
Abstract
Adolescents and young women (AGYW) represent 15.1% of the global population and face a heightened risk of depression, especially in low and middle-income countries. We investigated the prevalence and determinants of Depression among AGYW at risk of HIV in urban slums of Kampala. A quantitative cross-sectional design was used to assess depression in 394 AGYW (14-24 years) using the Patient Health Questionnaire from January to May 2023. Prevalence was analyzed using proportions and 95% confidence intervals. Statistical tests, including chi-square, Fisher’s exact, ANOVA, and Mann-Whitney U, explored associations. Logistic regression models assessed risk, and the Hosmer-Lemeshow test evaluated the model fit. The prevalence of depression was 7.9% (95% CI = 5.6%-11.0%). Marital status (P = .024), having a high number of multiple sexual partners in the last 3 months (P = .029), and having a high number of multiple paying sexual partners in the last 3 months (P = .005) were significantly associated with depression. Thus, advocacy is crucial for improving depression screening and treatment for AGYW.
Introduction
Globally, adolescent girls and young women (AGYW) aged 15 to 24 years account for 15.1% (594 million) of the world’s population1,2 and they are at a greater risk for mental health conditions such as depression. 3 Depression is closely related to suicide, which is the fourth most common cause of death among 15 to 29-year-olds. 3 Depression is more common in women compared to men, with a likelihood of onset during puberty.4 -6 Adolescence is a vital phase of development characterized by rapid physical, emotional, and social changes, and urban slum environments can exacerbate the challenges faced by young individuals, including mental health issues such as depression. According to recent data, 34% of adolescents worldwide reported having heightened self-reported depressive symptoms between 2001 and 2020. 7 In the USA, the frequency of major depressive episodes among teenagers grew dramatically from 8.1% in 2009 to 15.8% in 2019, according to the National Survey on Drug Use and Health. In Africa, studies conducted among adolescents and youth have reported rates of depression ranging from 12% to 36%.8 -10 Studies conducted in Uganda that have mainly focused on adolescents (10-19-year-olds) have reported rates of depression ranging from 18.2% to 34%.11 -15 Furthermore, in Uganda, depression has been reported more among AGYW compared to their male counterparts. 6 Several risk factors, such as hormonal fluctuations, societal expectations, academic pressures, interpersonal dynamics, experiencing bullying, having a family history of depression, education, and income, have been reported as predisposing to depression among AGYW.16 -18 AGYW living in urban slums of Kampala, where sex work, substance use, and intimate partner violence are more common, may be more prone to depression than AGYW in different environments.
Kampala, the capital city of Uganda, is characterized by a diverse socio-economic landscape, with urban slums emerging as focal points. Yet, the inhabitants face challenges such as food security, money, theft, access to medication, energy access, and sanitation, 19 which predispose them to unique health disparities. Research has consistently demonstrated the adverse effects of living in urban slums on mental health. 20 Overcrowded living conditions, limited access to basic amenities, and high levels of environmental stressors contribute to increased vulnerability to mental health disorders. 21 AGYW residing in urban slums often confront a combination of socio-economic, environmental, and psychosocial stressors that may predispose them to mental health challenges, including depression. 22 Several factors contribute to the vulnerability of AGYW in urban slums to depression, including limited access to quality education, economic opportunities, and healthcare services, societal expectations, gender-based violence, poor quality of home life, and the latent violence factor.6,9,23,24
A direct correlation between AGYW with depression, developing new HIV infections, has been documented. 25 In the sub-Saharan Africa region, approximately 160 000 new HIV infections occurred among AGYW aged 15 to 24 in the year 2022, while in Uganda, 15 000 new HIV infections were recorded. 26 Interventions such as pre-exposure prophylaxis (PrEP) for HIV prevention are effective27 -29 yet it is greatly affected by depression symptoms that cause low uptake and non-adherence.30,31 Data on depression among AGYW living in urban slums and at risk of HIV infection are still limited. This study aimed to determine the prevalence and determinants of Depression among AGYW at risk of HIV in urban slums of Kampala. This will inform targeted interventions, policy recommendations, and community-based support systems designed to improve mental health outcomes and enhance the overall quality of life for this vulnerable population.
Methodology
Study Design and Setting
This was a cross-sectional study (January-May 2023) nested within a randomized controlled trial (RCT) that aimed to determine the effect of a peer support intervention on oral PrEP uptake and adherence. AGYW were included in the RCT if they were HIV and Hepatitis B negative, not pregnant, not taking oral PrEP, and were willing to attend study visits. The study site was the AIDS Information Center (AIC) - Kampala branch. The AIC, established in 1990, is a non-governmental organization providing HIV prevention, treatment, and care services to individuals and communities in Uganda living with and affected by HIV through 8 branches countrywide.
Study Population
AGYW (15-24 years) were mobilized from urban slums characterized by sex-work venues, alcohol, and drug consumption.
Inclusion and Exclusion Criteria
All AGYW enrolled in the RCT were included in this cross-sectional analysis.
Data Collection Procedures
Data collection was conducted by both the study staff and the participants themselves. The study staff collected data on socio-demographics, patient health questionnaire 9 (PHQ-9), and alcohol use. While the participants self-entered their data electronically in a REDCap database that had both the read and audio versions mounted on a tablet. This data included their sexual behavior, IPV, drug use, and contraceptive use. The use of the 2 data collection methods helped improve the privacy, understanding, and honesty, especially for sensitive topics such as sexual behavior or substance use. These tools were available in either English or Luganda, with the Luganda version offered in both read-only and audio formats to enable illiterate participants to self-administer the questionnaires. All study participants were trained on the use of tablets during their first visit before the commencement of data collection.
Dependent Variable
The main outcome was depression, which was assessed using an interviewer-administered patient health questionnaire (PHQ-9) on 394 AGYW (that was not on the tablet). The PHQ-9 has 9 items with a total score of 0 to 27 and has been validated for use in the Ugandan setting. 32 A cutoff point of ≥10 was considered in this study32,33 with those scoring below 10 being regarded as non-depressed, while those with a score of ≥10 were regarded as depressed. A total of 394 AGYW were assessed for depressive scores using the PHQ-9.
Independent Variables
These variables included; demographics (age, tribe, country of origin, highest level of education, marital status, and weekly income), vulnerability factors (nature of job, sexual activity, use of modern contraception, multiple sexual partners, sex in exchange for money, having unprotected sex, and use of drugs of addiction), and stress factors (number of children, physical abuse in the past 3 months, and psychological/emotional abuse in the past 3 months). The drugs of addiction were assessed by asking the participants if they had ever used any drugs of addiction in their lifetime and in the past 3 months. The drugs asked about included: marijuana, sniffing petrol/solvent, heroin, cocaine, khat, tobacco, and Kuber.
Statistical Analysis Methods
This analysis aimed to determine the prevalence of depression and identify its determinants among adolescent girls and young women (AGYW) at risk of HIV in urban slums of Kampala. To achieve this, data were analyzed using
Descriptive statistics were used to summarize participants’ socio-demographic, vulnerability, and stress-related characteristics. Categorical variables were presented as frequencies and percentages, while continuous variables were summarized using means with standard deviations or medians with interquartile ranges, depending on their distribution. The prevalence of depression was estimated with corresponding 95% confidence intervals.
To assess associations between depression and explanatory variables, bivariate analyses were performed using chi-square or Fisher’s exact tests for categorical variables, and ANOVA or Mann-Whitney U tests for continuous variables as appropriate. Variables that were statistically significant at this stage were considered for multivariable analysis.
A multivariable logistic regression model was then fitted to identify independent factors associated with depression, adjusting for age and other relevant covariates identified a priori. Adjusted odds ratios (aOR) with 95% confidence intervals were reported. Model adequacy was assessed using the
Conceptual Framework
Figure 1 above shows how the socio-demographic, vulnerability and stress factors lead to the occurrence of depression in an individual.

Conceptual framework of risk factors for depression.
Ethical Considerations
We obtained ethical clearance from the Uganda Virus Research Institute ethics committee (ref: GC/127/918), the Uganda National Council for Science and Technology (ref: HS2490ES).
Consenting Procedures
All study participants provided written informed consent before engaging in study procedures. This included participants aged 15 to 17 years who are regarded as emancipated/mature minors in this study, as per the prevailing national guidelines, and were allowed to provide their written informed consent independently. 34
Results
Socio-demographic factors: a total of 394 study participants were interviewed in this study, with a mean age of 19.4 years (SD ± 2.3). Almost two-thirds of the participants, 258 (65.5%), were Baganda by tribe, 388 (98.5%) were Ugandans, 310 (78.7%) had completed a primary level of education, 57 (14.5%) were separated/widowed, and the majority 254 (64.5%) earned an income between 2.6 and 13 US dollars (Table 1).
Socio-Demographic and Vulnerability Factors.

For vulnerability factors, 311 (78.9%) were sex workers, 340 (86.3%) were currently using a contraceptive method, with the main method used being condoms (139 (40.9%)). Two hundred and three (52.1%) of the participants had a low number of multiple sexual partners within the last 3 months, while 230 (59.4%) had a low number of multiple sexual partners (paying) within the last 3 months. Only 159 (41.1%) of the participants used condoms consistently, while the rest 228 (58.9%) were inconsistent condom users. For those who had paying sexual partners, only 162 (43.7%) had consistent condom use. More than a third, 140 (35.5%), reported having ever used any drugs of addiction, and of these, 121 (86.4%) had used them in the past 3 months, with 46 (38.0%) reporting daily usage. Most of the participants, 50 (41.3%), used drugs during work, and the most common drug of use being was marijuana, 33 (27.3%), followed by tobacco, 31 (25.6%). The main reason for drug use was to get the courage to do their job, 57 (47.1%), followed by forgetting their problems/relieving stress, 34 (28.1%), and only 12 (10.3%) reported sometimes injecting themselves with drugs of addiction (Table 1).
Among the stress factors, 135 (34.3%) of the participants had 1 or more child/children, 128 (84.2%) had experienced physical violence, and 143 (84.6%) had experienced psychological/emotional violence.
Prevalence and the Determinants of Depression Among the Participants
The prevalence of depression was 7.9% (95% CI = 5.6%-11.0%) among the participants.
In an unadjusted analysis, marital status, having multiple men in the last 3 months, having multiple paying sex partners in the last 3 months, and having experienced physical violence were significantly associated with depression among AGYW (Table 2). After fitting in a multivariate logistic regression model; marital status (aOR = 2.62, 95% CI: 1.14-6.02), having a high number of multiple sexual partners in the last 3 months (aOR = 2.37, 95% CI: 1.09-5.13), and having a high number of multiple paying sexual partners in the last 3 months (aOR = 3.11, 95% CI: 1.42-6.81) were the only factors that had a significant association with depression among AGYW (Table 2).
Determinants of Depression Among AGYW At Risk of HIV Infection In Kampala, Uganda (January To May 2023).
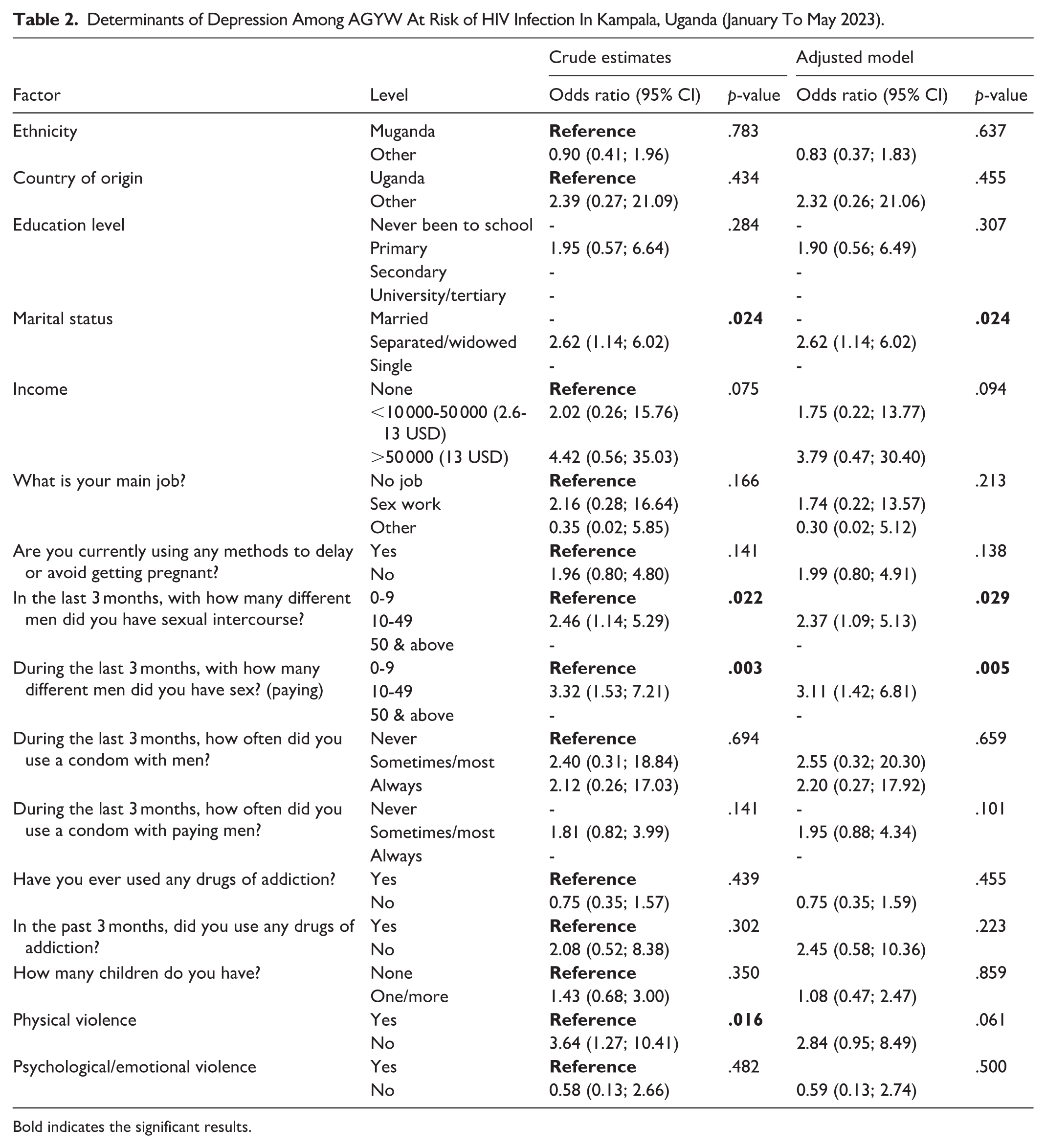
Bold indicates the significant results.
Discussion of Results
This study aimed to determine the prevalence and determinants of Depression among AGYW at risk of HIV in urban slums of Kampala. We found a low prevalence of depression of 7.9%. This is much lower than earlier studies conducted in Uganda, which showed prevalence rates ranging from 18.2% to 34%.11,13,15 This difference may be due to the following reasons: one of these studies was conducted at a primary healthcare facility that lacked provision of mental health services 15 while the other study was conducted among participants with a confirmed diagnosis of cancer, who were on treatment. Dealing with a diagnosis of an incurable illness and the side effects of treatment are stressful situations, putting them at high risk for depression. 11 The other study was conducted in Northern Uganda, where the participants were living in a humanitarian and fragile setting that had been affected by civil war for close to 2 decades. 14 The prevalence from the current study is similar to a study by Kinyanda et al 35 where 7.6% of the participants had a major depressive disorder in 4 districts of north-eastern Uganda. This similarity may be because both studies did not focus on people seeking treatment at the health facility, as the latter study was conducted at a community level, while the current study recruited its participants from a community, despite being facility-based. Therefore, both studies give a true reflection of the burden of depression at a community level, which calls for community-based interventions while combating depression among AGYW.
The only sociodemographic factor linked to depression in this study was marital status, with the separated/widowed AGYW being at risk of developing depression 2.6 times compared to their married counterparts. This result is consistent with research conducted in Northern Uganda by Kabunga and Nambozo, 14 which noted marriage as a protective factor against depression. Similarly, other researchers have noted that marriage protects against mental health problems35 -38 for reasons that marriage protects against stress, a key factor in causing depression. 39
As regards vulnerability factors, having had sexual intercourse with a high number of multiple partners in the last 3 months was significantly associated with depression. This is in agreement with findings from a cross-sectional population-based study conducted in Uganda among participants aged 18 to 30 years, in which female participants with a greater number of lifetime sexual partners were at high risk for depression. 40 Researchers in other areas have documented similar associations,41 -43 yet such a positive association wanes with age and only remains significant in young adulthood. 44 Also, more than half of the participants (58.9%) inconsistently used condoms, putting them at high risk for unintended pregnancies and sexually transmitted infections, including HIV infection, which predisposes them to mental health problems such as depression. On the contrary, Ramrakha et al 45 in their study noted that having multiple sexual partners was not linked to a higher incidence of depression.
Having had sex with a high number of multiple paying partners in the last 3 months was also significantly associated with depression. This may be because sex work is illegal in most parts of SSA, including Uganda, 46 which leads to broad criminalization by society as well as inadequate access to healthcare and support for this group 47 hence putting them at high risk for mental health problems, including depression.
Lastly, although not focused on in this study, a bidirectional relationship between depression and risky sexual behaviors has been documented. 25 With suggestions that it may predispose AGYW to risky sexual practices through mechanisms such as low self-esteem, impaired decision-making, and the search for emotional validation. This therefore calls for interventions that focus on breaking the intertwined relationship to reduce vulnerability to both depression and HIV risk among adolescent girls and young women.
Conclusion
Our study found a low prevalence of depression, with factors such as marital status, having had sexual intercourse with a high number of multiple partners in the last 3 months, and having had sexual intercourse with a high number of multiple paying partners in the last 3 months being significantly associated with depression. Therefore, there is a need for continued advocacy for mental health service provision among AGYW to increase the screening, early identification, and treatment in this population.
Limitations of the Study
This being a cross-sectional study, the causal direction of factors associated with depression could not be determined.
The sample size was calculated using the main RCT outcome (PrEP uptake), hence was likely underpowered for assessing factors associated with depression. The study, however, contributes information on an underlying prevalence of depression among AGYW in urban slums who would not be identified in the routine HIV prevention programs.
Supplemental Material
sj-doc-1-inq-10.1177_00469580251412738 – Supplemental material for Prevalence and Determinants of Depression Among Adolescent Girls and Young Women at Risk of HIV in Urban Slums of Kampala
Supplemental material, sj-doc-1-inq-10.1177_00469580251412738 for Prevalence and Determinants of Depression Among Adolescent Girls and Young Women at Risk of HIV in Urban Slums of Kampala by Philip Amanyire, Eugene Kinyanda, Leticia Kyohangirwe, Richard Stephen Mpango, Wilber Ssembajjwe and Yunia Mayanja in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580251412738 – Supplemental material for Prevalence and Determinants of Depression Among Adolescent Girls and Young Women at Risk of HIV in Urban Slums of Kampala
Supplemental material, sj-docx-2-inq-10.1177_00469580251412738 for Prevalence and Determinants of Depression Among Adolescent Girls and Young Women at Risk of HIV in Urban Slums of Kampala by Philip Amanyire, Eugene Kinyanda, Leticia Kyohangirwe, Richard Stephen Mpango, Wilber Ssembajjwe and Yunia Mayanja in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We acknowledge the contribution of the AGYW from the urban slums of Kampala who constituted our study sample. We also recognize the efforts of the research assistants and the contributions of the staff of the AIDS Information Center (AIC) - Kampala branch.
ORCID iDs
Consent to Participate
All study participants provided written informed consent before engaging in study procedures. This included participants aged 15 to 17 years who are regarded as emancipated/mature minors in this study, as per the prevailing national guidelines, and were allowed to provide their written informed consent independently. 34
Authors Contributions
PA, EK, LK, RSM, WS, and YM made significant contributions to the conception, design, acquisition of data, drafting of the manuscript, critical review, and coming up with the final version for publication. WS helped with the data analysis.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was part of the second European & Developing Countries Clinical Trials Partnership (EDCTP2) program supported by the European Union (CSA2020NoE-3102). The contents of this manuscript are the responsibility of the authors and do not necessarily state or reflect those of EDCTP.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Due to confidentiality requirements, the datasets created and analyzed for this work are not publicly available; however, upon reasonable request, the corresponding author can provide them in an aggregated and de-identified format.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.