
Abstract
Climate change and mental health research has predominantly focused on adults in non-clinical settings; investigations among youth and in clinical settings are lacking. Our objectives were to understand the relationship between adult caregiver and adolescent patient climate-anxiety and to examine caregivers’ community-level concerns and their association with adolescent climate anxiety. This cross-sectional study occurred in a single-center pediatric emergency department (ED) and data collection spanned January to December 2024. Exposures included adolescent demographic factors (age group, sex, race and ethnicity, insurance payor) and adolescent and caregiver general anxiety disorder-7 (GAD-7) scores, as well as caregiver perspectives captured on (1) the climate change anxiety scale (CCAS), (2) a domestic and global issues poll, and (3) an environmental community survey. The outcome was adolescent climate anxiety, operationalized using the CCAS. In total, 557 patient-caregiver dyads completed CCAS surveys, with low within-dyad agreement in scores, ICC = 0.224 (95% CI 0.142, 0.274). Both caregivers and adolescents had higher levels of climate anxiety if the caregiver reported concerns about housing, public services, and pollution in their community (P < .05). Moderate-severe generalized anxiety (GAD-7) was the strongest predictor of climate anxiety in both adolescents and caregivers (ORadj 6.59, 95% CI 3.52-12.30, P < .001). Caregivers viewing climate change as very important had higher odds of moderate-severe CCAS (ORadj = 4.50 (95% CI 2.03, 9.98), P < .001), with no significant effect of their perception on adolescent CCAS (P = .172). Generalized anxiety and adult caregiver community-level concerns appear to be associated with adolescent climate anxiety in this large pediatric study, but there is no direct relationship between caregiver climate anxiety and the climate anxiety of the adolescent.
Introduction
The adolescent period is defined by physical, social, and cognitive changes in development which drive emotional responses and sensitivity to world issues. 1 Today’s youth in the United States are exposed to highly publicized and reported severe global weather and climate events, with 85% feeling at least moderately worried about climate change, 42.8% reporting climate change impact on their mental health, and 38.3% acknowledging that their feelings about climate change negatively affect their daily life and functioning.1,2 Despite these alarming statistics, the mechanisms underlying youth anxiety about climate change remain poorly understood.
Climate anxiety is defined as heightened emotional, mental, or somatic distress in response to detrimental changes in the climate.3,4 It represents a specific form of eco-anxiety, the broader construct encompassing distress about negative environmental changes in general, including pollution and biodiversity.2,4 While climate- and eco-anxiety are often used interchangeably in the literature, we focus specifically on climate change-related anxiety. In addition to being a psychological descriptor, the term climate anxiety has been operationalized as a psychometric construct in the climate change anxiety scale (CCAS), increasingly implemented in samples of young people.5 -9 Climate anxiety represents a growing mental health crisis among young people: climate-related events are associated with posttraumatic stress, sleep disruption, depression, and anxiety. 10 These disastrous events also can disrupt caregiving and family functioning as stressors such as loss of financial, food, and housing resources can wear on familial relationships and connectivity. 10
Despite growing recognition of climate anxiety as a public health concern, 4 critical gaps persist in the literature. First, research has focused predominantly on adult populations in non-clinical settings (Supplemental Table 1). 11 Second, there is no widely validated youth-focused instrument for measuring climate anxiety, though the adult CCAS has been recently applied to adolescent samples. 5 Third, the familial transmission of climate anxiety remains unexplored, with few studies investigating the interaction between parental climate perspectives and those of the adolescent child.12,13 Fourth, the role of socioeconomic and community resources – such as housing quality, food security, access to public services – in shaping youth climate anxiety has not been systematically investigated, although youth in underserved, low-resource communities are particularly susceptible to climate anxiety. 14
The primary objective of this clinical study was to identify factors affecting climate anxiety in adolescent patients and adult caregivers. The secondary objective was to characterize caregivers’ community-level concerns and their association with climate anxiety (as measured on the CCAS) in both adolescents and caregivers. A familial dyad-based approach is expected to provide insight on intra- and interpersonal, as well as community level factors contributing to climate anxiety.
Methods
Study Design
This study utilized a cross-sectional design in a single emergency department (ED) of a free-standing pediatric hospital in Southern California. Adolescents ages 12 to 17 years of age who presented to the ED with medical and mental health chief complaints from January 8, 2024 to December 11, 2024 and were accompanied by an adult caregiver were included. Patients with an Emergency Severity Index (ESI) of 1 (most severe, acute medical or trauma presenting complaint) or on a 72-h involuntary psychiatric hold (eg, 5585 hold) were excluded. A team of 32 trained study personnel completed an IRB-approved verbal consent procedure after sharing a study information sheet with adolescent patient participants and their adult caregiver, collecting data on REDCap (Research Electronic Data Capture) via digital tablet.
We utilized a convenience sampling approach between the hours of 8am and 10pm, 6 days a week, during 12 contiguous months and no monetary compensation was offered. The surveys are described in the following sub-section. Surveys were available in English and Spanish for caregivers, with the Spanish surveys prepared through a certified Spanish translator. Data collectors were immediately alerted via a REDCap response if participants indicated an acute mental health concern such as suicidal ideation. A protocol was in place for the study investigator to alert a clinician to determine if a social worker intervention was needed. The Institutional Review Board approved all study activity (#230104).
Measures
Climate Anxiety
Both adolescent and caregiver participants completed the CCAS, a 13-item, five-point Likert-scale-based measurement of emotional and behavioral response to climate change, validated in adults (Appendix 1).15,16 The CCAS score is a measure of cognitive-emotional and functional impairment. The instrument was recently introduced in 2020; although it was not developed specifically for children, the CCAS has been implemented in youth under 18 years of age6 -9 and a shorthand youth version internally validated 5 – therefore, we utilized the CCAS among both our adult and pediatric samples in this study. In collaboration with the original scale developer (SC), wording of select items on the CCAS underwent minor adaptation – for example, simplifying the words “analyze” (item 7), “sustainability” (item 10), and “undermine” (item 12) in the original scale – to be implemented in readers as young as 12 years.
Internal consistency of all scale items was high in our sample (α = .92). We utilized established clinical thresholds and optimal Youden’s index with severe generalized anxiety (GAD-7 score ≥ 15) to categorize total CCAS scores (13-65) into 4 levels: minimal (≤18), mild (19-22), moderate (23-32), and severe (≥33). 17 Only complete CCAS survey data from adolescent-caregiver dyads were included; of 788 adolescents who completed the CCAS, 557 had a corresponding caregiver survey. A Spanish adaptation of the CCAS was recently validated in a Spanish population sample with high psychometric adequacy, Cronbach’s alpha coefficient, α = .87. 18
Generalized Anxiety
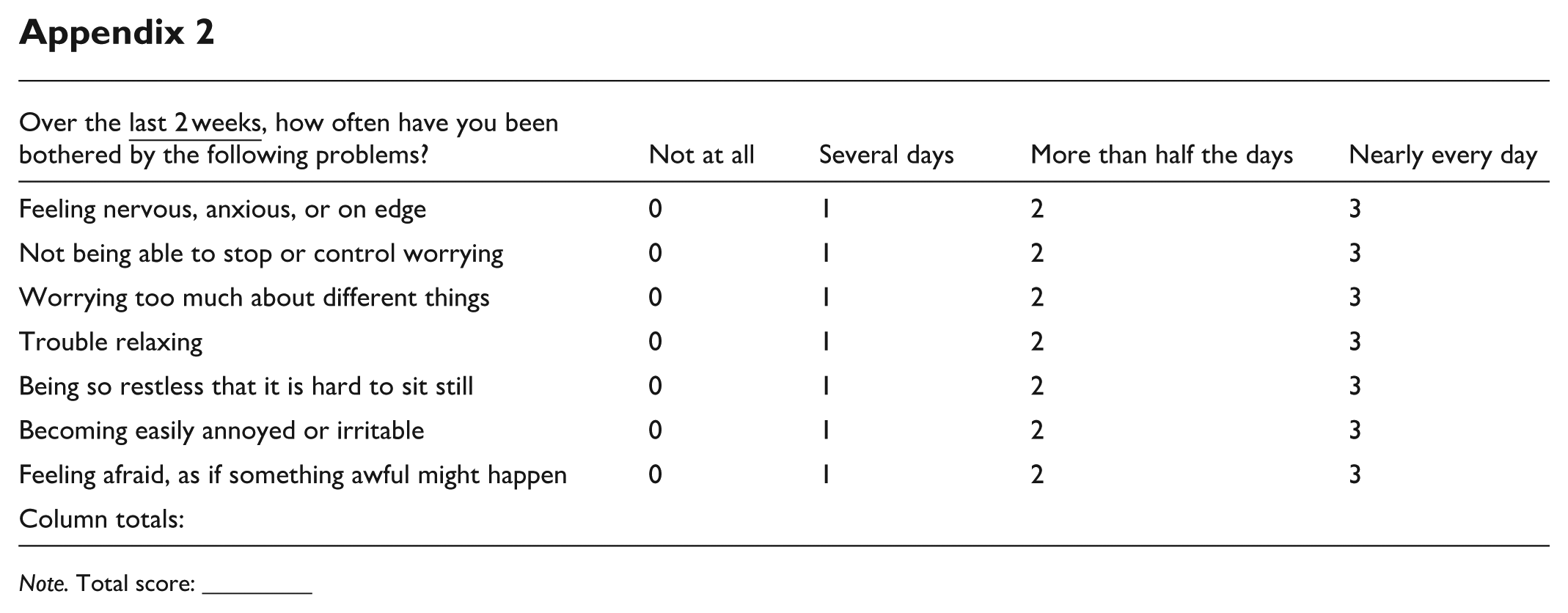
Both adolescent and caregiver participants completed the general anxiety disorder-7 (GAD-7), a widely implemented 7-item measure validated in general19,20 and pediatric populations 21 (Appendix 2). It is scored on a four-point Likert scale (maximum summative score = 21) with 4 levels of severity: not detected (<5), mild (5-9), moderate (10-14), and severe (≥15). Our sample yielded high internal consistency (α = .918).
Domestic and Global Issues
Only the caregiver participants completed the Washington Post-Kaiser Family Foundation Poll, an assessment of the perception of 8 common public policy domains 22 (Appendix 3). This measure was integrated to gage the perceived importance of climate change relative to other domestic and global issues. In the public poll, each item is tallied on a four-point Likert scale with an additional “No opinion” option. Among responses, we used a dichotomous variable to capture perceived importance (“very important” or “extremely important) or ambivalence (“somewhat important,” “not important,” or “no opinion”) of a given domain.
Community-Level Concerns
Only the caregiver participants completed an adapted version of the Alameda County Environmental Justice Community Survey, an assessment of 5 community-level domains: housing, public facilities, health and physical activity, access to healthy food, and pollution 23 (Appendix 4). We integrated this measure not just in recognition of climate change as a social driver of health (SDOH), 24 but also to gather contextual data of social and political forces that determine differential exposure to environmental harm and adversity among populations. Each item contains a variable amount of responses, and participants may select as many as apply to them.
Demographic Information
Demographic data was self-reported by the adult caregiver of the adolescent patient seen in the ED. Data – including patient gender, race and ethnicity, and insurance payor type (public or private) – was retrospectively extracted from the electronic medical record. Health insurance coverage type was used as a proxy for household income status.25,26 Categorization of the social construct of race and ethnicity (Hispanic, non-Hispanic) was based on the Office of Management and Budget Standards. 27 Multi-racial participants selected “Other” racial category, and missing racial data was categorized as “unknown.” Presenting chief complaints of the adolescent patient in our ED were categorized as medical, mental health, or psychosomatic. We defined the latter category as physical symptoms without an underlying medical condition or pathology identified on physical, laboratory, and/or imaging examinations and each patient case was reviewed by a pediatric emergency medicine physician (RRA) to determine appropriate category.
Statistical Analysis
Patient and caregiver characteristics were described in terms of counts and percentages with defined trait or mean (SD) for continuous variables. Climate change anxiety severity, categorized as: not detected, mild, and moderate–severe was described for adolescents and caregivers overall and across characteristics. The Stuart-Maxwell test compared CCAS distributions between roles (adolescents and caregivers) within each factor level, and Chi-square tests compared CCAS distributions across factors within each role.
We conducted mixed effects logistic regression to identify predictors of moderate-severe CCAS and to assess whether associations differed by role. The modeling procedure considered main effects for demographic and SDOH variables, as well as 2-way interaction terms with role. A random intercept was included to account for clustering within dyad. Terms included in the final model were selected based on a stepwise approach, in which variables were entered in order of significance from univariate analyses, and both main and interaction terms were retained if statistically significant at the .05 level. Forest plots were constructed using the ggplot2 package in R (version 4.4.2), based on model estimates generated with the lme4 and broom.mixed packages, to display adjusted odds ratios (ORs) and their 95% confidence intervals for fixed effects retained in the final model. ICC assessing agreement in CCAS score between adolescent and caregiver within each dyad was estimated using the performance package with weighted kappa reported on categorical scale. Descriptive statistics and univariate comparisons were performed using SPSS Statistics, version 29.0 (IBM Corp).
Results
Characteristics of the 557 adolescent patient-adult caregiver dyads are summarized in Table 1. The adolescent sample was racially and ethnically diverse, the majority of which presented with medical chief complaints (80.3%) and with public health insurance (59.8%). Detected levels of generalized anxiety among both adolescent and caregiver groups were widely distributed, ranging from not detected, mild, and moderate-severe. A total of 36 caregivers (6.5%) completed surveys in Spanish.
Description of the Family Dyads (Adolescent Patient and Adult Caregiver), n = 557.

Note. In 307 parents who responded to sex question: 80.5% identified as female.
Missing (n = 60).
A comparison of adolescent and caregiver CCAS score (not detected, mild, moderate-severe) by respondent characteristics via univariate analysis is presented in Table 2. Overall, the distribution of climate anxiety (not detected, mild, moderate-severe) was not significantly different between the adolescents and caregivers. Interestingly, we observed low within-dyad agreement in climate anxiety score on both a continuous scale (ICC = 0.224: 95% CI 0.142, 0.274), and on 3-point scale (weighted kappa (quadratic weights) = .249: 95% CI 0.158, 0.339). Notable demographic differences in CCAS among adolescents included higher rates of moderate-severe climate anxiety in females (21.2%) compared to males (12.4%), P = .014, and in those with public health insurance (21.0%) compared to private (11.1%), P = .009. Generalized anxiety in adolescents was strongly associated with their level of climate anxiety (proportion of moderate-severe climate anxiety in those with moderate-severe generalized anxiety vs no generalized anxiety (32.4% vs 7.4%, P < .001); this was also observed among caregivers (32.4% vs 9.3%, P < .001).
Comparison of Adolescent and Caregiver CCAS Overall and by Respondent Characteristics (Univariate Analyses).

Note. Superscript P-value next to variable name in first column was based on Chi-square test and assessed difference in CCAS level across factor levels within each role: A (adolescents), C (caregivers).
P-value in far right column was based on Stuart-Maxwell test and assessed distributional difference in response within stratum comparing adolescents to their caregiver’s response. The bold values indicates p < .05.
The domestic and global issues poll (Washington Post-Kaiser Family Foundation Poll) results are presented in Supplemental Table 2. Caregivers who rated climate change as important (n = 220 of 505 respondents) tended to have higher levels of moderate-severe CCA (compare 25.9% vs 7.7% among those who were ambivalent to climate change, P < .001). Though not statistically significant, children of caregivers who believe climate change is important also demonstrated relatively higher reported climate anxiety compared to children whose caregivers were ambivalent to climate change (19.1% vs 15.4% moderate-severe climate anxiety). Additionally, caregivers who rated affordable education, renewable energy, and immigration as important also reported significantly higher levels of moderate-severe climate anxiety compared to caregivers who felt ambivalent about these subjects (P < .05).
Caregivers’ community-level concerns (Alameda County Environmental Justice Community Survey) are presented in Table 3. In caregivers with concerns (access to housing, public services, recreational exercise, and healthy food, as well as exposure to pollution), there was a statistically significant portion reporting moderate-severe climate anxiety (P < .001). The adolescent children of these particular caregivers mirrored that trend, particularly among housing (P = .027), public services (P = .013), and pollution (P = .019).
Comparison of Adolescent and Caregiver CCAS Responses Overall and by Neighborhood Level Caregiver-Perceptions (Univariate Analyses) In Subset Who Answered Alameda County Environmental Justice Community Survey (n = 506).

Note. Superscript P-value next to variable name in first column was based on Chi-square test and assessed difference in CCAS level across factor levels within each role: A (adolescents), C (caregivers). No – Did not check box “Does not apply” and checked boxes indicating reason(s) why they have problems/issues/concerns. Yes – Respondent checked box that indicated “Does not apply” with description listed in table.
P-value in far right column was based on Stuart-Maxwell test and assessed distributional difference in response within stratum comparing adolescents to their caregiver’s response. The bold values indicates p < .05.
In adjusted analyses (Figure 1, Supplemental Table 3), moderate-severe generalized anxiety was the strongest predictor of moderate-severe climate anxiety in both adolescents and caregivers (ORadj 6.59, 95% CI 3.52-12.3, P < .001). Limited access to public services continued to be associated with moderate-severe CCAS (ORadj = 2.63 (95% CI 1.59, 4.35), P < .001). Caregivers viewing climate change as very important had higher odds of moderate-severe CCAS (ORadj = 4.50 [95% CI 2.03, 9.98], P < .001); however, their perception on this issue had no significant effect on adolescent CCAS (P = .172).

Predictors of moderate-to-severe climate change anxiety (CCAS ≥23) and role-specific associations (adolescents vs. caregivers), adjusted for significant predictors and role interactions in the final model as shown in forest plot.
Discussion
To our knowledge, this is the first study to examine climate anxiety in adolescent-caregiver dyads within a clinical setting and to integrate perspectives on environmental and community-level issues. Our findings extend the predominantly adult-focused, non-clinical climate anxiety literature in important ways.11,28 -32 We found that generalized anxiety was a strong predictor of climate anxiety among both adult caregivers and adolescent patients as measured on the CCAS. However, neither caregiver CCAS score nor their perspectives on domestic and global issues – including climate change – were associated with adolescent CCAS score. Rather, public health insurance (as a proxy of household income) and caregiver concerns about neighborhood factors – particularly access to public services – were associated with adolescent CCAS. Our findings expand understanding of adolescents’ unique psychological, emotional, and social vulnerabilities to climate-related stressors, suggesting that climate-related distress is impacted by socioeconomic disparity and existing generalized anxiety, and less so by familial perspective on climate change.
The strong association between generalized anxiety and climate anxiety observed in this clinical sample of adolescent patients and adult caregivers points toward the various interactions and manifestations of anxiety in the 2 age groups. Climate anxiety can be a manifestation or specific subtype of generalized anxiety, while generalized anxiety may also increase vulnerability to climate-specific distress.6,17,29,33 Further, climate anxiety is a psychological stressor that may lead to cognitive-emotional and functional impairment while negatively impacting existing mood disorders and overall well-being, as seen in both adult2,15,29,33 -35 and youth literature.5 -9 Longitudinal research is needed to disentangle these pathways. There may be an indirect relationship between caregiver generalized anxiety and adolescent climate anxiety, since familial interactions influence youth development of anxiety disorders. In fact, a meta-analysis of anxiety disorders found that offspring of adults with generalized anxiety are at a 2.54-fold risk for any anxiety disorder. 36 Additionally, climate anxiety may indirectly influence child development by disrupting family relationships and functioning, with increases in family conflict and anxious parenting reported in the literature. 10
Between 38.3% and 45% of youth describe climate anxiety as a daily challenge impacting their functioning, which has implications on adolescent resilience and long-term mental health trajectories.2,11 Climate anxiety is known to trigger poor sleep, appetite, and concentration,37,38 as well as developmental regression, such as showing less independence in daily routine and episodes of acting out behaviorally. 37 Generalized anxiety appears to be just one underlying vulnerability in children – who are inherently dependent on their caregivers – and is likely exacerbated by climate-related stressors. 39
A lack of correlation between adult caregiver perspective on domestic/global issues and CCAS score with the adolescent patient CCAS score challenges the existing theoretical framework of social learning, which presumes that youth observe and imitate their caregiver’s belief system.28,40,41 The results observed in our study can be explained by several developmental and contextual factors. First, adolescents have a unique combination of developmental growth, socialization, and education.12,14 According to family systems theory, adolescents may demonstrate emotional differentiation by unconsciously avoiding matching parental anxiety patterns 42 – this is likely reinforced by a lack of role modeling among adult caregivers and authority figures on the urgency of climate change. 37 Second, adolescent psychosocial well-being may be more influenced by the opinions of their peers and social media news sources 9 than their caregivers – a form of social reference group effect – although we did not investigate peer influence in this clinical study. 43 Third, the absence of visible parental action on climate change, despite expressed concern, may lead adolescents to discount parental anxiety as performative rather than genuine. A unique psycho-developmental pathway driving generational incongruency around climate perspectives is becoming evident in literature documenting a predominant sense of “betrayal” that climate anxious youth feel regarding their parents’ generation,2,11 while aligning themselves with peer-driven eco-advocacy.7,8 While caregiver climate anxiety itself did not directly predict adolescent climate anxiety in our study, caregiver concerns about community resource and SDOH did emerge as significant predictors, suggesting an indirect transmission pathway.
Specifically, adult caregiver concerns about access to public services, along with economic disadvantage (public health insurance) were associated with adolescent CCAS in adjusted analyses, while concerns of housing and pollution were significant in univariate analyses. Climate change is a ubiquitous SDOH given its negative health impact on vulnerable communities and exacerbation of other existing SDOH that disproportionately impact under-resourced communities facing challenges in food/housing insecurity, transportation, and social support.24,44 Examples of how climate may compound existing SDOH include poor housing quality (lack of insulation and increased penetrance of outdoor pollutants), difficulty paying energy bills, 45 and decreased ability to evacuate during extreme weather-related events, 46 all of which may be sources of distress and negatively impact resiliency of children and their families. Following climate-related events, lower-income adult caregivers may suffer psychological distress through a strain on financial resources with downstream deterioration of family functioning. 10 A combination of less socioeconomic advantage and the emotional-cognitive functional burden of climate anxiety2,11,14 may serve as a double hit to adolescent resiliency and limit opportunity for growth and academic success.
Conclusion
Our findings address a research gap in further characterizing climate change-derived stressors through a caregiver-child dyad lens. We propose a distinct theoretical pathway: emotional responses to climate change (measured by the CCAS) do not transmit directly from caregiver to child, but environmental values and concerns do. Adult caregiver practical concerns may have influenced adolescent climate anxiety scores through an indirect transmission pathway in which caregivers guide adolescent attention – consciously or subconsciously – toward particular environmental and community-level issues, without necessarily modeling specific anxiety responses. Adolescents may internalize parental values and concerns about community and environmental issues and go on to develop their own anxiety response based on their own cognitive appraisal and emotional regulation patterns.
In the developing field of youth climate anxiety, we advocate that mental health practitioners integrate demographic and community-level data to identify adolescent patients most vulnerable to climate change-derived stressors. Our data points toward socioeconomic disadvantage and existing generalized anxiety as 2 underlying predictors of climate anxiety. As screening for climate anxiety in adolescents is still in its infancy, we encourage greater collaboration between pediatric psychological and medical societies to develop policy and practice guidelines in rollout of adolescent climate anxiety screening alongside routine mental health assessments. Wider, external validation of a youth-specific climate or eco-anxiety tool is instrumental in this effort, including in the general pediatric clinical setting. Researchers and educators should recognize that, similar to other social drivers of health, climate change burdens low-resource communities disproportionately and should continue to identify community level features that play a role in youth climate anxiety, such as housing quality and access to fresh food. Targeting subgroups with inequitable drivers of climate anxiety should guide resource allocation and interventions.
This study is limited by a cross-sectional design in which reported findings are limited to associations rather than casual relationships. Generalizability is limited by convenience sampling data collection in a single clinical site rather than community setting, with climate and weather patterns typical to Southern California compared to other regional settings which may experience different climatic and weather events. Due to the exploratory nature of this child-caregiver dyad study in the pediatric ED, we did not calculate a precise sample size, but rather, collected data for 12 consecutive months to control for possible seasonal variability effect on climate anxiety outlook. Those with the most severe medical conditions (ESI 1) and on involuntary psychiatric holds were excluded per the IRB protocol. Demographically, the study sample was diverse and included both Spanish- and English-speaking caregivers. The adapted CCAS that we implemented among adolescents and adults for ease of readability has not been validated, and more generally, the CCAS itself has not been widely validated in children. There was limited assessment of potential confounders, such as amount and type of news consumption, as well as family communication. Collected SDOH variables were also limited and not comprehensive (eg, immigration and employment status, income) and we collected data on concerns related to community and environmental exposures, rather than the objective exposure.
Further analyses should explore additional socioeconomic factors that shape youth climate anxiety. It would be beneficial to conduct studies in the general pediatric office setting, where routine mental health assessments are performed. Also needed in the literature are studies on the impact of peer relationships on youth climate anxiety.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251411470 – Supplemental material for An Adolescent-Caregiver Dyad Approach to Climate Anxiety in the Pediatric Emergency Department
Supplemental material, sj-docx-1-inq-10.1177_00469580251411470 for An Adolescent-Caregiver Dyad Approach to Climate Anxiety in the Pediatric Emergency Department by Raymen R. Assaf, Shelby K. Shelton, Tricia Morphew, Susan Clayton and Jun Wu in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580251411470 – Supplemental material for An Adolescent-Caregiver Dyad Approach to Climate Anxiety in the Pediatric Emergency Department
Supplemental material, sj-docx-2-inq-10.1177_00469580251411470 for An Adolescent-Caregiver Dyad Approach to Climate Anxiety in the Pediatric Emergency Department by Raymen R. Assaf, Shelby K. Shelton, Tricia Morphew, Susan Clayton and Jun Wu in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-3-inq-10.1177_00469580251411470 – Supplemental material for An Adolescent-Caregiver Dyad Approach to Climate Anxiety in the Pediatric Emergency Department
Supplemental material, sj-docx-3-inq-10.1177_00469580251411470 for An Adolescent-Caregiver Dyad Approach to Climate Anxiety in the Pediatric Emergency Department by Raymen R. Assaf, Shelby K. Shelton, Tricia Morphew, Susan Clayton and Jun Wu in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-4-inq-10.1177_00469580251411470 – Supplemental material for An Adolescent-Caregiver Dyad Approach to Climate Anxiety in the Pediatric Emergency Department
Supplemental material, sj-docx-4-inq-10.1177_00469580251411470 for An Adolescent-Caregiver Dyad Approach to Climate Anxiety in the Pediatric Emergency Department by Raymen R. Assaf, Shelby K. Shelton, Tricia Morphew, Susan Clayton and Jun Wu in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Appendix 1
Appendix 2
| Over the |
Not at all | Several days | More than half the days | Nearly every day |
|---|---|---|---|---|
| Feeling nervous, anxious, or on edge | 0 | 1 | 2 | 3 |
| Not being able to stop or control worrying | 0 | 1 | 2 | 3 |
| Worrying too much about different things | 0 | 1 | 2 | 3 |
| Trouble relaxing | 0 | 1 | 2 | 3 |
| Being so restless that it is hard to sit still | 0 | 1 | 2 | 3 |
| Becoming easily annoyed or irritable | 0 | 1 | 2 | 3 |
| Feeling afraid, as if something awful might happen | 0 | 1 | 2 | 3 |
| Column totals: |
Note. Total score: _________
Appendix 3
Appendix 4
Acknowledgements
Carolina Amaya, Kellie Bacon, Selena Nguyen, Phat Nguyen, Parisha Babuta, Vanessa Ngo, Myra Thai, Raymond Nguyen, Shelly Yu, David Vu, Kyle Tran, Shadawn Henderson, Khang Bui, Leone Manaloto, Ngoc-Han Nguyen, Axs Avenido, Shannon Phan, Mikel Concepcion, Brian Alba, Gabrielle Norris, Mason Do, Zoe Ta-Perez, Dishita Arora, Christine Huynh, John Francisco, Mai-Vy Tran, Saba Firouzabadi, Shazabe Siddique, Aisha Ahmad, Haneen Allahaleh, Grace Yip, Karen Sarabia.
Ethical Considerations
All research activity was approved by the Institutional Review Board (IRB, #230104).
Consent to Participate
Informed consent was verbal only; formal consent was waived by the IRB based on risk/benefit ratio and project design wherein risks have been minimized.
Author Contributions
Dr. Raymen Assaf conceptualized and designed the study, contributed substantially to interpretation of data, drafted the initial manuscript, and critically reviewed and revised the manuscript for important intellectual content.
Shelby Shelton contributed to study design, directed and supervised data collection, contributed substantially to data interpretation, and critically revised the manuscript.
Tricia Morphew led modeling for acquisition of data, data analysis, and interpretation, drafted portions of the manuscript, and critically reviewed and revised the manuscript.
Drs. Susan Clayton and Jun contributed substantially to study conceptualization, analysis and interpretation of the data and critically reviewed and revised the manuscript for important intellectual content.
All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The authors abide by the journal’s data sharing policy. Data is available and shared upon approved request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.