
Abstract
Stress and depression are common in textile industry employees due to inadequate working conditions and challenging socioeconomic conditions. The objective of the study was to assess depression and mental health among adolescent and young females currently employed in a textile factory located in Tamil Nadu compared with past employees and women who have never been employed. This cross-sectional study included a total of 107 participants in each study group who were interviewed. The Patient Health Questionnaire–9 and Strengths and Difficulties Questionnaire were administered to screen participants for depression and mental health. More current employees (16.82%) and past employees (15.88%) suffered from depression severe enough to require treatment compared with never employed girls and young women (2.8%). Of the study participants, 59.8% of current employees, 63.6% of past employees, and 32.7% of never employed women had mental health or behavior problems. In the regression model, history of abuse was significantly associated with depression. Participants who were current employees and reported family debt and a history of abuse were significantly more likely to have mental health or behavior problems. Mental health issues such as depression and behavior problems were more likely among adolescent girls currently employed in textile industries. Further studies into the causes of this phenomenon are needed.
Keywords
Adolescence is a period of opportunity (Dahl, 2004). Of the 1.2 billion adolescents worldwide, 243 million adolescents live in India. Nurturing adolescents supports their potential and breaks cycles of poverty and inequity (The United Nations Children’s Fund, 2011). Tobacco and alcohol use, mental disorders, high-risk sexual behaviors, and stress are specific health problems among this population and have lasting impact (Sunitha & Gururaj, 2014). Community studies in India have reported the prevalence of common mental disorders among children and adolescents to be 6.46% (Malhotra & Patra, 2014). In India, domestic violence is common among adolescents with female adolescents more affected than male adolescents (Sarkar, 2010; Sunitha & Gururaj, 2014). Abused adolescent victims are observed to suffer from depression, anxiety, posttraumatic stress disorder, suicide, and behavioral problems (Sprah, 2008).
Working during adolescence could result in poor academic achievement, health problems, and impaired identity formation (Staff & Mortimer, 2007; Staff & Schulenberg, 2010). Employment might suggest pseudo-maturity, encouraging adolescents toward early sexuality and substance use (Mortimer, 2010). A working adolescent might not form or achieve future goals due to the effect of work on schooling (Zimmer-Gembeck & Mortimer, 2006). Working during adolescence has been associated with behavioral problems and substance use (Lee, Oi-yeung Lam, Ju, & Dean, 2017; Paternoster, Bushway, Apel, & Brame, 2003). This study assessed the mental health status of adolescent girls working in the textile industry of Tamil Nadu and compared them with adolescent girls and young women who had previously worked in the textile industry and adolescent girls who had never been employed.
Method
This cross-sectional study was part of a larger study which assessed the health status of adolescent women currently employed in the Indian textile industries. Approval was granted by the Institutional Ethics Committee (IEC), St. John’s National Academy of Health Sciences, Bangalore, India, before data were collected. All participants received oral and written information before giving their written consent. Study participants included adolescent and young women who were current textile employees, adolescent and young women who were past textile employees, and adolescent and young women who had never been employed in the textile industry. In addition, current and past employees were included in the study population only if they had worked for at least 1 year in area textile factories. Each study group included 107 participants.
The study was conducted in the Sirkazhi, Sembanar Koil, and Kollidam blocks of the Nagapattinam, a coastal and economically challenged district of the state of Tamil Nadu in India. This district has a population of about 1.61 million individuals (Nagapattinam District Population Census 2011, Tamil Nadu Literacy Sex Ratio and Density, 2011). The Nagapattinam District is primarily agricultural, but is also a a place where adolescent and young women work in textile factories.
Instruments
Study tools included the Patient Health Questionnaire (PHQ-9) to screen for adolescent depression and the Strengths and Difficulties Questionnaire (SDQ) to screen for behavioral problems (i.e., emotional, conduct, hyperactivity, peer problems, and prosocial behavior). The PHQ-9 has acceptable sensitivity and specificity, and its use in primary care settings has been validated. Both these questionnaires were translated and administrated by trained data collectors in the women’s native language, Tamil. A sociodemographic questionnaire specifically designed for the study gathered data on alcohol, tobacco, and drug use, and history of abuse as part of the Indian Adolescent Health Questionnaire. In the qualitative part of the study, the researchers conducted three focus group discussions (FGD) among the never been employed adolescent and young women, three FGD among current adolescent and young women employees, and three FGD among past adolescent and young women employees. In addition, three FGD were conducted with the parents of current and past employees. Six in-depth interviews (IDI) were conducted in the study area among key stakeholders.
Data Collection
The study was conducted from January 12 to 19, 2016, by trained data collectors during the “Pongal” (harvest festival) holidays because it was expected that working adolescent and young women would be available at their homes for interviews. Simple random sampling was used to choose the 107 currently employed adolescent and young women from the list of all currently employed adolescent and young women working in textile factories in the study area. For each current employee, the nearest residing adolescent female or young women who had worked in the textile industry in the past or had never been employed were chosen for the comparative groups.
Statistical Analysis
The chi-square test was used to assess associations between categorical variables. In the analysis, a two-tailed p value <.05 was considered statistically significant. Logistic regression analysis adjusted for confounders and assessed the independent association between variables and health status. Independent variables that were significant at the p < .05 level in univariate analysis were included in the multivariate analysis to control for confounding in regression models. The results are presented as odds ratios with 95% confidence intervals (CI).
Results
A total of 321 study participants were sampled, with 107 adolescent and young women placed in each study group. The participants’ ages ranged from 12 to 28 years. The mean age of the currently employed adolescent and young women workers was 18.14 years, past employees was 21.64 years, and the never been employed was 16.54 years. The baseline characteristics of the study population are displayed inTable 1.
Baseline Characteristics of the Study Groups
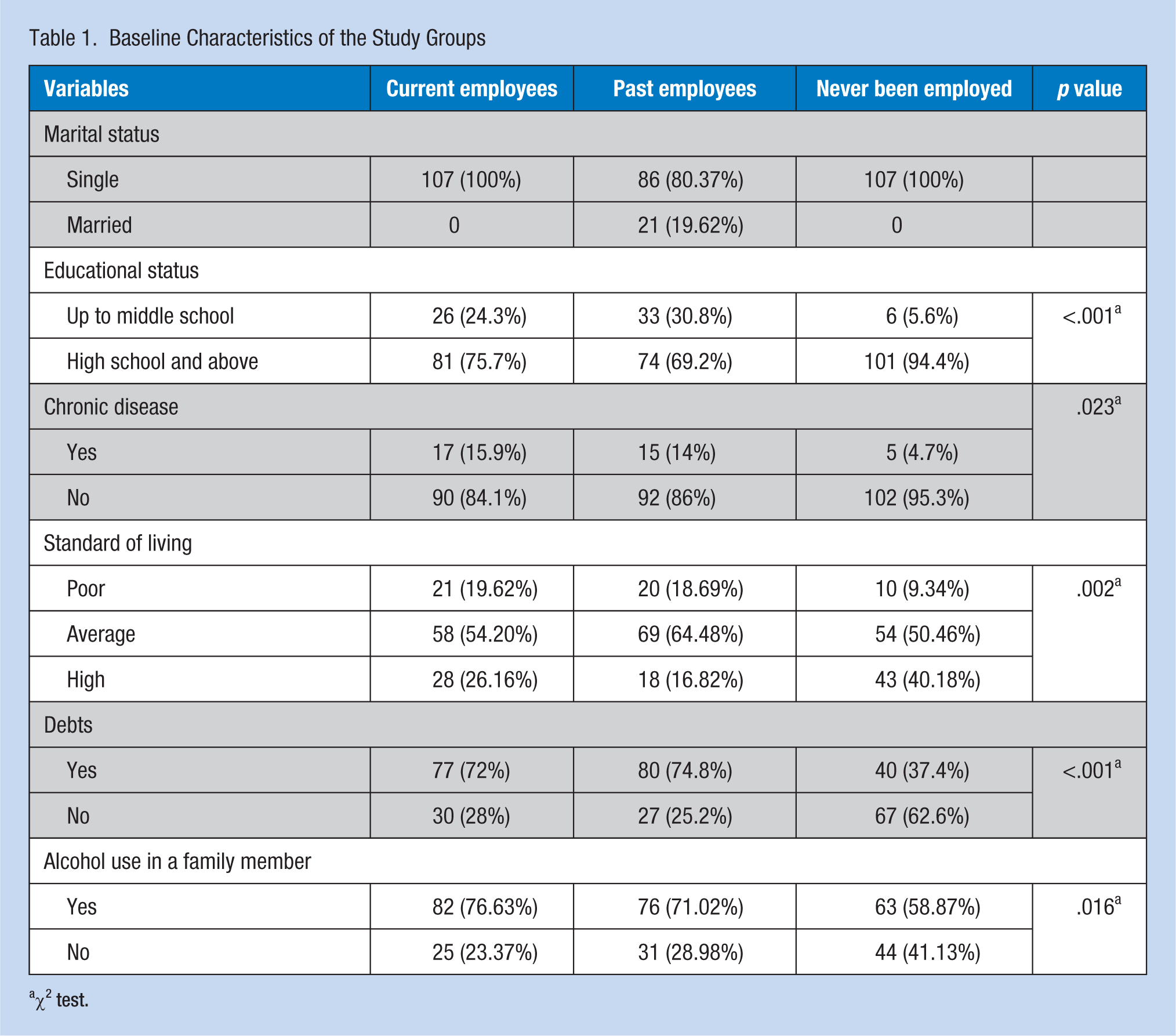
χ2 test.
Alcoholism and Abuse
Alcoholism was present in the family for 76.63% of current employees, 71.02% of past employees, and 58.87% of never employed. During FGD with the mothers of study participants, alcoholism was identified as a major social problem in the study area. Most of the mothers complained that men in the community consumed alcohol every day and this behavior had a significant impact on families causing financial problems and domestic violence and abuse.
History of abuse was reported by 50.46% of current employees, 34.57% of past employees, and 10.28% of never employed. From Table 2, it is observed that many adolescents when asked if they had experienced abuse ever said no. However, when questions on specific types of abuse were asked, they reported abuse experiences. This difference in reporting explains the discrepancy in the number of participants who reported a history of abuse and various types of abuse in Table 2. Hence, it can be said that 37 study participants who experienced verbal abuse, eight who experienced physical abuse, and two who experienced sexual abuse did not identify the experience as abuse or were fearful of stigma when the first question on history of abuse was asked. A significant difference was found between study groups regarding their abuse histories.
History and Type of Abuse Among Study Groups
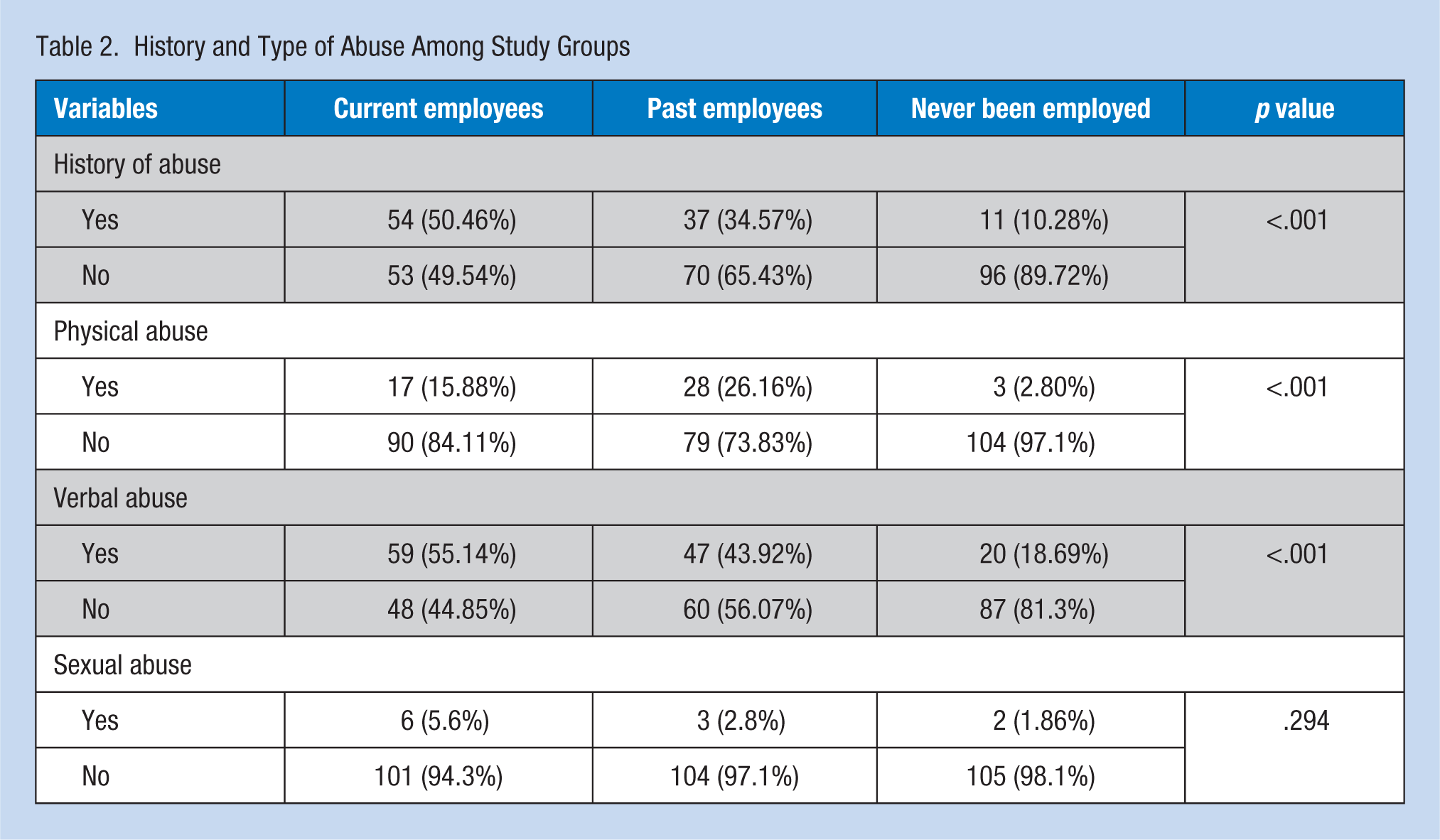
Both physical and verbal abuse were reported by 36 study participants, verbal and sexual abuse were reported by two participants, and all three types of abuse were reported by four participants.
Of those who reported a history of abuse, 41 (12.8%) were abused at home, two (0.6%) were abused at school, and 32 (10%) were abused elsewhere. A total of 40 current and 24 past employees reported abuse at the workplace. Of current and past employees, 55 (53%) reported verbal abuse, 35 (36%) reported physical abuse, and nine (9%) reported sexual abuse. Type of abuse that occurred at the workplace was not enquired in this study.
Substance Use
None of the adolescent and young women never employed reported using tobacco. However, seven current employees and two past employees had used tobacco. Some adolescent and young women in all three groups had consumed alcohol (nine current employees, 10 past employees, and 11 never employed). Drug use was reported by few women in each study group (eight current employees, 13 past employees, and nine never employed). Consumption of alcohol at the workplace was reported by three current employees and one past employee.
Depression
Mental health was assessed by screening study participants for depression and other behavioral problems, and significant differences among the groups were found (Table 3). Based on PHQ-9 questionnaire data, 32 (29.9%) current employees reported suicidal thoughts in the past month compared with 26 (24.3%) past employees and 12 (11.2%) never employed. Fourteen (13.1%) current employees had attempted suicide during their lifetimes compared with 26 (24.3%) past employees and 12 (11.2%) never employed. The researchers did not assess the method of suicide. More current (16.82%) and past (15.88%) employees needed treatment for depression compared with never employed women (2.8%) per PHQ-9 scores.
Mental Health Status of the Study Groups
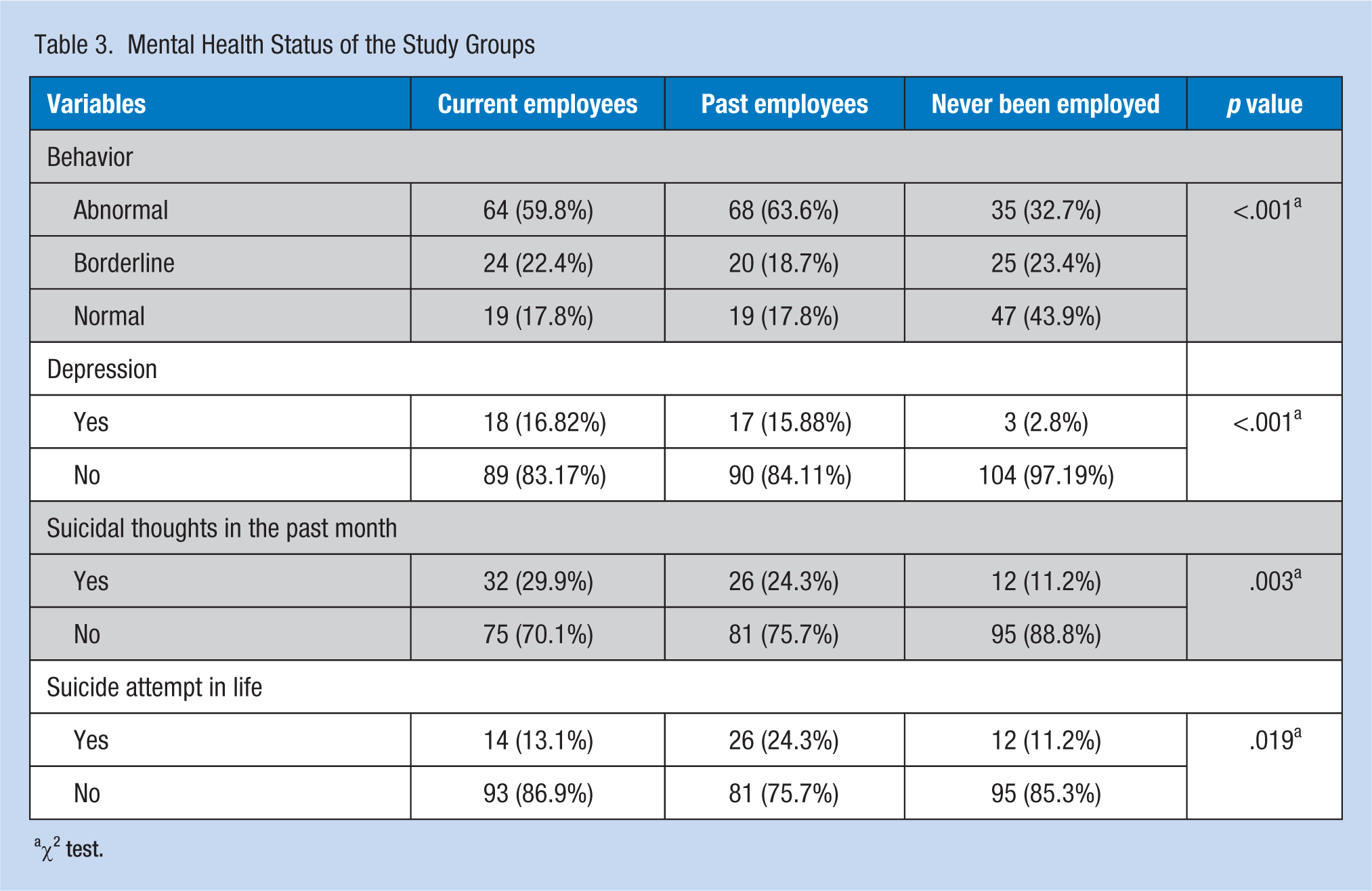
χ2 test.
From the FGD with study participants, the following factors were associated with depression: separation from parents, lower socioeconomic status, stressful work, family economic burden, family alcoholism, and less time for recreation at the workplace.
Behavioral Problems
Behavioral problems also differed significantly among all three study groups, with more current and past employees suffering from these mental health concerns. Behavioral problems identified by the SDQ included emotional, conduct, hyperactivity, and peer problems (Table 4). Prosocial behavior was normal among most of the study participants with 103 (96.3%) current employees, 95 (88.8%) past employees, and 86 (80.4%) never employed exhibiting normal prosocial behavior. Behavioral problems were more prevalent among current (59.8%) and past (63.6%) employees compared with never employed (32.7%). Behavioral problems of current and past employees could be explained by the higher prevalence of participant abuse, family alcoholism, less education, and inadequate standards of living.
Types of Behavioral Problems Among Study Groups
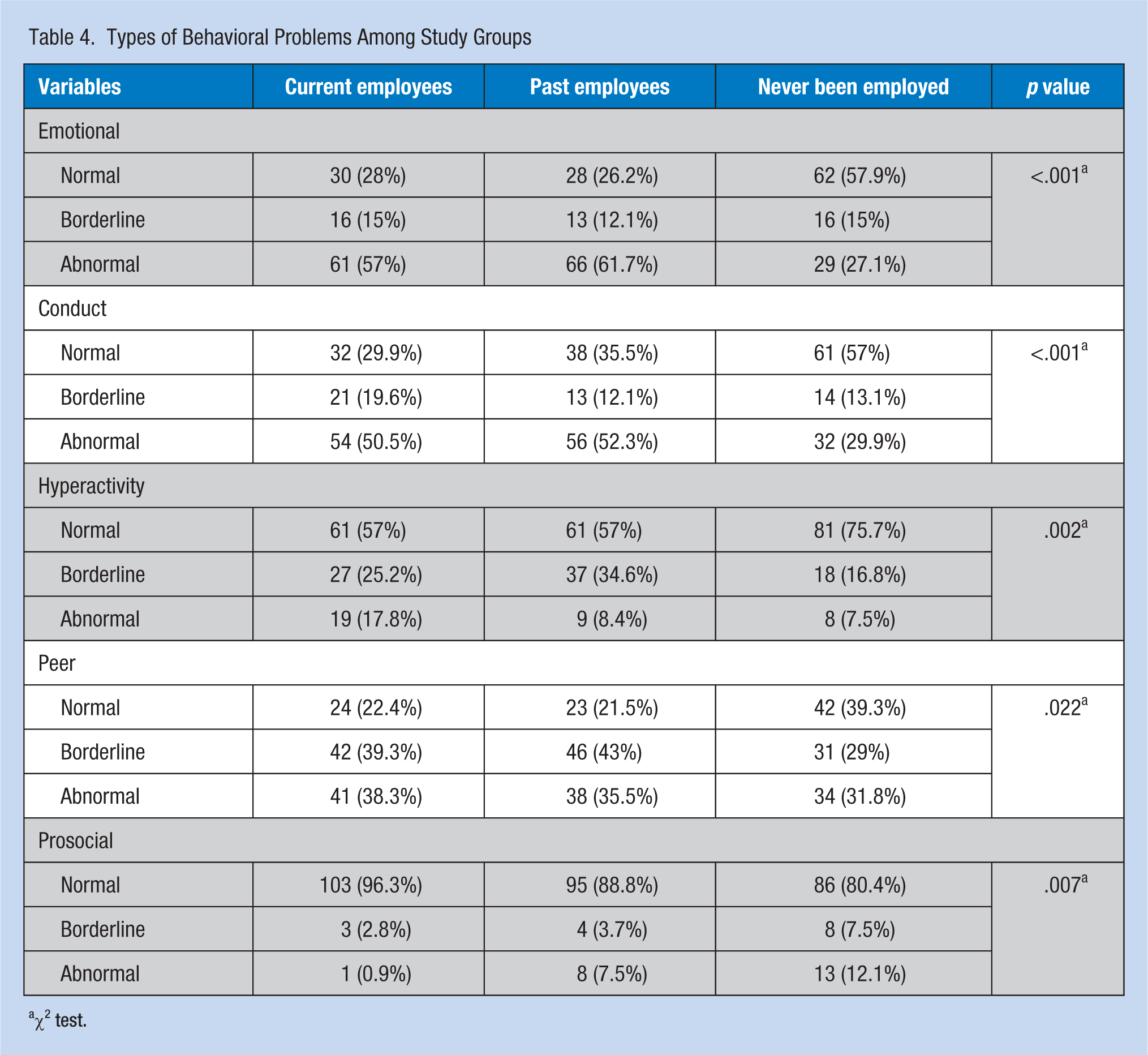
χ2 test.
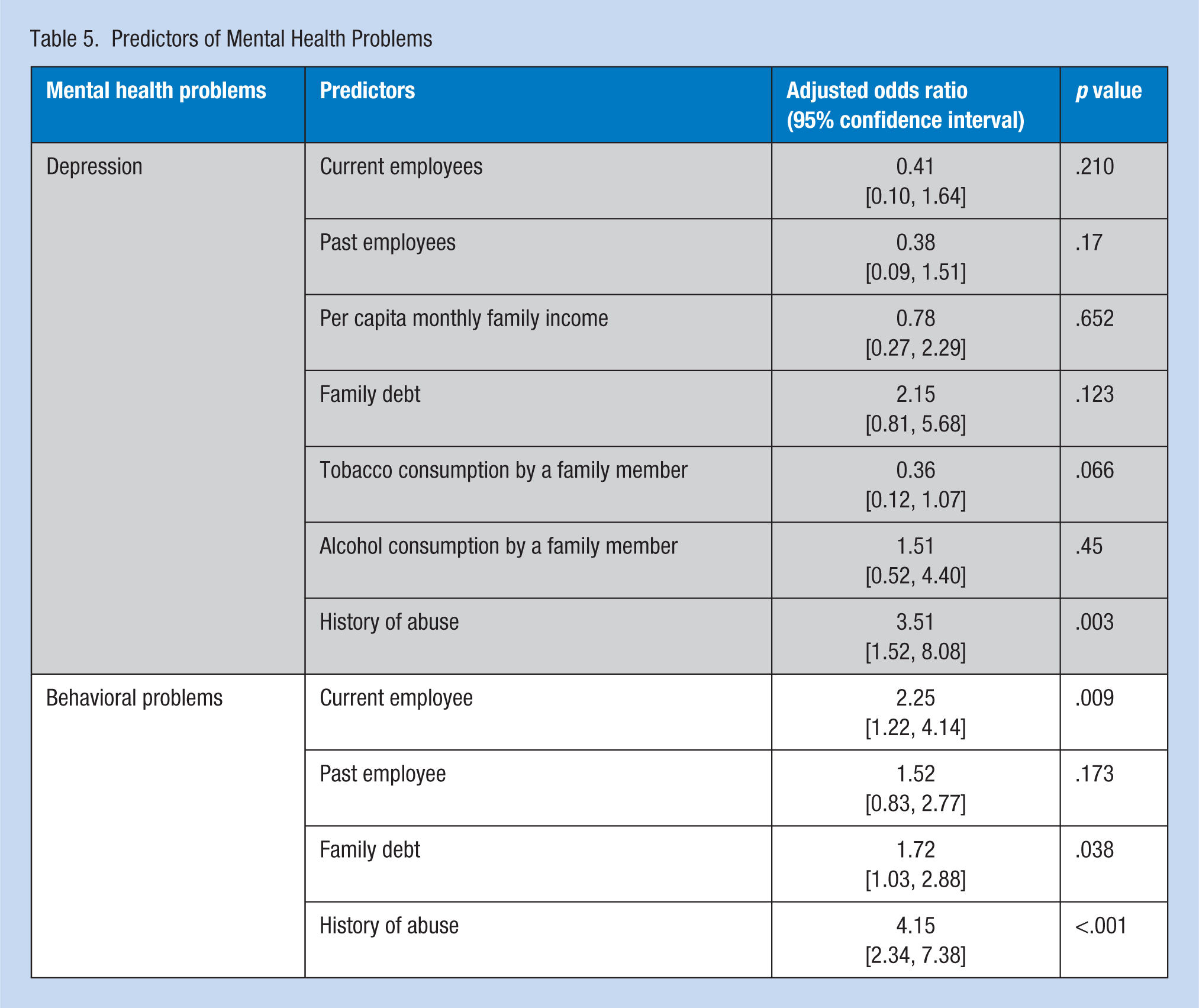
Factors significantly associated with depression in the univariate analysis were used in the regression model; it was observed that depression was significantly associated with history of abuse (adjusted odds ratio [AOR] = 3.51, 95% CI = [1.52, 8.08]; Table 5). Family factors such as alcohol and tobacco use, lower socioeconomic status, and employment (e.g., abusive disciplinary action in factories) could have resulted in abuse and resulting depression. Factors significantly associated with behavioral problems in the regression model were current employee (AOR = 2.25, 95% CI = [1.22, 4.14]), family financial problems (AOR = 1.72, 95% CI = [1.03, 2.88]), and history of abuse (AOR = 4.15, 95% CI = [2.34, 7.38]).
Predictors of Mental Health Problems
Discussion
Studies conducted in Tamil Nadu have shown a 5.7% to 62.4% alcoholism prevalence in the general population (Dutta et al., 2014; Easwaran, Bazroy, Jayaseelan, & Singh, 2015; Kaur et al., 2011; Kumar et al., 2013; Logaraj, Hegde, John, & Balaji, 2014). In the state of Tamil Nadu, the sale of Indian Made Foreign Liquor (IMFL) is controlled by the state government through the Tamil Nadu State Marketing Corporation Limited (TASMAC), which has reported successful retail business with high turnover and sales volume resulting in increasing revenue for the state (“Turnover of TASMAC,” 2015). Alcoholism is a major problem for the families of the study population; more than 50% of the study population had at least one family member who suffered from alcoholism. Interrelationship between substance use in parents and physical and sexual abuse of children have been reported in the scientific literature (Calhoun, Conner, Miller, & Messina, 2015; Rockville, 2004; Solis, Shadur, Burns, & Hussong, 2012). Low socioeconomic status, stressful relationships between parents and children, diminished control over behavior, and impaired parental bonding due to alcoholism can lead to child abuse (Miller, Maguin, & Downs, 2002). Children of alcoholics suffer from behavioral and personality problems which could be linked to future psychiatric problems and substance use (Hinrichs, DeFife, & Westen, 2011; Mahato, Ali, Jahan, Verma, & Singh, 2009; Waldron, Martin, & Heath, 2009).
The regression model for this study did not demonstrate that family alcoholism was significantly associated with depression or behavior problems among study participants. However, the researchers concluded that family alcoholism is detrimental to the health and well-being of families. Prohibition of alcohol sales is unlikely in the near future. However, slow implementation of prohibition could offer the state time to find other revenue streams (Doshi, 2016; Nathan, 2016).
Conduct disorders are more likely among women with histories of physical and sexual abuse (Green, Russo, Navratil, & Loeber, n.d.). The association between child abuse and future behavior problems has been well documented in the literature (Fergusson, Horwood, & Lynskey, 1997; Garnefski & Diekstra, 1997; Moylan et al., 2010; Odhayani, Watson, & Watson, 2013). Similar to these findings, history of abuse among study participants was significantly associated with behavior problems. Due to the cross-sectional nature of the study, data on time of abuse were not gathered from study participants.
In this study, a total of 64 (29.9%) current and past employees reported abuse at the workplace. The abuse of adolescent and young women workers has been documented in the South Indian textile industry (Theuws & Overeem, 2014). The textile industry in Tamil Nadu has a long history of abuse at the workplace; most of the supervisors are male and some display authoritarian and abusive behaviors. Commonly, when production targets have not been met, they resort to physical and verbal abuse of employees (Chamberlain, 2012; Theuws & Overeem, 2014).
Adolescence and young adulthood is a high-risk period for suicide (Vijayakumar, John, Pirkis, & Whiteford, 2005). It is a leading cause of death among youth in rural South India (Aaron et al., 2004). Female gender, not attending school or college, experience of physical and sexual abuse and violence, and common mental disorders are known risk factors for suicide (Pillai, Andrews, & Patel, 2009). In this study, 14 (13.1%) current employees had attempted suicide in their lifetimes compared with 26 (24.3%) past employees and 12 (11.2%) never employed participants. Suicidal thoughts in the past month were reported by 32 (29.9%) current employees, 26 (24.3%) past employees, and 12 (11.2%) never employed. Limited literature is available on suicidal behavior among adolescents in India. Sharma, Grover, and Chaturvedi (2008) reported that 16% of Indian adolescents reported suicide ideation and 5% of adolescents in South Delhi had attempted suicide. Chaudhury, Kenswar, Kumar, and Dixit (2013) reported that 33.2% of school-attending adolescents in Ranchi had suicidal ideations. From these two studies, it is evident that suicidal thoughts and attempts are significantly more common in this study population compared with adolescents in other studies. Suicide and depression in this population are a major mental health problem requiring urgent action.
Using the PHQ-9, the workers were screened for depression. The researchers observed that more current employees (16.82%) and past employees (15.88%) demonstrated depression requiring treatment compared with adolescent and young women who had never been employed (2.8%). However, in the regression model, depression was not associated with employment status for this study population.
The researchers observed that history of abuse was significantly associated with depression. The link between childhood abuse and depression has been reported in the literature; physical and sexual abuse in childhood has been associated with adult onset major depression (Bradley et al., 2008; Cukor & McGinn, 2006). Krishnakumar, Satheesan, Geeta, and Suresh Kumar (2014) reported a significant association between Kerala adolescents’ feelings of insecurity and isolation at home, being disliked by parents, and depression and a history of sexual abuse. Timing of abuse was not determined in this study, so it could have happened in childhood or in adolescence.
Tobacco use is a substance abuse disorder per the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013; “Substance-Related and Addictive Disorders,” 2013). Adolescents usually start smoking out of curiosity and later become habitual smokers (Park, 2011). In this study, very few young women reported tobacco use. General prevalence of tobacco use among adolescent girls in India ranges from 0% to 2.8% (Chadda & Sengupta, 2002; Sharma, Grover, & Chaturvedi, 2010). Tobacco consumption, especially smoking, is a relatively new phenomenon among adolescent girls in India over the past 10 to 15 years (Chadda & Sengupta, 2002). Prevalence and pattern of substance use in this population should be studied further.
Adolescents are prone to various behavioral problems; they are at high risk for behavioral problems which can be socially disruptive (Bartlett, Holditch-Davis, & Belyea, 2005). This study demonstrated that behavioral problems were more prevalent among current employees compared with past employees and never employed adolescent and young women. The researchers further observed that family debt was significantly associated with behavioral problems for the study population (AOR = 1.72, 95% CI = [1.03, 2.88]). Strong associations between socioeconomic status, debt, and antisocial behavior are well documented in the literature (Hoeve et al., 2014; Piotrowska, Stride, Croft, & Rowe, 2015). Consistent with this study, Berger and Houle (2016) found that unsecured debts impacted the socioemotional well-being of children. Family environment has also been found to contribute to behavioral problems (Pathak et al., 2011).
The association between work and behavioral problems among adolescent and young adult women is consistent with the literature (Bachman, Staff, O’Malley, Schulenberg, & Freedman-Doan, 2011; Kinney, 1993). In this study, current textile employees were likely to have behavioral problems. More than half of the current employees in this study demonstrated behavioral disorders through screening. No comparative studies of female adolescents working in the textile industry were found. However, Benvegnú, Fassa, Facchini, Wegman, and Dall’Agnol (2005) observed that 9.5% of working adolescents had behavioral problems. The difference in prevalence between the two studies could be due to the tools used and the difference in sociodemographic characteristics of the study populations. The high prevalence of behavioral problems among study participants could also be due to work responsibilities, work that does not promote acquisition of vital skills, and less time for socialization.
Limitations
Timing of abuse in the lives of adolescent and young women and suicidal methods used during past suicide attempts were not assessed in this study. The sample size was small; past employees and never employed adolescent and young women were sampled conveniently. The study sample came from a three-block area of a single district in Tamil Nadu which restricts the generalizability of the study. The researchers recognize that other variables (e.g., familial and genetic risk factors, history of bereavement, family discord, and resilience) could have played a role in the incidence of depression among the women in this sample (Conley & Rudolph, 2009; Raheel, 2015; Sajjadi et al., 2013; Saluja et al., 2004; Stapinski et al., 2013).
Implications for Occupational Health Nurses
In developing countries like India, few companies provide occupational health services. Occupational health and safety training programs for nurses are limited (Tiwari, Sharma, Zodpey, & Patel, 2015). India does not publish statistics regarding the number of practicing occupational health nurses or their area of work (Tiwari, Sharma, Zodpey, & Khandare, 2014). To the researchers’ knowledge, few occupational health nurses are currently practicing in India. However, in almost all textile factories, a nurse, trained in General Nursing and Midwifery (GNM), is appointed as the “industrial nurse.” Her job most commonly includes providing primary care to employees with illnesses.
In view of the substantial number of employed adolescent and young women suffering from mental health conditions such as depression and behavioral problems, occupational health nurses are needed in Indian textile factories to identify mental health disorders and suicide risk among employees and provide counseling, behavior therapy, and referrals for other health care treatment. Occupational health nurses might also involve human resource departments and unions in providing mentally safe environments for adolescent and young women workers considering the abuse that has been reported at workplaces. Mental health promotion (e.g., building resilience and coping skills, improving communication, endorsing positive behaviors, and modifying lifestyle risks) could also be provided by occupational health nurses.
Conclusion
Mental health problems such as depression, suicide risk, and behavioral problems are more likely among employed adolescent and young women who worked or had worked in the textile industry in Tamil Nadu compared with never employed adolescent and young women. Further studies are needed to assess the pattern and causes of mental health problems in this population.
Applying Research to Practice
Adolescent female employees are at high risk for mental health problems such as depression and behavioral problems. Occupational health teams at workplaces should prevent, screen, and treat mental health conditions through provision of safe work places, life skill education, and counseling and referral services. Simple screening tools for depression, behavioral problems, and abuse must be developed for use at workplaces. Annual health examinations could include mental health screening and promotion of positive mental health. Employees should be made aware of the laws in relation to prevention of workplace harassment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Nancy Angeline Gnanaselvam is a faculty member in the Department of Community Health, St. John’s Medical College. She has a passion for women’s health, and she works toward the betterment of working women’s lives.
Bobby Joseph is a professor and Head of the Department of Community Health, Division of Occupational Health Services, St. John’s Medical College. His areas of interest include primary health care and work-related health of employees in plantation, apparel, and health care settings.