
Abstract
Post-traumatic stress disorder (PTSD) is often debilitating, with current treatments limited by low adherence, high costs, and accessibility issues. Innovative technologies such as virtual reality (VR), augmented reality (AR), and therapeutic video games provide immersive environments that may improve treatment outcomes. This systematic review and meta-analysis evaluated the efficacy of these approaches and explored their potential advantages over traditional methods. A comprehensive search of PubMed, PsycINFO, CINAHL, Web of Science, and Cochrane identified relevant studies. Two reviewers independently screened articles, extracted data, and assessed quality using the Mixed Methods Appraisal Tool (MMAT). A random-effects model was used to calculate pooled effect sizes (Hedges’ g), and heterogeneity was evaluated with the Q test and I2 statistic. Publication bias was examined with funnel plots, Egger’s, and Begg’s tests. Analyses were performed in Stata version 17.0. From 480 records, 21 studies were included in the review and 12 in the meta-analysis. VR-based treatments yielded a pooled effect size of –0.35 (95% CI [–0.57, –0.13]), indicating a small-to-moderate reduction in PTSD symptoms. The effect was statistically significant (z = –3.13, P < .01), with moderate heterogeneity (I2 = 46.28%, P = .03). Funnel plots and statistical tests suggested minimal publication bias. Meta-regression showed no moderating effect of gender. Subgroup analyses indicated significant benefits in male-only samples, participants aged 20 to 30 and over 40, and studies with follow-up periods ≤7 months. Larger effects were observed in studies with 15 to 30 participants. VR, AR, and video game interventions significantly reduce PTSD symptoms and may enhance accessibility and engagement compared to traditional treatments. These findings support the integration of immersive technologies into therapeutic practice to improve outcomes for individuals with PTSD.
Introduction
Posttraumatic stress disorder is a common mental disorder that can arise after traumatic experiences such as war, sexual violence, accidents, or natural disasters. 1 These experiences can have long-lasting psychological effects and significantly impact the patient’s quality of life, with a higher risk of mortality.2,3 The prevalence of PTSD is estimated to affect 3.9% (app. 320 Mio people) of the global population. 4 Primary treatments for PTSD include medication, cognitive-behavioral therapy (CBT), Eye Movement Desensitization and Reprocessing (EMDR), and exposure therapy. 5 However, challenges such as low medication adherence, limited access to healthcare, and side effects of drugs can hinder effective treatment.6,7 Traditional therapy models often fail to provide the immersive experiences necessary for trauma recovery, and barriers like high costs, long waiting lists, and logistical issues complicate access to care.8,9 Furthermore, it can be difficult to fully immerse patients in traumatic scenes using conventional methods, making alternative approaches to treatment essential. 10
Emerging technologies such as virtual reality (VR), augmented reality (AR), and video games offer promising new ways to treat PTSD. VR creates immersive, controlled environments where patients can confront traumatic memories safely, while AR integrates therapeutic elements into the real world, enhancing cognitive and behavioral interventions.11,12 Although AR has been less frequently applied in PTSD treatment, recent studies suggest it can provide real-time exposure and emotion regulation training by overlaying trauma related cues onto real environments. This blended approach may enhance generalization of coping skills and offer a more gradual and realistic exposure experience. 13 Video games designed for mental health offer interactive ways to practice coping skills and reduce symptoms. 14 Gamification integrates rewards, challenges, and progress tracking further boosts engagement and adherence to treatment, which is often a challenge in traditional therapy methods.15,16 However, the specific role of gamification in PTSD treatment is still underexplored. While gamification has shown promise in enhancing engagement in other mental health treatments, 17 there is limited research on its direct impact on PTSD symptom reduction. Further investigation is needed to understand how specific game mechanics, such as rewards and progression systems, can enhance the effectiveness of PTSD therapies. VR therapy can be conducted both in the presence of a therapist, where guidance and support are provided during exposure to traumatic scenarios, and independently, where patients can engage with the therapy on their own. In the latter case, the VR system is often designed to guide the patient through the therapeutic process, with remote monitoring or follow-up consultations by a therapist as needed. Studies have shown that VR interventions can be effective when used in both therapist-guided and self-guided formats, with some research suggesting that patients can complete VR exposure therapy independently, with minimal therapist involvement. 18
The use of these technologies in PTSD treatment depends on their ability to create immersive, customizable experiences based on individual needs. VR, for instance, has been employed to recreate trauma-related scenarios in a controlled environment, allowing patients to confront and process their trauma safely. 19 AR and video games can support skills training and behavioral practices in engaging formats, potentially improving adherence and efficacy. 20 Recent studies have examined the efficacy of virtual and augmented reality technologies, as well as therapeutic video games, in mental disorders. For example, a study investigated the effects of VR exposure therapy and found significant reductions in PTSD symptoms, with participants experiencing improvements in their emotional regulation and symptom severity. 10 Additionally, a systematic review showed the promising outcomes of virtual reality in trauma therapy, noting that VR interventions often result in better engagement and adherence compared to traditional methods. 21 When compared to traditional treatments such as EMDR, prolonged exposure therapy, or pharmacotherapy, VR offers unique advantages in terms of immersion and engagement. The highly interactive and personalized nature of VR therapy has the potential to overcome the limitations of conventional treatments by providing more immediate, accessible, and tailored interventions, which may lead to quicker symptom relief. 20
To the best of our understanding, no studies have specifically evaluated the effects of AR on improving symptoms of PTSD. However, there are some studies that show the impacts of AR on anxiety disorders, phobias, and other related mental disorders. A systematic review assessed the potential of AR in phobias, finding that it could improve the therapeutic process by providing a more interactive and engaging experience for patients. 22 Compared to existing systematic reviews, this study aims to address significant gaps in the literature by specifically investigating the impact of AR technologies on PTSD, an area that has received limited attention. Emerging evidence supports the integration of VR and AR technologies in therapeutic contexts, indicating a notable reduction in PTSD symptoms when combined with cognitive-behavioral therapy (CBT). 23 Moreover, this review explores the role of gamification within these interventions, emphasizing its potential to enhance treatment effectiveness and improve patient adherence, an aspect that has been insufficiently addressed in previous reviews, including those focused on VR. Therefore, the objective of this systematic review and meta-analysis is (1) to assess the effectiveness of emerging technologies, including VR, AR, and video games, assessing their impact on PTSD symptom reduction and therapeutic outcomes. And (2) To investigate the role of gamification elements within these interventions, examining whether their inclusion enhances both treatment efficacy and patient adherence.
Methods
This systematic review and meta-analysis were reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines 24 (see Supplemental Appendix A).
Study Selection
Studies published until May 15, 2024, were retrieved through systematic literature searches in PubMed, PsycINFO, CINAHL, Web of Science, and Cochrane. The articles were identified using a range of keywords, including terms related to PTSD and interventions involving gamification, virtual reality, augmented reality, video games, serious games, computer games, and virtual reality exposure therapy. The terms included in the search based on the PICO guideline are presented in Table 1.
Search Strategy and Key Terms.

In addition to database searching, we performed backward citation screening (by reviewing the reference lists of included studies) and forward citation searching using Google Scholar to identify more recent articles that cited the included studies.
Selection Criteria
Eligible studies comprised randomized controlled trials (RCTs) and single-group trials focusing on participants with a primary diagnosis of PTSD. Studies were required to evaluate the impact of interventions utilizing VR, AR, or video game technologies. Outcome measures specifically assessed PTSD symptoms using validated assessment tools. No studies were excluded based on methodological quality assessment.
We included both RCTs and single-group trials in the systematic review to provide a comprehensive overview of immersive interventions for PTSD. However, only RCTs were included in the meta-analysis due to their higher internal validity and ability to control for confounding variables, which ensures more reliable estimation of treatment effects 25
Inclusion criteria: Studies involving individuals formally diagnosed with PTSD, Interventions that employed VR, AR, or video game technologies as a therapeutic approach, Studies comparing VR, AR, or video game interventions to non-VR/AR control groups, such as cognitive behavioral therapy (CBT), prolonged exposure (PE), treatment as usual (TAU), or waitlist controls, Studies published in peer-reviewed journals in English, Studies with clearly defined pre- and post-intervention outcome measures.
Exclusion criteria: Studies lacking PTSD outcome data related to VR, AR, or video games, Studies that were unavailable in full-text format, Review articles, abstracts, conference papers, protocols, letters, or editorials, Studies without a clear intervention description or control group comparison.
Data Extraction
For the systematic review, based on the PRISMA guideline 24 2 authors separately reviewed data from the chosen studies. The information they gathered included the authors’ names, the year the study was published, the country where the research was done, the aim of the study, the type of sample used, the total number of participants, details about the control group, the types of technology used, the measures used to assess outcomes, the results of the study, any gamification features, and the involvement of therapists. Study screening and data extraction were conducted independently by 2 authors, and discrepancies were resolved through discussion or consultation with a third reviewer.
For the meta-analysis, data were extracted on the following variables: total sample size, treatment group sample size, control group sample size, gender distribution in both groups, measurement tools, the mean and standard deviation for both groups, type of intervention and control, and follow-up data for both groups. Only studies that reported mean and standard deviation (SD) scores of CAPS, PCL, or other comparable PTSD measures before and after randomization were included in the meta-analysis. Studies that did not report these values were included only in the systematic review. In studies that reported multiple PTSD outcome measures, we applied a decision rule to maintain consistency across analyses. Specifically, when both the Clinician-Administered PTSD Scale (CAPS) and the PTSD Checklist (PCL) were reported, we prioritized the CAPS as it is considered the gold standard for PTSD assessment due to its structured clinical interview format and higher diagnostic validity. If CAPS was unavailable, we selected the PCL or the next most widely validated and commonly used PTSD measure 26 (Bovin et al.). When studies reported outcomes for both PTSD and other mental health conditions (eg, depression), only PTSD-related outcomes were included in the meta-analysis. This decision was based on our study’s primary objective to evaluate PTSD symptom reduction. Depression outcomes, while relevant, were beyond the scope of the current meta-analysis and were therefore excluded from quantitative synthesis.
Data Synthesis and Analysis
Data synthesis and analysis were conducted using STATA version 17.0. To assess potential biases in the studies, we utilized several methods, including a funnel plot, Egger’s test, and Begg’s test. The funnel plot visually illustrates the likelihood of publication bias by examining the symmetry of study results; greater asymmetry suggests a higher probability of bias in smaller studies. Egger’s and Begg’s tests provide statistical evaluations of this bias.
To evaluate heterogeneity among the effect sizes of the studies, we employed the I2 statistic, which quantifies the percentage of variance attributable to heterogeneity rather than chance. The extent of heterogeneity was further evaluated using the Q statistic. An I2 value of 25% denotes low heterogeneity, 50% represents moderate heterogeneity, and 75% indicates high heterogeneity.
Standardized mean differences were calculated using Hedges’ g based on post-treatment scores (mean and standard deviation) reported for the intervention and control groups. In addition, meta-regression analysis was conducted to determine whether specific study characteristics moderate the observed heterogeneity. Given the expected variability among studies, a random effects model was applied to compute a 95% Confidence Interval (CI) for the effect sizes.
Risk of Bias Assessment
Two reviewers independently assessed the data using the Mixed Methods Appraisal Tool (MMAT, version 2018). a comprehensive tool designed to evaluate the quality of mixed study reviews, encompassing qualitative, quantitative, and mixed-methods research. 27 The MMAT evaluates methodology across 5 categories: qualitative studies, randomized controlled trials (RCTs), non-randomized studies, quantitative descriptive studies, and mixed methods research. In cases of disagreement, additional reviewers were consulted to resolve differences through discussion and consensus. Studies were assessed using MMAT criteria specific to their study type. The latest version of the MMAT employs a descriptive approach for quality assessment rather than assigning scores. Reviewers respond with “yes,” “no,” or “unclear” for each criterion in a study’s category. A “unclear” response indicates insufficient information to make a determination.
To assess the impact of study quality on the robustness of the findings, we conducted a planned sensitivity analysis by excluding studies rated as low quality (ie, those with an MMAT score below 60%). This methodological decision was made in accordance with the Cochrane MECIR conduct standards (C57), which recommend incorporating risk of bias assessments into evidence synthesis through sensitivity analyses that examine whether results differ when studies at high risk of bias are excluded. 28
Results
Study Selection
A thorough initial search retrieved 480 articles. After duplicate removal, 334 studies remained to be reviewed thoroughly and systematically using strict inclusion and exclusion criteria. The titles and abstracts were screened independently by 2 authors. The review paid close attention to each study’s methodologies, findings, and relevance to the objectives of this research. Disagreements were resolved by consulting a psychologist.
Out of this rigorous process of screening, 22 publications were selected for the systematic review, and out of those, 12 met the criteria for the meta-analysis (Figure 1; Table 2).

PRISMA flowchart illustrating the screened and included studies assessing the impact of virtual/augmented reality and video games on PTSD improvement.
Summary of the Studies Included In the Analysis.

Note. References with “*” are those included in the Meta-Analysis. Column “Outcome Intervention-control*” Reported mean scores or score differences between intervention and control groups for primary PTSD outcome measures at post-treatment (eg, CAPS, PCL).
AU = treatment as usual; PE = prolong exposure therapy; VRET = virtual reality exposure therapy; CAPS = clinician-administered PTSD scale; PCL = PTSD checklist; BDI = beck depression inventory; BASIS-SS = behavioral and emotional support inventory – social support; IASMHS = inventory of attitudes toward seeking mental health services; SSRPH = stigma scale for receiving psychological help; 3MDR = multi-modular motion-assisted memory desensitization and reprocessing; CET = cognitive exposure therapy; IES-R = impact of event scale-revised; HADS = hospital anxiety and depression scale; SRHR = self-reported health-related; SRSR = self-reported symptom reduction; HR = heart rate; BR = breathing rate; OQ-45-2 = outcome questionnaire – 45 – second edition; WTC = world trade center.
The majority of studies were conducted from 2015 onward (n = 16, 76.19%). Studies conducted prior to 2015 represented a smaller proportion (n = 5, 23.80%). The majority of the studies were conducted in the United States (n = 15, 71.42%), with smaller contributions from the United Kingdom (n = 2, 9.52%), and the Netherlands (n = 2, 9.52%; Figure 2). Moreover, the majority of the studies (n = 17,80.95%) focused specifically on military personnel, soldiers, or veterans, addressing combat-related PTSD.

Frequency of articles by country.
In terms of control groups, the most commonly used designs were waitlist, treatment as usual (TAU), or minimal attention (n = 15, 71.42%). From these 15 papers, 2 studies included control groups that received 3MDR after a 12-week delayed intervention. For comparison purposes, we consider the data from these control groups before the 12-week intervention period.34,47 Other unique control conditions included prolonged exposure therapy(n = 2, 9.52%),40,49 tasks such as listening to philosophy podcasts (n = 1, 4.76%), 41 cognitive exposure therapy (CET; n = 1, 4.76%), 32 and present-centered therapy (PCT; n = 1, 4.76%). 33
Most studies (n = 19, 90.47%) utilized VR as part of the intervention either as a standalone therapy or in combination with 3MDR (Multi-Modular Motion-Assisted Memory Desensitization and Reconsolidation; n = 3, 13.63%),29,30,34,47 cognitive behavioral therapy (CBT), prolonged exposure (PE), or other therapeutic strategies. Two studies (n = 2, 9.52%) specifically explored the use of video games, such as Tetris, to disrupt intrusive traumatic memories.38,41
The Clinician-Administered PTSD Scale (CAPS) served as the most frequently utilized outcome measure across the studies (n = 15, 71.42%). Other commonly utilized tools included the Beck Depression Inventory (BDI; n = 5, 23.80%) and the PTSD Checklist (PCL; n = 5, 23.80%). Additionally, some studies incorporated other tools such as the Behavioral and Emotional Support Inventory (BASIS-SS), the Generalized Anxiety Disorder scale (GAD-7), the Patient Health Questionnaire (PHQ-9), and Subjective Units of Distress (SUD) to assess related symptoms of anxiety, depression, and distress.
Only 3 studies (n = 3, 14.28%) were mentioned to have used gamification elements.38,41,48 The gamification elements included interactivity and engagement, clear goals and tasks, remote accessibility, feedback mechanisms, reminder cues, and customizable options.
Across the included studies, intervention groups receiving VR-based treatments generally showed greater reductions in PTSD symptoms compared to control groups. These improvements were most commonly measured through CAPS and PCL scores and were evident at various timepoints, including immediately post-treatment and during follow-ups. Some studies also reported secondary benefits, such as reductions in heart rate, improved emotion recognition, and enhanced role-play performance.
Out of the 21 included studies, the majority (n = 19, 90.5%) reported that the interventions, such as virtual reality or video games, were delivered and supervised by professionals. One study (4.76%) explicitly stated that the intervention was conducted without professional involvement, while another (4.76%) did not specify who administered the intervention.
Quality Assessment
Table 3 presents the findings from the quality assessment of the included studies, conducted using the Mixed Methods Appraisal Tool (MMAT). Quality scores ranged from 20% to 100%. Based on the predefined threshold (MMAT score <60%), 1 study 50 was classified as low quality and excluded from the sensitivity analysis.
Findings from the quality evaluation of the studies.
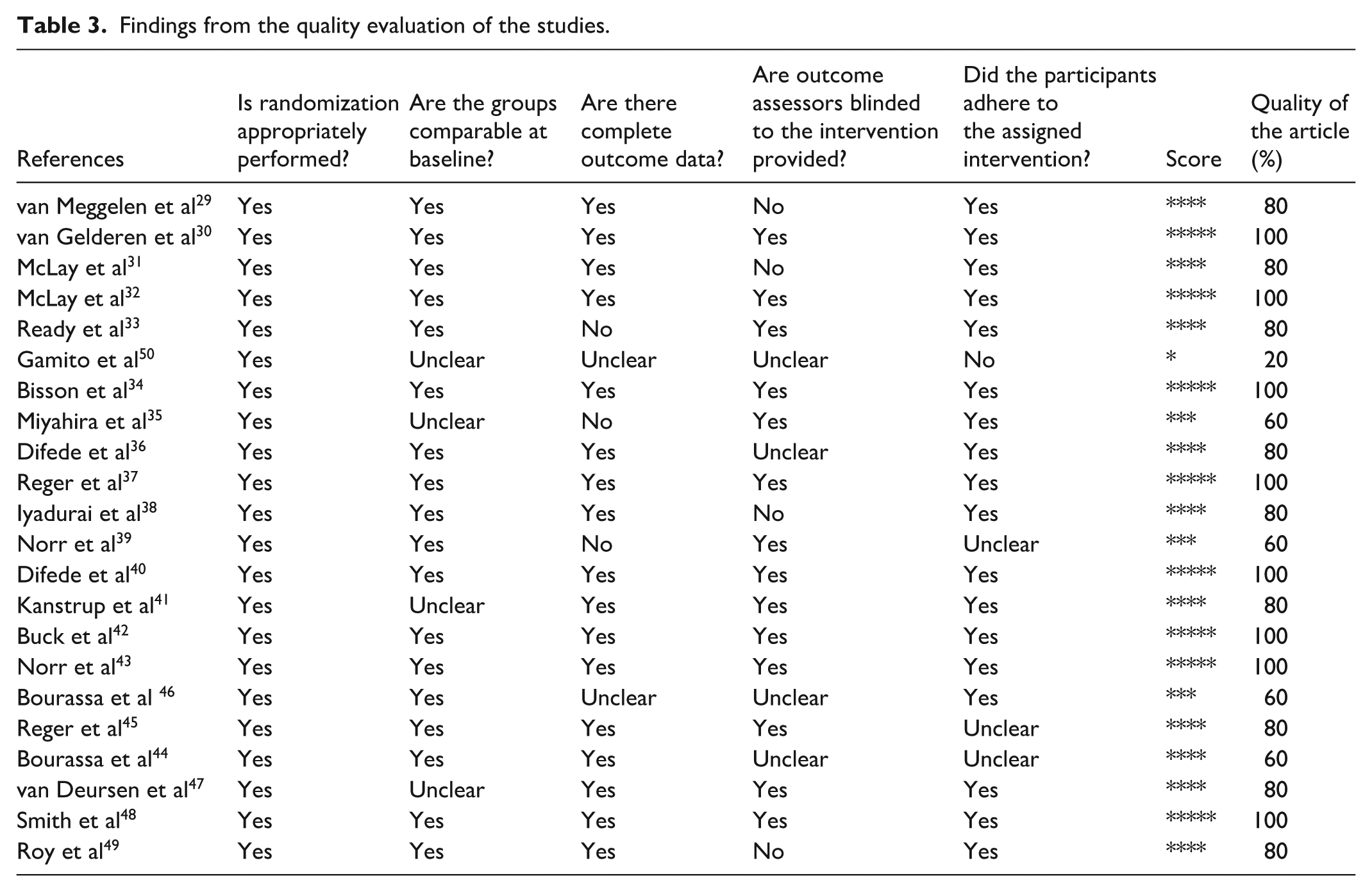
The remaining 21 studies (95%) met the minimum quality criteria (score ≥60%) and were retained for the main analysis.
Studies Effect Size
The provided findings illustrate the assessment of the impact of various treatments on PTSD. Each study contributed uniquely to the overall effect size, with weights varying from about 2.61% to 13.03%. The overall effect size (Hedges’s g) for the treatment effect on PTSD was estimated at −0.35, with a 95% confidence interval of (−0.57, −0.13). This indicates a small to moderate effect of the interventions in alleviating PTSD symptoms. The statistical analysis revealed significant results (z = −3.13, P = .00), confirming that the treatments assessed are statistically significant in improving PTSD symptoms outcomes (Figure 3).

Overall effect size results combining all studies.
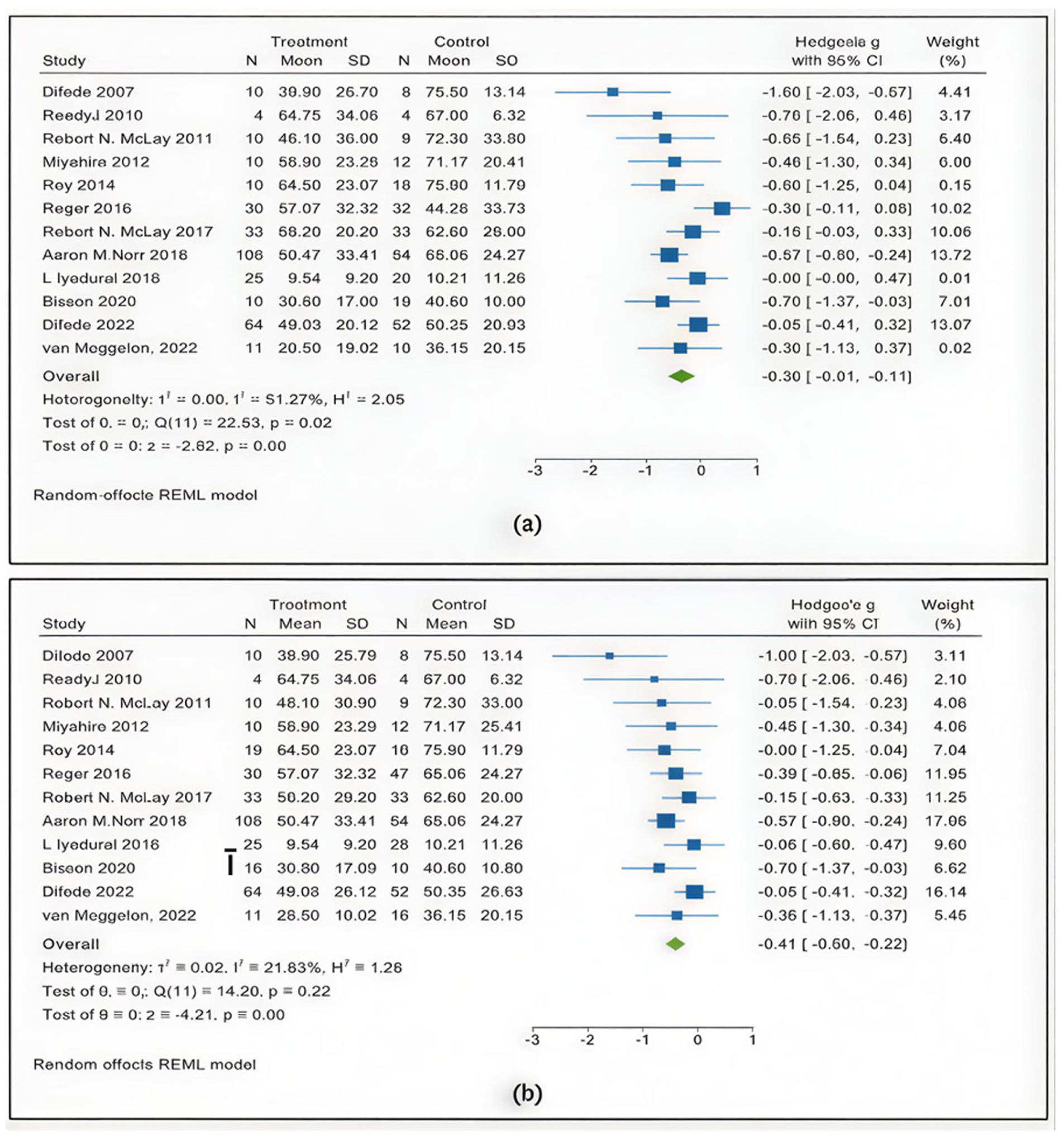
Separate effect size results for the comparison of VRE with (a) the waitlist control group and (b) PE.
It should be noted that the data from Reger et al. (2016) were extracted in 2 rounds, as the study compared Virtual Reality Exposure (VRE) both with a waitlist control group and with Prolonged Exposure (PE). The results of these 2 rounds are reported separately in Figure 4a and b.
In Figure 4a, the overall effect size (Hedges’s g) for the treatment effect on PTSD was estimated at −0.36, with a 95% confidence interval of (−0.61, −0.11). This indicates a small to moderate effect of the interventions in reducing PTSD symptoms. Statistical analysis revealed significant results (z = −2.82, P = .00), confirming that the treatments evaluated are statistically significant in improving PTSD outcomes. The heterogeneity among studies was moderate (I2 = 51.27%).
Moreover, in Figure 4b, the overall effect size (Hedges’s g) was estimated at −0.41, with a 95% confidence interval of (−0.59, −0.22), indicating a moderate effect of the interventions in alleviating PTSD symptoms. Statistical analysis showed significant results (z = −4.21, P = .00), supporting the statistical effectiveness of the treatments. The heterogeneity among studies was lower compared to Figure 4b (I2 = 21.83%), indicating greater consistency across studies.
Publication Bias
The funnel plot revealed a relatively symmetrical distribution of studies around the estimated overall effect size (θ_iv), indicating minimal evidence of publication bias (Figure 5). This pattern indicates a balanced representation of positive and negative study results, supporting the reliability of the findings on the role of virtual reality interventions in reducing PTSD symptoms.

Funnel plot of studies assessing the impact of virtual reality on improving the symptoms of PTSD.
Moreover, the Egger’s regression-based test for small-study effects indicated no significant small-study bias. The test yielded a beta coefficient of −1.60 (SE = 0.967), with a z-value of −1.66 and a P-value of .0978. Since the P-value is greater than .05, it suggests that the null hypothesis of no small-study effects cannot be rejected, indicating minimal evidence of publication bias.
Similarly, the Begg’s test for small-study effects indicated no significant small-study bias. The Kendall’s score was −22.00 (SE = 16.391), with a z-value of −1.40 and a P-value of .2001. Since the P-value exceeds .05, it suggests that the null hypothesis of no small-study effects cannot be rejected, providing minimal evidence of publication bias in the studies analyzed.
Heterogeneity Among Included Studies
The analysis revealed moderate heterogeneity among the studies (I2 = 46.28%, P = .03), indicating that the results are somewhat consistent across different studies. This suggests that the variations in effect sizes are not solely attributable to chance, and there may be underlying factors influencing this variability. The Q-test for heterogeneity showed a significant result (Q [12] = 22.65, P = .03), indicating that there is notable heterogeneity among the studies analyzed.
Meta-Regression Analysis
Meta-regression analysis was conducted to explore whether study-level characteristics moderated the treatment effects on PTSD outcomes. As shown in Table 4, none of the moderators reached statistical significance at the conventional alpha level (P < .05). However, this association did not reach statistical significance. Similarly, other moderators, including participant age, sample size, and follow-up duration, showed β values near zero and high P-values, indicating no meaningful moderating effects. These findings suggest that the examined study-level characteristics did not significantly moderate the observed treatment effects. As none of the moderator variables reached significance, no definitive conclusions can be drawn about their influence on PTSD outcomes.
Meta-Regression Coefficients (β) for Potential Moderators of PTSD Treatment Effect Sizes.

Subgroup Analyses Based on Study Characteristics
Subgroup analyses based on study characteristics are presented in Table 5. The pooled effect size for male-only samples indicated a small to moderate reduction in PTSD symptoms (SMD = −0.39, 95% CI [−0.77, −0.01], P = .05) with low heterogeneity (I2 = 29.33%). Studies including both male and female participants showed a smaller and non-significant effect (SMD = −0.26, 95% CI [−0.77, 0.25], P = .32) with substantial heterogeneity (I2 = 75.84%). Interestingly, studies where gender was not reported exhibited a larger significant effect (SMD = −0.57, 95% CI [−0.85, −0.29], P < .01) with no heterogeneity.
Subgroup Analyses Based on Study Characteristics.

Participants aged 20 to 30 years showed a significant moderate effect (SMD = −0.57, 95% CI [−0.91, −0.24], P < .01) with no heterogeneity. The 31 to 40 years subgroup demonstrated no significant effect (SMD = 0.06, 95% CI [−0.28, 0.39], P = .74) and low heterogeneity (I2 = 23.85%). For participants over 40 years old, a significant reduction in symptoms was found (SMD = −0.59, 95% CI [−1.05, −0.13], P = .01) with moderate heterogeneity (I2 = 51.44%). Studies not reporting age also showed a significant effect (SMD = −0.47, 95% CI [−0.82, 0.13], P = .01).
Short-term follow-up (1-3 months) revealed a significant small effect (SMD = −0.35, 95% CI [−0.63, −0.08], P = .01) with moderate heterogeneity (I2 = 32.05%). The 4 to 7 months follow-up subgroup showed a larger significant effect (SMD = −0.67, 95% CI [−1.27, −0.07], P = .03) without heterogeneity. Studies without follow-up information showed a non-significant effect (SMD = −0.22, 95% CI [−0.78, 0.35], P = .46) with high heterogeneity (I2 = 80.94%).
Smaller studies with sample sizes between 1 and 15 participants showed a non-significant effect (SMD = −0.91, 95% CI [−2.36, 0.55], P = .22). Studies with 15 to 30 participants demonstrated a significant effect (SMD = −1.14, 95% CI [−2.11, −0.17], P = .02), while larger studies (>30 participants) revealed a smaller but significant effect (SMD = −0.27, 95% CI [−0.49, 0.06], P = .01).
Discussion
This review and analysis confirm that immersive technologies like VR, AR, and video games can be helpful tools for treating PTSD. These technologies create controlled, immersive environments that allow patients to safely and gradually face trauma-related triggers, which is a key part of proven PTSD treatments.36,52 The findings show a small to moderate but meaningful improvement in PTSD symptoms with VR interventions (Hedges’s g = −0.35), indicating their effectiveness. 53 This effect size, though categorized as small to moderate, carries meaningful clinical significance in the context of PTSD treatment. Even modest reductions in symptom severity can lead to substantial improvements in functioning and quality of life for individuals with PTSD. Notably, the observed effect size aligns with findings from other evidence-based treatments. For example, cognitive-behavioral therapy (CBT), a widely recognized first-line intervention for PTSD, typically demonstrates effect sizes ranging between 0.30 and 0.60. 54 This comparison suggests that VR-based interventions may be as effective as conventional therapies, while also offering added benefits such as enhanced engagement and immersive experiences that may support adherence and emotional processing.
The funnel plot analysis revealed a relatively symmetrical distribution of studies around the estimated overall effect size (θ_iv), which suggests minimal publication bias. Publication bias was assessed and found to be minimal, increasing the reliability of the synthesized evidence.
Most of the studies focused on using VR to treat PTSD related to combat. VR is particularly useful because it can recreate realistic, trauma-specific situations. This helps patients confront and work through their traumatic memories in a safe and controlled environment. 55 Gonçalves et al 56 noted that VRET reduces PTSD symptoms in military as well as civilian populations and pointed out its versatility across different trauma situations. The lasting improvements in symptoms over time highlight the long-term effectiveness of VR-based treatments. 54 These results align with earlier research showing that immersive environments can improve how people engage with therapy and the results they achieve. For example, studies by36,57 show that VR helps people stick to therapy and manage their emotions better. Freeman et al add that automated therapy using VR decreases avoidance behavior and anxiety in patients with anxiety disorders, proving it’s suitable for large-scale interventions in mental health. 58 Comparing these results with traditional therapies, VR-based treatments often show similar or even superior outcomes in engaging patients and enhancing their adherence, as evidenced by studies such as those by Maples et al, 19 which found VR to be particularly effective in keeping patients engaged longer than standard exposure therapies. Additionally, the interactive features of video games and AR make therapy more engaging, reducing fatigue and encouraging continued participation. 59 A systematic review by Wechsler et al 60 assessed the efficacy of VRET in treating specific phobias. The review concluded that VRET was superior to waitlist controls and equally effective as in vivo exposure therapy in alleviating phobia symptoms. The study also noted that VRET has the potential to increase accessibility to exposure therapy for individuals who may not have access to traditional treatment methods. When compared to traditional in vivo therapies, VRET offers a more flexible and scalable solution, especially for individuals in remote or underserved areas, as shown in the works of, 61 which demonstrated the efficacy of remote VR therapy in treating PTSD.
While Virtual Reality (VR) has received the most attention in PTSD treatment research due to its ability to recreate trauma-specific environments, emerging technologies such as Augmented Reality (AR) are beginning to offer complementary possibilities. Unlike VR, which immerses patients entirely in a simulated environment, AR overlays therapeutic elements onto the real world. This approach enables patients to gradually confront trauma-related cues within familiar contexts while maintaining a sense of control and safety. By blending virtual stimuli with real-life settings, AR may enhance the generalization of coping skills beyond the clinical environment and provide a smoother transition from therapy to everyday life. Furthermore, AR can complement traditional exposure therapies by offering more accessible, mobile-based, and context-sensitive interventions. Future research should explore real-time AR applications through mobile apps or wearable devices to extend the reach of PTSD treatment and support ongoing symptom management in daily settings.13,20
The 3 studies reviewed suggest that gamification elements can improve engagement and adherence in PTSD interventions. Smith et al 48 used VR job interview training, where the interactive nature of VR likely enhanced participant involvement, suggesting gamification may improve adherence. Kanstrup et al 41 incorporated task-based interventions to prevent intrusive memories, indirectly using gamified elements to maintain focus and engagement. Iyadurai et al 38 used Tetris, a clear example of gamification, to reduce intrusive memories, showing how game-based interventions can enhance cognitive engagement. Together, these studies imply that gamification can play a key role in improving participation in PTSD treatments, though more research is needed to compare its efficacy against non-gamified methods. Despite the limited number of studies employing gamification elements (only 14.28%), the limited available evidence suggests that gamification elements may enhance therapeutic engagement and adherence, though further studies are needed to confirm their impact on outcomes.38,41,48 Gamified interventions can include features such as progress tracking, achievement badges, feedback loops, and rewards, all of which are known to increase user motivation and engagement. 58 In mental health contexts, these elements can reduce dropout rates and increase adherence, particularly among younger or tech-savvy populations. Studies such as Freeman et al 58 have demonstrated the ability of gamification to sustain user involvement and improve treatment retention. Future research should explore how these techniques can be systematically integrated into both VR and AR-based PTSD therapies.
Another important issue is making VR and AR technologies accessible to everyone. Although these technologies are becoming cheaper, they are still hard to use in places with limited resources. Finding ways to make them more affordable and easy to use could help more people around the world benefit from them in mental health care. 56 Research into simpler, portable VR systems and remote therapy options could also make these tools more widely available. 51 Freeman et al 58 advocate for cost-effective, automated VR systems that could address logistical challenges and make therapy accessible even in low-resource settings. This aligns with findings by Gómez Bergin and Craven, which emphasized that cost reduction and remote access are critical factors for scaling VR therapy beyond high-resource settings. 62
The way VR-based therapies are designed and how users experience them also need attention. Studies show that features like instant feedback, personalized situations, and gamification elements can make users more engaged and improve treatment results. 63
VR, AR, and video games have great potential for helping people with PTSD, but more research is needed to improve these tools and make them as effective as possible. Studies that compare these technologies to traditional treatments and look at how they can be used alongside current therapies will be key to making them more useful in practice. 57 This review highlights how these immersive technologies could change mental health care, offering new, easy-to-access, and effective ways to treat PTSD. A systematic review by Gonçalves et al 56 evaluated the efficacy of VRET in treating PTSD. The review found that VRET produced statistically significant improvements in PTSD symptoms compared to waiting lists. However, there was no significant difference observed between VRET and traditional exposure therapy, suggesting that VRET is as effective as conventional methods. This finding is consistent with the work of 9 Vonèche-Cardia et al, who concluded that while VR therapies showed similar outcomes to traditional methods, their adaptability and potential for personalization offer a substantial advantage. Supporting this, a recent randomized trial found that a digital mental health intervention significantly reduced trauma-related symptoms, highlighting the promise of digital approaches for PTSD care. 64
Most studies (n = 19, 90.5%) emphasized professional involvement in delivering VR and video game interventions, which supports adherence, safety, and personalized care.19,37 One study (4.8%) lacked professional oversight, and another did not specify the provider, raising concerns about consistency and safety. 58 Future research should compare professionally supervised and self-guided approaches, emphasizing accessible solutions like automated systems with remote oversight.51,58
The moderate heterogeneity observed (I2 = 46.28%) indicates some variability across studies. This heterogeneity may be attributed to differences in VR intervention designs, including variations in immersion levels, exposure techniques, and hardware used. Additionally, sample characteristics, such as variations in PTSD severity, age distributions, and comorbid conditions, could contribute to inconsistencies in treatment outcomes. Differences in intervention duration, the number of sessions, and control group conditions further introduce variability.
Study Implications and Limitations
Theoretical Implications
This study adds to the growing research on new ways to help people with PTSD. By showing that VR-based treatments improve PTSD symptoms, our findings highlight the importance of technology, especially virtual reality, in tackling trauma-related issues. Additionally, although the meta-regression did not find statistically significant moderator effects, variations in VR treatment design highlight the need for careful and detailed evaluation of these interventions. Knowing how different VR treatments work can help create customized therapy plans for specific groups of people with PTSD. This can also strengthen the idea of personalized treatment for trauma recovery.
Practical Implications
This study has important practical uses for doctors, caregivers, and policymakers who work with people suffering from PTSD. The results show that using VR tools can help reduce PTSD symptoms, which means adding these technologies to treatment plans could improve patient care. Doctors might want to include VR, especially immersive games, alongside traditional therapy methods. Caregivers could consider using VR-based treatments at home, providing an easy and engaging way to support those with PTSD. Policymakers should think about supporting the use of VR in healthcare, as it has the potential to make PTSD care better and improve the lives of those affected. However, one critical practical consideration is the accessibility of VR technologies, particularly in low-resource settings. Despite the decreasing cost of VR systems, affordability remains a significant barrier to their widespread use. Research into simpler, more affordable VR setups, along with remote therapy options, could increase the availability of these tools in underserved areas. As Freeman et al. suggest, cost-effective and automated VR systems could make therapy more accessible, ensuring that individuals in remote or low-income settings can benefit from these treatments.
In addition, ethical considerations must be addressed. One concern is the risk of re-traumatization during VR exposure therapy, where patients may be confronted with highly distressing trauma-related stimuli. Clinicians must carefully monitor emotional responses and provide adequate support to mitigate this risk. Another issue is data privacy, as VR and AR systems often collect sensitive health information. Ensuring secure data storage and protection against unauthorized access is vital for maintaining patient trust. Future research should therefore not only refine methodological approaches but also establish ethical guidelines to ensure safe and responsible application of VR-based PTSD treatments.
Study Limitations
This study has several limitations. First, it focused exclusively on articles published in English, which may limit the inclusivity of the analysis. Future research should consider incorporating studies published in other languages to achieve a broader perspective. The second limitation identified in this review is the lack of a standardized protocol for conducting VR-based PTSD interventions. The studies included in this review varied significantly in terms of intervention duration, VR platform design, and outcome measures, which complicates the process of drawing robust and comparable conclusions. This variability not only limits the generalizability of findings but also underscores the need for a universally accepted framework to guide future research. Developing and adhering to a standardized protocol would enable researchers to better align their methodologies, thereby enhancing the reliability of meta-analyses and cross-study comparisons. Furthermore, the majority of studies reviewed were conducted on U.S. military personnel, which poses challenges in generalizing findings to other populations. While these studies provide valuable insights into the efficacy of VR interventions for PTSD within this specific group, they overlook diverse demographics such as civilians, children, and individuals from different cultural and socioeconomic backgrounds. This lack of diversity limits the applicability of the results to broader populations. Future research should prioritize inclusivity by recruiting participants from varied age groups, cultural backgrounds, and settings to enhance the generalizability of findings.
Conclusion
In this study, the impact of virtual reality on improving PTSD was assessed. our detailed review and analysis showed that using virtual reality can reduce PTSD symptoms, with moderate evidence from existing studies to support this finding. Some included studies suggested that immersive games may increase patient involvement and potentially improve treatment results, although our pooled analysis did not isolate their specific effect. These findings suggest that virtual reality could be a useful part of PTSD recovery plans and that adding game-based methods can lead to better treatment outcomes. More studies in this area could give us a deeper understanding of how virtual reality can be used to help with PTSD, both in medical and everyday settings.
Despite the challenges of methodological variability and limited participant diversity, this review highlights the promising potential of VR-based interventions in supporting PTSD therapy. The results indicate that VR can be an effective tool for addressing PTSD symptoms, particularly within structured and immersive environments. However, to fully realize its potential, future research must adopt standardized protocols and expand the scope of studies to include diverse populations. These advancements would not only improve the quality of evidence but also enhance the applicability of VR-based therapies across different contexts and settings.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251413101 – Supplemental material for Assessing the Impact of Virtual Reality, Augmented Reality, and Video Games on Improving Post-Traumatic Stress Disorder Symptoms: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-inq-10.1177_00469580251413101 for Assessing the Impact of Virtual Reality, Augmented Reality, and Video Games on Improving Post-Traumatic Stress Disorder Symptoms: A Systematic Review and Meta-Analysis by Saeideh Goharinejad, Salime Goharinezhad, Khadijeh Moulaei, Björn Krüger and Thomas Spittler in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We would like to express our sincere gratitude to Dr. Shahrzad Mazhari for her valuable guidance and support throughout the research process. Her insights and feedback were instrumental in improving the quality of this manuscript.
Abbreviations
VR: virtual reality; AR: augmented reality; CBT: cognitive-behavioral therapy; EMDR: eye movement desensitization, reprocessing; PTSD: post traumatic stress disorder; CAPS: clinician-administered PTSD scale; BDI: beck depression inventory; PCL: PTSD checklist; GAD: generalized anxiety disorder scale; PHQ: patient health questionnaire; SUD: subjective units of distress; TAU: treatment as usual; VRET: virtual reality exposure therapy; BASIS-SS: behavioral and emotional support inventory – social support; IASMHS: inventory of attitudes toward seeking mental health services; SSRPH: stigma scale for receiving psychological help; 3MDR: multi-modular motion-assisted memory desensitization and reprocessing; CET: cognitive exposure therapy; IES-R: impact of event scale-revised; HADS: hospital anxiety and depression scale; SRHR: self-reported health-related; SRSR: self-reported symptom reduction; HR: heart rate; BR: breathing rate
Ethical Considerations
Not applicable, as this study is a systematic review and meta-analysis and did not involve new human participants.
Author Contributions
Saeideh Goharinejad and Salime Goharinezhad reviewed the papers based on PRISMA guidelines and selected the final papers. Saeideh Goharinejad wrote the manuscript. Khadije Moulaei conducted the meta-analysis and wrote the results section of the meta-analysis. Professor Thomas Spittler and Professor Björn Krüger reviewed the manuscript and provided feedback. All authors reviewed and approved the final manuscript before submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.