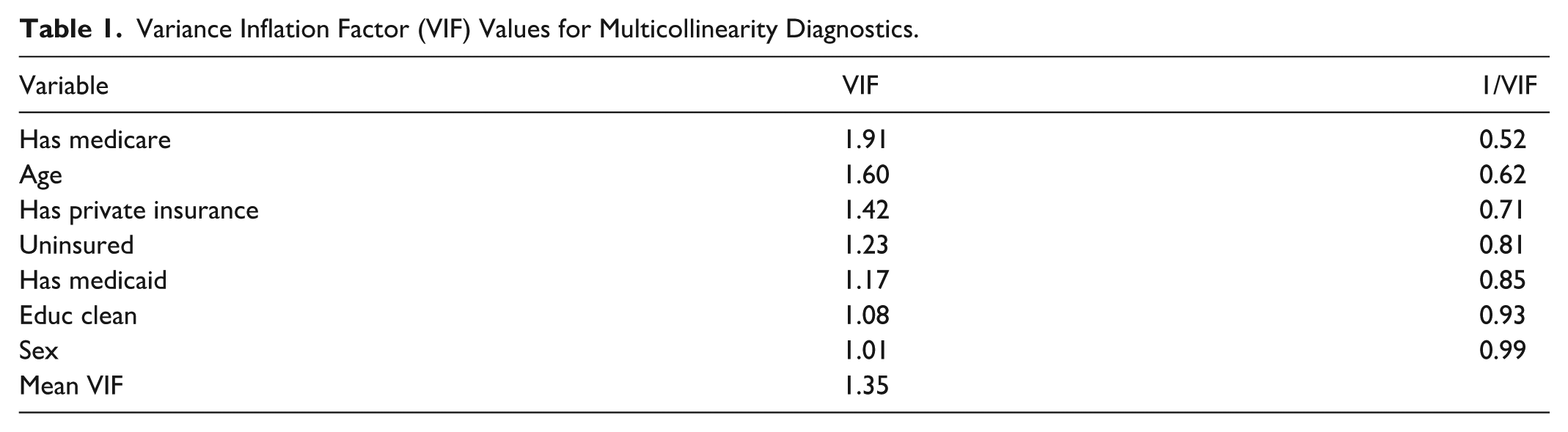
The study examined healthcare access and financial strain in persons aged 60 and above using logistic regression models. Three outcomes were analyzed: (1) consistent access to healthcare, (2) financial burden/strain, and (3) unmet healthcare demands related to cost. The primary predictors included subcategories of health insurance coverage (private insurance, Medicare, Medicaid, or uninsured), in along with socioeconomic and demographic factors including age, gender, and educational level. The effects of interaction and potential multicollinearity were assessed using the Variance Inflation Factor (VIF), giving a mean VIF of 1.35 (Appendix 1), which indicates the lack of significant multicollinearity among predictors.
Logistic Regression Models
Table 5 illustrates the results of 3 logistic regression models examining the associations between different predictors and the likelihood of (1) receiving regular care, (2) encountering financial hardship, and (3) expressing unmet healthcare needs attributable to cost. The dependent variables capture key indicators of healthcare access and financial burden among foreign-born adults aged 60 and older, a population often facing compounded economic and linguistic barriers to care. The coefficients indicate the log-odds of each the end, with standard errors provided in parentheses.
Survey-Weighted Logistic Regression Predicting Healthcare Access and Financial Outcomes.

Source. NHIS 2020 to 2023, survey-weighted estimates.
Note. Exponentiated coefficients (odds ratios) displayed; 95% confidence intervals in brackets. Reference group = uninsured; Model includes survey weights, strata, and PSU adjustments. Logistic regression models estimate the association between insurance coverage, socioeconomic, and demographic characteristics with 3 health-related outcomes among individuals aged 60 and older. The reference group for insurance type is Uninsured; for gender, Male; and for education, Lower educational attainment. Pseudo R2: .1389/.0117/.0988.
Significance levels: *P < .05; **P < .01; ***P < .001.
This study explores the impact of insurance coverage, demographic variables, and socioeconomic characteristics on healthcare outcomes in elderly individuals. Model 1 highlights inequalities in regular healthcare, wherein patients without insurance face considerable obstacles. Expanding on this, Model 2 analyzes financial obligations, with private insurance providing essential coverage. In the end, Model 3 shows that unmet health care needs continue to be present notwithstanding particular kinds of coverage, exposing systemic inadequacies.
Model 1: Has Regular Care
For foreign-born individuals aged 60 or older, insurance coverage plays an important role for creating a regular source of healthcare. Those with Medicare coverage were over twice as likely to report having a regular place of care compared to those without insurance (OR = 2.21, P < .01). Individuals with Medicaid coverage showed more than double the probability of having a regular care provider (OR = 2.27, P < .05), but those with private health insurance were around 1.5 times more likely to receive regular medical attention (OR = 1.54).
Whereas, lacking insurance significantly decreased the probability of maintaining regular access to healthcare (OR = 0.16, P < .001), highlighting the persistent coverage-related barriers faced by older immigrants inside the U.S. healthcare system. Demographic controls showed that female participants were less likely than the male respondents to receive regular care (OR = 0.70, P < .05), suggesting the possibility of gender disparities in healthcare utilization within older immigrant communities. Age and educational attainment demonstrated not a statistically significant relationship in this model. Model 1 demonstrates that access to insurance is the most important facilitating factor for regular healthcare utilization among older immigrants.
Model 2 Financial Burden
Model 2 analyzes factors affecting the probability of experiencing monetary hardship due to medical costs among immigrants aged 60 and above. Although health insurance coverage usually offers security, none of the coverage categories show statistically significant correlations with financial strain in this model. Individuals with private insurance (OR = 1.32) and Medicare (OR = 1.25) have significantly reduced odds of facing financial hardship compared to uninsured individuals; however, the confidence intervals include 1, indicating that the difference is insignificant. Medicaid coverage shows a modest but not statistically significant correlation (OR = 1.22).
Demographic variables such as age, sex, and education are not significantly associated with economic hardship, suggesting that their effects decrease after accounting for health insurance and other controls. The limited predictive capacity of this model (Pseudo R2 = .0117) indicates that financial strain among older immigrants has been influenced by other unidentified factors, like household wealth, remittance obligation, or underlying healthcare costs that insurance cannot fully reduce. 32
In findings, Model 2 suggests that insurance enrollment alone insufficiently protects older immigrants from economic pressures connected to healthcare, likely due to the limitations of inadequate coverage, co-payments, and administrative obstacles. The results illustrate a need for expanded affordability policies and culturally specific financial aid programs that adapt to the unique needs of older immigrant households.
Model 3: Unmet Need Due to Cost
Model 3 evaluated whether respondents delayed or neglected needed treatment due to financial constraints. The findings clearly show that insurance coverage significantly reduces unmet medical requirements among elderly immigrants. Compared to the uninsured, those with Medicare (OR = 0.53, P < .01) and private insurance (OR = 0.59, P < .05) had a significantly lower likelihood of avoiding care due to financial constraints. In contrast, uninsured individuals showed nearly 5 times greater likelihood of reporting unmet needs (OR = 4.94, P < .001), emphasizing the significant obstacles to lacking safety net accessibility.
Among demographic characteristics, age exhibited an encouraging and marginally significant association (OR = 1.03, P < .05), indicating that older people in this cohort face more challenges in obtaining affordable care. Neither gender nor education demonstrated statistical significance. However, the direction effects suggest slightly reduced cost barriers among women. This model illustrates that regular coverage and affordability are critical for overcoming access barriers, particularly for immigrant elders who commonly rely on restrictive benefits or experience administrative challenges in maintaining eligibility.
Discussion and Conclusion
This study explored the effect of health insurance coverage, demographic factors, and socioeconomic characteristics on healthcare access and cost related to health care for elderly immigrants in the United States. Logistic regression models were used for analyzing data from the National Health Interview Survey (NHIS) conducted between 2020 and 2023, emphasizing 3 main outcomes: consistent healthcare access, economic difficulty, and unmet healthcare needs due to cost among foreign-born adults aged 60 and older. The results offer vital insights into the persistent disparities faced by elder immigrants and highlight the necessity of tailored policy responses.
Interpretation of Results
Health Insurance Coverage as the Determining Factor
Health insurance coverage emerged as an essential variable affecting healthcare in healthcare access, aligning with the Behavioral Model of Health Service Utilization.15,28 Private insurance consistently demonstrated the most positive effects increasing the likelihood of regular care, reducing financial burden, and substantially decreasing unmet healthcare needs. These results confirm earlier national evidence showing that insurance expansion under the Affordable Care Act enhanced utilization but left significant gaps for marginalized groups.12,18
These findings highlight the vital role of private insurance for promoting healthcare access and maintaining economic stability. On the other hand, the mixed or little impact of Medicare and Medicaid suggest potential limitations in the design and accessibility of public insurance programs for elderly immigrants. 16 However, uninsured faced significant disadvantages, including substantially decreased likelihood of getting regular care and significantly elevated chances for unmet healthcare needs. These disparities highlight the need to improve and expand health care coverage, particularly among those populations who are at-risk. Comparable findings have been acknowledged in Oregon’s Medicaid expansion, where increased healthcare use did not explain into parallel gains in financial protection. 8
The Role of Age and Education
Age influences healthcare outcomes in 2 separate ways. Older individuals showed a lower probability of having regular access to care, suggesting barriers to consistent healthcare use among this cohort. However, they indicated slightly decreased financial pressures, which may indicate deferred or foregone care rather than improved economic relief. Interestingly, higher educational attainment associated with an increase in unmet healthcare demands, suggesting the structural barriers that even highly qualified persons face while obtaining the healthcare system. This aligns with findings that highly educated immigrants still experience bureaucratic and linguistic hurdles that limit care access. 32 This surprising finding highlights the complex nature of healthcare access and requires further research.
Gender-Based Disparities
Gender differences have been observed in healthcare access and unmet need. Women were less likely to report regular use of healthcare than men but faced lower probabilities of unmet healthcare requirements. The findings show that while women might face obstacles obtaining ongoing medical treatment, they can also use methods of coping or utilize community support structures that mitigate the consequences of unfulfilled needs. The gendered patterns of healthcare utilization highlight the importance of incorporating These gendered dynamics may reflect cultural expectations, caregiving roles, or differing health-seeking behaviors among immigrant men and women. 10 The study’s measure for prevention healthcare access to regular care reflects the general relationship with medical providers rather than the specific use of preventive services such screenings, vaccinations, or counseling. This variable corresponds to prior studies that utilized routine care as a proxy for preventive access. 4 However it is unable to adequately represent the full spectrum of preventive behaviors. Therefore, the findings should be considered indication of access to healthcare facilities rather than the implementation of specific preventative measures.
Overall Project Implications
This study highlights systematic disparities in healthcare access and financial effects for elderly immigrants in the United States. Private insurance serves as a protective factor, whereas gaps in governmental insurance programs and the challenges faced by the uninsured indicate major flaws. Demographic factors, including age, education, and gender, increase these gaps, demonstrating the intersectional nature of healthcare inequality.
The findings theoretically correlate with the Social Determinants of Health Theory and the Behavioral Model of Health Service Utilization, emphasizing the relationship of demographic, social, and systemic factors affecting health outcomes. The study’s reliance on national data and advanced analytical techniques, such as logistic regression and propensity score matching strengthen the validity of these conclusions; yet limitations such as the cross-sectional nature of the data limit causal inferences. Considering these strengths, the study contains many limitations. The cross-sectional approach prevents certain causal inference, because unexplained heterogeneity, such as pre-existing medical conditions or regional policy variations, can affect outcomes. In addition, self-reported factors from NHIS could cause reporting bias. Additionally, because the NHIS does not include clinical biomarkers (eg, blood pressure or HbA1c levels), this study cannot directly evaluate the link between insurance status and objective health outcomes. Future research linking survey responses to biomedical data would help clarify these associations. 25 Similar limitations are recognized in national insurance evaluations.10,25 Social support significantly impacts healthcare access for older immigrants. The participation of young adults or caregivers accompany patients, especially those with limited English proficiency, reduces transportation and linguistic barriers to medical care.4,10 However, many older immigrants live away from younger family members due to patterns of migration or financial constraints, which could threaten continuity of care and increase reliance on emergency services. These findings correlate with prior studies linking social isolation with decreased utilization of preventative healthcare. 24 This research contains several limitations. The cross-sectional design limits causal inference, and the reliance on self-reported data contributes to recall and reporting biases. Missing variables, such as the distance to care or health status, might confound associations. Finally, as NHIS excludes institutionalized populations, the findings may not be generalized to the overall elderly immigrant population.
Policy and Practical Implications
The policy implications of these results highlight the critical role of insurance type in determining healthcare access among elderly immigrants. The quality and scope of coverage vary substantially among different types of insurance. Private insurance usually offers larger provider networks as well as higher reimbursement rates, resulting in enhanced access to preventative care. 29 on the other hand, those receiving Medicaid frequently face access obstacles due to limited provider involvement, while Medicare’s design may inadequately cater to the linguistic and cultural needs of immigrant elders.6,8 These structural differences highlight why elderly immigrants with private insurance face fewer unmet needs and economic hardships.
Although the NHIS data do not specifically measure the use of complementary and alternative medicine (CAM), prior study suggest that older Asian immigrants often reach out to herbal remedies, acupuncture, and conventional treatments when biomedical care is either prohibitively costly or not accessible.9,19 These findings are consistent with research emphasizing the need for culturally adaptive interventions that integrate traditional practices into public health outreach. 32 The results underscore the urgent need of addressing inequalities in healthcare availability and affordability for elderly immigrants. Policymakers should focus on boosting the availability of insurance coverage through improving the adequacy of Medicare and Medicaid or increasing enrollment in private insurance to enhance access and relieve financial burdens. Moreover, providing culturally appropriate treatment is crucial; focused marketing and training medical professionals in linguistic and cultural consciousness can enhance medical services for elderly immigrants. Ultimately, specialized therapies must adapt to the needs of vulnerable populations, such as women, elderly folks, and individuals with higher levels of education who consistently encounter obstacles to obtaining care. The stigma related to immigration status and the COVID-19 pandemic impacted healthcare-seeking behaviors. From 2020 to 2023, research found that racialized stigma toward East and Southeast Asian communities prevented many older immigrants from seeking healthcare due to fear concerning discrimination and infection. 11 This context explains temporary reduction in the consumption of preventative services and encourages continuous efforts that improve cultural safety across clinical settings.
Future Research Directions
This study shows substantial inconsistencies and disparities; however, future research is needed for understanding the mechanisms behind these findings, particularly the unanticipated impacts of education. Longitudinal analyses are essential to discovering causal relationships among insurance coverage, demographics, and healthcare outcomes. In addition, future studies ought to assess the effectiveness of government initiatives intended for improving healthcare access for elderly immigrants. Future research should analyze how intersectional factors, such as gender, migrations status and history, and digital access, interact with insurance type to identity health outcomes among immigrant elders.
Conclusion
This study offers strong evidence of the significant influence of health insurance on access to healthcare and economic outcomes for elderly immigrants in the United States. Addressing these identified gaps requires coordinating strategy including policy reforms, social engagement, and culturally sensitive healthcare delivery. Promoting equal opportunity and diversity in health policy may improve preventive care utilization, decrease financial vulnerability, and enhance overall health for aging immigrant communities. By integrating cultural awareness into national and local health initiatives, governments may establish a more accessible, equitable, and efficient healthcare system which meets the needs of all elderly people.
Supplemental Material
sj-docx-1-inq-10.1177_00469580261421981 – Supplemental material for Health Insurance Coverage and Access to Care Among Older Immigrants: Evidence from the National Health Interview Survey, 2020 to 2023
Supplemental material, sj-docx-1-inq-10.1177_00469580261421981 for Health Insurance Coverage and Access to Care Among Older Immigrants: Evidence from the National Health Interview Survey, 2020 to 2023 by Momna Rani and Dale E. Yeatts in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Appendix 1
Variance Inflation Factor (VIF) Values for Multicollinearity Diagnostics.
| Variable | VIF | 1/VIF |
|---|---|---|
| Has medicare | 1.91 | 0.52 |
| Age | 1.60 | 0.62 |
| Has private insurance | 1.42 | 0.71 |
| Uninsured | 1.23 | 0.81 |
| Has medicaid | 1.17 | 0.85 |
| Educ clean | 1.08 | 0.93 |
| Sex | 1.01 | 0.99 |
| Mean VIF | 1.35 |
Appendix 2
Flow of Sample Selection and Insurance Distribution.

| Step | Count | Percent |
|---|---|---|
| NHIS 2020-2023 raw sample | 147 430 | 100 |
| Excluded: <60 years | 98 540 | 66.8 |
| Adults aged 60+ | 48 890 | 33.2 |
| Foreign born adults 60+ | 5611 | 11.5 of 60+ sample |
| Excluded US-born or missing birthplace | 43 279 | 85.5 of 60+ sample |
| Excluded: Missing key analytic | 0 | 0.0 |
| Final analytic sample (complete cases) | 5611 | 100 of analytic sample |
Acknowledgements
N/A.
Ethical Considerations
All analyses were carried out utilizing publicly available, de-identified data from the National Health Interview Survey (NHIS). The study was exempt from review by the University of North Texas institutional evaluation Board (IRB evaluation attached in supplementary documents) due to the use of secondary, publicly accessible data. This study conformed to the STROBE reporting standard for cross-sectional studies33
Consent to Participate
Not applicable.
Author Contributions
Momna Rani: Conceptualization, data curation, formal analysis, writing original draft, review, and editing. Dale E. Yeatts: Supervision and critically revised the manuscript, approved the final version of the article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data used in this study are publicly available through the National Center for Health Statistics (NHIS datasets, 2020–2023).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.