
Abstract
The rapid integration of digital technology in early childhood education has raised concerns about managing preschool screen time (ST) and its potential harm to children’s health and development. These concerns intensify during crises like pandemics or conflicts, when remote learning becomes necessary. Identifying risk and protective factors related to digital exposure is essential for child well-being. To investigate health risks and protective strategies linked to ST among preschool children during remote learning. A literature review was conducted from 2010 to 2025 using scientometric databases. Studies on health effects of digital exposure in early childhood were included. The review was illustrated with findings from our study of 1312 parents of preschoolers aged 4 to 6, which explored the relationship between ST and mastery of learning programs. Excessive ST was associated with reduced physical activity, irregular sleep, emotional difficulties, and delayed language acquisition. Higher ST was also linked to lower odds of completing the preschool learning program. Effective protective strategies included structured routines, parental co-viewing, and limiting passive ST. Reducing parental technoference emerged as a protective factor. Contextual factors such as socioeconomic disparities and caregiver digital literacy influenced outcomes. Remote learning presents both challenges and opportunities for preschoolers. While excessive screen use and parental technoference can negatively impact health and learning, evidence-based strategies, such as co-viewing, regulated content, and mindful parental engagement, can help reduce harm. Developing health-informed digital practices in early education is critical in times of crisis.
Keywords
Remote learning during crises now extends to preschool education, requiring increased public health attention and evidence-based guidance.
Excessive screen exposure in early childhood is associated with poorer learning outcomes, language delays, reduced attention, disrupted sleep, emotional dysregulation, and long-term challenges in social interaction and emotional connectedness.
Prolonged passive screen time increases risks of physical health issues such as obesity and myopia, while limiting real-world exploration and play.
Parental technoference, which is disrupted interaction caused by adult device use, further weakens emotional bonding and behavioral regulation.
Active, co-viewed, and developmentally appropriate digital engagement can support learning when combined with daily routines and mindful parental presence.
Introduction
Digital education has expanded significantly in recent years due to the COVID-19 pandemic, global transitions to online learning, and, in Ukraine, the ongoing military conflict. While remote learning offers continuity and emotional support for children in crisis situations, its application to preschool-aged children (2-6 years) presents distinct challenges.1-4 At this developmental stage, children have limited attention spans, immature executive functions, and require hands-on, socially interactive, and emotionally responsive learning environments. 1
International guidelines from the World Health Organization (WHO) and the American Academy of Pediatrics (AAP) recommend limiting screen time (ST) to a maximum of 1 h per day for children aged 2 to 5 years. They emphasize the importance of high-quality content and active parental involvement.1,5-7 These recommendations are grounded in mounting evidence linking excessive screen exposure to a range of negative outcomes.3,5-18 Neuropsychological research suggests that early and prolonged screen exposure may impair attention regulation, memory consolidation, and fine motor development.9,12,14,16-18 It is also associated with reduced physical activity, language delays, behavioral issues, and disturbed sleep.12,13,15-18 Recent studies highlight broader health concerns, including mental health difficulties, ADHD-like symptoms, and increased risks of obesity and myopia.10,16,18
In addition to children’s screen time, parental technoference, disruptions in parent-child interactions due to parental device use, has emerged as a critical factor influencing child well-being.7,8,19 It undermines the warmth of parent-child bonds and negatively affects children’s emotional and cognitive development. 19
Despite these concerns, many countries, including Ukraine, have implemented or are experimenting with remote preschool learning. This has occurred both during the pandemic and in response to infrastructure disruptions and safety risks caused by war. However, evidence-based guidelines for remote learning in early childhood remain scarce, particularly in non-Western contexts. 20
The balance between educational needs and health risks in digital environments is difficult to define without empirical data.3,4,10 Since distance learning involves extended screen time (ST) for both educational and social activities, it is essential to assess the health effects of this exposure. Current research indicates that ST is characterized by rapid information intake while increasing overall screen use. Reviewing studies conducted before the era of fast-paced content may therefore provide more meaningful insights into which aspects of distance learning require sustained focus.
This study aims to bridge the gap in understanding the impact of ST on the health of preschoolers in a distance learning context. We present a hybrid publication that combines a narrative review of the international literature on the subject with original data from a multicenter cross-sectional study involving 1312 preschool children aged 4 to 6 years in Ukraine. This study aimed to investigate whether screen duration affects preschool children’s cognitive engagement in learning tasks. Additionally, we provide practical recommendations for implementing remote learning for preschoolers in a health-informed manner.
Materials and Methods
Narrative Review
We conducted a narrative literature review of publications from January 2010 to April 2025 via the following databases: PubMed, Scopus, Web of Science. The search strategy combined terms such as “preschool children,” “screen time,” “remote learning,” “digital media,” “sleep,” “cognitive development,” “language development,” “visual health,” and “emotional behavior.” Boolean operators (AND/OR) were applied.
Inclusion criteria:
- Peer-reviewed articles published in English and Ukrainian between 2010 and 2025.
- Studies involving children aged 2 to 6 years.
- Research examining associations between ST and developmental or health outcomes (cognitive, behavioral, emotional, physical, or sleep-related).
Exclusion criteria:
- Articles focusing on ST unrelated to learning or media exposure (eg, telemedicine, parental use only).
- Nonhuman research, conference abstracts, editorials, or nonpeer-reviewed sources.
Reference lists of key papers were screened for additional eligible studies. Preference was given to recent large-scale studies, systematic reviews, and those with clear outcome measures.3-5,8-10,13-30
Empirical Findings
Design and Participants
In the spring of 2012, we conducted a survey of parents of preschool children aged 4 to 6 years regarding their children’s daily routines. A total of 1312 questionnaires were included in the analysis (50.5% boys). The parents completed daily diaries over 7 consecutive days, which are provided in the Supplemental Materials (Supplemental file 1). The diaries were pilot tested on a focus group (n = 20) and demonstrated excellent reliability, with ICC values ranging from 0.82 to 0.95 in a test-retest procedure conducted over a 1-week interval.
This multicenter study involved respondents from 4 regions of Ukraine. All kindergartens were publicly owned and operated under a unified educational standard. Kindergarten educators, trained by our staff during a 1-day seminar, worked directly with the parents. The questionnaire included items about children’s daily routines as well as their learning process.
Given the hybrid nature of this article, we used a small subset of this database to illustrate the impact of ST duration on the acquisition of the educational program.
Data Processing
Trained research assistants manually reviewed and processed the individual logs. The quantitative values (eg, bedtime) were transformed into categorized intervals (eg, “Before 21:00”). The total daily ST was calculated by summing the time spent watching television, playing games, and using electronic devices for educational purposes. A binary variable was generated for screen time: 1 = “≤1 h/day”; 0 = “>1.1 h/day”. The outcome variable was cognitive engagement in learning tasks (1 = yes; 0 = no).
Cognitive engagement was measured via a binary variable defined by the response to the following question: “Does the child understand the educational material taught at kindergarten?” The response options were “yes” and “no.”
Statistical Analysis
Descriptive statistics were calculated for key variables. Logistic regression was performed with cognitive engagement as the dependent variable. The independent variables included screen time, sex, residential status (urban/rural), and sleep duration (in minutes). Odds ratios (ORs) with 95% confidence intervals (CIs) are reported. Model performance was evaluated via receiver operating characteristic (ROC) curve analysis, and the threshold with the best balance of sensitivity and specificity was identified.
All statistical analyses were conducted using IBM SPSS Statistics for Windows, Version 26.0 31 and verified using R software, Version 4.3.1. 32
Results
The literature consistently indicates that excessive screen time in preschool-aged children is associated with adverse developmental and health outcomes. These include reduced language development,4,9,13,14,21 impaired executive functioning and attention regulation,2,3,15,22-25 increased risks of overweight and myopia,3,10,27,29,30 emotional dysregulation and social difficulties,12,18,19,30 and disrupted sleep patterns3,5,6,12 (Table 1). In addition, studies highlight distinctions between active and passive screen time that influence developmental trajectories.26-29
Summary of Literature Review Findings.

Meta-analyses and large-scale surveys have shown that only 24% to 36% of children under 5 meet ST recommendations.4,5,11 Parental co-view and interactive digital content can reduce certain risks, although potential long-term effects on brain development remain under investigation.4,14,23
The main key points identified are presented in Figure 1.

Additionally, emerging evidence suggests that technoference, defined as the disruption of parent-child interactions due to adult screen use, may further exacerbate emotional and behavioral challenges in young children (Figure 2).
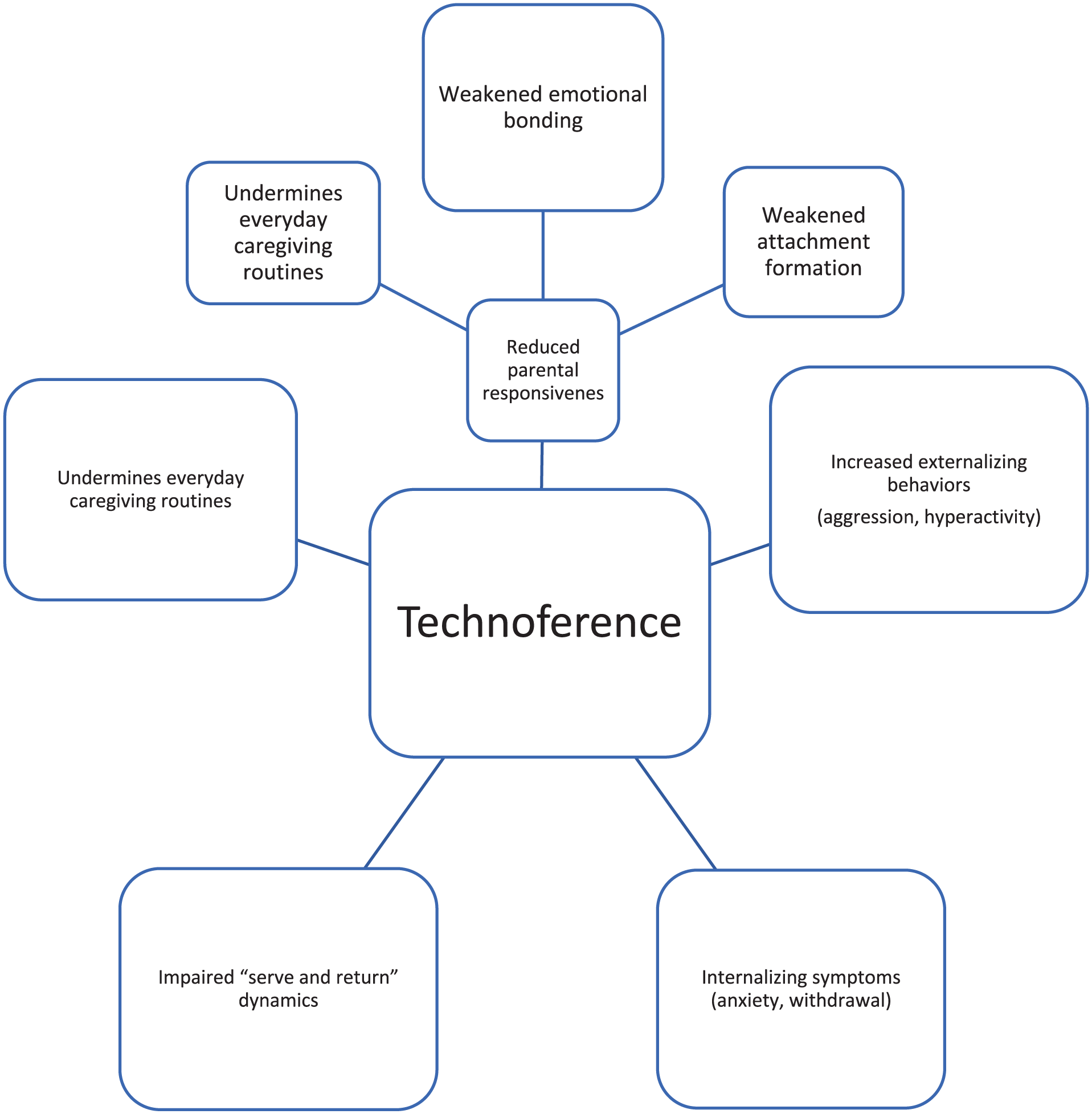
Invisible interruptions: how technoference shapes childhood.
Recent studies show that parental technoference is not merely a background behavior but a distinct risk factor for child development. These disruptions can lead to increased irritability, attention-seeking behaviors, and difficulties in emotional regulation, particularly when children perceive digital devices as competing for parental attention.16,19 Technoference also undermines everyday caregiving routines and safety monitoring.
Given its impact, it should be considered a separate digital exposure variable alongside screen time in models of early childhood health.
Empirical Findings
The average daily ST in the total sample was 63.8 min (SD = 56.2), with boys and girls averaging 67.8 min (SD = 58.6) and 59.7 min (SD = 53.5), respectively (F = 6.7; P = .010). The proportion of children aged 4 to 6 years with STs exceeding 1 h per day was 49.3% for boys, 40.4% for girls (χ² = 10.4; P = .001), and 44.9% in the overall sample. Table 2 presents sample characteristics stratified by sex, including qualitative and quantitative data.
Demographic Profile and Screen Time Patterns (N = 1312).

Successful education refers to how effectively children comprehend and retain knowledge.
DL is developmental learning denotes learning activities using electronic screen devices.
Values are presented as the mean (standard deviation).
The composition of STs between boys and girls did not differ significantly and consisted of 73.4% television viewing, 16.2% video gaming, and 10.4% developmental learning activities (Figure 3).

Composition of screen time in preschool children stratified by sex, %.
The largest share of ST was allocated to television viewing (73.4%), with video gaming and developmental activities accounting for 16.2% and 10.4%, respectively. Girls spent a slightly greater proportion of their ST watching television (Figure 3), whereas boys had higher proportions engaging in video games and developmental activities; however, these differences were not statistically significant (P > .1).
Children residing in rural areas had significantly lower average STs (53.5 min, SD = 34.8) than did their urban counterparts (84.3 min, SD = 80.0; F = 94.4; P < .001).
Children who successfully acquired the educational program had an average ST of 54.3 min (SD = 35.2), whereas those with learning difficulties averaged 172.2 min (SD = 111.4).
Among children with more than 1.1 h of screen exposure per day, 10.05% reported not assimilating educational material in kindergarten, whereas among those with less than or equal to 1 h, only 3.24% reported doing so. The relationship was statistically significant (χ² = 24.98, df = 1, P < .001), and a weak but significant positive correlation was found (Spearman’s ρ = .139, P < .001).
Logistic regression analysis revealed that children who exceeded 1.1 h of ST per day were 3.33 times more likely to be reported as not assimilating educational material in kindergarten (OR = 3.33, 95% CI: 2.03-5.47, z = 4.76, P < .0001). This association remained significant even after controlling for other factors.
Table 3 presents the coefficients from both the unadjusted and adjusted logistic regression models. The unadjusted model revealed that each 1-min decrease in ST per day increased the odds of successful acquisition of the educational program by 2.5% (OR = 0.975; 95% CI: 0.972-0.979). The adjusted odds ratio indicated a 2.2% increase per minute (OR = 0.978; 95% CI: 0.974-0.982).
Logistic Regression Model Coefficients.
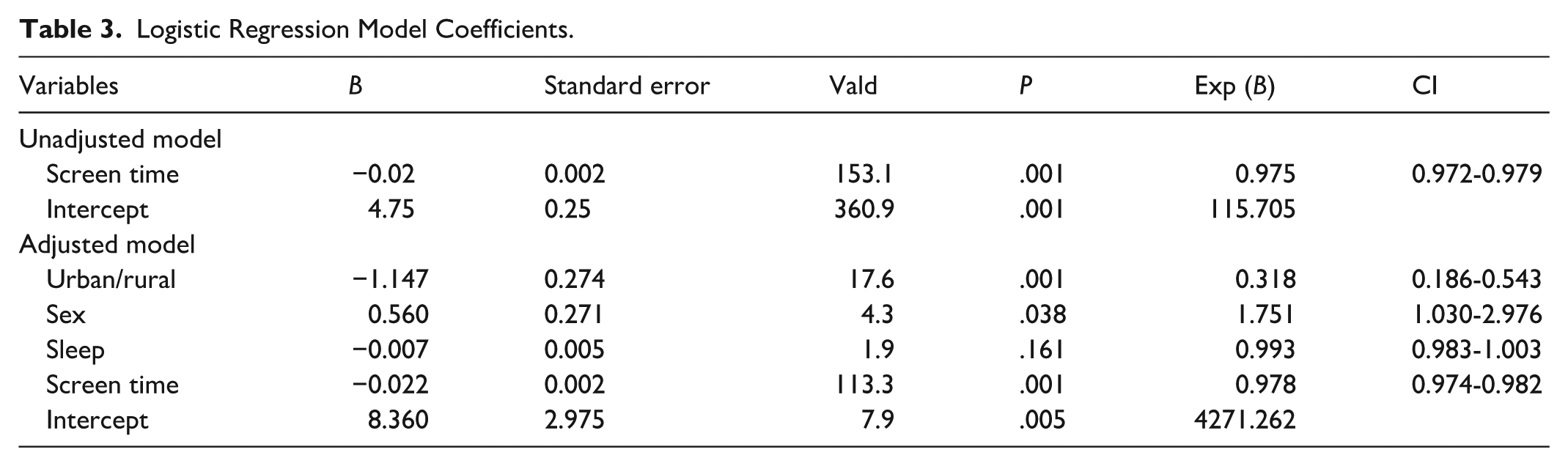
In addition to the effect of ST, the covariates sex (OR = 1.751; 95% CI: 1.030-2.967) and place of residence (OR = 0.318; 95% CI: 0.186-0.543) were significant in the model. The model correctly classified 95.9% of the cases. The model demonstrated strong predictive ability (Model χ²(4) = 289.51, P < .001). The area under the ROC curve (AUC) was 0.941, indicating excellent discriminative power. The optimal cutoff point provided a sensitivity of 0.89 and specificity of 0.87.
Discussion
Our literature review presents evidence suggesting that excessive ST may be associated with various developmental challenges in early childhood. These include potential language delays, difficulties in attention and executive function, emotional dysregulation, behavioral issues, sleep disturbances, and an increased likelihood of obesity and myopia.3-6,9-12,21,23,27,30,33-37
Our data analysis indicated that each additional minute of screen exposure was linked to a decrease in the odds of cognitive engagement of more than 2.2% (OR = 0.978; 95% CI: 0.974-0.982). These findings align with existing research showing that children exceeding the recommended daily ST are at greater risk of learning difficulties. While the observed effect size is modest (r = .14), the consistent results across both adjusted and unadjusted models highlight the potential negative cognitive implications of excessive ST. Our study also found that exceeding 1 h of screen time per day triples the likelihood of academic failure (OR = 3.33, 95% CI: 2.03-5.47).
The relationship between ST and health is believed to stem from both physiological factors, such as melatonin suppression and sedentary behavior, as well as a decrease in engaging, health-promoting activities in children’s daily routines.3-6,10,12,30-34 These activities include physical exercise, interactive play, reading, and emotionally rich interactions between adults and children. Additionally, unsupervised or passive screen use, especially with dynamic or algorithm-driven content, may further hinder preschool children’s ability to regulate attention, verbal reasoning, and emotional stability.10-12,14,30,34-36
Recent developments in digital technologies have prompted research into the effects of both active and passive STs.26,30,34,35,38 Understanding this distinction is crucial for evaluating their impact on children. International recommendations from the WHO and AAP limit ST to no more than 1 h per day for children aged 2 to 5 years, with at least 70% of that time devoted to active, co-viewed, or interactive content.3,6,10,12,26,30,34,36,39 This means that digital time should ideally involve communication, learning, or regulated physical activity.
These guidelines also reflect the developmental characteristics of preschoolers and their attention capacity. Children aged 2 to 3 years can concentrate on a single task for approximately 5-10 min, whereas those aged 4 to 5 years can sustain attention for 10-15 min, potentially extending to 20 min with adult involvement. Therefore, a single video lesson, whether exercise, story, or logical game, should not exceed 15 min for 2- to 3-year-olds and should be limited to 20 min for older preschoolers.
On the basis of our analysis of the literature on ST among preschool children aged 4 to 6 years, particularly during the 2010 to 2015 period, and supplemented by more recent meta-analyses, excessive screen exposure clearly continues to pose a significant developmental risk. Studies from this earlier period, as well as subsequent systematic reviews such as the 2024 meta-analysis,3,5,8-10,12,30,34-36,40,41 demonstrate that a large proportion of children aged 2 to 5 years exceed the recommended daily ST limit, often without parental supervision or age-appropriate content.
Recent research has highlighted that technoference, the interruption of interpersonal interactions by digital devices, affects not only the quality of parent-child bonding but also children’s emotional regulation. 19 When parental attention is diverted to screens, children may perceive it as emotional neglect, which can trigger irritability, crying, aggression, and attention-seeking outbursts.16,19 These reactions reflect deeper disruptions in attachment and trust-building processes.16,19,42,43 Moreover, children may internalize the message that devices are more important than their presence, undermining the development of self-worth and social responsiveness. This dynamic reinforces the need for intentional digital boundaries within family routines.
Moreover, contemporary studies examining ST in the context of remote learning may not accurately reflect the current pace and style of digital media consumption.30,34,35,39,44-47 Modern children are increasingly accustomed to fast-paced, highly stimulating digital content that significantly departs from traditional media formats. Therefore, the design of remote learning programs must account not only for opportunities for social interaction and play-based engagement12,14,30,34,36 but also for attention span, overstimulation risks, and the quality of content delivery.
These findings also raise critical questions about the adequacy of “ST” as a standalone indicator of media exposure in preschool-aged children.11,29,30 There is growing recognition that this metric may oversimplify the multifaceted nature of early digital engagement.1,3,11,29,30,35,36,46-48 Modern platforms depend heavily on fast-paced, highly engaging content, which can both positively and negatively impact cognitive load, attention span, and emotional regulation, regardless of duration.
Our review indicates that parental co-view, the use of interactive formats, and adherence to daily ST limits are among the most promising protective strategies.3,4,12,14,30,34,36,37 However, implementation varies widely across settings, particularly in non-Western and crisis-affected regions.14,34,38,39,44,45,49 This variation underscores the urgent need for practical, culturally sensitive recommendations and rigorous evaluation of digital learning programs in early childhood contexts. 1
Our findings further support the argument that remote learning during early childhood must be carefully regulated. Although online platforms may offer cognitive stimulation, continuity of care, and emotional scaffolding, particularly during emergencies such as pandemics, unsupervised or excessive screen exposure may undermine these potential benefits.3,5,10,12,14,30,34-36,39-41,44,45
It is essential to recognize that, when utilized thoughtfully, digital tools can play a valuable role in supporting development and learning. Interactive media that are age-appropriate and foster sensorimotor engagement, turn-taking, storytelling, and verbal interactions can enhance early cognitive skills, promote language development, and strengthen parent-child relationships when experienced together.12,14,20,28,36
Additionally, structured digital content, particularly when viewed alongside adults, can offer continuity of care, emotional support, and enriching learning experiences during challenging times or periods of routine disruption. Rather than dismissing digital platforms, early childhood education should seek to cultivate media literacy within families and emphasize the importance of quality over quantity in ST. Reducing parental technoference can further enhance the emotional benefits of shared digital experiences, transforming screen time into moments of connection rather than distraction.
The strengths of our study lie in the integration of a narrative synthesis of the world literature with original empirical data collected from a context that deserves further attention. These data were obtained before the pervasive digitalization and rapid content consumption that characterize our era. Therefore, we believe that using retrospective data to analyze the impact of distance learning on children’s health is a valid approach, as it considers the effects of developmental learning.
While much of the research on the impact of ST on the health of preschoolers has focused on high-income Western countries, our findings from Ukraine provide insight into an Eastern European perspective that is often underrepresented. In this region, differences in access to digital technologies, educational resources, and family practices are quite pronounced compared with those in the West.
The limitations of the empirical section of this study include our reliance on retrospective data collected before the era of global digitalization, changes in content, and the rise of distance learning. As a result, we were unable to fully capture the effects of contemporary information content on the health of preschoolers.
Another limitation was the restricted ability to account for all factors that might influence cognitive ability and the acquisition of the kindergarten curriculum. For future prospective studies, it will be important to include additional indicators of development and behavior, such as morbidity, sleep quality, emotional state, and interactions with peers, parents, and caregivers.
Recommendations and Implications
On the basis of the reviewed literature and our empirical findings, we propose the following recommendations to guide policy, research, and practice in early childhood digital learning:
In addition to the above recommendations, we have developed a concise handout for parents and caregivers, outlining 7 practical steps to support healthy digital habits and reduce technoference in early childhood (Supplemental File 1, Supplemental Material 2). This material is available as supplementary content and may be adapted for use in educational, clinical, or community settings.
Conclusions
This study emphasizes the importance of managing screen exposure for preschool children, especially during remote learning. Our findings reveal a significant correlation between increased screen time and a reduced likelihood of mastering educational content, which aligns with existing evidence on the health risks associated with excessive digital media use in early childhood.
While digital tools can offer valuable support during challenging times, they should be used with careful consideration of age-specific needs, developmental vulnerabilities, and health guidelines. Screen-based learning should focus on interaction, be concise, involve adult participation, and be integrated into a holistic daily routine that includes physical activity, social engagement, and adequate sleep.
Future policies and digital education initiatives should be based on evidence-informed strategies that strike a balance between innovation and the well-being of children. Furthermore, additional research is needed to understand the long-term cognitive, emotional, and social impacts of remote learning on preschool-aged individuals.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251390766 – Supplemental material for Digital Exposure in Early Childhood: Health Risks and Protective Strategies During Remote Learning
Supplemental material, sj-docx-1-inq-10.1177_00469580251390766 for Digital Exposure in Early Childhood: Health Risks and Protective Strategies During Remote Learning by Olena Yelizarova, Tetiana Stankevych, Alla Parats, Viktor Yelizarov, Olha Puzanova, Natalia Lebedynets and Svitlana Hozak in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We thank the teachers and respondents who participated in this study, and gratefully acknowledge the assistance of the large language model ChatGPT (GPT-4o, GPT-5, OpenAI) and Copilot (Microsoft), which was used to support the translation and language refinement of the manuscript. All intellectual content and final wording were determined by the authors.
ORCID iDs
Ethical Considerations
The survey was approved by the Bioethics Committee of the SI “O.M. Marzieiev Institute for Public Health.”
Consent to Participate
The participants were informed about the survey’s objectives, confidentiality measures, data usage conditions, and contact information for the principal investigator. All the participants read and signed an informed consent form.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Clinical Trial Registration
Clinical trial number not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.