
Abstract
Chronic non-communicable diseases are widespread in the US and exert a high burden on its society. Poor lifestyle habits contribute to this contemporary public health crisis. To address the prevalence of non-communicable diseases and related risk factors in Americans, we studied trends in US health professionals’ delivery of health-related lifestyle advice. The major aim was to identify trends and long-term directions in the predicted probability of lifestyle advice delivery. We conducted a secular trend analysis of 18 426 participant reports over 4 consecutive National Health and Nutrition Examination Survey cycles (2011-2018) to estimate the predict probability of their receiving specific lifestyle recommendations by a health professional. Lifestyle-related advice included: (1) sodium or salt intake monitoring; (2) physical activity or exercise encouragement; (3) fat or calorie intake monitoring; and (4) weight control within the last 12 months. In all 4 analyzed NHANES cycles combined, 24.79% (CI: 23.52-26.11) of participants received advice to reduce salt intake, 39.91% (CI: 38.67-41.16) were told to exercise and 30.01% (28.73-31.32) were advised to reduce fat/calories. Compared with 2011-2012, modest increases were observed in 2017-2018 across all lifestyle recommendations; about one-third of participants reported receiving advice to reduce sodium/salt/calories or control/lose weight. The predicted number of lifestyle recommendations received increased over the examined time frame (contrast for 2017-2018 vs 2011-2012: +0.23 (0.13-0.35), P < .001). Health professionals’ competency in delivering health-related lifestyle advice appears deficient warranting its prioritization given health promotion is an established accredited health professional competency comparable to drug prescription.
Keywords
● Non-communicable diseases constitute a global crisis, yet lifestyle advice by health professionals is variably administered.
● Over four NHANES cycles, 30% or fewer participants were advised to reduce salt/sodium, fat/calories, and weight; and 40% to increase exercise.
● Given the prevalence of epidemiological indicators, health professionals’ competencies in lifestyle behavior change warrant being priorities comparable to the rigor of drug prescription.
Introduction
Health promotion and disease prevention are important pillars of many public health strategies. 1 Traditionally, health promotion focuses on behavioral risk factors, including tobacco use, obesity, diet and physical inactivity, and thus significantly overlaps with disease prevention. 2
Most Americans would benefit from prescribed health promotion, an accredited duty-of-care of health professionals (HPs),3,4 in this era of lifestyle-related non-communicable diseases (NCDs).5,6 Inadequate nutrition and inactivity as well as smoking and alcohol are pertinent NCD factors. 7 That over 70% of adults have a body mass index (BMI) ≥ 25 kg/m2, 8 a primary risk factor for heart disease, cancer, and diabetes, 4 supports the need for effective weight management. Further to that, over 90% of Americans exceed sodium/salt intake recommendations 9 ; under 25% meet exercise recommendations. 10 Both support need for competently-prescribed, health-related lifestyle advice.
Supported by various studies based on the National Health and Nutrition Examination Surveys (NHANES) database in the United States (US), HPs miss opportunities to prescribe lifestyle advice, including individuals without overt NCDs yet likely have at least 1 risk factor, a prime target group.11 -13 Although predictors of lifestyle counseling by HPs have been well documented, whether such practice has increased commensurate with need awaits documentation.
Knowledge of prevalence and longitudinal patterns of risk factor counseling and practice gaps would enable HPs to target/tailor their counseling more effectively/efficiently. Performing secular trend analysis, we studied the delivery of health-related lifestyle advice by HPs reported by NHANES participants between 2011 and 2018, over 4 survey cycles.
Methods
NHANES are conducted in the US by the National Center for Health Statistics (NCHS) of the Centers for Disease Control and Prevention (CDC). 14 The NCHS Ethics Review Board approved the NHANES study protocols including ethics.6,15 For our analysis, we appended 4 consecutive, cross-sectional NHANES cycles (2011-2018) which included data on delivery of health-related lifestyle advice by HPs, reported by survey participants. The incomplete NHANES cycle during the COVID-19 pandemic was not analyzed; from 2020 onward, the variables of interest were no longer included in the NHANES.
The delivery of lifestyle advice by HPs in the NHANES was captured in 4 selective questions12,13: ‘During the past 12 months have you ever been told by a doctor or health professional to: (1) to watch or reduce the amount of sodium or salt in your diet?’; (2) to increase your physical activity or exercise?”; (3) to watch or reduce the amount of fat or calories in your diet?”; and (4) control your weight or lose weight?”
The primary outcome was the predicted probability of each of the 4 lifestyle recommendations over the 4 examined NHANES cycles. Sampling weights provided by the NHANES were used to account for the complex survey design (including oversampling) and survey non-response.16,17 As 4 NHANES cycles were combined, an 8-year interview weight was constructed. Only participants without missing data were considered. Participants with missing data on any outcome/covariable of interest were excluded.
Secular trend statistics were based on univariate logistic regression models with each respective lifestyle variable serving as a dependent variable and the NHANES cycle variable as the independent variable. The 2011-2012 cycle was selected as the baseline in those analyses. To estimate marginal predicted probabilities by sex, age and other sociodemographic predictors, we performed unconditional subclass analyses. No adjustments for additional sociodemographic variables were made. Marginal predicted probabilities were computed using the ‘margins’ function in Stata 18 (StataCorp. 2023. Stata Statistical Software: Release 18. College Station, TX: StataCorp LLC). We visualized the results using Stata’s ‘marginsplot’ and ‘combomarginsplot function’.17,18 The post-estimation command ‘pwcompare(effects)’ was used to form margins-based contrasts. The latter constitute differences in the predicted probability between 2 specific NHANES cycles. Alpha was set at .05 for all analyses. This research followed the Strobe Guidelines for Observational Studies (Supplemental Table 1).
Results
The sample included 18 426 participants; thereof 4629 from the 2011/2012 cycle, 4822 from the 2013/2014 NHANES cycle, 4598 from the 2015/2016 cycle, and 4377 from the 2017/2018 cycle. Supplemental Figure 1 displays a stepwise participant inclusion flowchart. Table 1 displays the sample’s characteristics.
Sample Characteristics (Based on 18 426 Participants).
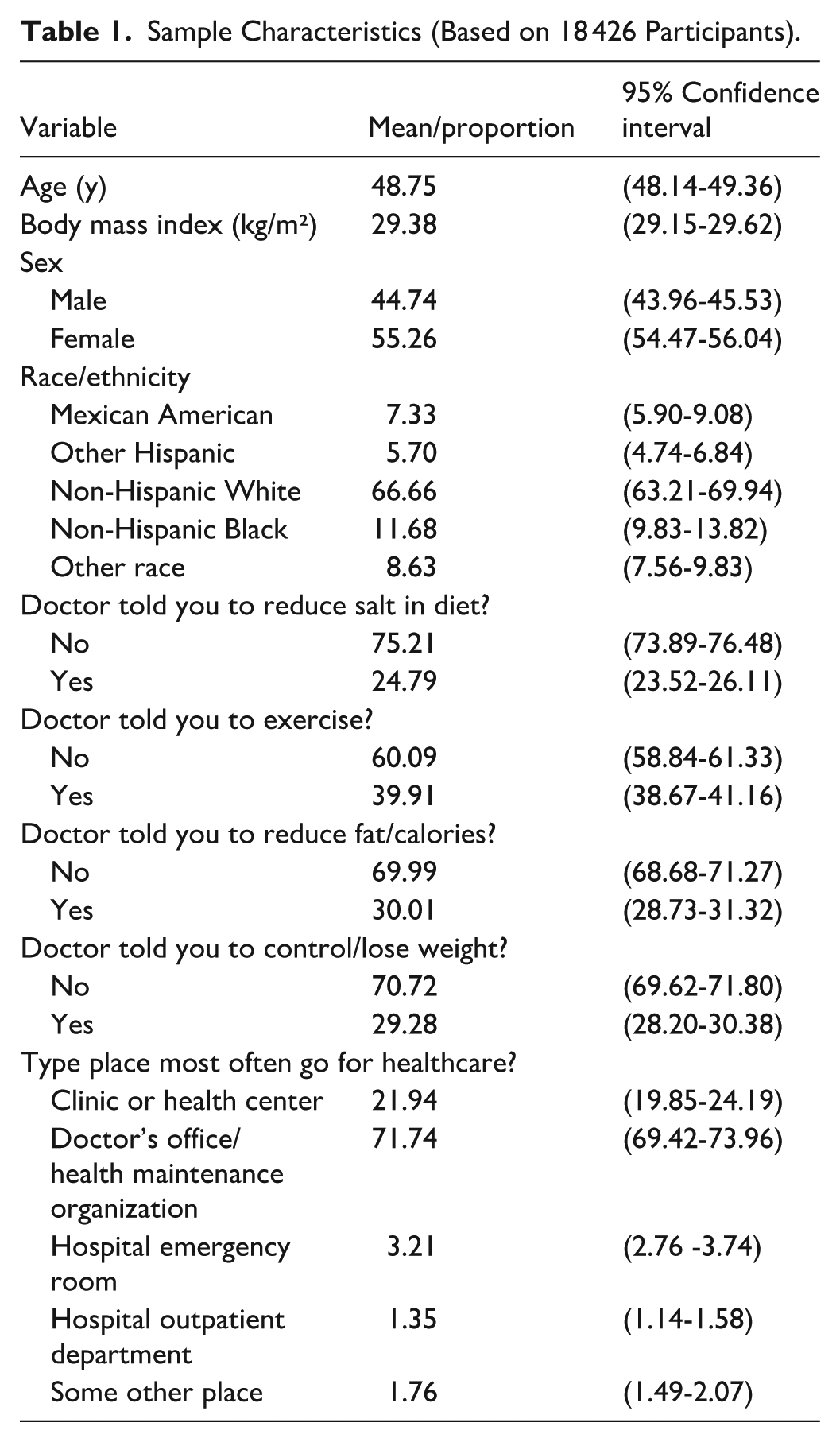
Weighted proportions for males and females were 44.74% (CI: 43.96-45.53) and 55.26% (CI: 54.47-56.04), respectively. The sample’s mean age was 48.75 years (CI: 48.14-49.36) and mean BMI was 29.38 kg/m² (CI: 29.15-29.62). Table 2 displays crude predicted probabilities by NHANES cycle (2011-2018) that a NHANES participants received lifestyle-related recommendations. Figure 1 shows secular trends in the delivery of the 4 examined lifestyle advices in a sex-specific manner.
Crude Predicted Probabilities by NHANES Cycle (2011-2018) that a NHANES Participants Received Lifestyle-Related Recommendations.

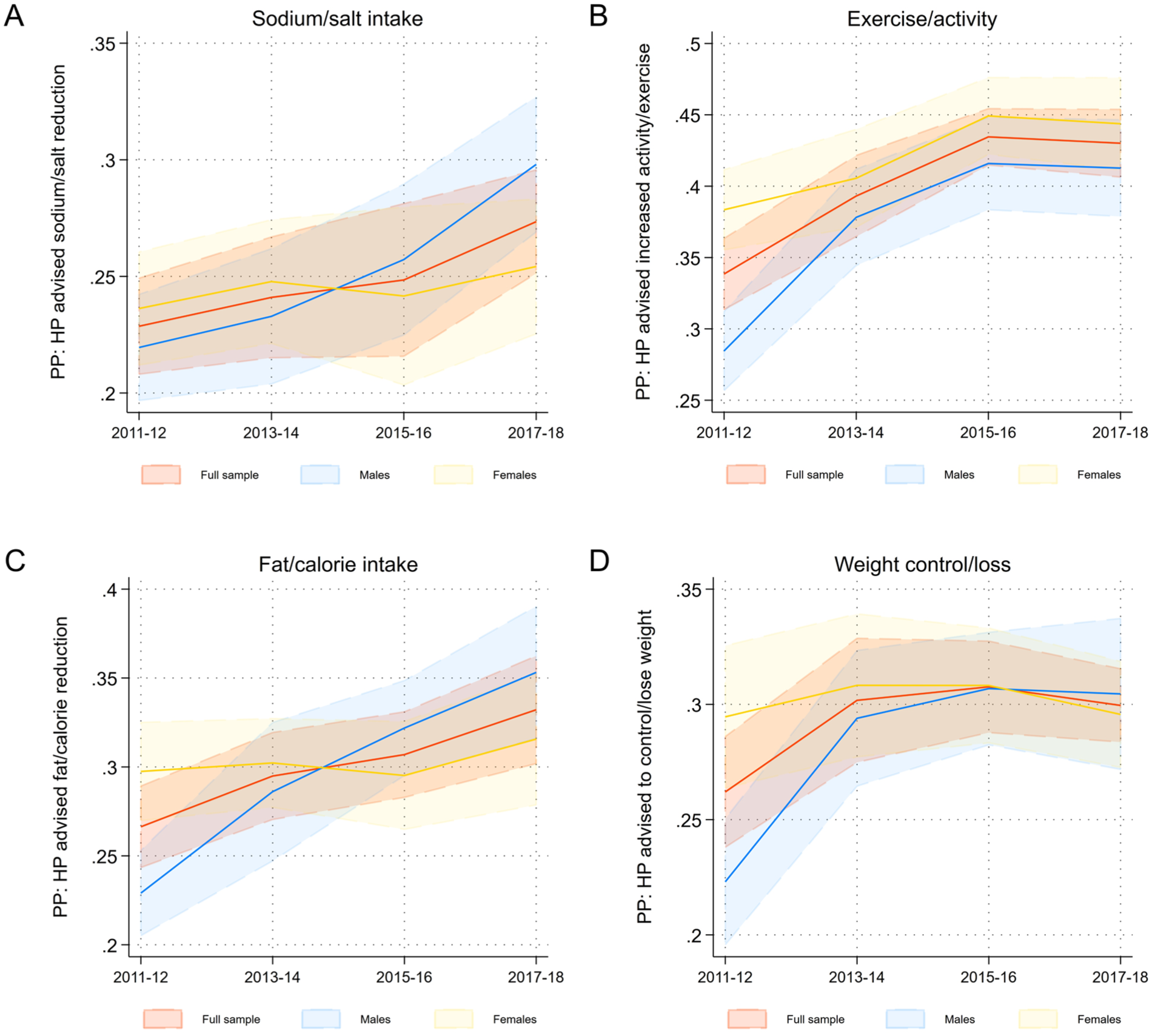
Secular trends in the predicted probability (PP) of the delivery of lifestyle advice by health professionals (HP) in the NHANES 2011 to 2018 (based on n = 18 426 observations).
Less than one-third of participants reported receiving advice to reduce sodium/salt or control/lose weight. Compared to 2011-2012 however, an increase was observed for the delivery of both recommendations (margins-based contrasts in predicted probabilities: +0.045 (0.015-0.075) and +0.038 (0.001-0.066); P = .004 and .011, respectively). Up to 40% of participants were advised to exercise in 2017 to 2018, which constitutes a contrast of +0.092 (0.057-0.126) compared to 2011-2012 (P < .001). Overall, differences between sexes were small, with the largest contrast observed for the sodium/salt reduction recommendation. Figure 2 shows the average predicted number of recommendations in each of the 4 NHANES cycles.

Secular trends in the predicted number of given lifestyle recommendations by health professionals (NHANES 2011-2018; based on n = 18 426 observations). Panel D is based on 16 200 observations due to the age categories recommended in the NHANES for stratified analyses (adults aged 18-19 years were not considered in this graph).
The predicted number increased over the examined time frame (contrast for 2017-2018 vs 2011-2012: +0.23 (0.13-0.35), P < .001). The predicted number of recommendations delivered was twice that in participants with obesity compared with those overweight (Panel B). Panel B in Figure 2 shows that participants with normal weight were less likely to receive lifestyle advice. Panel D in Figure 2 suggests that the same applied to younger participants (20-34 years). In Panel C, stable trends were observed for advice given in clinics and health centers, doctor’s offices and in hospital outpatient departments, whereas an increase was observed for hospital emergency rooms (contrast for 2017-2018 vs 2011-2012: +0.42 (0.007-0.831); P = .046).
Discussion
This study is the first to examine the status of health-related lifestyle advice given by HPs to Americans in the form of a secular trend analysis based on 4 NHANES cycles from 2011 to 2018. Given most Americans could benefit from healthier lifestyles, responses to the 4 questions suggest that health promotion advice remains insufficient. To align with the duty-of-care to promote health that is documented in accreditation standards of established HPs (eg, Caron 1 and The Essentials of Baccalaureate Education for Professional Nursing Practice 4 ) and to respond to epidemiological indicators, a shift in the way healthcare including medicine is practiced, is warranted.
Arguments for not delivering health promotion advice (eg, perceived benefit, and lack of knowledge, skills and time) are not substantiated based on the evidence unequivocally supporting the benefits of healthy lifestyles. HP education warrants prioritizing health promotion competencies given that they are not only specified in education programs as a duty-of-care, but also that outcomes need to be evaluated comparable to other professional competencies. The demand for lifestyle counseling has been documented elsewhere.6,19
Assessment, education and evaluation tools have been developed to facilitate HPs systematically addressing health-related practices. The World Health Professions Alliance, an alliance of the 5 global leading HPs, for example, developed the Health Improvement Card. 20 This short 2-page, traffic-light-coded card, includes biometric data, and practices related to diet, activity, tobacco, alcohol, stress, and sleep. Also, it includes the Health Improvement Action Plan for both patient and HP.
Strengths of our study include its large, nationally-representative sample which adds confidence about its validity and generalizability. This benchmark analysis supports a persisting gap between the health-related advice needed by Americans and that delivered by HPs; specifically, gaps in identifying who to target and what advice to give. Previously deleted related questions need to be reviewed regarding their specificity and expanded to better reflect the congruence of lifestyle change and NCD risk, for example, smoking, nutrition quality, prolonged sitting, stress, and sleep. 7 Also, the questions need to identify which HP provided each health-related lifestyle advice. A limitation is the absence of multivariable regression models which link the findings with NCD prevalence. Nonetheless, this has been previously addressed.11 -13 Additional limitations include the cross-sectional study design, potential bias in participants’ responses (eg, recall and reporting bias) as well as the limited time frame that was analyzed for NHANES-specific reasons (such as the COVID-19 pandemic as discussed earlier).
Conclusion
Given the prevalence of NCDs in the US and adverse health-related lifestyle practices of Americans,8 -10 most NHANES participants were eligible for receiving lifestyle advice as a primary preventive intervention consistent with HP accreditation standards. Collective systematic effort across established HPs warrants prioritizing competency in health-related lifestyle advice, thereby better aligning practice with a duty-of-care documented in their professional accreditation standards.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251404788 – Supplemental material for Secular Trend Analysis of NHANES Data Suggests Only Modest Increases in Health-Related Lifestyle Advice Delivered by Health Professionals
Supplemental material, sj-docx-1-inq-10.1177_00469580251404788 for Secular Trend Analysis of NHANES Data Suggests Only Modest Increases in Health-Related Lifestyle Advice Delivered by Health Professionals by Maximilian Andreas Storz and Elizabeth Dean in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580251404788 – Supplemental material for Secular Trend Analysis of NHANES Data Suggests Only Modest Increases in Health-Related Lifestyle Advice Delivered by Health Professionals
Supplemental material, sj-docx-2-inq-10.1177_00469580251404788 for Secular Trend Analysis of NHANES Data Suggests Only Modest Increases in Health-Related Lifestyle Advice Delivered by Health Professionals by Maximilian Andreas Storz and Elizabeth Dean in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
n/a.
Author Note
This work been approved by all co-authors.
Ethical Considerations and Consent to Participate
NHANES was approved by the National Centre for Health Statistics research ethics review board and informed consent was obtained from all participants. The respective ethical approval protocols were #2011-17 and #2018-01 which were approved in 2011 and 2018, respectively.
Consent for Publication
Written informed consent was obtained from all participants.
Author Contributions
MAS conceived the study. MAS performed the analysis and constructed the illustrations. MAS interpreted the data. ED contextualized the findings. Writing original draft: MAS and ED. Writing—review and editing: MAS and ED. Both authors reviewed and approved the final manuscript. Both authors agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work were appropriately investigated and resolved.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: No funding was required for this study. The authors acknowledge support by the Open Access Publication Fund of the University of Freiburg.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Copyrighted Material
No copyrighted material, surveys, instruments, or tools were used in the research described in this article.
Trial Registration Number/Date
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.