
Abstract
Young adulthood is a critical period for identity formation, yet young adults with mental health–related disabilities often engage with care systems that erode rather than support selfhood. This qualitative study draws on critical realist metatheory, which aligns with interpretive inquiry while enabling layered explanation. Conducted in partnership with young adult co-researchers with lived experience of mental health–related disabilities from equity-deserving communities, the study treats participant narratives as situated meaning and as analytic entry points into the institutional, relational, and structural dynamics that generate persistent inaccessibility. Thirteen young adults with lived experience of mental health–related disabilities and unmet healthcare needs described extensive interactions with clinics, hospitals, and community services across Canada. Despite this, they remained unseen and unmet. Functional impairments collided with institutional demands for legibility, coherence, and compliance, producing recurring patterns of misrecognition, fragmentation, and withdrawal. Critical realism’s stratified ontology distinguishes between what is experienced (empirical), what happens whether or not it is experienced (actual), and the underlying forces that generate those events (real). Through abductive and retroductive reasoning, the study identifies five explanatory clusters and presents the Rupture–Repair Roundabout, a model that illustrates how health systems can either destabilize or scaffold young adults’ emerging selves. Participants described access as extractive rather than supportive, requiring strategic masking and self-erasure to remain eligible. Findings suggest that addressing unmet healthcare needs requires not only expanded services but also a structural and relational reorientation toward attuned, identity-holding care. Without this, healthcare risks functioning not as a site of healing but as a site of existential undoing.
Keywords
Introduction
Young adulthood is a period of profound transformation (De Vries et al., 2025; Erikson, 1980; Marcia, 1966). More than a transition between adolescence and full adulthood, this period is foundational to the formation of selfhood and the pursuit of a meaningful life trajectory. Drawing from Erikson’s (1980) seminal work, identity formation involves the exploration of life possibilities and the commitment to a sense of who one is and intends to become. Adolescents and young adults begin to integrate their past, present, and future into autobiographical meaning-making, producing stories that help answer existential questions of who they are and why their life matters (Branje et al., 2021).
Identity and meaning in life are therefore deeply interwoven: while identity helps individuals define the protagonist of their life story, meaning provides the thematic arc or purpose that renders that story intelligible and worthwhile (Negru-Subtirica et al., 2016). Historically, societies have offered scaffolding for these developmental processes (Turner et al., 1969). Institutions such as extended family, local community, religious practice, and collective ritual once provided young people with the relational and symbolic tools needed to assemble a sense of purpose and place. However, the erosion of these communal structures has shifted the burden of self-formation to young adults themselves (Alderson & Morrow, 2020; De Vries et al., 2025; Green & Pescosolido, 2024). In many late-modern contexts, young adults must now navigate identity development amid institutional discontinuity, economic instability, and fragmented systems of care.
These processes of identity and meaning-making are deeply implicated in how young adults experience and access healthcare. Encounters with care systems—whether validating or dismissive—can affirm, fracture, or reshape a young person’s sense of coherence and worth. For young adults living with mental health–related disabilities, such as depression or anxiety, these challenges are amplified (Statistics Canada, 2024). Mental health–related disabilities can interfere with the cognitive, emotional, and relational capacities needed to manage daily life, sustain relationships, and develop coherent self-narratives (Luyckx et al., 2008; Marin & Shkreli, 2019). These effects are often far-reaching, affecting both daily functioning and long-term life trajectories (Aass et al., 2021; Malla et al., 2018). While healthcare access could offer opportunities for intervention, it remains inconsistently realized for young adults with mental health–related disabilities. Recent research has shown that young adults with mental health–related disabilities experience significantly higher rates of unmet healthcare needs (Rao, 2025). However, there remains limited understanding of how and why these inequities persist.
While it is possible that functional impairments themselves complicate engagement with care, the specific processes through which mental health–related disabilities intersect with healthcare systems to produce exclusion are not well understood. This qualitative study draws on Bhaskarian critical realism (Bhaskar, 2008, 2009; Bhaskar & Danermark, 2006), a metatheoretical approach that retains the foundational commitments of qualitative research while enabling a move toward explanation. As Sims-Schouten and Riley (2019) note, critical realism allows researchers to examine how discourse, materiality, embodiment, and institutional context converge in shaping participant meaning-making. Critical realism values participant narratives as analytic entry points into deeper generative mechanisms (Koopmans & Schiller, 2022).
This study is a core component of the Helping Enable Access and Remove Barriers To Support (HEARTS) study (Rao, 2023; Rao, Dimitropoulos, Jardine, et al., 2024). The HEARTS study is a Canada-wide patient-oriented research study (Rao, 2022) led by a team of 16 young adult co-researchers with lived and living experiences of mental health–related disabilities, unmet healthcare needs, and systemic minoritization (Sotto-Santiago, 2019), alongside three institutional researchers, one of which is a doctoral candidate. The co-researchers represent all 10 Canadian provinces, living in urban, rural, and remote communities, and bring diverse cultural, gender, and socio-economic perspectives, including South Asian, Vietnamese, Filipino/x, Indigenous, Black diasporic, and Two-Spirit, Lesbian, Gay, Bisexual, Transgender, Queer, and other sexual and gender-diverse identities.
The HEARTS study developed an egalitarian approach grounded in the principle of Primus inter PARES, or “first among equals” (Rao, et al., 2024), and enacts equality in decision-making and co-creation of outputs. This integration of lived expertise with academic rigor forms the foundation of the HEARTS study. Each young adult co-researcher was involved throughout the research process. Detailed descriptions of the study design are available elsewhere (Rao, 2023; Rao, Dimitropoulos, Jardine, et al., 2024; Rao, Jardine, et al., 2024, 2025). Grounded in critical methodological pluralism, the HEARTS study integrates extensive (quantitative) and intensive (qualitative) methods to support multi-level causal explanation (Danermark, 2002). This qualitative study represents the intensive component and is guided by the critical realist research question: from the perspectives and experiences of young adults with mental health–related disabilities, what mechanisms contribute to healthcare inaccessibility and unmet healthcare needs, and how do functional impairments shape their capacity to access and engage with care?
Materials and Methods
This qualitative study represents the intensive arm of the HEARTS project and is situated within a Bhaskarian critical realist metatheory (Bhaskar, 2008). Semi-structured interview data were analyzed using critical realist thematic analysis to identify mechanisms shaping healthcare access among young adults with mental health–related disabilities. The sections that follow outline the recruitment approach, participant characteristics, ethical safeguards, and analytic procedures used to support rigorous causal explanation.
Recruitment and Study Participants
Recruitment followed a purposive sampling strategy consistent with criterion-i approaches, selecting participants based on direct experience of the phenomenon of interest (Palinkas et al., 2011). To address known limitations of conventional criterion-i sampling, a maximal variation strategy was incorporated to enhance explanatory depth and support intersectional analysis (Palinkas et al., 2011). Extensive data from the HEARTS study (Rao, 2025) informed the recruitment criteria by identifying subgroups of young adults with the highest and lowest rates of unmet healthcare needs, mood and anxiety disorders, and functional impairments. This strategic sampling enabled the identification of both convergent and divergent patterns across cases. Participants at both ends of the spectrum were not seen as more or less valid but as uniquely positioned to illuminate how mechanisms manifest under different conditions. Including both poles allowed us to theorize why similar impairments result in different access trajectories and to identify hidden dynamics that might be missed in more homogeneous samples. This design aligns with critical realist logics of inquiry, where explanatory robustness is strengthened by examining variation across context and condition, rather than assuming uniform causality.
This process was supported by a demographic and impairment screener that included the World Health Organization Disability Assessment Schedule (WHODAS 2.0) (WHO, 2010). Recruitment prioritized young adults aged 18 to 30. For the purposes of this study, young adulthood refers to individuals aged 18 to 30. This extended range reflects a transitional life stage in which education, employment, identity, and relationships are still forming, often amid structural and relational instability. For young adults with mental health–related disabilities, these transitions frequently intersect with episodic impairment, fragmented supports, and policy thresholds that shape access to care. This framing situates young adulthood as both a developmental and structural category, rather than a purely chronological one (Gustafson et al., 2025; McGorry et al., 2025; Rao et al., 2026).
Consistent with the study’s justice-orientation, participants were purposefully recruited from equity-deserving groups with lived experience of mental health–related disabilities. Recruitment intentionally engaged individuals with lived experience navigating healthcare systems, capable of providing experientially grounded insight into systemic barriers, service design, and relational dynamics. Potential participants were identified through the Access Research Registry, a voluntary database managed by Alberta Health Services (AHS) in Alberta, Canada, that includes individuals who have expressed interest in contributing to health research. Outreach prioritized young adults whose decision to join the registry reflected a purposeful intent to share their stories, improve services, or advance change. In this way, participant selection was guided by mutuality and reciprocity, ensuring the research relationship was relational rather than extractive (Smith, 2021; Wilson, 2008).
A clinical research coordinator screened individuals based on initial inclusion criteria: young adults aged 18 to 30 with self-identified mental health–related disabilities, specifically depression and/or anxiety. Eligible individuals received an email containing a plain-language overview of the study and links to optional accessible materials, including short videos, blogs, and zines co-developed with young adult co-researchers. Interested participants were invited to meet with the lead researcher to discuss the study, explore alignment with their goals, and review informed consent before committing to participation. Those who wished to proceed completed a demographic and functional impairment screener. The lead researcher conducting recruitment had no clinical or therapeutic relationship with participants and was unaffiliated with their service providers. Individuals who declined or did not respond were not contacted further.
The study was designed to fundamentally reconfigure the research encounter, moving beyond accommodation toward structural and relational transformation. Grounded in a methodological commitment to radical hospitality (Piepzna-Samarasinha, 2018; Watkins et al., 2019), the study approached research as a relational space where participants’ ways of being, knowing, and mattering could take shape. Radical hospitality, as conceptualized here, reframes participation as an act of welcome, reciprocity, and mutual recognition, prioritizing the epistemic, emotional, and existential realities of those historically excluded from knowledge creation.
This ethos departed from conventional models of accessibility, which often emphasize barrier reduction as a technical or individual adjustment. Instead, participation was intentionally structured around the needs, rhythms, and capacities of young adults living with mental health–related disabilities. Accessibility was understood not as retrofitting an existing design but as constructing conditions in which different ways of being, knowing, and moving through the world could flourish. This methodological architecture was operationalized across all phases of the study.
Participants selected their preferred mode of engagement (phone, video, text, email, or in-person), with options to revise, pause, or withdraw at any time without penalty. Interviews could occur in a single sitting or unfold across multiple encounters. Of the thirteen participants, eight chose to participate through multiple touchpoints, including phone calls, emails, Zoom, and text, often spaced out over days, weeks, or, in one case, six months. This temporal flexibility accommodated life disruptions such as hospitalization, caregiving, or episodic impairments and enabled participants to revisit unfinished thoughts, expand on difficult topics, and engage more deeply as familiarity and trust increased. These principles were informed by crip time and slow scholarship (Kaufman et al., 2024; Nolan, 2025), centering the understanding that relational, epistemic, and ontological care must structure research participation, not be appended thereafter. All participants provided informed consent prior to participation, with written consent obtained by the lead researcher.
Research Ethics
This study received ethics approval from the Conjoint Health Research Ethics Board at the University of Calgary (REB22-1063) and operational approval from AHS. Ethics in the HEARTS study was an ongoing, relational, and reflexive process embedded throughout every stage of the research (Rao, Dimitropoulos, & Patten, 2025). The study design prioritized safety, accessibility, and reciprocity. The HEARTS study developed an ethics model to guide the work and was operationalized through the appointment of a Lived Experience Ethics Officer to co-lead ethical deliberations, a Community Builder role and Buddy System to support peer connection and well-being, and an independent Ombudsperson with an Incident Reporting process to ensure accountability and transparency, among others. These measures, co-developed with co-researchers, reflect an ethics-in-practice framework grounded in care, inclusion, and mutual respect, consistent with the study’s egalitarian and justice-oriented principles.
Data Collection
Data collection consisted of two phases: initial screening and qualitative interviews. The screener gathered demographic, social, and health-related information, including adapted items from the WHODAS 2.0. Semi-structured interviews were conducted using a guide developed to support causal inquiry, consistent with Step 1 of critical realist thematic analysis (Fryer, 2022). Interview questions explicitly distinguished among experiences (subjective perceptions), events (what occurred), and generative mechanisms (the underlying structures or forces producing those events). Participants selected their preferred mode of engagement (e.g., telephone, video conferencing, text, email, or in person), with the option to revise modes as needed.
Interviews varied in format and duration based on participant capacity. In cases where participants engaged across multiple modalities or sessions, each discrete interaction was treated as a separate transcript to preserve temporal and contextual integrity. Audio-based interviews were recorded with consent and transcribed verbatim; text-based and email interviews were analyzed in their original written form. Participants were invited to revisit, revise, or supplement their narratives following initial engagement. This recursive process reflected the study’s commitment to epistemic justice, relational attunement, and participant agency, supporting the surfacing of insights that evolved over time. Interview pacing and structure were adapted responsively in real time to accommodate fluctuating cognitive, emotional, and relational capacities.
Thirteen participants completed interviews, with sample size guided by the critical realist principle explanatory sufficiency, which refers to the point at which additional cases no longer contribute new causal insights, and by the complementary concept of information power (Malterud et al., 2016, 2021; Rao, Dimitropoulos, Milaney, et al., 2024). Collectively, these frameworks emphasize theoretical depth and causal adequacy rather than numerical saturation or frequency-based criteria (Danermark, 2002; Fletcher, 2017; Fryer, 2022; Sayer, 1997, 2000; Wiltshire & Ronkainen, 2021). All data were de-identified and stored on encrypted servers managed by University of Calgary, in accordance with institutional and health system data security protocols.
Notably, the study operated with three distinct but interrelated layers of questioning. First, the interview guide consisted of questions posed directly to participants, focused on their lived experience, emotional responses, healthcare navigation, and personal interpretations of need, care, and exclusion. These questions were open-ended, situated, and grounded in qualitative traditions of relational and experiential inquiry. Second, following data collection, the analysis was structured around abductive and retroductive questions posed to the data, not to participants. Abduction involved re-describing participants’ accounts using relevant theoretical frameworks; retroduction asked what underlying structures or mechanisms must exist for these accounts to make sense across contexts. Finally, at the deepest level, the study addresses philosophical questions about the intransitive dimension of reality. The first author conducted all interviews and transcriptions, in line with participants’ preferences and logistical considerations. Participants were offered the option to be interviewed by a young adult co-researcher; however, all elected to be interviewed by the lead researcher.
Data Analysis
This study employed critical realist thematic analysis developed by Fryer (2022). Critical realist thematic analysis explicitly conceptualizes themes as causal explanations of observed patterns (Archer, 2020). This analytic stance is especially valuable in health research, where events such as service exclusion or unmet healthcare needs are not reducible to individual factors but are co-produced through dynamic interactions across institutional, relational, and structural levels of reality (Koopmans & Schiller, 2022; Lauzier-Jobin & Houle, 2021). From a qualitative perspective, this enables a layered form of analysis that attends closely to participants’ accounts while situating them within the broader structures and mechanisms that shape experience (Fryer, 2022; Sims-Schouten & Riley, 2019). This study followed critical realist thematic analysis’ five interconnected stages, including (1) developing causal research questions; (2) familiarizing with the data; (3) applying, developing, and reviewing codes; (4) identifying and refining causal themes; and (5) synthesizing and reporting the findings.
In critical realism, causality is not synonymous with statistical association or predictive power (Bhaskar, 2008; Koopmans & Schiller, 2022; Maxwell, 2004; Mingers & Standing, 2017). Rather, it refers to the generative mechanisms that produce particular outcomes when activated under specific contextual conditions. These mechanisms may be structural, cultural, or psychological in nature. They may remain latent, become counteracted, or be expressed in different ways depending on the setting. Importantly, the use of causal language in this study does not reflect a positivist or deterministic orientation. Nor does it dismiss the insights of interpretivist scholarship. Instead, it reflects a different explanatory ambition. Rather than remaining at the level of interpretation alone, this study seeks to understand the conditions of possibility for the experiences described. In this way, it integrates participant meaning-making into a broader explanatory project. Within critical realism, interpretation and explanation are not competing goals but complementary dimensions of rigorous social inquiry.
Causal inference in this study is pursued through abductive and retroductive reasoning. Abduction re-describes participant accounts through relevant theoretical concepts, while retroduction asks what underlying mechanisms or conditions must exist for these accounts to be intelligible (Bhaskar & Danermark, 2006; Danermark, 2002; Maxwell, 2012). These strategies do not claim universal laws but aim to generate plausible, theory-informed explanations for why young adults with mental health–related disabilities encounter unmet healthcare needs despite sustained help-seeking.
Consistent with qualitative research traditions that value contextual depth, reflexivity, and multiple ways of knowing (Cannella & Lincoln, 2009; Denzin & Lincoln, 2011; Guba & Lincoln, 2005), this study treats knowledge as partial, situated, and fallible. Critical realist thematic analysis enabled participant accounts to be interpreted not in isolation but within the wider social, cultural, and institutional structures that contour them. By reasoning from recurring experiences toward underlying mechanisms, the analysis offers theoretically grounded explanations that remain responsive to the complexity of lived realities. Data analysis proceeded through critical realist thematic analysis’ interconnected stages. Screener data were anonymized, cleaned, and organized into structured spreadsheets to support analytic context. All data, including transcripts, screener summaries, and post-interview reflections, were uploaded to NVivo, a qualitative data management platform used for data organization, annotation, memoing, and coding.
Step 2: Familiarization
Multiple full readings of each transcript were conducted. The first round emphasized immersion and open memo-writing; the second centered on identifying analytic tensions, including silences, contradictions, and conceptual patterns. Reflexivity was practiced throughout, foregrounding the epistemic fallibility of emerging interpretations, the influence of researcher positioning, and the application of judgmental rationality—the systematic adjudication between competing explanations (Alderson, 2021; Isaksen et al., 2024; Quraishi et al., 2022; Rybczynska-Bunt et al., 2021). Young adult co-researchers played a critical role, helping to surface interpretive risks, clarify ambiguous meanings, and identify latent mechanisms that might otherwise remain obscured.
Step 3: Coding
Descriptive codes were developed inductively, capturing both surface-level (semantic) content and underlying (latent) patterns of meaning. Coding proceeded iteratively across small batches of transcripts, identifying within- and cross-case demi-regularities—that is, recurrent but non-universal patterns of experience characteristic of open systems (Bhaskar, 2008). Codes were annotated with memos to document evolving abductive and retroductive reasoning. Early patterns were reviewed for co-occurrence, divergence, contradiction, silence, and absence, building toward causal explanations.
Step 4: Theme Development
Data-led codes were grouped into causal families, defined as clusters of mechanisms operating at similar ontological levels (e.g., structural, cultural, and relational). These families were iteratively refined based on theoretical coherence and explanatory reach. Causal families were then organized into broader causal clusters, reflecting how different mechanisms interacted to shape healthcare inaccessibility and unmet healthcare needs. Causal constellations (patterns of mutually reinforcing mechanisms) and causal chains (sequences of linked mechanisms across ontological levels) were mapped to model the interplay of causal forces within open systems.
Throughout, analysis remained explicitly retroductive. Rather than taking accounts at face value or staying at the level of thematic description, this involved working backward from what participants said to theorize the deeper social, institutional, and relational mechanisms that could explain those patterns. Retroduction allowed the analysis to move beyond documenting what was said to asking why such patterns persist, even across different people, places, or systems. Potential mechanisms were evaluated for comprehensiveness, depth, coherence, and transfactual relevance. Mechanisms were mapped as primary (central), secondary (contextual), contingent (locally relevant), or unsupported (insufficient evidence). A reflexive audit was conducted to examine how researcher assumptions, disciplinary background, and epistemic oversights may have influenced the visibility of mechanisms, in alignment with critical realist thematic analysis’ emphasis on epistemic humility.
During analysis, young adult co-researchers participated in group sessions focused on abductive and retroductive reasoning, reviewing preliminary codes and developing explanatory propositions. These sessions allowed for interpretive dialogue that integrated experiential and theoretical insight. Institutional co-authors provided iterative feedback on coding and thematic synthesis, and senior critical realist researchers and methodological experts offered conceptual review and guidance to ensure analytic coherence and rigor. This collective engagement reflects the principle of judgmental rationality within critical realism and the participatory commitments of the HEARTS study.
Step 5: Reporting
Causal diagrams were created to visualize explanatory clusters as critical realist artefacts, representing explanatory propositions grounded in empirical data and conceptual reasoning. Consistent with Fryer’s (2022) guidance on reporting critical realist thematic analysis findings, these diagrams are not supplemental but constitutive of the analytic process itself. Fryer identifies the production of causal explanation diagrams as integral to Step 5 of critical realist thematic analysis such that it is an explicit means of communicating how empirical experiences, actual events, and real-level mechanisms interrelate to generate observed outcomes. Accordingly, the figures presented in this study follow this convention: the first (empirical) domain includes direct participant quotations; the middle (actual) domain illustrates recurrent events across cases; and the final (real) domain theorizes underlying generative mechanisms. This visual schema therefore operationalizes critical realist thematic analysis’ stratified ontology, allowing readers to trace the reasoning from lived experience to causal explanation. Full details of the NVivo workflow, plain-language summaries and causal family summaries, and judgmental rationality details can be found on Open Science Framework (OSF) (https://osf.io/uc6j5).
Data Quality
Data quality was assessed using the principles outlined in critical realist thematic analysis, across three interrelated dimensions: descriptive, interpretative, and theoretical validity (Christodoulou, 2024; Fletcher, 2017; Fryer, 2022; Maxwell, 2012; Wiltshire & Ronkainen, 2021). Descriptive validity referred to the accuracy of the recorded data, including verbatim transcription of audio-recorded interviews and preservation of original language in text-based contributions. Interpretative validity was supported through careful attention to participant meaning, particularly during the abstraction of lived experiences into dispositional themes.
Theoretical validity was assessed through the retroductive development of causal explanations that coherently accounted for patterns and contradictions within and across transcripts. Additionally, the study’s design enhanced data quality by creating conditions for reflective, in-depth participant engagement. These practices reduced pressure for immediate responses and enabled richer insight into both personal experiences and systemic structures. Researchers engaged in systematic reflexivity, documenting analytic decisions transparently and evaluating explanatory propositions through judgmental rationality. Final explanatory clusters demonstrated theoretical coherence, causal plausibility, and sensitivity to the lived experiences and social locations of participants.
Findings
Sociodemographic Characteristics of Young Adults (18–30) With Mental Health–Related Disabilities (N = 13)
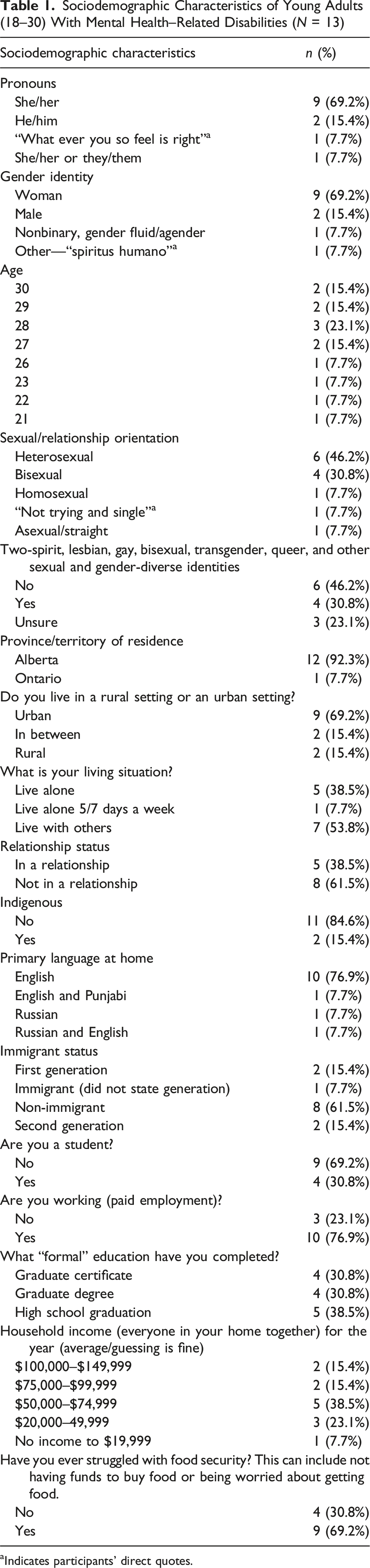
aIndicates participants’ direct quotes.
In accordance with the conventions of critical realist thematic analysis, synthesis and reporting of findings are presented using an integrated visual schema that maps empirical experiences, actual events, and real-level causal mechanisms (Fryer, 2022). This format is designed to make visible the stratified ontology and explanatory logic central to critical realist analysis. In each figure, the first box contains participants’ direct quotations, representing the empirical layer of the analysis from which higher-level patterns and mechanisms were derived. Subsequent boxes trace the analytic movement through the actual and real layers, showing how experiential accounts were interpreted and explained through causal reasoning. At the same time, we recognize that this structure may not resonate with all readers, particularly those whose ways of knowing are more relational, affective, or narrative in form. To support different ways of engaging with the data, and consistent with the study’s commitment to radical hospitality, we created an expanded narrative supplement that can be found on OSF (https://osf.io/uc6j5). This companion section offers an alternate mode of engagement. Below, we present five explanatory clusters. Each cluster identifies recurrent patterns of experience and the generative and causal mechanisms that produce or constrain access to mental healthcare.
Cluster A: Symbolic Violence in Diagnosis: Causal Mechanisms of Misrecognition, Fragmentation, and Epistemic Erosion
Figure 1 illustrates how diagnostic processes simultaneously structure care access and fragment identity. Participants were misrecognized, misdiagnosed, or dismissed, especially when their identities or behaviors diverged from clinical expectations. Although all participants identified as living with depression and/or anxiety, several also described additional or intersecting diagnostic and neurodevelopmental identities, including borderline personality disorder, post-traumatic stress, autism spectrum conditions, and attention-deficit/hyperactivity disorder. This diagnostic plurality was analytically significant. Participants’ narratives revealed that navigating multiple or shifting diagnoses produced profound fragmentation, both in how they were understood by others and in how they understood themselves. Diagnostic multiplicity often resulted in competing treatment pathways and contradictory explanations, reinforcing experiences of misrecognition and disbelief. The more layered and shifting their diagnostic histories became, the more participants described feeling rendered incoherent or less trustworthy within systems that privilege stable hierarchies of diagnosis and linear recovery trajectories. Cluster A: Symbolic violence in diagnosis: Causal mechanisms of misrecognition, fragmentation, and epistemic erosion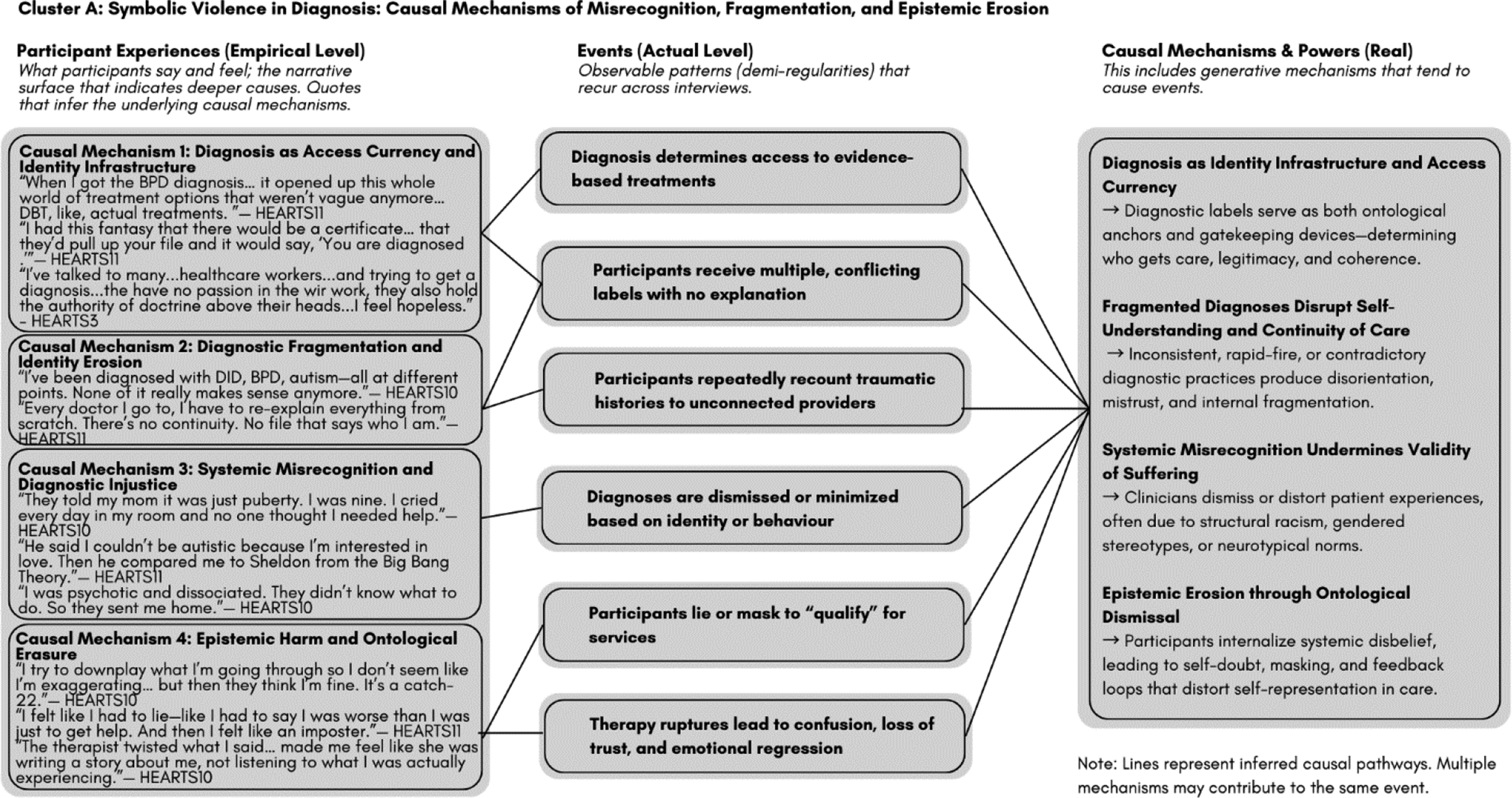
Cluster B: Misrecognition of Complexity as Noncompliance: Cultural and Epistemic Mechanisms of Exclusion
Participants navigating internal, episodic, or affective impairments were frequently interpreted as disengaged. Cultural norms equating coherence with capacity contributed to masking, self-doubt, and care avoidance (Figure 2). Cluster B: Misrecognition of complexity as noncompliance: Cultural and epistemic mechanisms of exclusion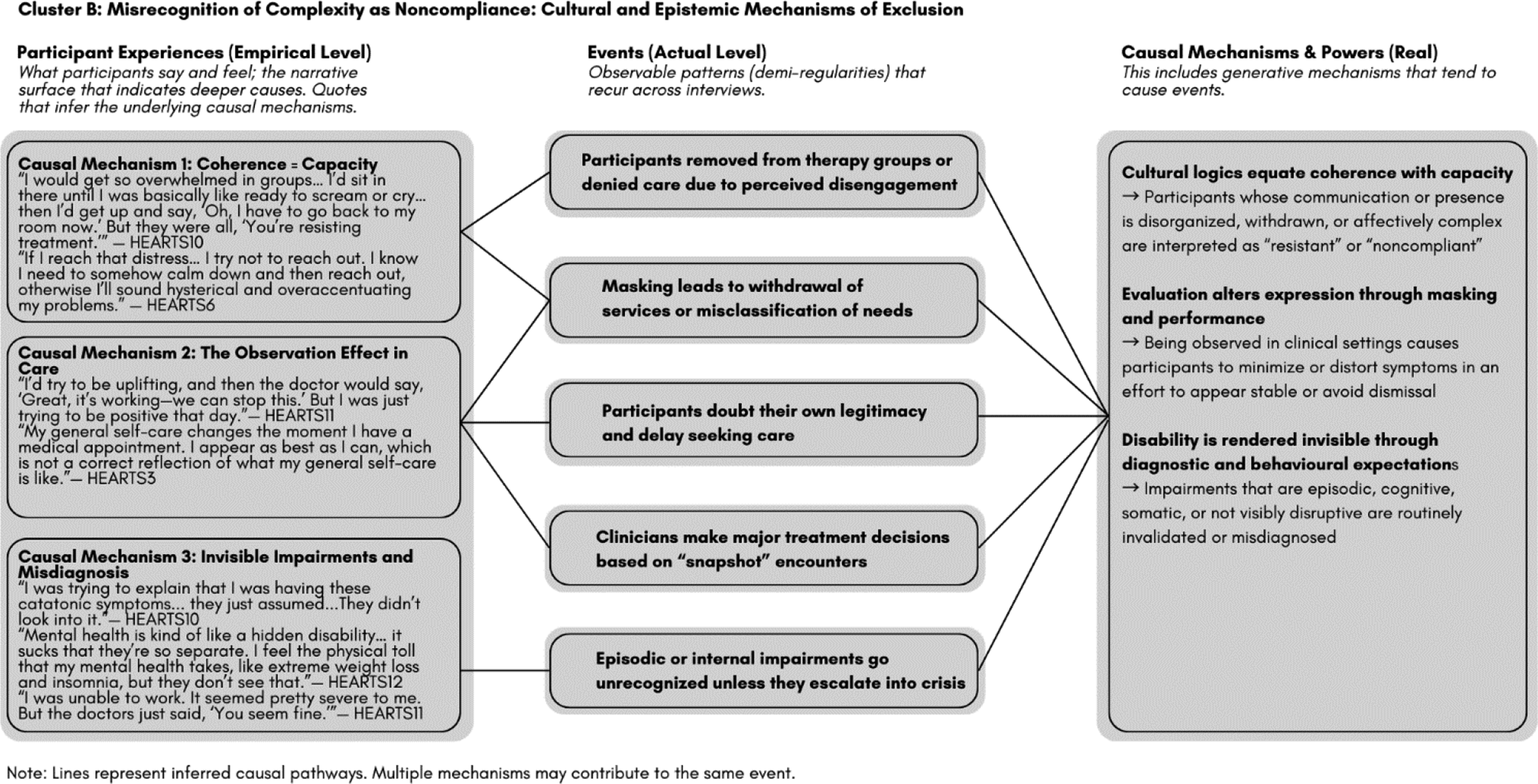
Cluster C: Trust Fractures and Epistemic Chaos: Causal Mechanisms Undermining Relational Continuity
Therapeutic relationships were destabilized by inconsistent care, contradictory messaging, and provider disbelief. Participants adapted by withholding disclosure or disengaging to protect themselves (Figure 3). Cluster C: Trust fractures and epistemic chaos: Causal mechanisms undermining relational continuity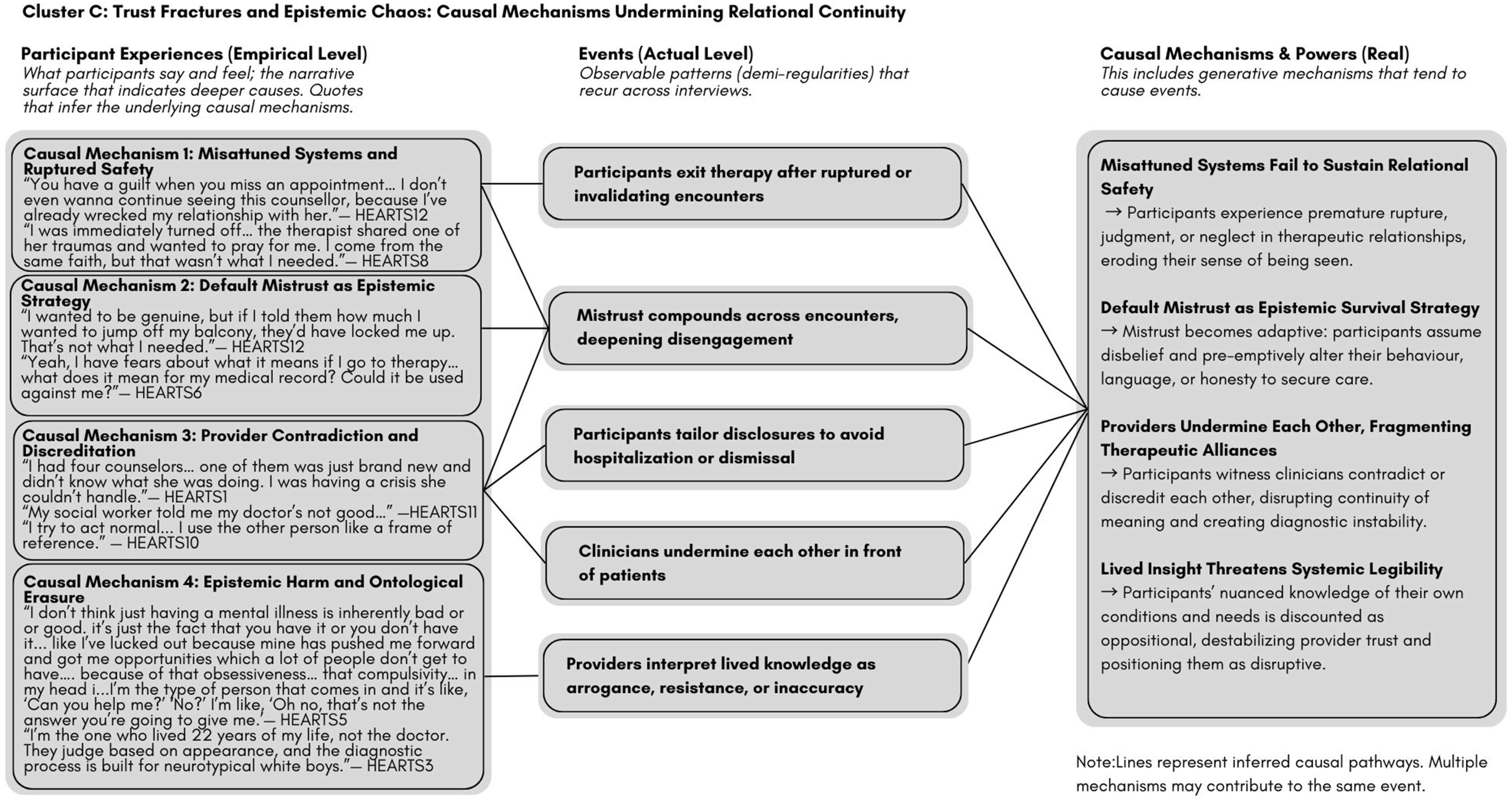
Cluster D: Fragments of Repair: Causal Mechanisms of Ontological Anchoring and Relational Safety
While rare, some participants encountered care that fostered ontological coherence. Micro-attunement, identity affirmation, and diagnostic validation enabled relational safety and renewed care engagement (Figure 4). Cluster D: Fragments of repair: Causal mechanisms of ontological anchoring and relational safety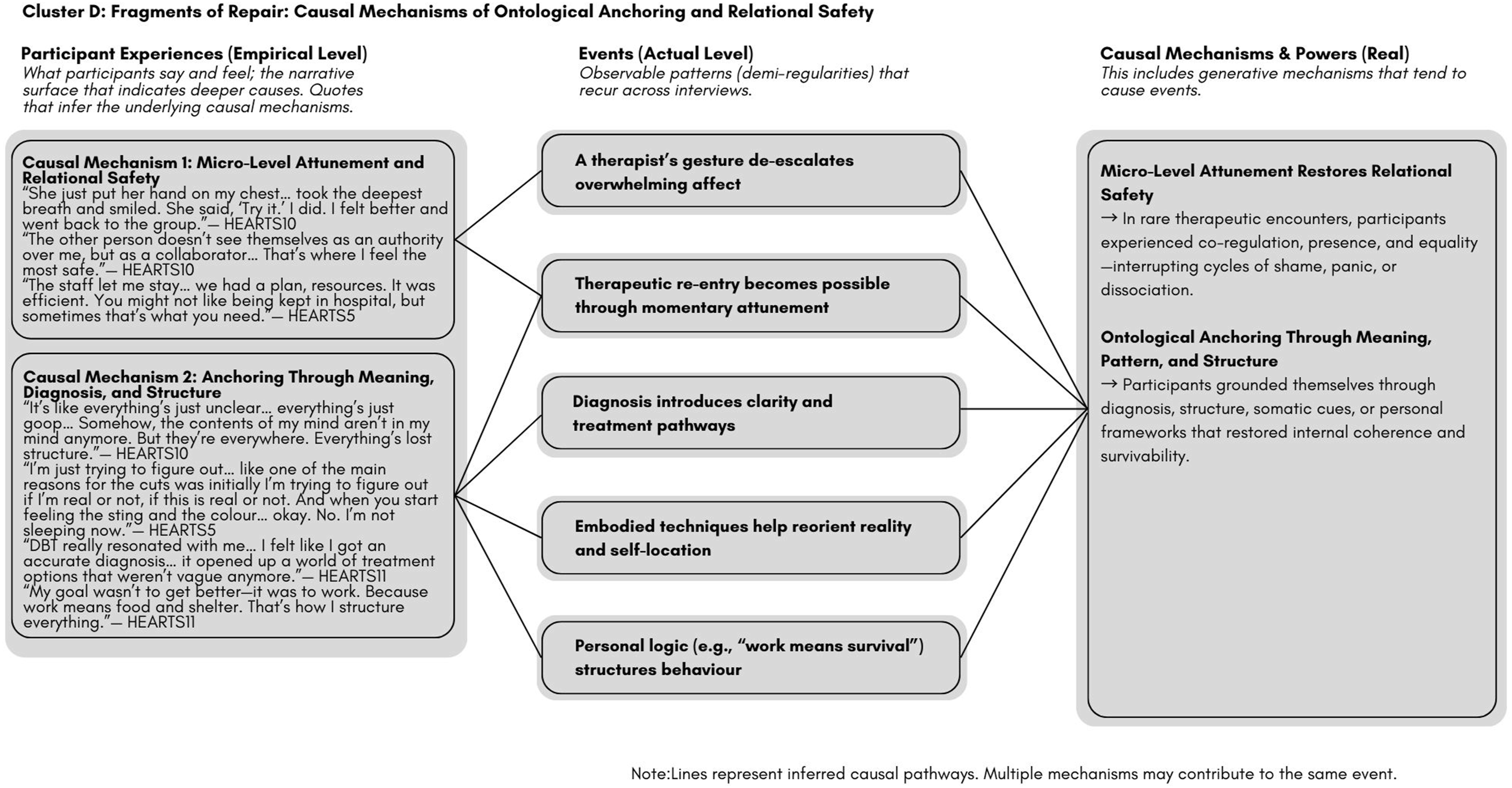
Cluster E: Broken Infrastructures, Forced Adaptations: Structural Mechanisms That Generate Inaccessibility
System design mismatches, bottlenecks, and institutional non-accountability forced participants to over-function, endure harm, or exit care (Figure 5). Cluster E: Broken infrastructures, forced adaptations: Structural mechanisms that generate inaccessibility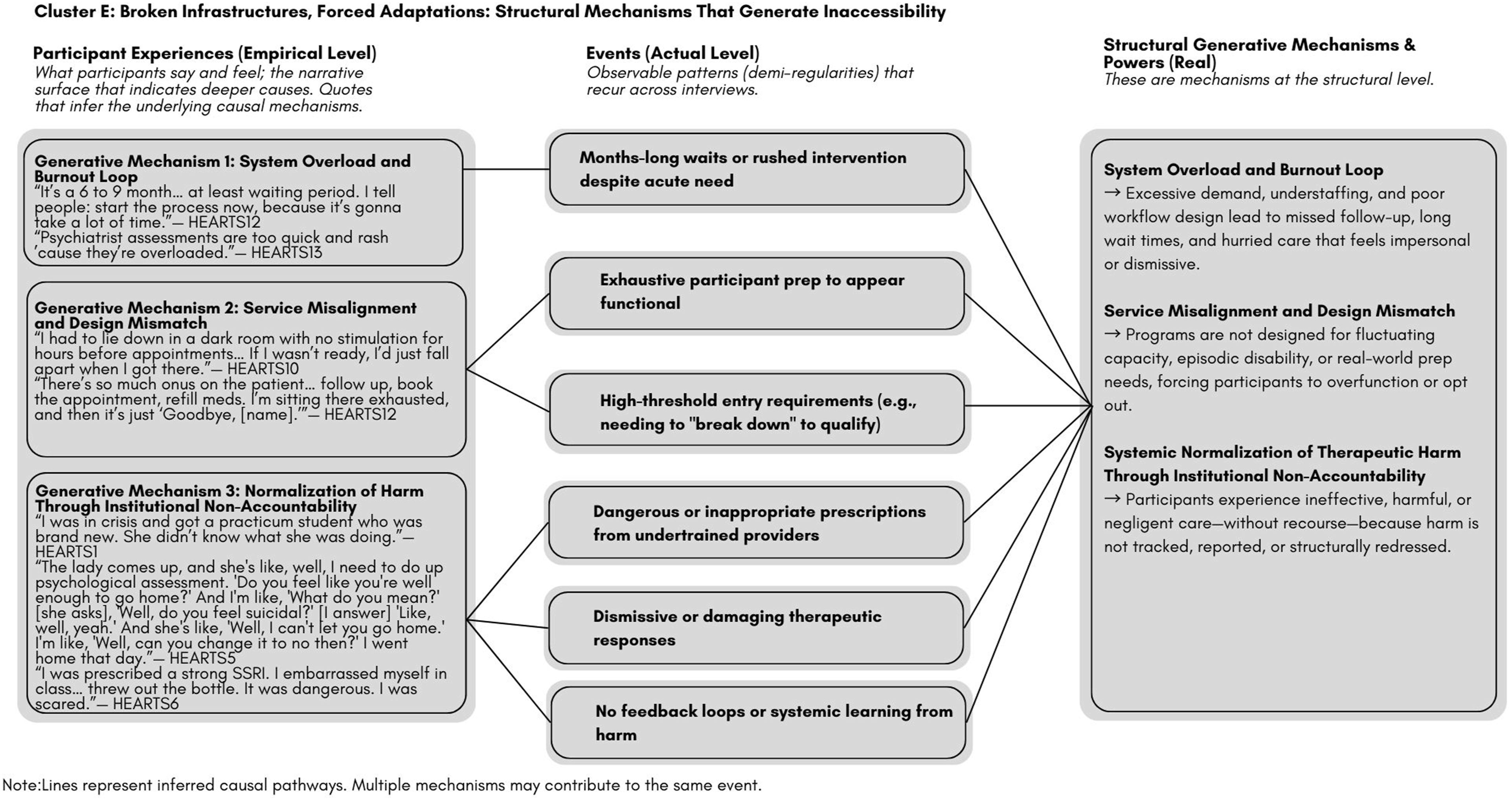
Figure 6 presents the Causality Pyramid of Mental Health Inaccessibility in Young Adults, a layered model that synthesizes the five causal clusters identified in this study. Organized across critical realism’s stratified ontology, the model explains how mental health–related disabilities interact with health systems to generate unmet healthcare needs, not as isolated barriers but as recurring patterns produced by deeper structures. At the real level, mental health–related disabilities function as a generative mechanism. It includes latent causal powers such as episodic impairment, disrupted narrative coherence, and fluctuating relational trust—tendencies that shape how young adults experience and navigate care. These powers interact with entrenched system-level mechanisms, such as classification demands, throughput pressures, and risk-averse protocols, which together produce actual-level events: misdiagnosis, system rupture, or withdrawal. These events occur whether or not they are immediately observable. At the empirical level, what becomes visible are the measurable signs, including missed appointments, disengagement, or diagnostic confusion that are too often misread or flattened without consideration of the underlying conditions. Collectively, the explanatory clusters demonstrate that unmet healthcare needs among young adults with mental health–related disabilities are not attributable solely to impairment severity. Rather, they emerge from the layered interaction of disabling structures, misrecognition and contradiction, and systemic responses to complexity. The causality pyramid of mental health inaccessibility in young adults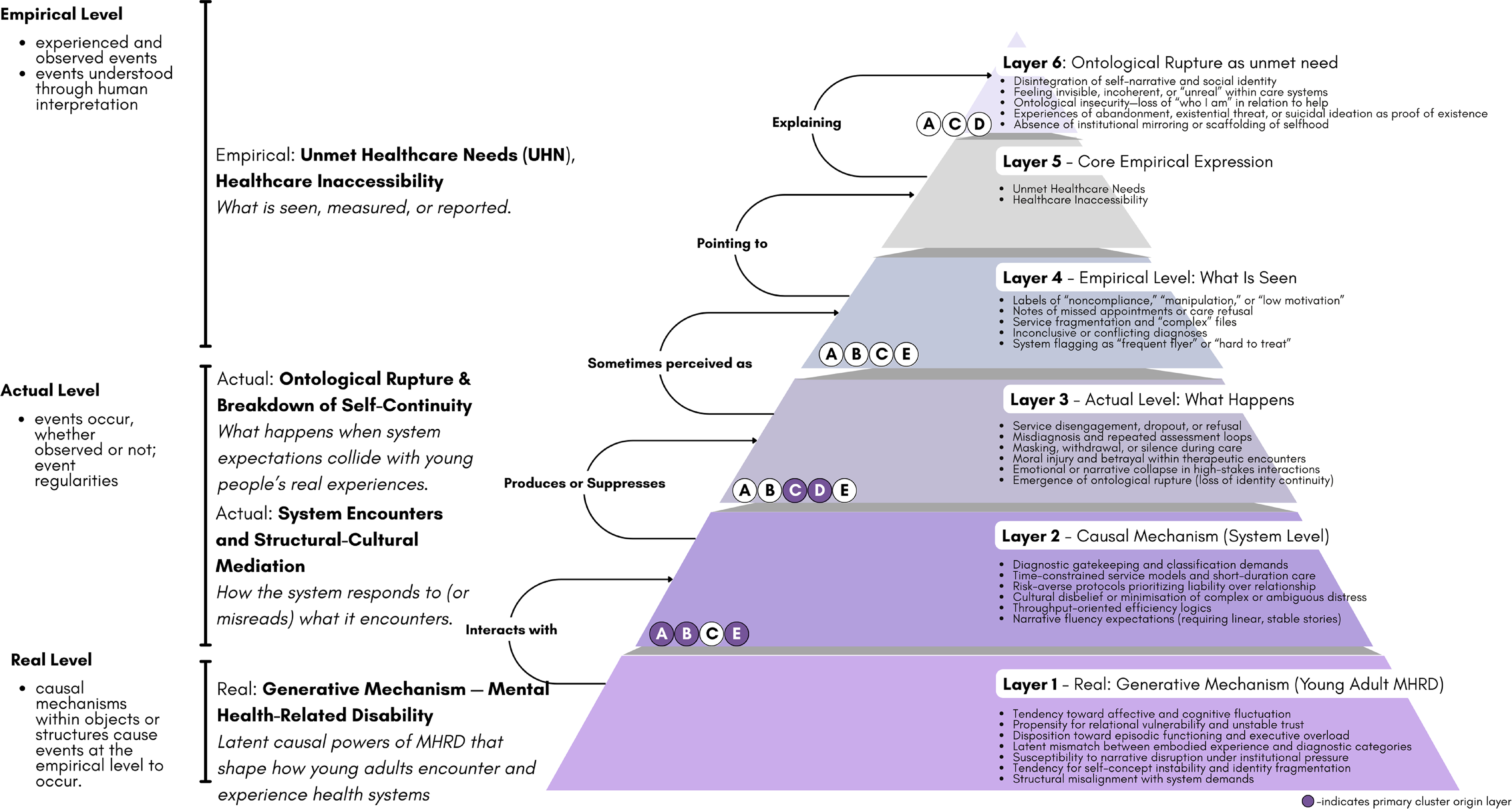
Discussion
This study aimed to explain how functional impairments contribute to healthcare inaccessibility and unmet healthcare needs among young adults with mental health–related disabilities. The findings affirmed that functional impairments significantly constrained access to care. Participants reported the disabling effects of episodic cognitive impairments, emotional dysregulation, narrative disorganization, and relational mistrust (Carlsson et al., 2015; De Vries et al., 2025; Luyckx et al., 2008; Marin & Shkreli, 2019; McLean & Pratt, 2006). These impairments limited their ability to seek help, navigate systemic demands, and sustain engagement with care. However, what emerged was not an absence of service use. Every participant had engaged extensively with the healthcare system, often over a span of many years, accessing a wide range of services across clinics, community programs, emergency departments, inpatient units, public and private providers, and multiple hospitals across multiple provinces. The paradox was not lack of entry but the persistence of unmet healthcare needs despite it.
This apparent contradiction invites a shift in how access is conceptualized. Entry into care systems should not be mistaken for accessibility. Participants accessed services not because they were easy to reach but because they had to. Access was not facilitated; it was endured. These young adults were not outside the system; they were inside it, but at great personal and existential cost (Corzine & Roy, 2024; De Vries et al., 2025; Dunn, 2019; Hultman et al., 2023). In the face of ontological survival, they surmounted structural barriers with extraordinary effort, suppressing distress and adapting themselves to fit institutional templates. Like a reflexive response in crisis, they did what was required to survive; but survival is not the same as safety. Their presence in the system does not mean the system is functioning.
Healthcare utilization, in this context, should be understood as endurance. What participants endured was not merely logistical inconvenience but systemic misattunement (Galanis et al., 2022; Piepzna-Samarasinha, 2018; Rao, 2024; Sins Invalid, 2019; Spade, 2020). Young adults with mental health–related disabilities encountered demands for linear narratives, emotional regulation, and diagnostic clarity—demands that directly contradicted the nature of their impairments. At every turn, they faced contradictory messages: disclose your story, but not too much; be sick enough to qualify, but not so sick you cannot complete intake processes; perform insight and self-advocacy, but do not speak with too much authority. These logics forced participants to contort their identities into serviceable shapes: camouflaging, masking, withholding, and fragmenting themselves just to remain eligible for care (Glyde, 2014; Hendry et al., 2022; Lorenz & Hull, 2024; Wang et al., 2024).
This recursive tension produced what we conceptualize as ontological rupture: a tearing in the continuity of self, a destabilization of identity not solely due to illness but due to systems that demand legibility without offering recognition (Berzonsky & Luyckx, 2008; Carlsson et al., 2015; Jones et al., 2024; Lynch et al., 2025; McLean & Pratt, 2006). Young adulthood is a developmental period defined by self-construction through relationships, reflection, and experimentation (Branje et al., 2021; Luyckx et al., 2008; Marcia, 1966). For participants in this study, mental health–related disabilities disrupted this process internally, while healthcare systems disrupted it externally. The result was not only delayed treatment or disengagement. It was a fundamental disruption in the sense of mattering, of being known, and of being worthy of care.
Throughout this study, mental health–related disabilities were described as an invisible disability (Dunn, 2019; Valeras, 2010). However, it became clear that it is not only the impairment that is unseen—it is the person (Borderon et al., 2021). The diagnostic category may be contested, but the deeper injury is ontological invisibility: young adults rendered illegible by their symptoms, dismissed by their providers, and denied the ability to inhabit their truth. What was described in the interviews was not simply access difficulty. It was existential erasure (Bauer et al., 2009; Namaste, 2000).
As Dunn (2019) articulates in the insider–outsider paradox, individuals with contested disabilities must often accept flattening or stigmatizing labels to receive support. In doing so, they gain access but lose something else: autonomy, dignity, and ontological legitimacy. Participants in this study reported how this paradox fractured their sense of personhood. Diagnosis became both a gateway and a wound. It offered validation but also reduction. Being believed became both a need and a risk. Navigating care required a continuous negotiation of self-erasure and self-advocacy.
Amid these patterns of rupture, we also observed moments of ontological anchoring: instances where participants encountered attuned providers, relational safety, or meaning-making structures that allowed them to remain intact (De Vries et al., 2025; Lee, 2022; Milner et al., 2019; Piepzna-Samarasinha, 2018; Watkins et al., 2019). These moments were not curative, but they were stabilizing. A therapist who listened without judgment, a diagnosis that named without confining, or a clinical encounter that held their reality rather than questioning it, these were moments in which participants felt seen. “If they can stand me,” one participant reflected, “maybe I can stand myself.” These inflection points disrupted the cycle of rupture and allowed for re-engagement, not just with care but with the self.
This study reframes access as more than a logistical or procedural issue. It is an ontological one. Care is not the same as being cared for. Access is not the same as attunement (Lundvall et al., 2022). And recognition is more than diagnosis. Young adults with mental health–related disabilities are not only trying to enter the system; they are trying to form a self. If the cost of care is the distortion or denial of that self, then access, however formally achieved, remains fundamentally unmet.
This analysis responds to broader calls for systems transformation by identifying the layered causal mechanisms that produce exclusion even in the presence of service use. In critical realist terms, the findings demonstrate how functional impairments and healthcare structures interact to generate, not merely reflect, healthcare inaccessibility and unmet healthcare needs. The harm produced is not incidental. It is structured. Unless care systems are reoriented to recognize, hold, and scaffold the existential realities of young adulthood with mental health–related disabilities, the crisis of unmet healthcare need will persist—not only as a clinical failure but as a crisis of being.
Strengths and Limitations
This study represents one of the earliest applications of critical realist thematic analysis to young adult mental health research. Grounded in critical realist metatheory, the analysis identified generative mechanisms contributing to healthcare inaccessibility through abductive and retroductive reasoning. Critical realist thematic analysis enabled the development of layered causal explanations, increasing both the explanatory power and theoretical contribution of the findings. The leadership of young adult co-researchers fundamentally reoriented the epistemic structure of the study. Rather than interpreting young people’s experiences through an adult-centric or institutionally distanced lens, their involvement challenged adultist assumptions often embedded in youth and young adult research and provided access to forms of knowledge typically inaccessible to external investigators (Alderson & Morrow, 2020). Their contributions extended beyond testimonial inclusion, offering epistemic authority that strengthened causal interpretation.
The study was also structured around radical hospitality, an approach that prioritizes relational and ontological safety over traditional accessibility frameworks, ensuring that participation was shaped by participants’ capacities, rhythms, and needs. Recruitment through a mental health registry aligned with the study’s values of reciprocity and mutuality, as participants had previously expressed interest in contributing to research. As a study limitation, this design choice may have preferentially included participants with greater system engagement, potentially underrepresenting individuals fully disconnected from care.
Implications for Practice and Policy
The Rupture–Repair Roundabout (Figure 7) is presented as a causal and practice-facing model for understanding how health systems generate either recursive disengagement or the conditions for ontological repair among young adults with mental health–related disabilities. Synthesizing explanatory findings across the five clusters, the model clarifies not only what happens when care is inaccessible but also why it happens and where system logics might be disrupted or transformed. The Rupture–Repair Roundabout extends existing models of engagement in health systems by situating service use within a layered ontology of access. Rupture–Repair Roundabout for young adults with mental health–related disabilities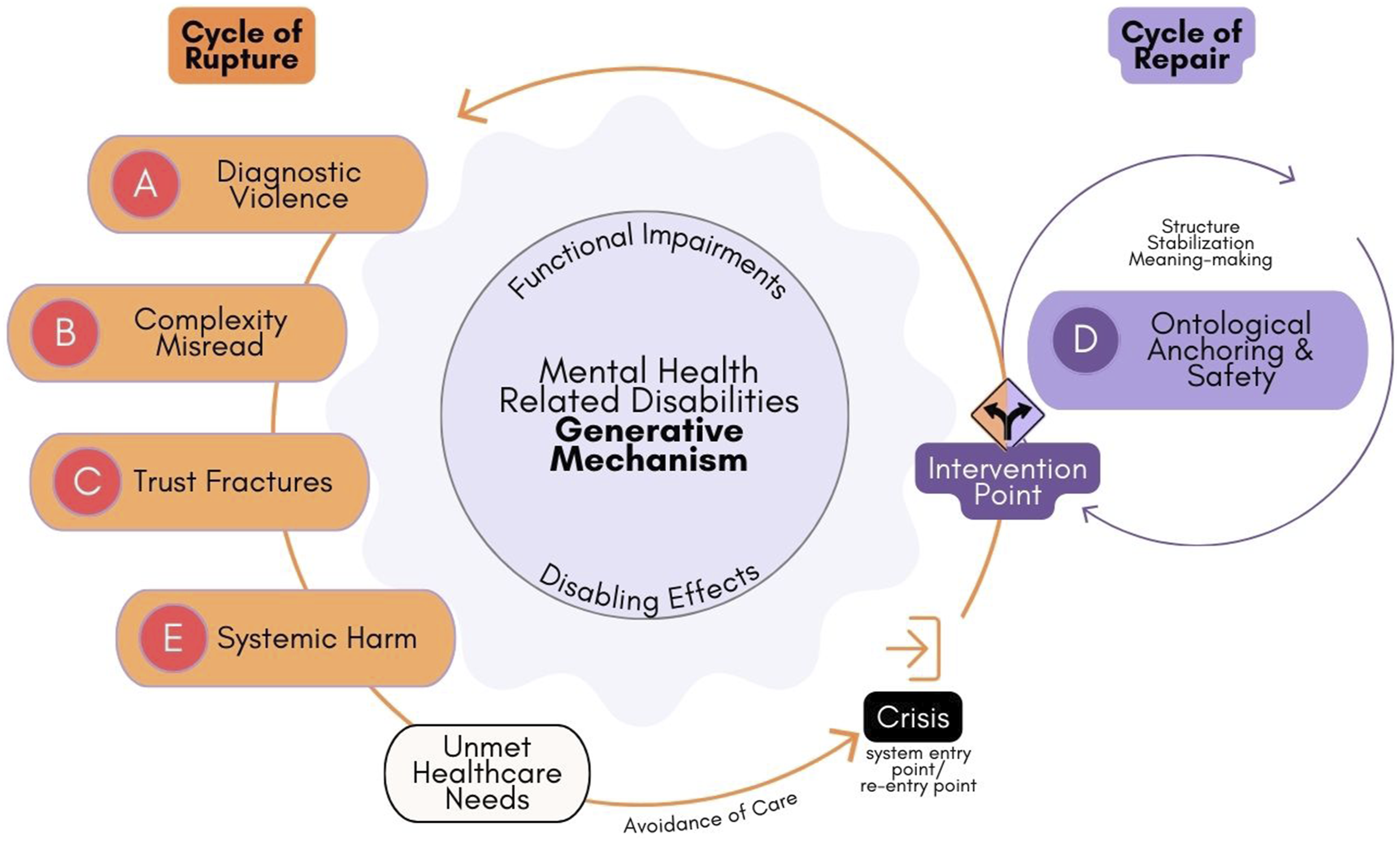
Whereas traditional frameworks emphasize motivation, compliance, or readiness for treatment, this model identifies engagement as contingent on the alignment of three interdependent conditions: individual capacity, relational safety, and structural design. It therefore explains disengagement not as personal withdrawal but as a systemic outcome produced when these layers fall out of sync. By illustrating how ontological rupture and repair unfold across these levels, the model provides a framework for practitioners and policy-makers to diagnose where and how care systems are generating harm and to intervene accordingly.
Cycle of Rupture
Rupture is triggered when functional impairments intersect with institutional demands for narrative fluency, diagnostic legibility, or behavioral compliance. Participants described being misrecognized, misdiagnosed, or disbelieved, resulting in masking, narrative collapse, relational mistrust, and withdrawal. These experiences are not simply service gaps. They represent ontological rupture, including a breakdown in identity continuity, meaning-making, and self-recognition. Individuals with contested or invisible disabilities often face a paradox: to gain access, they must accept reductive diagnostic categories that reinforce their outsider status. Diagnosis emerged as a double-edged mechanism. Although it was often misapplied or stigmatizing, it occasionally provided ontological relief by stabilizing experience, legitimizing suffering, and justifying help-seeking.
Cycle of Repair
Repair was initiated through moments of attunement, continuity, and relational recognition (Lundvall et al., 2022). These inflection points occurred through a provider who believed them, a diagnosis that named without reducing, or a structure that accommodated incoherence. These encounters enabled participants to reconstitute their sense of self and re-engage with care. Such anchors supported what we conceptualize as ontological safety, which reflects the capacity to be recognized, to matter, and to make meaning within care systems.
Although healthcare should not replace the societal functions that historically scaffolded young adults’ identity development, it must now be recognized that healthcare systems occupy a structural position. Systems can either exacerbate ontological rupture or contribute to ontological repair. Young adults continue to act as meaning-makers in motion (Berzonsky & Luyckx, 2008; Luyckx et al., 2008; Marcia, 1966; Marin & Shkreli, 2019; Negru-Subtirica et al., 2016). When healthcare encounters destabilize rather than scaffold being, the consequences are profound and extend beyond the clinical domain into the existential.
Our findings underscore the need to shift from systems that only ask “What is wrong with you?” or “What happened to you?” toward systems that ask “What matters to you?” Practice must move toward identity-attuned rather than identity-assumed care. Implications for practice include designing care that scaffolds the formation of selfhood through attunement, relational trust, and supported meaning-making, particularly for young adults with mental health–related disabilities. Policy responses must recognize that access is not merely a threshold to cross. Instead, access is a relational and ontological space that can either fragment or stabilize the self. The Rupture–Repair Roundabout offers a structured pathway for reconfiguring systems around recognition, continuity of self, and survivability.
Conclusion
Young adulthood is the crucible of becoming, but for those living with mental health–related disabilities, it unfolds in systems that obscure rather than illuminate the self. This study shows that access alone is insufficient when recognition is absent. What is eroded is not merely opportunity but ontology. To meet young adults where they are is not simply to treat symptoms but to hold their becoming as real, fragile, and worthy. To fail at this is not only to lose engagement but to lose people. Addressing healthcare inaccessibility must begin with restoring visibility to those made unseen.
Supplemental Material
Supplemental Material - Becoming Invisible: How Mental Health Systems Erode Selfhood in Young Adults With Mental Health–Related Disabilities
Supplemental Material for Becoming Invisible: How Mental Health Systems Erode Selfhood in Young Adults With Mental Health–Related Disabilities by Sandy Rao, Gina Dimitropoulos, Katrina Milaney, Dean T. Eurich, and Scott B. Patten in Qualitative Health Research
Footnotes
Acknowledgments
We acknowledge the HEARTS study co-researchers. We also want to acknowledge the participants in this study. This is for you. You were not asked to show up when it was easy. You were asked when you were already carrying too much. And still, you came. You answered questions that had no perfect words. You told truths that had long been ignored. You gave voice to experiences that others had dismissed, softened, or made into something else. You trusted that this time might be different. You spoke when speaking was effort. You returned when returning cost something. You named what hurts, what lingers, what repeats. You shared what systems have erased. You did not owe any of it. Yet, you gave it freely, with the hope that someone else might be met with more care than you received. This work is shaped by your insight, by the sharpness of your analysis, and by the clarity of your refusal to be made small. You were not just participants. You were co-theorists, critics, and witnesses. You showed what it means to keep going, not because the system made space for you but because you believed that someone else might need that space more. This study would not exist without what you offered. It carries your truths and your questions. It is accountable to your courage and to the generosity you extended in the face of exhaustion, invisibility, and risk. You did not have to say yes. But you did. And in doing so, you made something possible. Thank you.
Ethical Considerations
This study received ethics approval from the Conjoint Health Research Ethics Board at the University of Calgary (REB22-1063) and operational approval from Alberta Health Services (AHS). All recruitment and data handling procedures complied with the Tri-Council Policy Statement on Ethical Conduct for Research Involving Humans (TCPS2, 2022), Alberta’s Health Information Act, and institutional data use agreements. A Data Disclosure Agreement and Health System Access Approval were obtained to ensure secure and compliant access to the Access Research Registry, from which eligible participants were identified. Participants were recruited through a registry where individuals had previously provided informed consent to be contacted for research. This ensured that participation was initiated with reciprocity and mutual interest. Beyond procedural compliance, this study developed an integrated ethics model that emphasized ethics-in-practice, relational accountability, and structural justice. In alignment with this model, accessible materials were provided to support understanding, including plain-language summaries, videos, and zines co-created with young adult co-researchers. Use of these materials was optional, and participation in screening or interviews was entirely voluntary. The lead researcher had no affiliation with participants’ care teams, and individuals could choose not to respond without consequence.
Consent to Participate
Participants were provided with multiple opportunities to assess whether the research aligned with their values, needs, and capacity. Pre-interview meetings were offered to clarify expectations and review consent. All consent procedures were ongoing and dialogic. Privacy and data security protocols adhered to the standards of both AHS and the University of Calgary, including data de-identification, secure storage, encrypted communication, and the separation of identifiers from research data. This ethics approach was designed not only to minimize risk but to foster safety, trust, and meaning. All participants were given multiple opportunities to engage with the consent process. They received accessible study materials and were invited to review the consent form with either the lead researcher or a young adult co-researcher. Participants were encouraged to ask questions, assess alignment, and discuss any concerns prior to confirming their participation. Written informed consent was obtained from all participants prior to data collection.
Author Contributions
SR led the project, contributing to conceptualization, methodology, formal analysis, data curation, investigation, visualization, writing—original draft, and writing—review and editing. GD provided extensive supervision and contributed to conceptualization, methodology, validation, formal analysis, resources, and writing—review and editing, offering significant insights and feedback throughout the project. SBP provided extensive supervision and contributed to conceptualization, methodology, validation, formal analysis, resources, and writing—review and editing, offering significant insights and feedback throughout the project. DTE and KM contributed to conceptualization, methodology, validation, and writing—review and editing, with a particular focus on the development of initial ideas, models, and theoretical frameworks.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.