
Abstract
This study aimed to evaluate the impact of a simulation-based Advanced Life Support (ALS) training programme on the self-efficacy and communication of health personnel. The research focussed on whether such training could enhance both technical and non-technical skills, particularly in managing cardiopulmonary resuscitation (CPR) situations. A quasi-experimental pre- and post-intervention study was conducted in primary care centres across Andalusia, Spain. A total of 106 health personnel (doctors and nurses), aged 21 to 65 years, participated in the study. Participants completed questionnaires measuring self-efficacy and communication styles before and after a 27-hour blended ALS training programme, which incorporated high-fidelity simulation exercises. Communication was assessed across several dimensions, including expressiveness, preciseness, impression manipulativeness, and emotionality. Post-intervention analysis revealed significant changes in communication styles. Specifically, doctors exhibited a reduction in “impression manipulativeness,” while nurses showed an increase in “expressiveness.” Although self-efficacy scores improved slightly after the training, the changes were not statistically significant. Correlational analyses indicated that higher self-efficacy was positively associated with “expressiveness” and “preciseness,” and negatively associated with “emotionality.” In conclusion, simulation-based ALS training led to improved communication among health personnel, with distinct patterns emerging between doctors and nurses. While the simulation training did not significantly increase self-efficacy, the trends observed suggest potential benefits. These findings support the inclusion of simulation in continuing professional development programmes to strengthen non-technical skills essential for effective CPR performance.
Introduction
Cardiorespiratory arrest is a significant public health challenge. According to the OHSCAR registry, their incidence in Spain is 18.6 per 100 000 inhabitants in out-of-hospital settings and is estimated at 22 300 cases per year in hospitals. 1 Cardiopulmonary resuscitation (CPR), fundamental to reverse these situations, requires specialized skills for its advanced version. 2 The quality of CPR is determinant in the survival and recovery of these emergencies, 3 and its effectiveness is reinforced by previous experience and training in CPR. 4 Simulation programmes have been shown to be effective in medical training to improve these skills. 5
Simulation training for CPR allows realistic situations to be recreated, optimizing knowledge acquisition. 6 This approach overcomes the limitations of traditional methods and is effective in improving CPR skills in the short and long term. 7 It facilitates the transfer of knowledge to real-life contexts and the acquisition of technical and personal skills.7,8 Post-simulation feedback is crucial for perfecting techniques and overcoming errors, 9 gaining importance in CPR training and emphasizing personal skills. 10 The structured debriefing and immersive experience offered by simulation have proven effective in producing behavioural changes, as seen in controlled trials evaluating sedation crisis scenarios. 11
A challenge in CPR training is to prepare professionals not only in clinical skills but also in practical application under pressure and teamwork. 12 Stærk et al 13 identified common barriers to resuscitation, including lack of contextualized knowledge and training and non-technical skills. The performance of professionals depends not only on their knowledge, but also on cognitive and emotional abilities in critical situations, emphasizing the importance of psychological aspects in training. 10
Non-technical Skills of Health Personnel During Life Support
In the context of Life Support, the non-technical skills of health personnel are crucial to reduce adverse outcomes and improve the clinical management of teams. 14 Managing medical emergencies requires not only technical knowledge, but also psychological skills such as self-efficacy 10 and effective communication. 15 In accordance with Bandura et al’s 16 social cognitive theory, self-efficacy refers to an individual’s perception of their own ability to successfully address a variety of situations. Self-efficacy determines the extent to which health personnel trust their capacity to act in emergency contexts. Therefore, promoting self-efficacy within medical teams is essential for managing potentially challenging situations. 17
Lack of confidence among health personnel is one of the main barriers to achieving high-quality CPR, 18 as it can inhibit CPR performance even when individuals possess the knowledge required to carry it out. 2 Moreover, low self-efficacy has been linked to job satisfaction. 19 Similar protective effects of self-efficacy on mental health and stress management have been observed in other high-demand professional contexts. 20 Communication gaps, especially in emergencies, can decrease performance and increase adverse events, 8 being a key skill in critical situations such as cardiorespiratory arrest. 21
Communication styles are verbal and non-verbal interaction patterns that appear in individuals in a relatively stable manner. 22 These styles represent specific ways of engaging and managing interpersonal relationships, and they are linked to mental states and intentions that manifest through words and non-verbal cues. 23 When identifying communication styles, one of the most relevant instruments is the tool developed by de Vries et al, 24 which has been validated among health personnel, 25 revealing 6 communication styles: expressiveness (fluid, relaxed communication with humour and confidence in conversation), preciseness (characterized by structured, concise exchanges highlighting essential aspects), verbal aggressiveness (referring to hostile, distant, authoritarian, and disrespectful communication towards others), questioningness (involving thorough exploration of details and constant verification to confirm one’s own point of view), emotionality (marked by sentimentalism, tension, worry, and defencive attitudes), and impression manipulativeness (involving the use of compliments or praise while simultaneously withholding information to generate a specific perception). Ineffective and aggressive communication among professionals involved in resuscitation efforts is one of the main barriers to effective performance. In contrast, precise communication facilitates task coordination and team confidence during the CPR process. 26
Simulation training fosters a holistic learning scenario, where cognitive and emotional reactions, conflicts and doubts are addressed. 8 This training improves technical and psychological skills in multidisciplinary healthcare teams. 15 Studies such as Lavelle et al 15 and Dewolf et al 21 have shown improvements in personal competencies and communication between health personnel.
Nurses and physicians, first responders in cardiorespiratory arrest, require training in CPR not only technical but also personal competencies such as self-efficacy and communication for optimal performance.27,28
Study Aim
The purpose of this study is to evaluate the effectiveness of a simulation-based training programme for Advanced Life Support, focussing specifically on how such a programme affects the communication styles and self-efficacy of health personnel. Our main hypothesis is that participation in this training programme will result in significant improvements in both communication skills and self-efficacy of these professionals.
Materials and Methods
Study Design and Sample
A quasi-experimental study with a pre- and post-intervention evaluation was conducted following the TREND Statement. 29 The sample consisted of doctors and nurses working in primary care health centres in Andalusia (Spain). Participants were selected by consecutive non-probability sampling, including all individuals who enrolled in Advanced Life Support training. In total, a group of 106 health personnel aged 21 to 65 years participated.
The inclusion criteria were: (1) having completed studies in Medicine or Nursing; (2) practising at the time of the intervention in Primary Care Centres of the Andalusian Health Service; and (3) having completed the questionnaires in full on 2 occasions, before and after the intervention.
Questionnaire Design
An ad hoc questionnaire was used to collect socio-demographic and employment data: age, sex, education, profession, and length of service/experience in the profession.
To evaluate communication style, the Communication Style Inventory Revised (CSI-R) 25 was used. This is a questionnaire validated in the Spanish population that measures the predominance of certain communication behaviours through 21 items, with a Likert scale response mode (1 = strongly disagree and 5 = strongly agree). It provides information on 6 communication styles: Verbal aggressiveness or hostile, cold, authoritarian, and disrespectful communication with the other person; Impression manipulativeness, when personal charm, flattery, or concealment information is used to obtain some benefit.; Questioningness, where detail is sought and to corroborate one’s own point of view; Expressiveness, in this case the person converses in a relaxed manner, with humour and a mastery of dialogue; Emotionality or communication loaded with sentimentality, tension, concern, and defencive attitudes; Preciseness or the way in which a person structures their communication by being concise and pointing out the important aspects. In this work, the internal consistency indices presented adequate values for the different subscales: Verbal aggressiveness (ω and GLB = 0.72); Impression manipulativeness (ω and GLB = 0.75); Questioningness (ω = 0.62 and GLB = 0.72); Expressiveness (ω and GLB = 0.73); Emotionality (ω and GLB = 0.70); and Preciseness (ω and GLB = 0.74).
Self-efficacy was assessed using the General Self-Efficacy Scale. 30 This scale is validated in Spanish people. It’s composed of 10 items with a Likert-type response format that assesses a person’s perception of his or her own personal competence to effectively handle different stressful situations. In the present study, the internal consistency indices for the scale showed optimal values (ω = 0.86 and GLB = 0.91).
Procedure
The general procedure of this research work complies with the TIDieR guidelines 31 ensuring transparency and reproducibility of the intervention. The programme was structured into 4 consecutive phases, guiding participants from the initial access to training through to the final evaluation of learning outcomes.
Access to training: In the first phase, an e-learning approach was implemented to provide remote access to training. This allowed participants to become familiar with the basic concepts and adequately prepare for the practical sessions. The online component offered flexibility and ensured a homogeneous level of prior knowledge among participants.
Pre-Training Assessment: The second phase was conducted through questionnaires distributed before the start of the course. These instruments established a baseline of knowledge and skills, serving as the pre-test measure against which subsequent progress could be evaluated.
Implementation of the Training Programme: The third phase involved the implementation of the training programme, which focussed on an Advanced Life Support (ALS) course with a total duration of 27 h. The course combined 15 h of e-learning with 12 h of face-to-face sessions, delivered over 3 days. Content was organized into 5 thematic blocks, following the recommendations of the European Resuscitation Council (ERC), and addressed essential aspects of cardiac arrest management. Of the 12 in-person hours, 9.5 were dedicated to high-fidelity simulation, during which participants worked in rotating groups of 8. This design ensured that all participants received equal exposure to the simulated scenarios, thereby promoting the acquisition of practical competencies under realistic yet controlled conditions.
The training was delivered by ERC-accredited instructors, operating under a standardized quality assurance system to guarantee consistency across courses. This system includes a rigorous instructor accreditation process, supervision of each course by a director responsible for quality control, and mandatory recertification every 3 years—failure to comply results in the loss of instructor status. The teaching team was composed of an experienced course director and several instructors from nursing and medicine, who contributed expertise in airway management and clinical simulation. The ALS course was organized by IAVANTE, in collaboration with the Ministry of Health of the Andalusian Regional Government, the Spanish CPR Council, and the European Resuscitation Council, during the first half of 2022.
Post-Training Evaluation: finally, participants completed questionnaires again to assess changes in knowledge and skills, providing the post-test measure and enabling comparison with baseline results.
Overall, the procedure was characterized by a blended methodology that integrated online learning, intensive face-to-face practice, and high-fidelity simulation, all under strict quality standards. This design ensured not only the acquisition of technical competencies in cardiac arrest management but also the reliability and consistency of the outcomes obtained (Figure 1).
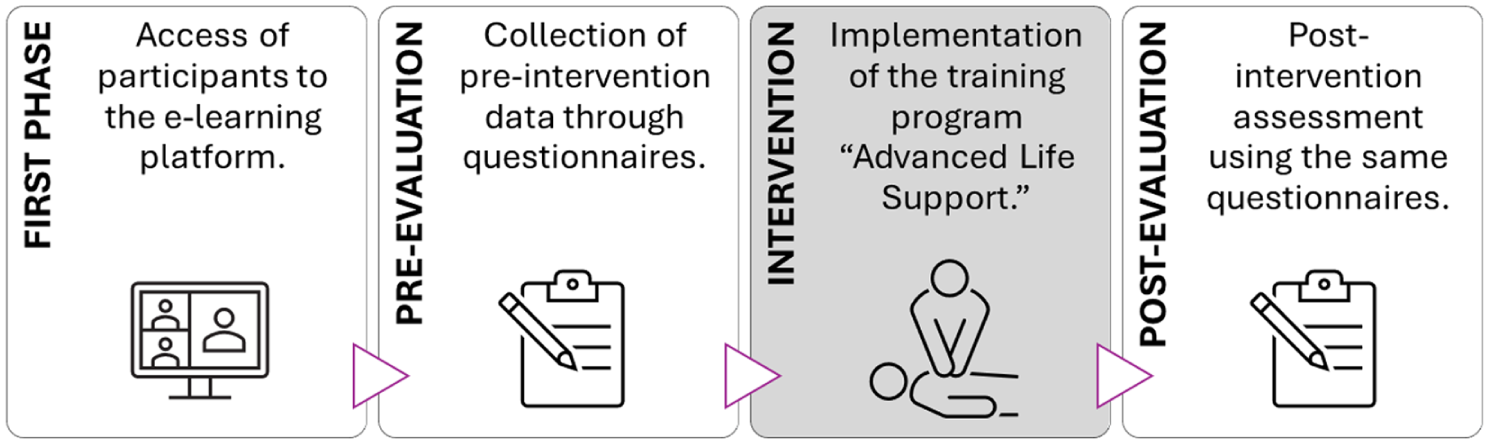
Programme phases.
Ethics
The research was approved by the Committee of Bioethics of the University of Almería with reference UALBIO2023/025 and the study adhered to the World Medical Association’s Code of Ethics (Declaration of Helsinki). The professionals targeted for this training were approached by the course director, who explained the study’s objectives. They were then asked to give their consent to participate. If the professionals chose not to be part of the research study, they could still engage in the training programme without their data being collected, ensuring their educational experience remained unaffected.
Statistical Analysis
Firstly, the normal distribution of the study variables was assessed, obtaining P > .05 in the Kolmogorov-Smirnov test. It is confirmed that the distribution of the data analysed did not meet the assumption of normality, therefore, non-parametric tests were used. A value of P < .05 was considered statistically significant. Analyses were performed with SPSS (Version 24, IBM, Armonk, USA).
Firstly, in order to check the relationship between the study variables (communication styles and self-efficacy), bivariate correlation analyses were carried out, taking into account the 2 measurement moments (pre and post). The correlation was assessed with Spearman’s correlation coefficients. To estimate effect size (p) and statistical power (1 − β), G*power (v. 3.1.9.4) was used, taking as reference values for effect size: 0.10 small, 0.30 medium, and 0.50 large. 32
To test for variations in communication style and self-efficacy scores before and after participation in the programme, a Wilcoxon signed-rank test was used. In addition, the effect size was estimated using the rank-biserial correlation measure (rrb), considering the following cut-off points: .10 small, .30 medium, and .50 large. 33
To examine the reliability of the instruments used for data collection, McDonald’s Omega coefficient is estimated, following the proposal and indications of Ventura-León and Caycho. 34 In addition, the Greatest Lower Bound (GLB) is estimated.
Results
Table 1 shows the data relating to the characteristics of the sample, together with the breakdown of the characteristics according to the distribution by professionals (medicine and nursing). With ages ranging from 21 to 65 years (corresponding to the working age of a professional who has completed their studies), the mean age of the participants was 44.71 years. Of the total sample, 62.26% were female, with a higher representation in both professions: 58.82% in medicine and 64.45% in nursing were women. In terms of work experience in the practice of the profession, an average of 18.42 years was observed for the total sample, with the nursing subsample having more years of experience (21.79 years) than the doctors (14.69 years of experience).
Socio-demographic Characteristics of the Sample.

Experience in practice in years.
Communication Styles and Self-Efficacy: Correlational Analyses
To find out whether the communication dimensions were related to general self-efficacy, a Spearman correlation was carried out, for each of the measures (pretest and posttest) the correlation coefficients, statistical significance (sig.), effect size (p), and statistical power (1 − β) can be seen in Table 2.
Correlations of Communication Styles with Self-efficacy in the Pre-test and Post-test. Total Sample and by Groups According to Profession.

Note. p = effect size (0.10 small, 0.30 medium, 0.50 large); 1 − β = statistical power.
Sig. < .05, **Sig. < .01, ***Sig. < .001.
The results obtained in the correlation test for the total sample (N = 106) show that there is a positive association of 2 of the communication styles (Expressiveness and Preciseness) with respect to self-efficacy that is maintained in both measures (pre and post), with large effect sizes, indicating that the magnitude of these relationships is important and relevant. On the other hand, the positive association between Questioningness and self-efficacy, with a medium effect size, starts to be significant before participation in the programme and, after the end of the programme, the correlation is lost. On the other hand, there is a negative association between Emotionality communication style and self-efficacy. The effect size is medium in the pretest and reaches a large magnitude in the posttest.
Furthermore, for the total sample, the absence of correlations between the study variables and years of experience was verified in the pre-intervention measure. However, post-intervention, positive associations could be observed between self-efficacy and the communicative styles: Impression manipulativeness (Spearman’s rho = 0.32, sig. < .01, P = .56, 1 − β = .99) and Questioningness (Spearman’s rho = 0.21, sig. < .05, P = .45, 1 − β = .99).
Looking at the profession, in the group of doctors (n = 51), positive associations were observed in the pretest between the communicative styles: Impression manipulativeness, Expressiveness and Preciseness, and self-efficacy, in all cases with large effect sizes. After doctors’ participation in the training programme, the association with self-efficacy that remains significant is Preciseness.
On the other hand, in the group of nurses (n = 55), a negative association is observed in the pretest between Verbal aggressiveness and self-efficacy, with a large effect size. However, this association is not observed in the posttest measure. Furthermore, in the pre- and post-test measures, in the group of nurses there are positive correlations between the communication styles: Expressiveness, Emotionality and Preciseness, and self-efficacy. In all cases, the effect sizes are large, which indicates that the magnitude of these relationships is important and relevant.
Effects of the Training Programme on Communication Styles and Self-Efficacy
Table 3 shows the results obtained for the study variables in the different measures (pre/post): descriptive statistics and the Wilcoxon test for non-parametric analysis of related samples. Statistically significant differences were found between the measurements taken before and after participation in the simulation training programme for basic life support training. Specifically, it can be observed that for certain communication styles such as Impression manipulativeness, the mean scores decreased significantly after participation in the training programme, with a medium effect size (rrb = 0.31). On the other hand, participants showed higher scores for Expressiveness after completing the programme sessions, with statistically significant differences from the pretest measure, with a medium effect size (rrb = 0.36).
Communication and Self-efficacy. Paired Samples Wilcoxon’s Test (N = 106).

Note. M = mean; SD = standard deviation; W = Wilcoxon signed-rank test.
Sig. < .05, **Sig. < .01.
Table 4 presents the results of the non-parametric analyses of the Wilcoxon test for the group of doctors. In this case, it is observed that the communication style Impression manipulativeness shows a significant decrease, with a medium effect size (rrb = 0.38) after participation in the training programme, compared to the scores obtained in the pre-test.
Communication and Self-efficacy. Paired Samples Wilcoxon’s Test (Doctors n = 51).

Note. M = mean; SD = standard deviation; W = Wilcoxon signed-rank test.
Sig. < .05.
Table 5 presents the results for the group of nurses. In this case, a significant improvement in Expressiveness scores is observed, with a medium effect size (rrb = 0.35) after participation in the training programme, compared to the scores obtained in the pre-test. From the positive rank test (post-test > pre-test), it could be observed that 26 out of 55 nurses participating in the training programme obtained better Expressiveness scores after the training.
Communication and Self-efficacy. Paired Samples Wilcoxon’s Test (Nurses n = 55).
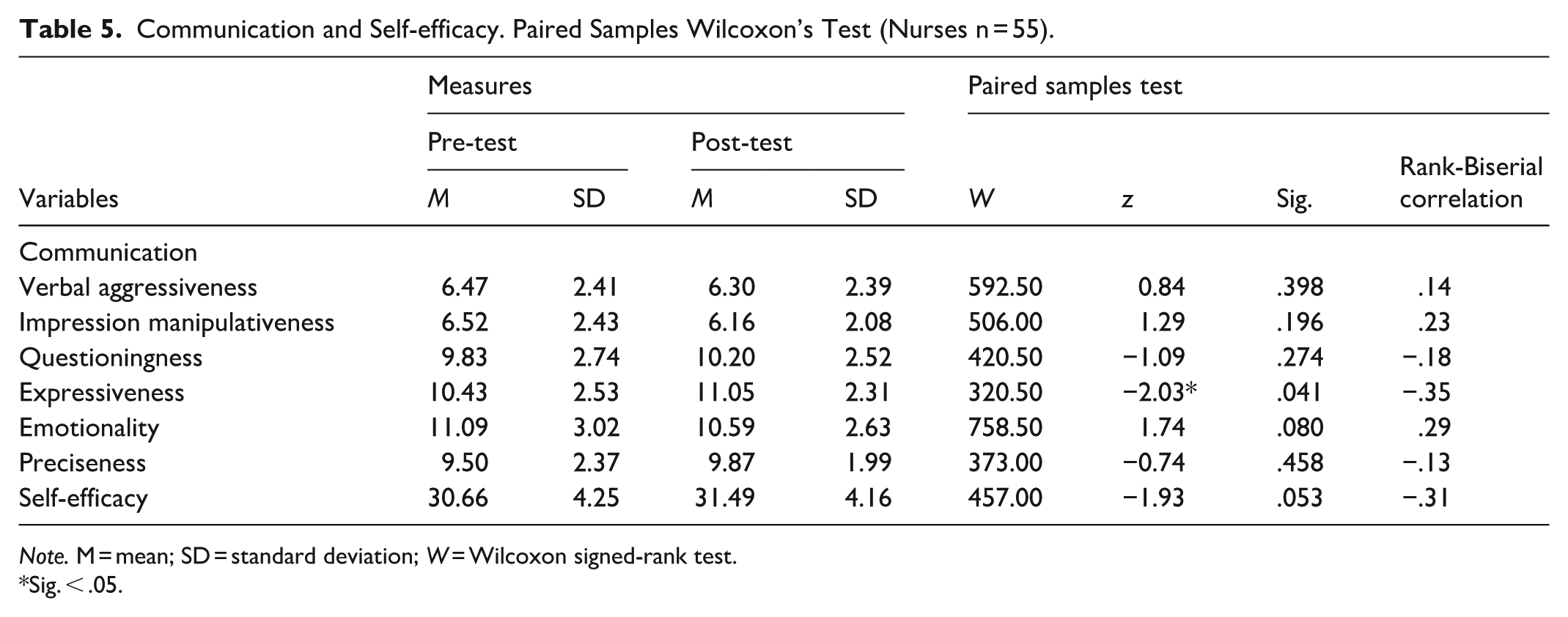
Note. M = mean; SD = standard deviation; W = Wilcoxon signed-rank test.
Sig. < .05.
Discussion
Existing research has established a direct connexion between the effectiveness of cardiopulmonary resuscitation (CPR) and subsequent patient outcomes, highlighting the crucial importance of the quality of resuscitation. 3 Furthermore, it is stressed that in order to effectively perform CPR, it is essential that health personnel are adequately educated and trained in these techniques. 4 However, effectiveness in emergency situations depends not only on technical knowledge but also on psychological skills such as communication and a sense of self-efficacy.10,12,13 In this context, our quasi-experimental study focussed on assessing how a life support simulation programme affects communication styles and self-efficacy in health personnel.
We first analysed the association between communication styles and self-efficacy. Positive correlations were identified between self-efficacy and communication styles expressiveness and preciseness, while the relationship with emotionality was negative at both points in time. These relationships suggest that higher perceived confidence in managing stress is associated with clearer and more controlled communication. Interestingly, the initial positive correlation between questioningness (characterized by asking many questions in order to obtain confirmation of one’s view) and self-efficacy disappeared after training, which may indicate that training improved self-efficacy and effective communication, reducing the need to seek external confirmation. This change aligns with the findings of Navalpotro et al, 2 who observed an improvement in self-efficacy and a reduction in behaviours that inhibited or delayed CPR after training, such as asking multiple corroborating questions.
When analysing the groups of doctors and nurses separately, differences in the results were observed. In the case of the doctors, the pre-test revealed positive relationships between self-efficacy and the communication styles Impression manipulativeness, Expressiveness and Preciseness. However, post-intervention, only the relationship between self-efficacy and Preciseness remained significant. This suggests that, for clinicians, a sense of efficacy was associated with structured and focussed communication on key issues, both pre- and post-training. After the simulation, the communication style involving pleasing the interlocutor by withholding information was no longer associated with self-efficacy. This could indicate that the training led doctors to associate greater efficacy with more direct and honest communication. Following Bolton et al, 35 coordination and problem-solving within teams composed of professionals with interdependent roles are enhanced when timely and precise communication is present. Therefore, healthcare teams facing a CPR situation may improve their coordination and performance when the physician adopts a transparent and rigorous communication style. In this regard, a study conducted with a specialized neonatal resuscitation team found that professionals consider effective communication from the leader to be the most important asset in the team’s performance. 36 Perceived self-efficacy in communicating with patients is also crucial for patient outcomes and satisfaction and has been found to be positively related to physician experience. 37 Furthermore, it has been observed that more satisfied cardiac patients with a positive outlook tend to follow medical recommendations better, 38 highlighting the importance of effective communication on long-term outcomes.
In the nursing group, before the simulation, self-efficacy was found to be positively related to Expressiveness and Preciseness communication styles, but negatively related to Emotionality and verbal aggressiveness. After the intervention, these relationships were maintained, except for verbal aggressiveness, which was no longer negatively associated with self-efficacy. This suggests that the training helped nurses to dissociate efficacy from a cold and authoritarian communicative approach. Given that nurses often initiate CPR before the arrival of the medical team, 38 training that encourages accurate communication away from aggressiveness and tension is crucial for successful management in the critical moments of cardiorespiratory arrest.
The effects of the training programme “Advanced Life Support” on the communication styles of health personnel were evaluated. Overall, changes in Impression manipulativeness and Expressiveness communication styles were noted. Specifically, physicians showed a significant decrease in Impression manipulativeness, indicating a reduction in communication that combines flattery with withholding information. On the other hand, nurses experienced significant improvements in Expressiveness, implying more controlled and effective communication. These changes are especially relevant in nursing, where effective communication is fundamental not only in CPR, but also in the interaction with patients, families, and the care team.39,40 Furthermore, it is highlighted that strengthening accurate and empathic communication styles can positively influence professional relationships and job satisfaction, as well as the quality of patient care.
As previously discussed, the training produced different effects on the communication styles of doctors and nurses. This may be related to their distinct professional roles. In interprofessional emergency teams, doctors are responsible for leading the medical team, managing tasks, and making decisions. 41 Meanwhile, nurses take an active role within the team, contributing significantly to multiple aspects of resuscitation, including team dynamics, outcomes, patient safety, and clinical communication with patients and families. 42 Enhancing resuscitation training for health personnel may strengthen their professional identity, leading doctors to assume leadership roles without the need to manipulate the rest of the team. In the case of nurses, such training may foster improvements in team dynamics and communication with colleagues and families through a more expressive communication style.
Although pre- and post-intervention results on self-efficacy showed no significant statistical differences, an improvement in mean scores was observed in both nurses and doctors. This suggests a potentially positive impact of the intervention. Nevertheless, this trend should be interpreted with caution. The relevance of self-efficacy, particularly in high-stress situations, is essential in healthcare practice. Stærk et al 13 highlight the importance of including non-technical skills in life support training. Although the improvement in self-efficacy was inconclusive, simulation-based training remains valuable in developing psychological competencies in health personnel. This type of training has been shown to be effective in the acquisition of behavioural, cognitive, and emotional management skills, being a positive and successful learning tool. 7
Finally, we agree with Fraga-Sampedro 7 on the importance of promoting simulation-based life support training in interdisciplinary teams, especially because cardiopulmonary resuscitation is a task that requires the collaboration of different specialists. Coordination and communication within the team are essential, and simulation training has been shown to be effective in developing psychological and emotional competencies in these settings. 15 Our study highlights the need to approach certain competencies, such as communication styles, differently between doctors and nurses, given the different roles they play in care teams.
Among the limitations of our study, it is important to mention the absence of a scale to determine the initial level of self-efficacy of the professionals. This limitation could explain the lack of significant changes in this variable, as it is possible that the initial levels of self-efficacy were already medium or high, thus limiting the observation of notable improvements. In future research, it is recommended not only to assess self-efficacy, but also to establish its initial range in order to determine the need for training in this area. Another significant limitation was the lack of a control group. For future studies, it is suggested to include a sample of professionals not participating in the training intervention, which would allow for a more effective comparison of results and more robust conclusions. In addition, the non-probability consecutive sampling limits the generalizability of the results, and the diversity of the sample, centred in Andalusia, Spain, could affect the applicability in different contexts. The variety in the professional experience of the participants and the absence of long-term follow-up are important aspects to consider. The study also relied on self-assessment of competences, which may be subject to self-perception bias.
These findings point to specific actions that can enhance clinical training outcomes. First, incorporating simulation training as a standard part of continuing professional development can significantly improve healthcare teams’ ability to respond in cardiopulmonary emergencies. Programmes should be designed to explicitly address communication strategies and team dynamics, particularly differentiating approaches for doctors and nurses based on their roles.
Second, simulation environments should be leveraged not only for procedural learning but also for developing resilience and psychological preparedness. Providing realistic, emotionally charged scenarios helps build confidence and reduces reliance on counterproductive communication styles, such as manipulativeness or emotional defensiveness.
Finally, healthcare institutions and education bodies should invest in interdisciplinary simulation-based training as a long-term strategy to improve coordination, decision-making, and ultimately, patient outcomes. Embedding these practices into organizational culture can ensure sustained improvement in both technical performance and soft skills.
Conclusions
Successful management of cardiorespiratory arrest requires health personnel to possess both clinical and psychological competencies. Often, training programmes focus on clinical aspects, leaving out psychological aspects. Our study highlights that simulation training in Basic Life Support is effective in improving the communication style of doctors and nurses, a skill often underdeveloped according to previous studies.
Future research should look further into the improvement of personal competencies through simulation-based continuing education. It is crucial to assess the initial needs and demands of staff in order to establish an adequate baseline. The results suggest that designing specific programmes to develop personal skills requires a detailed prior analysis and considering the profession as a key differentiating factor.
Simulation training can strengthen communication and self-efficacy of health personnel. It provides a practical environment where skills can be practised under pressure. Although changes in self-efficacy were not significant, the improvements observed indicate a potential positive impact of simulation on the perception of self-efficacy especially in nurses, which is crucial in stressful situations such as CPR.
This study contributes to clinical practice by highlighting the importance of non-technical skills in the training of health personnel. Improved communication and self-efficacy, achieved through simulation training, is vital for the effective management of critical situations such as cardiorespiratory arrest. These advances can lead to better coordination of the healthcare team, more effective decision-making and, ultimately, better patient care. By emphasizing the relevance of these skills, the study underscores the need to incorporate simulation training into the educational curriculum of health personnel, not only to improve their technical skills but also to strengthen psychological competencies essential for high-quality care.
In conclusion, these findings support the efficacy of simulation training in improving communication skills and self-efficacy in health personnel, positively impacting patient care and the management of critical situations.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251411471 – Supplemental material for Self-efficacy and Communication in Health Personnel After Simulation Training in Cardiopulmonary Resuscitation: A Quasi-experimental Study
Supplemental material, sj-docx-1-inq-10.1177_00469580251411471 for Self-efficacy and Communication in Health Personnel After Simulation Training in Cardiopulmonary Resuscitation: A Quasi-experimental Study by María del Carmen Pérez-Fuentes, María del Mar Molero Jurado, Armando Romanos-Rodríguez, África Martos Martínez, Francisco J. Gómez-Gómez and Javier Aguado-Campos in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
Collaboration Agreement between the University of Almería and IAVANTE-Progress and Health Foundation, Andalusian Regional Health Ministry for the Research Project to “Analyze personal competencies involved in training processes based on the use of simulation, in the health field”.
Ethical Considerations
The study involving human participants was approved by the Committee of Bioethics of the University of Almería with reference UALBIO2023/025 and the study adhered to the World Medical Association’s Code of Ethics (Declaration of Helsinki). The studies were conducted in accordance with the local legislation and institutional requirements.
Consent to Participate
Informed consent was obtained from all subjects. In addition, the professionals targeted for this training were approached by the course director, who explained the study’s objectives. They were then asked to give their consent to participate. If the professionals chose not to be part of the research study, they could still engage in the training program without their data being collected, ensuring their educational experience remained unaffected.
Author Contributions
All individuals who have made a significant contribution to the work have been recognized as authors, and that all authors have reviewed and approved the final version of the manuscript and agreed to its submission. The specific contributions of each author are as follows: María del Carmen Pérez-Fuentes, María del Mar Molero Jurado, África Martos Martínez: Writing – original draft, Methodology, Formal analysis, Data curation, Conceptualization, Writing – review & editing, Software, Investigation, Data curation. Supervision, Resources. Armando Romanos-Rodríguez, Francisco J. Gómez-Gómez, Javier Aguado-Campos: Project administration, Conceptualization, Methodology, Investigation, Writing – review & editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
All data pertaining to this research article are included within the manuscript as written.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.