
Abstract
This study explores the relationship between precarious employment and unmet healthcare needs among low-skilled migrant workers with E-9 visas in South Korea, addressing health disparities in a rapidly aging society. Using microdata from the 2024 Survey on Immigrants’ Living Conditions and Labor Force (n = 2576), latent class analysis identified 3 employment types: High Precarity Type (37.8%), Moderate Precarity Type (34.0%), and Low Precarity Type (28.2%). Logistic regression, controlling for demographic, and immigration-related factors, showed that the Moderate Precarity Type (OR = .53, P < .05) and Low Precarity Type (OR = .37, P < .01) had lower odds of unmet healthcare needs compared to the High Precarity Type. Higher wages (OR = .48, P < .05) and income satisfaction (OR = .69, P < .01) reduced unmet needs, while workplace discrimination (OR = 2.43, P < .01) increased them. Employment status based on contract duration, working hours, and workplace size showed no significant associations. These findings highlight how structural vulnerabilities within the Employment Permit System (EPS) exacerbate healthcare access barriers. Policy recommendations include prohibiting workplace discrimination to promote equitable work environments, reducing healthcare copayments for low-income migrant workers, and reforming the EPS to ease workplace mobility and enhance visa stability.
Keywords
Introduction
South Korea (Korea) is rapidly transitioning into a super-aging society, 1 leading to significant labor shortages, particularly in the so-called “3D industries” (dirty, difficult, and dangerous), such as manufacturing, construction, and agriculture. 2 To address the structural labor gaps caused by the reluctance of native workers to engage in these sectors, the South Korean government established the Employment Permit System (EPS) in 2004, enabling low-skilled foreign workers to legally enter and work in the country under the E-9 visa. 3 Among the 2.65 million foreign residents in South Korea, approximately 12.7% are low-skilled migrant workers holding E-9 visas, playing a pivotal role in filling essential labor roles shunned by native workers.2,4
According to the Human Resources Development Service of Korea, 3 under the EPS, the E-9 visa serves as a primary mechanism for addressing labor shortages in sectors such as manufacturing, agriculture, construction, fisheries, and services. Recruitment is restricted to nationals of 16 designated sending countries, such as Vietnam, Cambodia, Mongolia, and others, with eligibility confined to individuals between the ages of 18 and 39 who are selected through a point-based system that evaluates Korean language proficiency, functional skills, and job-related competencies. Upon entry, E-9 visa holders are authorized an initial 3-year period of stay, which may be extended once, contingent upon employer request, for less than 2 additional years, with the maximum duration capped at 4 years and 10 months. Following the expiration of this term, workers are required to repatriate; however, limited pathways for re-entry exist through 2 specific mechanisms: the Special Re-employment program, which enables return to the same workplace under narrowly defined contractual and sector-specific conditions, and the Special Korean Language Test, which permits re-entry for those who have voluntarily departed and who satisfy prescribed residency and occupational requirements. Legally, employment-eligible foreigners in Korea are categorized into 3 groups: professional, unskilled, and other. Despite being categorized as “unskilled,” E-9 visa holders are subject to more severe employment, job mobility, and length-of-stay restrictions compared to professional and other visa groups, as well as other unskilled visa types. Non-compliance with visa conditions, including unauthorized employment, overstaying, or participation in prohibited activities, may result in immediate revocation of legal status with few avenues for appeal.
However, the structural characteristics of the EPS and the institutional constraints of the E-9 visa inherently place migrant workers in precarious employment conditions. First, E-9 visa holders are permitted to stay in Korea for a maximum of 4 years and 10 months. 3 Fear of visa revocation prevents these workers from reporting discrimination or unfair treatment in the workplace and forces them to endure precarious employment conditions. 5 Second, workplace mobility is highly restricted. E-9 visa holders may change employers up to 3 times within the first 3 years of their stay, but only under specific conditions outlined in the law, such as non-payment of wages, unfair treatment, or business closure. 3 Institutional constraints hinder workers’ ability to freely choose their employers, fostering dependency and deepening structural employment instability. 6 In addition, most E-9 visa holders are employed by small businesses with fewer than 5 employees. 7 These businesses are often excluded from key provisions of the Labor Standards Act, and thus lack essential protections such as paid leave, severance pay, and prescribed working hours.8,9 This employment insecurity not only worsens working conditions but also negatively impacts health, leading to deteriorating physical and mental well-being, increased stress, and restricted access to healthcare services for migrant workers.10,11
Precarious employment is generally characterized by unstable work environments and job insecurity. 12 While earlier interpretations primarily emphasized contract types or employment status, 13 contemporary research has redefined precarity as a complex, multifaceted concept that includes factors such as job continuity, income adequacy, workplace protections, access to social benefits, and workplace power imbalances. 14
This study utilizes the framework from Kreshpaj et al. 14 to analyze precarious employment. After reviewing 63 studies, Kreshpaj and colleagues conceptualize precarious employment across 3 core areas: employment insecurity, income inadequacy, and lack of rights and protection. 14 The first area, employment insecurity, covers 4 aspects: contract type (direct vs indirect), contract length (permanent vs temporary), working hours (full-time vs part-time), and number of jobs held. Income inadequacy is the second area, which assesses both low income levels and a subjective feeling of not having enough money. The third area, lack of rights and protection, includes a lack of union membership, social security, company welfare, and workplace rights against unfair treatment. This framework is especially useful for understanding migrant workers’ experiences, as they often lack institutional support. 11 Even when applying the same analytical framework for precarious employment, indicators measuring precarious employment vary due to differences in national contexts 14 and available data. 15 In Korea, studies using the framework of Kreshpaj et al. 14 have also included workplace size as an indicator.16,17 The Korean Labor Standards Act exempts workplaces with fewer than 5 employees from certain protections, such as a 40-h workweek, severance pay, paid leave, or overtime compensation, 9 making workers in these smaller businesses more vulnerable.
Precarious employment has been consistently shown to have negative health effects across empirical studies. 18 Precarious employment is associated with increased levels of stress, 11 limited access to health-related resources, and reduced opportunities to maintain physical well-being. 19 As a result, precarious employment is associated with decreased utilization of health services 20 and increased unmet healthcare needs.21,22
Recent studies have further advanced this field by categorizing different forms of precarious employment and linking them to health outcomes.23-25 In particular, Baek and Yoon 26 found that groups facing high levels of multidimensional instability had significantly higher rates of unmet medical needs compared to groups in more stable employment situations.
The National Assembly Budget Office reports that Korea’s National Health Insurance (NHI) system is funded through mandatory contributions from employees and employers, along with government subsidies. 27 The NHI provides health insurance benefits to all citizens and registered foreigners, including E-9 visa holders. The NHI premium assessment in Korea applies different criteria to employed subscribers and regional subscribers. For employed subscribers, a single income-based system is used to calculate the premium. This is done by multiplying the subscriber’s monthly salary by a set premium rate. This straightforward method also applies to foreign workers, including those on E-9 visas. In contrast, the premium for regional subscribers, who are typically self-employed, is determined by a more complex method. Their premium is calculated by multiplying a comprehensive assessment score by a per-point cost. This score is derived from a detailed evaluation of various factors, including their income, property, and vehicles, to reflect their overall financial capacity. The coverage includes hospitalization, outpatient care, and diagnostics, with co-payments typically ranging from 20% to 60% depending on the service.
Formal healthcare coverage, which is the financial protection a healthcare system provides against medical expenses, 28 is distinct from effective healthcare access. A healthcare system’s formal coverage is evaluated by the proportion of the population insured, the range of services included, and the share of costs covered by insurance. 29 Robust healthcare coverage helps reduce out-of-pocket spending, thereby improving both healthcare accessibility and overall public health, and allowing individuals to obtain necessary medical care without facing financial hardship. 30
Effective access is the ability of an individual to receive appropriate healthcare services at the right time and place. 31 It depends on overcoming various barriers, often referred to as the “5 A’s”: availability (the sufficiency of medical resources including staff, beds, and equipment), accessibility (the ease of physical travel to a facility and the acquisition of information), affordability (the ability to pay healthcare costs), accommodation (the extent to which healthcare delivery methods consider patient convenience), and acceptability (the congruence of cultural and psychosocial factors). 32
For immigrants, particularly E-9 visa holders in Korea, this distinction is critical. Despite potentially having formal coverage, they face significant obstacles that hinder their ability to actually use healthcare services. These barriers include limited language proficiency, discrepancies in cultural norms related to healthcare, financial hardships, and a lack of information about the healthcare system. 33 These challenges create a critical gap between the formal coverage provided and its effective utilization, making immigrant populations particularly vulnerable to health disparities. 34
While the unmet healthcare needs rate among native Koreans is approximately 1%, 35 it reaches as high as 25% among low-skilled migrant workers. 36 Failure to address these unmet needs not only poses direct threats to individual health 37 but also exacerbates health disparities between migrants and native populations. 38 Addressing the unmet healthcare needs of precariously employed migrant workers is thus a critical step toward achieving health equity.
Existing research in Korea on the relationship between precarious employment and unmet healthcare needs has primarily focused on native workers.21,22,26,39 Studies addressing migrants have largely concentrated on the unmet healthcare experiences of marriage migrants, with limited attention to the link between precarious employment and health outcomes.40-42 Although some studies examine migrant workers,36,43 empirical analyses adopting a multidimensional approach to precarious employment among E-9 visa holders remain scarce. The aim of this study is to address gaps in prior research by identifying distinct types of precarious employment among E-9 visa holders and analyzing how both these types and their underlying indicators are associated with unmet healthcare needs.
Methods
Data and Participants
This study utilized microdata from the 2024 Survey on Immigrants’ Living Conditions and Labor Force, conducted by the Ministry of Justice and Statistics Korea. The survey, administered annually since 2017, includes health-related items in even-numbered years. Trained enumerators conducted face-to-face interviews to collect the data, ensuring comprehensive coverage of health and employment variables. The 2024 dataset is publicly available through Statistics Korea’s Microdata Integrated Service upon request, subject to approval.
The survey targeted individuals aged 15 years and older who had resided in Korea for at least 91 days or obtained naturalized citizenship within the past 5 years. A stratified systematic sampling approach was used: foreign residents were sampled by region and residency status; naturalized citizens by region, age, marital status, and former nationality. The initial sample included 24,039 respondents (20 000 foreign residents, 5000 naturalized citizens), from which 3248 E-9 visa holders were identified. To ensure data quality, respondents without clearly defined employment contract periods or weekly working hours were excluded. This study ultimately used 2576 individuals as the final analytical sample.
This study was exempted from review by the Institutional Review Board of University (IRB No. 1040173-202502-HR-008-02).
Measures
The dependent variable in this study was unmet healthcare needs, defined as the inability to access needed medical services between May 15, 2023, and May 14, 2024. Measuring unmet healthcare needs with a single-item subjective question offers several advantages. This method simplifies survey administration, allowing for the quick assessment of a respondent’s perceived medical needs. 44 As a result, it facilitates data collection and the assembly of large, representative samples, which in turn enhances the viability of a study. 44 This streamlined approach is widely adopted in numerous surveys to capture individuals’ subjective experiences of unmet healthcare needs.45,46
Precarious employment was measured using Kreshpaj et al.’s 14 framework, with 3 dimensions operationalized as follows: (1) employment insecurity via employment status (contract duration: non-regular <1 year, regular 1-3 years, regular >3 years) and weekly working hours (<50 vs ≥50 h), (2) income inadequacy via monthly wages (dichotomized at 3 million KRW, approximately 2250 USD as of August 2025, using an exchange rate of 1 USD = 1333 KRW) and income satisfaction (5-point scale), and (3) lack of rights and protection via workplace discrimination (yes/no) and workplace size (<5 vs ≥5 employees, as smaller workplaces are exempt from Labor Standards Act protections). Workplace size is used as a proxy measure, while other variables are directly assessed, in line with the framework’s multidimensional methodology.
Control variables included demographic and immigration-related characteristics likely to influence unmet healthcare needs. Demographic variables were selected based on Andersen’s Behavioral Model of Health Service Use 47 and included gender, age, education level, residential area, social networks (household size, number of Korean friends, and number of friends from the country of origin), and health. Immigration-related characteristics, conceptualized as reflecting cultural and structural differences between the host country and the migrants’ countries of origin, 34 included duration of residence in Korea, Korean-speaking ability, and country of origin.
Detailed measurement methods for all variables used in this study are presented in Table 1.
Descriptive Statistics of Demographic and Immigration-Related Characteristics.

Note. Categorical variables are presented as percentages (%), and continuous variables are presented as mean (standard deviation, SD).
KRW = Korean Won (3 million KRW is approximately 2250 USD).
Analytical Approach
The analysis was conducted in 4 stages. First, descriptive statistics were computed to examine the key characteristics of the sample, including frequencies, means, and standard deviations, to provide an overview of the respondents’ profiles.
Second, latent class analysis (LCA) was used to classify distinct forms of precarious employment. To select the optimal number of latent classes, various model fit indices were evaluated, including Akaike information criterion (AIC), Bayesian information criterion (BIC), sample-size adjusted BIC (saBIC), entropy, and Vuong–Lo–Mendell–Rubin adjusted likelihood ratio test (VLMR-LRT). After selecting the best-fitting model, the characteristics of each latent class were analyzed based on distribution ratio and item-response probability to identify the structure.
Third, multinomial logistic regression was utilized to investigate how demographic and immigration-related factors predict membership in specific latent classes, identifying key determinants of different types of precarious employment.
Finally, logistic regression analyses were conducted to examine: (1) the association between latent categories of precarious employment and unmet healthcare needs and (2) the relationship between individual indicators of precarious employment and unmet healthcare needs.
Odds ratios and 95% confidence intervals were calculated for both logistic and multinomial logistic regression analyses, with statistical significance determined using a 2-tailed test at P < .05. LCA was performed using Mplus Version 8, while all other statistical analyses accounted for sample weights and the complex stratified systematic sampling design using the “svy” command in STATA Version 15.
Typology of Precarious Employment: Latent Class Analysis
Optimal Number of Latent Classes
Table S1 presents the model fit indices used to determine the optimal number of latent classes. Lower values of the AIC, BIC, and saBIC indicate better model fit. 48 In this study, the three-class model was selected as the best fit based on the lowest BIC and saBIC values. The entropy value for the 3-class model was .750, exceeding the acceptable threshold of .6 and approaching the excellent threshold of .8. 48 Additionally, the VLMR-LRT assesses whether adding a class significantly improves model fit, with a P-value below .05 indicating a statistically significant improvement. 49 Considering these indices collectively, the three-class model was chosen for its balance of statistical fit and interpretability.
Characteristics of the 3 Classes
Table S2 reports the item-response probabilities for the 3 latent classes of precarious employment, identified based on indicators such as employment status based on contract duration, monthly wages, income satisfaction, working hours, workplace discrimination, and workplace size.
The 3 classes demonstrate distinct profiles based on income, employment stability, and discrimination. Class 1 (37.8%) is a vulnerable group with moderate income satisfaction and the highest rate of workplace discrimination (17.9%). Nearly all members (98.7%) earn less than 3 million KRW and have a relatively high rate of non-regular employment (4.9%). Class 2 (34.0%) is the largest group, characterized by high income satisfaction (70.5% reporting “very satisfied”). However, 96.5% still earn less than 3 million KRW, representing a group with stable employment but low wages. In contrast, Class 3 (28.2%) is the highest-earning and most stable group, with minimal discrimination. All members of this group earn 3 million KRW or more, and a significant portion (60.6%) have over 3 years of tenure, reflecting a secure and well-compensated status.
Based on the characteristics of each class, this study labeled Class 1, 2, and 3 as High Precarity Type, Moderate Precarity Type, and Low Precarity Type, respectively.
Predictors of Precarious Employment Types: Multinomial Logistic Regression Analysis
Table S3 presents the multinomial logistic regression results examining predictors of employment class membership, using the High Precarity Type as the reference. For the Moderate Precarity Type, a 1 to 3 years stay increased membership odds (OR = 1.40, P < .05), while non-metropolitan residence decreased odds (OR = .77, P < .05). For the Low Precarity Type, more co-national friends (OR = 1.20, P < .01), male gender (OR = 4.82, P < .001), and longer stays (1-3 years: OR = 1.63; 3-5 years: OR = 2.34; 5+ years: OR = 2.26; all P < .01) increased membership odds, while non-metropolitan residence (OR = .52, P < .001) and origins from Indonesia, Thailand, Cambodia, or Nepal (OR = .50-.54, P < .05 or P < .01) decreased odds. In summary, Class 2 represents the Moderate Precarity Type primarily influenced by length of stay and residential region, while Class 3 is the Low Precarity Type shaped by gender, ethnic networks, country of origin, and duration of stay.
Results
Descriptive Statistics
The sample’s demographic, immigration-related, and economic characteristics are presented in Table 1, with data weighted to correct for the complex sampling design.
This study’s sample (N = 2576) was predominantly male (90.60%) and fell into 2 main age cohorts: 15 to 29 years (45.38%) and 30 to 39 years (45.29%). A majority had a high school education (50.18%), while a quarter had a college degree or higher (25.15%). The residential distribution was nearly split, with 53.76% in non-metropolitan areas and 46.24% in metropolitan regions. The sample reported positive health outcomes, with 98.31% rating their health as fair or good, and only 4.69% reporting unmet healthcare needs.
The sample was diverse in terms of origin and time in Korea. The most common countries of origin were Cambodia (15.43%), Nepal (15.04%), and Vietnam (13.04%). In terms of length of stay, the largest groups had been in the country for 1 to 3 years (36.57%) or 5+ years (32.98%). Social networks appeared limited, with respondents reporting an average of only .70 Korean friends (SD = .03) and 1.81 friends from their home country (SD = .03). The average Korean-speaking ability was 2.84 on a 5-point scale (SD = .02).
Employment characteristics highlight the nature of work for this population. Over 62% of respondents held regular employment for more than 3 years, while a third worked on shorter-term contracts. Most reported working less than 50 h per week (68.86%) and earned under 3 million KRW per month (71.79%). Despite this, the average income satisfaction score was 4.14 on a 5-point scale (SD = .02). The majority of the sample worked in establishments with 5 or more employees (89.61%), and 11.61% reported experiencing workplace discrimination.
Associations Between Precarious Employment Types, Indicators, and Unmet Healthcare Needs: Logistic Regression Analysis
Table 2 presents the results examining the associations between the types of precarious employment and unmet healthcare needs. Employment stability was significantly associated with lower odds of unmet healthcare needs. Compared to Class 1 (High Precarity Type), Class 2 (Moderate Precarity Type) had significantly lower odds of unmet healthcare needs (OR = .53, 95% CI: .33-.94, P < .05). Class 3 (Low Precarity Type) exhibited an even lower likelihood (OR = .37, 95% CI: .21-.77, P < .01).
Associations Between the Types of Precarious Employment and Unmet Healthcare Needs.

Note. Class 1 refers to the High Precarity Type; Class 2 to the Moderate Precarity Type; and Class 3 to the Low Precarity Type. The Adjusted Model controlled for demographic and immigration-related variables listed in Table 1.
OR = odds ratio; CI = confidence interval; ref = reference.
P < .05. **P < .01.
Table 3 summarizes the associations between each precarious employment indicator and unmet healthcare needs. When analyzing individual precarious employment indicators, adjusted for demographic and immigration-related variables, monthly income and income satisfaction emerged as significant predictors. Migrant workers earning 3 million KRW or more had significantly lower odds of unmet healthcare needs compared to those earning less (OR = .48, 95% CI: .25-.93, P < .05). Higher income satisfaction was also associated with lower odds of unmet healthcare needs (OR = .69, 95% CI: .54-.88, P < .01). Conversely, experiences of workplace discrimination significantly increased the likelihood of unmet healthcare needs (OR = 2.43, 95% CI: 1.45–4.07, P < .01). No significant associations were found between unmet healthcare needs and employment status based on contract duration (regular employment of 1-3 years or over 3 years vs non-regular employment of less than 1 year; OR = 1.09, P > .05), weekly working hours (≥50 vs <50 h), or workplace size (≥5 vs <5 employees).
Associations Between the Indicators of Precarious Employment and Unmet Healthcare Needs.
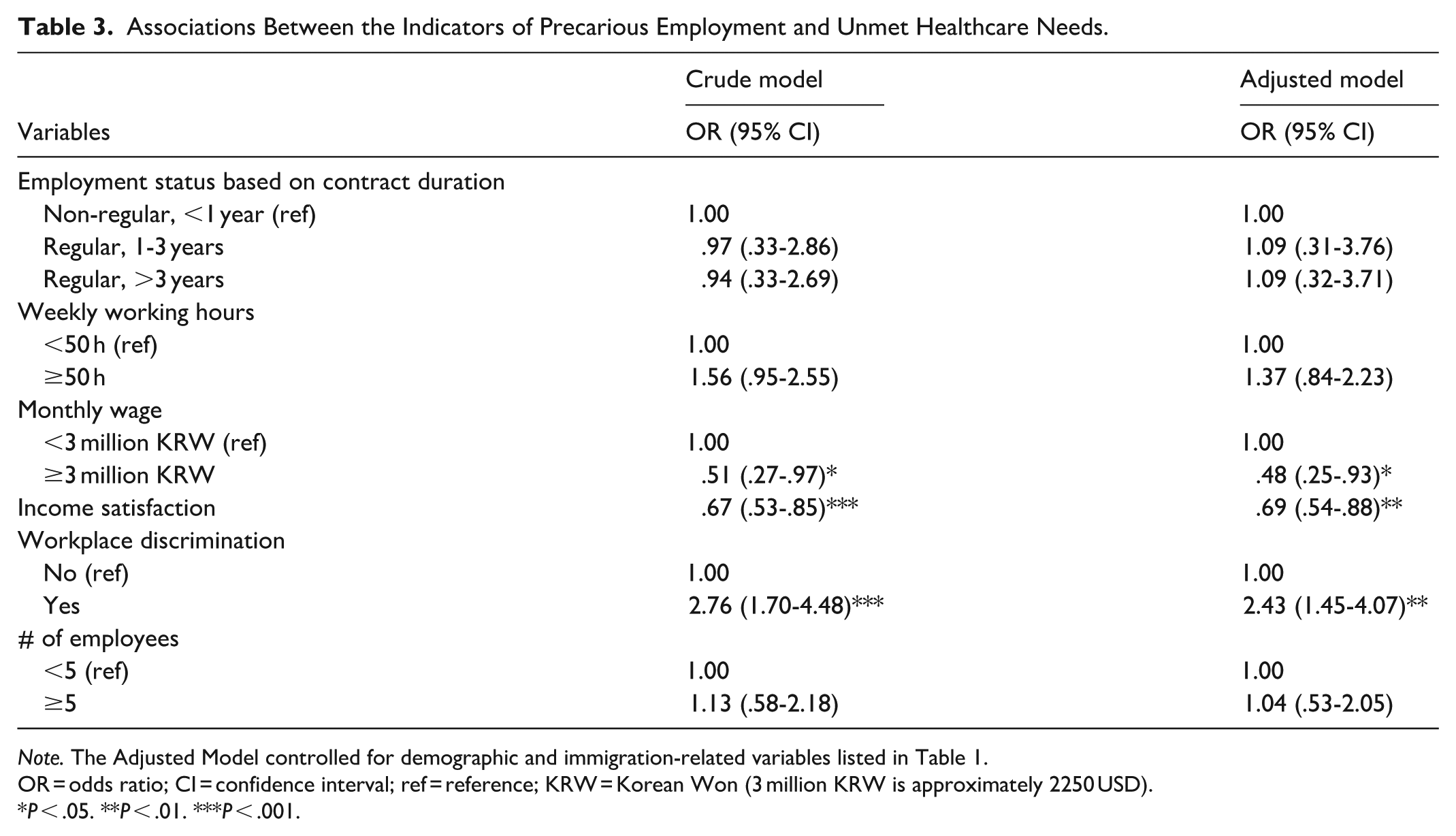
Note. The Adjusted Model controlled for demographic and immigration-related variables listed in Table 1.
OR = odds ratio; CI = confidence interval; ref = reference; KRW = Korean Won (3 million KRW is approximately 2250 USD).
P < .05. **P < .01. ***P < .001.
Discussion
This study explored how various types of precarious employment relate to unmet healthcare needs among low-skilled migrant workers holding E-9 visas in Korea. The LCA identified 3 distinct employment profiles, each demonstrating a statistically significant relationship with unmet healthcare needs. Compared to those in the “High Precarity Type,” individuals classified under the “Moderate Precarity Type” and “Low Precarity Type” were significantly less likely to report unmet healthcare needs. Additionally, this study reveals that individual indicators of precarious employment, such as contract duration, working hours, and workplace size, do not significantly correlate with unmet healthcare needs. However, higher monthly income and greater earnings satisfaction serve as protective factors, while workplace discrimination represents a critical structural barrier to healthcare access. These findings highlight the importance of a comprehensive approach that considers multiple dimensions of precarious employment conditions to better understand and address gaps in healthcare access among migrant workers in Korea.
Unmet Healthcare Needs Among Migrant Workers
The findings indicate that 4.69% of low-skilled migrant workers reported unmet healthcare needs, a rate lower than the 25% reported by K.-T. Kim and colleagues, 36 but higher than the 1% observed among native Koreans. 35 This discrepancy can be attributed to differences in sampling methodologies. K.-T. Kim and colleagues employed non-probability sampling with a sample size of 700, 36 whereas this study utilized systematic sampling with national representative weights, providing more robust estimates.
The 4.69% prevalence rate highlights persistent health disparities among migrant workers who are formally enrolled in the national health insurance system but whose access to health services is severely limited due to structural problems associated with precarious employment. In particular, barriers such as language barriers and cultural differences are likely to impede access to health services. 34 Furthermore, the need to maintain an E-9 visa for legal residency may discourage workers from seeking health services due to concerns about visa cancellation, especially in unstable employment environments. 5 These findings highlight the importance of addressing systemic barriers faced by migrant workers to reduce health inequities and increase access to health services.
Precarious Employment Types and Unmet Healthcare Needs
The LCA revealed 3 distinct categories of precarious employment, each significantly linked to unmet healthcare needs. The “High Precarity Type” exhibited a notably higher probability of unmet healthcare needs compared to the “Moderate Precarity Type” (OR = .53, P < .05) and the “Low Precarity Type” (OR = .37, P < .01). These findings are consistent with prior research,21,22,26 which indicates that employment precarity experiences unmet medical needs.
While prior studies primarily focused on the relationship between single indicators, such as contract type 22 or employment status,39,50 and unmet healthcare needs, this study adopts a multidimensional approach to employment precarity. By integrating factors such as job continuity, working hours, wage disparities, and workplace size, the analysis revealed that groups experiencing precarious employment are more likely to face unmet healthcare needs compared to those in more stable conditions. These findings highlight the theoretical and practical significance of a multidimensional framework in explaining disparities in healthcare access.
Precarious Employment Indicators and Unmet Healthcare Needs
This study reveals a complex relationship between individual factors of precarious employment and unmet healthcare needs, with some findings aligning with prior research while others present notable contrasts. Consistent with existing literature, elevated monthly wages (OR = .48, P < .05), higher income satisfaction (OR = .69, P < .01), and the presence of workplace discrimination (OR = 2.43, P < .01) were all identified as significant determinants of unmet healthcare needs. Specifically, higher income and income satisfaction were found to reduce the likelihood of unmet needs,38,43,51 while workplace discrimination was a significant contributing factor.5,52-54 In contrast to previous studies, however, this research found no significant association between unmet healthcare needs and several other factors, including employment status based on contract duration, weekly working hours, and workplace size. These findings diverge from a body of research that has previously linked non-regular employment,39,50,55 extended work hours,8,39,56,57 and smaller workplaces21,39 to greater barriers in accessing health services.
This seeming contradiction highlights the limitations of analyzing these factors in isolation.
First, financial precarity and workplace discrimination are significant, intertwined barriers to healthcare access. Migrant workers who face discrimination are often trapped in low-wage, informal jobs with few social protections.52,53 This combination of economic insecurity and psychological stress tends to create a powerful disincentive to seek medical care. 54 The fear of losing wages or their job for taking sick leave is compounded by a hostile work environment, 58 making them less likely to seek care when they need it. 5
Second, an analysis of unmet healthcare needs must look beyond simple indicators of precarious employment, such as contract length or weekly working hours. These factors are not reliable predictors on their own. For example, a worker with a long-term contract may still face significant barriers to care due to low wages 51 or chronic discrimination. 52 Conversely, shorter working hours may not guarantee better access if they lead to financial instability.43,58 It is the unique combination of factors, such as a flexible schedule with a living wage or, conversely, a permanent position with low pay and high-stress conditions, that truly determines a worker’s ability to access care. 26
Third, re-conceptualizing workplace size is crucial for understanding its role in healthcare access. Although larger companies often provide formal benefits, these are not always equally accessible to all employees, particularly those on the margins.8,9 Conversely, some smaller workplaces may offer a more supportive and flexible environment. 59 Therefore, the true determinants of healthcare access lie in the collective conditions of the workplace, including wage levels, organizational culture, and the practical application of benefits, rather than simply its size.
In conclusion, this study demonstrates that a multidimensional framework is essential for understanding the barriers related to unmet healthcare needs among precarious workers. By moving beyond simple causality, this approach provides a more thorough understanding of how the various aspects of precarious employment combine to create systemic, interconnected barriers to healthcare access.
To improve healthcare access for precariously employed migrant workers, this study proposes several policy recommendations. First, legislation mandating the prohibition of workplace discrimination is essential to foster equitable work environments, thereby enhancing employment stability and promoting healthcare access. Second, given that Korea’s NHI system requires out-of-pocket copayments, policies to reduce these costs for economically disadvantaged migrant workers could significantly improve healthcare utilization. Third, reforming the EPS by easing restrictions on workplace mobility and enhancing visa stability could alleviate fears of job loss, thereby facilitating access to medical services.
Despite its contribution, this study has several limitations. First, in an effort to ensure data quality, this study systematically excluded respondents with ambiguous employment contract periods or incomplete data on weekly working hours. However, this methodological decision may have introduced a selection bias, as it disproportionately removed some of the most precariously employed workers from the sample. Future studies should employ targeted sampling strategies or alternative data collection methods to mitigate this specific form of selection bias. Second, cross-sectional studies are ineffective for examining temporal trends or determining causality. Longitudinal studies are needed to explore the dynamic interplay between employment precarity and healthcare access. Third, due to constraints of secondary data, key indicators of precarious employment, such as union membership, social insurance coverage, and direct versus indirect employment, were not included. Future research should incorporate these indicators to strengthen multidimensional analyses. Fourth, unmet healthcare needs were measured as a binary variable, which did not account for the severity, frequency, or specific reasons for unmet needs (eg, financial constraints, time limitations, or lack of information). The limitations of secondary data further restricted the inclusion of diverse data sources. Future studies should employ more nuanced measures of unmet needs and conduct subgroup analyses by reason. Fifth, the study could not account for additional variables potentially influencing unmet healthcare needs, such as distance to healthcare facilities, transportation access, or service provider characteristics, 60 due to secondary data limitations. Future research should explore these factors to provide a more comprehensive understanding of healthcare access disparities.
Conclusion
This study examined the link between precarious employment and unmet healthcare needs among E-9 visa holders in Korea. Using the LCA, 3 employment profiles were identified: High, Moderate, and Low Precarity Types. Compared to the High Precarity Type, those in Moderate and Low Precarity Types were less likely to report unmet healthcare needs. Individual factors such as contract length, working hours, and workplace size showed no significant link to unmet needs, suggesting that analyzing employment indicators in isolation is insufficient. Higher income and earnings satisfaction were protective, while workplace discrimination was a major barrier to healthcare access. The findings highlight the need for a holistic approach to precarious employment conditions and systemic reforms in the Employment Permit System to improve healthcare access for E-9 visa holders. Finally, this study advances several policy recommendations aimed at enhancing healthcare access for precariously employed migrant workers holding E-9 visas in Korea.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251390282 – Supplemental material for Unmet Healthcare Needs in Unstable Jobs: Perspectives from Low-Skilled Migrant Workers in South Korea
Supplemental material, sj-docx-1-inq-10.1177_00469580251390282 for Unmet Healthcare Needs in Unstable Jobs: Perspectives from Low-Skilled Migrant Workers in South Korea by Min-Chul Hwang in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
This study was conducted using secondary data analysis of microdata provided by Statistics Korea and the Ministry of Justice. We express our sincere gratitude to Statistics Korea and the Ministry of Justice for making this research possible through their data provision.
Ethical Considerations
This study received an exemption from the Institutional Review Board of Sunchon National University (IRB No. 1040173-202502-HR-008-02).
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Other Identifying Information
No additional information is included that might compromise the anonymity of the author, their institution, funders, or approval committees.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.