
Abstract
The COVID-19 pandemic has affected countries at different times and to varying degrees, placing significant pressure on healthcare systems and challenging the delivery of end-of-life care. Palliative care professionals faced unprecedented circumstances, requiring rapid adaptation to maintain the quality of care for vulnerable populations. Thus, the aim of this study was to explore the experiences, challenges, and perspectives of healthcare professionals providing palliative care in Brazil and England during the COVID-19 pandemic. This qualitative multicenter study was conducted with 36 healthcare professionals (18 occupational therapists and 18 nurses) from various palliative care services in Brazil and England. Data were collected remotely through semi-structured interviews and analysed using reflexive thematic analysis. Findings revealed that professionals experienced intense emotional distress and ethical challenges, particularly related to providing care in isolation and managing silent mourning processes. The study also highlighted the rapid adaptation of palliative care services in response to pandemic constraints, such as the implementation of telehealth and restructured workflows. Despite challenges, professionals demonstrated creativity and resilience, with innovations emerging from crisis situations to ensure continuity of care. The COVID-19 pandemic profoundly disrupted palliative care delivery, prompting teams to develop new strategies to support patients, families, and colleagues. The experience fostered reflection on care practices and emphasised the critical role of palliative care in public health emergencies. These findings provide valuable insights for future preparedness and underline the need for stronger integration of palliative care in healthcare systems during pandemics.
Keywords
Highlights
● Palliative care professionals experienced emotional strain, ethical dilemmas, and grief while providing care under pandemic restrictions.
● Services rapidly adapted through telemedicine and flexible workflows, ensuring continuity and compassion despite crisis conditions.
● The findings highlight the urgent need to strengthen and integrate palliative care within health systems to preserve dignity and support both patients and professionals during future emergencies.
Introduction
The COVID-19 pandemic was first reported in Southeast China in November 2019 and was officially declared a global pandemic on March 11, 2020. The virus spread rapidly across the world, resulting in unprecedented increases in mortality worldwide.1,2 The pandemic affected countries at different times and to varying degrees. In March 2020, both Brazil and the United Kingdom (UK) declared a state of public calamity and implemented lockdowns as part of a series of measures aimed at containing the spread of the SARS-CoV-2 virus.3,4 Regardless of the evident disparities in the healthcare systems of these countries, the National Health Service (NHS) in the UK and the Unified Health System (SUS) in Brazil both experienced significant mortality rates and considerable pressure on their healthcare services during the pandemic. As of April 2024, the UK had recorded 232 112 deaths attributed to the virus, 5 while Brazil had reported 711 380. 6 These data illustrate the severe impact of the pandemic on both countries, particularly on vulnerable populations.
Background
Due to the rapid progression of severe symptoms associated with a COVID-19 diagnosis, end-of-life care has become routine for most staff working in hospitals and other healthcare facilities during this period. 7 Palliative care (PC) is a healthcare specialised approach that focuses on enhancing the quality of life of both clients and their families while they are dealing with life-limiting illnesses. It includes a holistic strategy that attends to the emotional, social, and spiritual facets of care in addition to the physical symptoms. 8 The global pandemic imposed considerable challenges on healthcare professionals worldwide, particularly those specialising in PC. As the virus spread rapidly, there was a consequential increase in demand for end-of-life care, which required healthcare workers to adapt their practices and implement new approaches to care.9,10
The nature of the impacts on PC services in the UK and Brazil differs significantly, primarily due to the distinct healthcare systems, available resources, and social contexts of each country. According to the quality of end-of-life care across 81 countries, the UK ranked first, while Brazil ranked 79th, highlighting the stark disparities in the quality of care provided in these settings. 11 The report suggests that the precariousness of end-of-life care in Brazil is primarily due to financial restrictions, a lack of recognition of the importance of PC, insufficient national strategies for implementing PC, and limited integration of PC within the country’s healthcare system. In contrast, the UK benefits from a more integrated and established PC system. Furthermore, the study also highlights the need for improvements that could indirectly enhance the delivery of end-of-life care, such as public education programmes, the promotion of compassionate communities, and investment in research. 11 These recommendations resonate with the renewed attention to death and the dying process triggered by the COVID-19 pandemic, underscoring the importance of taking action on these issues. 11
Despite their differences, both countries faced challenges during the pandemic, requiring adaptation to new care models and virus transmission mitigation strategies to provide adequate PC across various healthcare settings. This challenge emphasised the need for integrated PC models, properly trained professionals, and adequate resources to maintain care quality, particularly in crisis situations.1,12 -14
As the pandemic progressed, PC professionals faced unprecedented and complex challenges: higher patient discharges, reduced admissions due to overcrowding and infection risk, and drastic changes in communication and human contact. 15 These difficulties were exacerbated by the demands of social isolation and infection control measures, which disrupted traditional methods of care delivery but underscored the importance of PC practices. 16
The impact of the pandemic revealed significant vulnerabilities within healthcare systems, especially regarding the balance between demand and supply for intensive care resources. 17 As intensive care units became overwhelmed, PC services became more crucial for addressing both the clinical and emotional needs of patients and families. 12 Multidisciplinary PC teams played a crucial role during this time, managing symptoms, providing psychological support, and guiding families through the process of grief and loss.13,18
However, the sudden onset of the pandemic, combined with the constraints on healthcare delivery, forced PC teams to adapt rapidly to new workflows, triage processes, and digital technologies to provide remote support.4,7 While these adaptations were necessary, they placed significant strain on healthcare professionals, leading to an increase in emotional and psychological distress due to high workloads and the nature of the care required. 9
Despite the evident importance of PC during pandemics,1,12,18 -20 few studies have explored the impacts of COVID-19 on PC services, particularly on the professionals delivering this care.4,17,18,21,22 The emotional and psychological challenges faced by hospice and PC teams during the pandemic underscored the need for rapid adaptations in care delivery. These challenges were not only evident in the physical demands of the profession but also in the psychological aspect. 4 The psychological distress experienced by the palliative and hospice workforce was significant. 22 In response to these challenges, PC professionals demonstrated resilience, adjusting their practices through trial-and-error and adopting effective strategies to cope with the evolving crisis. 18 While examples of effective care delivery, collaboration, and communication emerged, if the core principles of PC are not restored, the workforce risks further fragmentation, which could undermine the quality of care provided. 21 These studies highlighted the importance of supporting PC professionals both emotionally and practically during crises, ensuring that the workforce remains resilient and able to continue delivering high-quality care under circumstances.
This study contributes to the understanding of how PC services were impacted by the COVID-19 pandemic, particularly in Brazil and the UK. While the pandemic was a global event, the response to this crisis, particularly in PC, varied depending on the healthcare infrastructure, resources, and socio–cultural-political context of each country. By exploring the experiences of PC professionals in both Brazil and the UK, this research provides an understanding of how these professionals adapted their practices to the challenges posed by the pandemic. Thus the research question was based on how PC professionals perceived how the pandemic affected them and their daily work during the first and second wave of the Covid-19 outbreak in Brazil and in England?
Purpose
To explore and understand the experiences of healthcare professionals working in PC with vulnerable patients during the COVID-19 pandemic in Brazil and England. By understanding how each country adapted to the crisis, this study highlights the lessons learned from their responses to the pandemic and identifies best practices that can be applied in future health emergencies.
Methods
Design
This study is part of a larger doctoral research project focusing on the perceptions of healthcare professionals regarding rehabilitation in PC. The research aimed to understand how the COVID-19 pandemic impacted PC services, which involved the collection of data from healthcare professionals working in PC services in both Brazil and the United Kingdom. The pandemic emerged during the course of the doctoral project, and this opportunity was seized to gather insights into the experiences of professionals working in PC settings during the crisis. This multicentre qualitative, cross-sectional study aimed to focus on meanings, intentions, beliefs, and attitudes in the interpretation of lived experiences. 23 Qualitative techniques use words rather than numbers, acknowledging dynamic realities and offering perspectives through the participants’ lens. 23 The study adopted a constructionist approach, where in meaning was co-constructed by PC professionals as they described their experiences amid COVID-19, while also considering the researchers’ interpretative lens. 24 Open-ended individual interviews were used to explore participants’ perspectives. 25 Reflexive thematic analysis supported the identification of key themes grounded in the data.26 -28 An inductive approach was chosen to better focus on the experience and perspective of the healthcare professionals.
Participants, Sampling, Setting, and Recruitment
Participants working in PC services were recruited from various settings, including hospices, hospitals, community-based PC centres, PC units, and nursing care homes in different areas of Brazil (Distrito Federal and the states of São Paulo, Alagoas, Pará, Minas Gerais, Paraná, Bahia) and England (London and surrounding boroughs).
In Brazil, potential participants were identified through the snowball sampling technique, a non-probability sampling method commonly used in qualitative research. This approach proved particularly useful in reaching PC professionals who met the study’s inclusion criteria but were difficult to access via other recruitment strategies. The research team initially contacted potential participants via email or telephone, utilising their professional networks. Once the first participants were identified, they were asked to recommend other colleagues who met the inclusion criteria (ie, PC professionals with at least 1 year of experience). This process continued with each new participant helping to expand the sample by referring others, creating a snowball effect that gradually built a network of eligible professionals. This method allowed for a diverse range of participants from various regions of Brazil. Although some participants in Brazil were known to the researchers through their professional networks, the recruitment process was strictly based on their eligibility criteria.
In England, recruitment was facilitated by gatekeepers and research leads within PC teams. These individuals shared the study’s details during team meetings and extended invitations to eligible professionals. Participants in the UK were not known to the researchers prior to the study, ensuring impartial recruitment.
Verbal consent was obtained from all participants prior to the interviews. The process was documented by audio-recording each participant’s explicit verbal agreement at the beginning of the interview, which was securely stored along with the research data. This approach ensured both ethical compliance and traceability of participants’ consent. 29
Eligibility criteria included: (a) being a qualified occupational therapist or nurse, (b) working as clinicians or managers in PC services, and (c) having at least 1 year of professional experience in providing PC. Additionally, participants had to be able to understand and communicate in English or Portuguese. Three eligible participants were excluded due to unavailability after 3 scheduling attempts.
A purposive sample of 36 professionals from Brazil and England was selected, considering both countries were heavily impacted by the pandemic. The sample size for this study adhered to the “information power” concept outlined by Malterud et al, as it is more suitable than “data saturation” in the context of reflexive thematic analysis. 30
Data Collection
Interviews offered insights into PC professionals’ perceptions during the first and second waves of the pandemic. Interviews were conducted remotely via Zoom®, Skype®, Google Meet®, or Microsoft Teams®. The audio and video recordings were made using each platform’s own recording programme and transcribed verbatim by the first author, who had undergone extensive training in research methods. The interviews were conducted between June 2020 and January 2022, using an open-ended interview guide. Interviews were characterised by low directivity, allowing participants to share their views freely. The interview guide was developed by the research team based on the basis of the literature, 23 prior to obtaining Research Ethics Board approval for the study. It included open-ended questions in which participants were asked to discuss their experiences in caring for vulnerable patients during Covid-19 outbreak in PC services (see Supplemental Appendix 1). The interviews were conducted in Portuguese for the Brazilian participants and in English for the UK participants, with each interview lasting between 15 and 90 min. Repeat interviews were not conducted; all interviews were 1-time sessions and participants did not provide feedback on the findings after data analysis was completed.
Data Analysis
Sociodemographic data were analysed using descriptive statistics, such as mean and percentile, using RStudio Team software. 31 Qualitative data were systematically coded using MAXQDA Analytics Pro Student 2020®. 32 To ensure methodological rigour, we followed a reflexive thematic analysis approach.26 -28 This approach is known for its flexibility in adapting to different research contexts while maintaining rigour and transparency. Initially, the data were read multiple times by researchers to identify broad themes and become familiar with the material, ensuring a deep understanding of the content. Themes were then generated inductively, grounded in the data, and refined through systematic coding. The researchers involved in this study were experienced in qualitative research methods and PC research. They had undergone formal training in qualitative data collection and analysis, particularly in thematic analysis. Researcher triangulation was applied to base coding and analytical decisions on convergent validation, by discussing coding and analysing among the researchers.26 -28 Transcripts were read multiple times in order to get a feeling for the depth of the data and to collect and discuss ideas that came up while reading the data. To ensure the qualitative coding, 2 researchers independently reviewed and coded the interview transcripts. This process allowed for an initial understanding of the data and ensured that the coding was grounded in the participants’ actual responses. Any discrepancies or differences in interpretation were resolved through discussions and consensus-building with a third researcher, ensuring an objective and balanced approach. The process was collaborative and aimed at ensuring consistency and coherence in the interpretation of the data. Codes were clustered into categories, with a final thematic framework developed.26 -28 Inductive cycles refined themes and subthemes, comparing within and across transcripts. The original transcripts in English and Portuguese were analysed. Quotations were translated to preserve narrative meaning. Given syntactic and semantic differences, translations prioritised the original intent. We used an interpretative approach by analysing thematically to identify patterns and categories in the data.26 -28 Data analysis was as inductive as possible, and emergent themes rather than theoretical concepts, lead the analytical process. In terms of reflexivity, we made it a priority to engage in ongoing self-reflection throughout the research process. Reflexivity was an important aspect of the research process. The researchers engaged in ongoing self-reflection throughout the study, keeping reflective journals to monitor their thoughts, assumptions, and potential biases. 27 This allowed for greater awareness of how their perspectives may have influenced the analysis. The researchers involved were experienced in qualitative research methods and PC research, having received formal training in qualitative data collection and analysis, particularly in thematic analysis. Reflexive bracketing was applied to help acknowledge and manage assumptions, ensuring that the analysis remained as objective and transparent as possible. Trustworthiness and credibility were supported through adherence to COREQ criteria 33 (see Supplemental Appendix 2).
Ethical Issues
The study followed the Declaration of Helsinki and Good Clinical Practice. It was approved by the Research Ethics Committees of Brazil, granted by the University of São Paulo (number 21189919.0.0000.5393) and the UK, by Kingston University (number 1468) on 5 May 2020, along with site-specific approvals in both countries. Written or verbal informed consent was obtained from all participants via e-mail or videorecording during the interviews. Participation was voluntary, with no form of compensation received. For data management and anonymity purposes, all interviews were transcribed and data was anonymised using identity numbers, such as P1, P2.. and also included BR or UK to identify the country of the participants. The data collection only took place after the consent was given.
Results
The study involved 36 healthcare professionals: 18 occupational therapists and 18 nurses, half of whom worked in England (n = 18—London and its boroughs) and the other half in Brazil (n = 18). The Brazilian participants came from different regions of the country, with significant cultural differences: most professionals were from the state of São Paulo (n = 10), 2 from the state of Bahia, 1 from the state of Alagoas, 1 from the Federal District, 1 from the state of Minas Gerais, 1 from the state of Pará, 1 from the state of Paraná and 1 participant was residing in Utah, in the United States of America, at the time of the interview.
Overall, most professionals (n = 32) were women with a mean age of 41.5 years, and only 4 were men with a mean age of 26 years, who had been working with PC for more than 7 years. Most participants worked in hospices (mainly participants from England) and hospital settings (in Brazil) and had more than 4 years of work experience in their respective locations (Table 1).
Socio-Demographic Characteristics of Participants.

Others - Professor, Home Care Service, Hospital setting and Compassionate community | < - less than | > - more than | % - percentile.
The analyses resulted in 4 main themes found within the experiences and perceptions about the pandemic period. The themes that emerged were described as follows in Table 2.
Data Analysis: Examples of Codes, Categories and Themes.

Resonant Echoes: Navigating the Depths of Pandemic Suffering
In addition to the organisational and logistical challenges faced by healthcare services, the suffering experienced during the COVID-19 pandemic extended far beyond the physical dimension. The measures needed to control the virus’s spread, particularly the unprecedented rise in deaths, created an environment that exacerbated the emotional burden on both patients and healthcare professionals. Healthcare professionals were not only managing the distress of patients but also dealing with their own personal suffering, balancing work duties with the psychological impact of the situation.
The restrictions, including isolation and quarantine measures, along with the generalised fear of contracting COVID-19, increased the feelings of loneliness, sadness, and fear among both patients and staff. As one participant from the UK shared, “Emotionally, you’re feeling down. . .I think all healthcare professionals are struggling right now. . .And I think patients have been struggling with the feeling of isolation, not just because they can’t have the same kind of contact with their families and professionals, but I think they have struggled with the lack of contact with people because it doesn’t seem the same” (P3-UK). This highlights the emotional isolation that pervaded both the healthcare staff and the patients they cared for.
The psychological distress was reported by participants, where healthcare workers faced overwhelming workloads, solitary and dehumanised deaths, and grief during the pandemic. For instance, another UK participant shared, “I think a lot of people are terrified and very anxious. In the hospice, I felt that everyone seemed quite tense and anxious because they didn’t really know how bad it would get. There was a lot of news about people dying” (P9-UK). This anxiety was further compounded by patients who died alone, without the physical presence of loved ones, significantly affecting the quality of death. One participant from Brazil shared, “Many of our patients died in the hallway on a rigid stretcher. . .and that’s everything we don’t want. It’s sad to think. It’s to cry” (P14-BR).
Both the UK and Brazil experienced significant rises in mortality rates, with the virus rapidly spreading among vulnerable populations, particularly in hospitals and nursing homes. These outbreaks in care facilities led to a reduction in the patients’ functional status and a decline in their social participation, directly impacting the quality of their death and intensifying the suffering of patients, family members, and healthcare professionals. One UK participant stated, “This affected us in many different ways, and the main one was a large number of deaths this year. There were times when we supported 100% more people than usual. . .We also supported people who had very different types of deaths from those we are used to, very sudden, unexpected deaths. And we had unexpected challenges, such as the massive outbreaks in nursing homes (. . .). So, for us, a lot of what we do is to accompany people, to be beside people in their suffering.” (P5-UK). “Unfortunately, we had COVID in the hospice, and it was very sad because, because we lost a lot of people unnecessarily as a result of this, people died prematurely because they were vulnerable.” (P6-UK). This highlights the chaotic nature of care during this period, where professionals had to navigate an overwhelming number of patients experiencing unexpected deaths.
Participants also expressed frustration with the lack of preparation for such an event, as many felt that government guidance was unclear, and resources like PPE were scarce. One UK participant shared, “There was no preparation for the pandemic. Government guidance needed to be improved. It was so confusing, little known, lacking PPE, and a lot of death. People were affected emotionally and psychologically. . .and we started to have similar reflexes, with no time for employees to reflect, think about what is happening, and how they are coping at work and home” (P1-UK). This indicates the profound systemic challenges faced in both countries, despite their different healthcare contexts.
Clearly, the focus on combating the pandemic has disorganised the system and thus modified the care of other diseases in addition to COVID-19. Another crucial point is the existing suffering among all those involved, patient, family, health team and managers, witnessing an increase in the rate of premature death, with a reduction in the quality of death due to the restrictions imposed as a way of reducing contagion, which adds more sources of stress and suffering.
The Rapid Adaptation of Palliative Care Assistance During the COVID-19 Outbreak
The necessity for rapid and significant adaptations in healthcare services was highlighted by participants, particularly within hospices and specialist PC teams. These adaptations encompassed logistical restructuring, emotional challenges, and the increased use of PPE. One Brazilian participant explained, “Our life turned upside down in every way, both professionally and personally. . .It was a very intense moment. . .we had to readapt to this new life, we will never have the life we had” (P11-BR). This dramatic shift in how PC was delivered highlights the resilience and adaptability of healthcare professionals, who were forced to confront the emotional, physical, and logistical challenges head-on.
The economic strain was also a significant challenge. Many hospices in both countries depend on charity funding, and the pandemic exacerbated financial crises as fundraising events were cancelled. One UK participant noted, “It’s been a challenge. We’re very lucky to have hospices, but our hospice is 75% funded by charity basically, and we fund a lot of that through charity shops and operations stores, so they’re all closed because of the pandemic and also any functions like gala dinners and raffles and stuff got canceled. Then we had a significant funding crisis” (P7-UK). Furthermore, the crisis arose from the reduction in the number of patient admissions to the services as noted in the UK, “Our admission rate has dropped about 15%, and it seems more, actually. Because people don’t want to go into hospices, or hospitals in general, where they can’t have visitors and things like that” (P2-UK). Similarly, Brazilian participants highlighted the reduction in hospice admissions, noting that the strict visitor restrictions and fear of the virus led to fewer people seeking care in these settings. One Brazilian participant shared, “We reduced admissions because we had a rigorous restriction on visits to try to reduce the transmission of the disease, so we don’t have visits allowed, which is desperately sad” (P12-BR).
The pandemic also necessitated the integration of alternative methods to deliver PC, such as telemedicine and teleconsultation. One UK participant shared, “We’ve had the added pressure of managing COVID using PPE and being attentive to patients with severe respiratory distress. This has been quite emotional; you really have to speak with your eyes. We just got online with everything. So phone calls, video calls, Zoom. So all of our circuit fitness classes went to Zoom. Dyspnea management moved to Zoom, and everything we’ve been doing continues but in a different medium. I usually do home assessments to assess your environment to see how we could adapt it to accommodate someone” (P8-UK). This shift to digital technologies became crucial for maintaining communication and providing care remotely, especially as in-person consultations were limited.
Thus, the rapid adaptations in PC services have demonstrated resilience and rapid adaptation of ways of providing assistance and care. However, pressure on healthcare professionals, the limitations of telemedicine to meet patients’ complex needs and financial challenges highlight areas where future crisis planning and support systems could be strengthened. The insights gained from this experience have the potential to inform the development of future models of PC delivery. This could ensure that services remain flexible and efficient in the face of unforeseen global health challenges, such as a pandemic.
Silent Mourning: The Burden of Isolated Death in the Pandemic
The emotional and psychological burden of the pandemic was particularly evident in how death and grief were handled. The inability of family members to be present during the final moments of a loved one’s life led to a more isolated death, which in turn complicated the grieving process. One UK participant shared, “The worst part is that most of the people who died, died without their relatives around because there was a lockdown, and people weren’t allowed to visit. . .it was awful. . .and you were left alone to care for them for the last few minutes. . .they could have died better if their relatives had been there” (P1-UK).
People affected by COVID-19 may experience a lonely death, directly impacting the quality of death. As a result, family members face an increased risk of experiencing complicated grief and emotional distress due to challenges in navigating the grieving and bereavement process.
It is crucial to emphasise that participants highlighted the profound sense of isolation in mourning experienced by both family members and patients. The inability to be physically present during a loved one’s final moments not only intensified the loss of the individual but also deprived them of the opportunity for closure.
Similarly, a Brazilian participant reflected, “We live a lonely death. . .and now it’s closed in the CTI, the person stays there and alone. . .it’s very individual. . .the grief is palpable, but if you don’t name it, you don’t find a face for it” (P15-BR). These expressions of grief underscore the profound emotional and social impacts the pandemic had on both healthcare providers and families.
The disruption of end-of-life care by the pandemic led to widespread emotional suffering, not only for patients but for their families and healthcare professionals as well. Both Brazil and the UK saw an increase in premature deaths, as well as a reduction in the quality of death due to the restrictions imposed to reduce contagion. These insights highlight the profound impact the pandemic had on all stakeholders in PC and emphasise the need for continued development in PCe systems that can better manage such crises.
Emerging Opportunities Amidst Crisis: Development and Innovation in Palliative Care
In response to the daily challenges posed by the pandemic, participants identified several unexpected opportunities for growth and innovation within the PC field. Despite the adversity, healthcare teams demonstrated remarkable resilience and creativity, leading to significant improvements in care delivery. One participant from the UK shared, “We’ve moved to virtual and Zoom, and that’s helped us reach more people because some people can’t physically travel to our center (. . .) we’re actually supporting more people now than before (. . .) we’re going to keep some of those outlets in place so that we can continue to reach those people in the community that we can’t see right now, or haven’t seen in the past. This is very interesting, something positive” (P10-UK).
This highlights the role of telehealth as a transformative force, expanding the reach of PC services to previously underserved populations and showing how digital platforms can provide long-term solutions for access to care.
The integration of telemedicine during the pandemic not only increased accessibility for patients who were unable to travel but also demonstrated the potential for these digital innovations to be an integral part of future PC models. This shift represents a positive, enduring change in the delivery of care, which is likely to continue shaping the way services are provided in the post-pandemic world.
Similarly, a participant from Brazil discussed how the pandemic presented unique opportunities to rethink the delivery of PC, especially in home settings. They noted, “The pandemic showed so many opportunities that we have, especially in palliative care, at home, you know, we managed to de-hospitalise many people because our thinking was precisely rehabilitative” (P13-BR). This statement highlights how the crisis has encouraged innovative methods of delivering care outside of traditional hospital settings and has extended the scope of PC into the community.
The pandemic also led to considerable personal and professional growth among healthcare workers. The unprecedented demands placed on professionals prompted them to reflect deeply on their roles and responsibilities, leading to profound transformations. As one Brazilian participant shared, “It made me grow more and more, it made the profession grow more and more (. . .). Still, it was a unique transformation that no health professional or person would come out of this pandemic unscathed. We will leave with reform, complete, spiritual, professional, personal, and social, there’s no way this can’t be transformative in each one’s life, even if it’s through pain and anguish and death faced daily, but that’s what we’re there for (. . .) it was open new paths” (P12-BR). This quote highlights the resilience and adaptability of professionals who faced extraordinary challenges and experienced personal and professional growth as a result.
Throughout the pandemic, healthcare professionals were forced to devise innovative solutions and strategies to ensure the continuity of essential healthcare services, despite significant resource constraints. The need for creativity in this context resulted in a culture of collaboration and problem-solving, which had a lasting impact on the field of PC. The ability to adapt and find solutions in the face of uncertainty became a pivotal strength of PC teams during this period, and these innovative strategies will likely shape the future of care delivery.
Looking back, the experience of PC during the pandemic reveals a complex and deeply human journey, characterised by layers of suffering, uncertainty, reinvention and growth. Initially, patients, families and healthcare professionals were confronted with forms of suffering that had long been unacknowledged: emotional, relational and existential pain permeating every level of care. In response, professionals found themselves thrust into unfamiliar territory, needing to adapt rapidly to chaotic and unpredictable conditions, often without adequate resources or guidance. As the crisis intensified, the painful reality of death in isolation came to light, highlighting the emotional impact of disrupted end-of-life rituals and the profound loneliness that characterised the final moments of many lives. Nevertheless, even in the midst of such devastation, the resilience of PC teams gave rise to innovative practices, expanded access through technology, and new ways of thinking about care beyond institutional walls. While this journey was marked by significant loss, it also became a catalyst for personal transformation, unveiling not only the damaged aspects of the self, but also the potential for reconstruction and rebirth. The lessons learned during this period have the potential to transform PC, ensuring that it remains flexible, compassionate and deeply attuned to the lived experiences of those it serves (Figure 1).
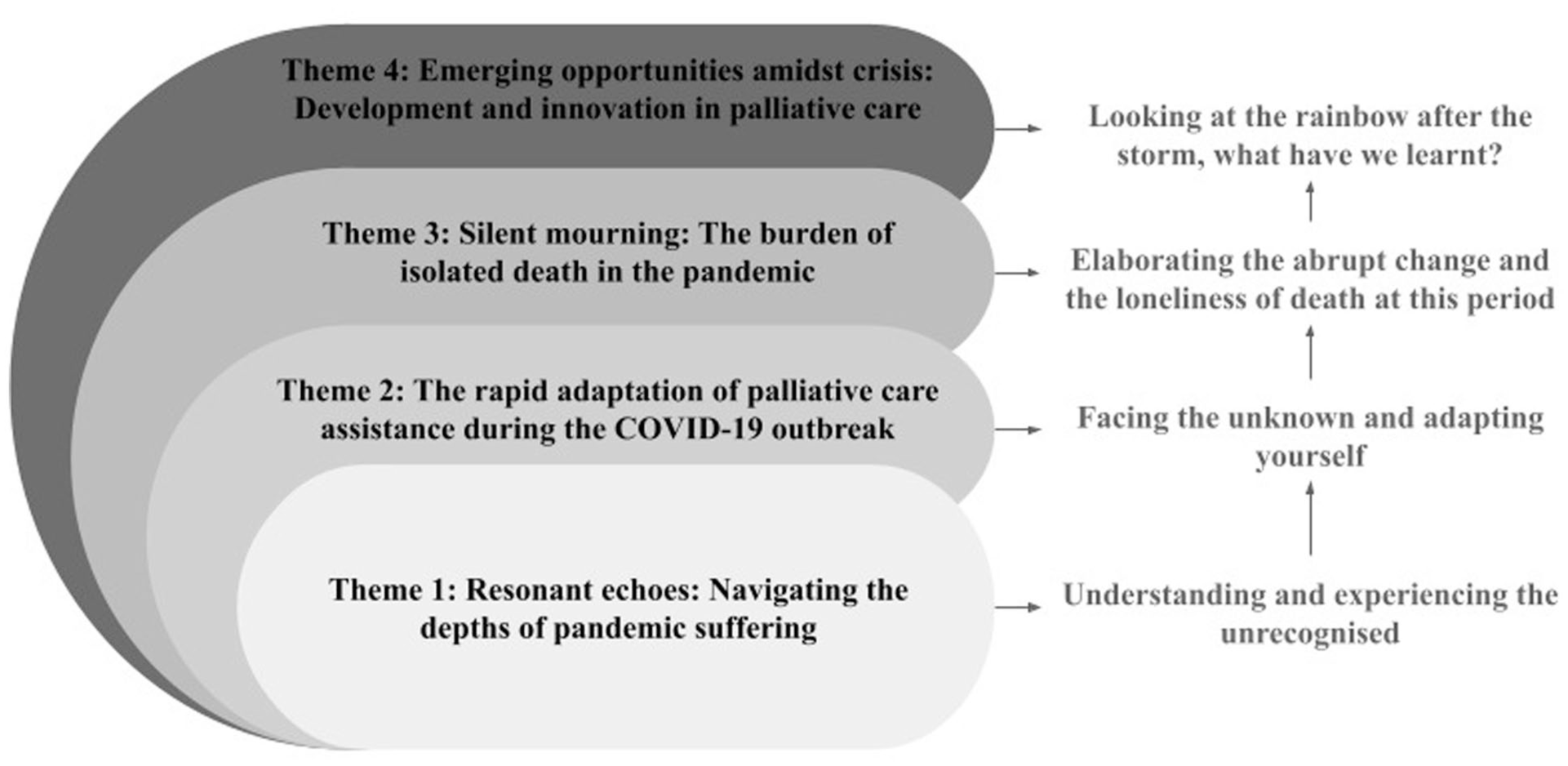
Route during the pandemic considering the thematic units.
Discussion
The COVID-19 pandemic triggered an unprecedented disruption in healthcare delivery, profoundly affecting PC services. This study explored the experiences of healthcare professionals working in PC during the pandemic in Brazil and England. The participants’ narratives revealed that the impacts were multidimensional, affecting their quality of life, clinical practice, and the care delivered to patients and families. These findings are corroborated by the results of a study conducted by Kates et al, 22 which indicate that the COVID-19 placed considerable strain on the PC workforce due to an increased demand for these services. Although demand increased, some healthcare facilities reduced their staff in an effort to contain the disease. As a result, healthcare professionals experienced work overload and difficulties in communicating with patients and families, due to restrictions which hindered effective shared decision-making, a central component of PC, especially at the end of life. 4 The pandemic prompted rapid, significant changes to service structures and delivery models.4,9,34
The differences in PC delivery between Brazil and England were highlighted, with these differences being shaped by structural and cultural factors. In England, PC traditionally prioritises advance care planning, community continuity and a multidisciplinary, person-centred approach to maintaining quality of life at home or in hospices. The pandemic required rapid adaptations, including team reorganisations, teleconsultations, and greater involvement of informal caregivers. However, gaps in integration with emergency services posed additional challenges.2,35 In Brazil, structural weaknesses, regional inequalities and a biomedical focus on cure intensified the challenges. Healthcare professionals experienced an increased workload, shortages of resources, and difficulties in providing humanised end-of-life care. Studies indicate the limited incorporation of PC for hospitalised middle-aged and older adults with COVID-19. Remote strategies and creative solutions are required to sustain patient dignity and interdisciplinary collaboration.36,37
Our findings indicate that healthcare professionals experienced substantial emotional burden during the COVID-19 pandemic, reporting distress related to witnessing patients die in isolation, managing multiple deaths, and coping with anxiety, fear, and guilt arising from infection control measures. Such demands included an increase in patient deaths, solitary and dehumanised deaths, reduced human contact, and uncertainty surrounding the progression of the pandemic. Consistent with Wallace et al 38 psychological distress arises from overwhelming workloads, solitary and dehumanised deaths, and cumulative grief. Evidence suggests that this distress translates into anxiety, burnout and moral suffering, mirroring the impact of the pandemic on mental health.18,39 These experiences negatively impacted their well-being, as also highlighted in previous studies.13,22
Staff reported additional concerns regarding hospices and palliative care services as potential sites of virus transmission, which contributed to uncertainty and heightened emotional stress. 10 Resource limitations, including shortages of personal protective equipment, medications, and other essential supplies, further challenged care delivery, sometimes causing delays or preventing certain interventions. Despite these difficulties, our results demonstrate that palliative care teams rapidly adapted to the situation by increasing online support groups, telephone follow-ups, and other forms of remote assistance, aligning with reports in the literature on innovative strategies adopted during the pandemic.10,34
An important aspect to consider regarding the role and response of health services to PC during COVID-19 is meeting the needs of family caregivers. Participants identified managing deaths and supporting those grieving as a significant challenge during the pandemic. Services were unprepared for the disease’s unpredictable progression, leading to a rise in solitary deaths, complicated grief, and a burden on healthcare workers as well as family members. Due to mandatory physical distancing measures and limitations on funeral ceremonies, such as limited time and the impossibility to see or have contact with the deceased, there is a higher likelihood of complicated grief and subsequent clinical and social consequences. 16
The implementation of social isolation measures and protective protocols to contain the spread of the disease required the restructuring of healthcare services. Traditionally, PC professionals rely on listening, visual contact, physical presence, and, out of necessity due to the pandemic, the integration of virtual care, and they have been forced to adopt various measures to address these challenges. The use of PPE, video calls with family members for healthcare professionals’ or caregivers’ training, and the adoption of measures to ensure continuous care, such as remote clinical consultations through telemedicine, have become predominant.40 -42 There is also a need for innovative methods to provide on-site training for healthcare professionals who are already overwhelmed by the increasing number of patients. It is essential to strike a balance between care provision and ensuring the well-being of healthcare professionals, as well as educating them on the principles of PC. 43 The multidisciplinary team needed to be creative in providing PC education, such as educational videos, individual education, and bedside guidance, 13 and in adopting alternatives to replace human touch, in-person care, communication, and the support of mourning and death in the most humane way possible, even in the face of restrictive measures.
Despite these challenges, the pandemic also offered opportunities for growth and innovation in PC. Professional growth and increased access to PC services were observed for patients and families who could not receive care due to the pandemic or the deterioration of their health conditions and travel difficulties. Services developed quickly to support patients, families, and staff. 44 In the UK, teleconsultation and video conferencing have been widely used by PC teams. 45 To reduce the risk of patient and healthcare professional exposure, institutions, including hospices and community services, have shifted their focus from in-person consultations to teleconsultation. 46 Therefore, it is crucial to ensure equitable access to technology, considering the vulnerabilities and limitations of patients and caregivers in terms of access and their knowledge of using such technologies. 40 Furthermore, the pandemic can serve as a catalyst for positive changes in the future through the adoption of hybrid rehabilitation approaches and the practice of ongoing integrated and collaborative work. 44
Thus, PC has been recognised as an essential component of international responses to the pandemic. There is an urgent need for alternative methods of delivering PC, such as telemedicine, teleconsultation, and bereavement support groups. 43 Our findings endorse the importance of high-quality information, resources, and training to prepare for unexpected events such as pandemics and guide service delivery by providing clear communication and support to manage changes in expectations and working conditions. Future efforts must define PC roles in critical care, develop telehealth protocols, and promote community education, intervention, and outcome research. 41
Furthermore, the findings offer insights that can be applied to practice, research, and education in PC, emphasising the importance of adapting care models, especially through the use of telemedicine, to ensure continuity of care during times of crisis. This practice can be transferred to other healthcare settings, particularly in rural or underserved areas where access to in-person care may be limited. Expanding the use of digital health technologies can increase accessibility and improve the reach of PC services globally. 47 The pandemic highlighted the vital role of PC during crises 18 in addressing the emotional and social needs of patients facing death in isolation, as well as the needs of families grappling with complicated grief. Incorporating PC into crisis response strategies is crucial to alleviating the suffering caused by isolated deaths. 38 This ensures that, even during pandemics, care remains compassionate and holistic, preserving the dignity of both patients and their families at the end of life and the urgent need for PC during pandemics.
Strengths and Limitations
This qualitative analysis yielded important insights into PC delivery during the pandemic, based on interviews in Brazil and England, countries heavily affected by COVID-19. The study captured challenges and strategies adopted by PC teams, offering perspectives often overlooked in quantitative research. By focusing on the lived experiences of healthcare professionals, this research highlights the adaptation, and emotional challenges faced by these workers during an unprecedented global health emergency.
However, the limitations must be considered. The study involved 2 distinct groups of professionals, one in Brazil and the other in the UK. While both countries were severely affected by the pandemic, their responses to it, shaped by the differences in their healthcare systems, are likely to have influenced the experiences of PC professionals.
Another limitation is that repeat interviews were not conducted, and the transcripts were not returned to participants for comment. Although this approach is common in many qualitative studies, it means that there is no opportunity for participants to validate or provide additional insights on their responses after data collection, which may have provided further depth or clarification.
Finally, as is typical in qualitative research, the findings cannot be generalised to broader populations due to the non-probability sampling methods and the subjective nature of the data. However, despite these limitations, the insights gained from this study provide important observations that can inform future research and contribute to the development of evidence-based practices in PC, particularly during health crises like the COVID-19 pandemic.
Conclusion
This study sheds light on the unseen challenges faced by PC professionals during COVID-19 in Brazil and England. Services underwent rapid adaptation to meet care demands, exposing staff to emotional strain, grief, and uncertainty. However, these experiences also fostered professional growth and expanded access to care through remote modalities.
Pandemic-related restrictions reshaped daily practice and underscored the need for integrated PC models. Health systems must strengthen PC capacity to ensure dignified care across all settings, especially in end-of-life scenarios.
Thus, this study underscores the importance of flexible and resilient PC systems capable of adapting to unforeseen challenges. The findings offer recommendations for improving PC practice, enhancing research on digital health technologies and professional wellbeing, and refining educational approaches to better prepare healthcare professionals for future health crises. The incorporation of these recommendations into healthcare systems on a global scale has the potential to enhance the quality of end-of-life care, support the mental well-being of healthcare professionals, and guarantee that patients receive dignified care, even during periods of crisis. Future international studies are essential to compare PC responses and identify facilitators in diverse contexts, enabling evidence-based strategies for improved care in future pandemics.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251384540 – Supplemental material for The Unseen Challenges: A Qualitative and Multicentre Study Exploring the Experiences of Palliative Care Professionals During COVID-19 Crisis
Supplemental material, sj-docx-1-inq-10.1177_00469580251384540 for The Unseen Challenges: A Qualitative and Multicentre Study Exploring the Experiences of Palliative Care Professionals During COVID-19 Crisis by Gabriela Rezende, Gabriel Morais Xavier dos Santos, Cristiane Aparecida Gomes-Ferraz, Ingrid Bacon and Marysia Mara Rodrigues do Prado De-Carlo in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580251384540 – Supplemental material for The Unseen Challenges: A Qualitative and Multicentre Study Exploring the Experiences of Palliative Care Professionals During COVID-19 Crisis
Supplemental material, sj-docx-2-inq-10.1177_00469580251384540 for The Unseen Challenges: A Qualitative and Multicentre Study Exploring the Experiences of Palliative Care Professionals During COVID-19 Crisis by Gabriela Rezende, Gabriel Morais Xavier dos Santos, Cristiane Aparecida Gomes-Ferraz, Ingrid Bacon and Marysia Mara Rodrigues do Prado De-Carlo in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We would like to thank all the services in Brazil and England that kindly collaborated in this work, especially the participants of this study, who gave their time for this research to be carried out, especially during such a difficult time.
ORCID iDs
Ethical Considerations
Ethics approval and consent for participation were granted by the University of São Paulo (number 21189919.0.0000.5393) and the Research Ethics Committee of Kingston University (number 1468) on 5 May 2020.
Consent to Participate
Verbal consent was obtained from all participants prior to the interviews. The process was documented by audio-recording each participant’s explicit verbal agreement at the beginning of the interview, which was securely stored along with the research data. This approach ensured both ethical compliance and traceability of participants’ consent.
Consent for Publication
Participants provided consent to be quoted in publications.
Author Contributions
Gabriela Rezende: organisation of sources and analysis, elaboration of the text, correction, and final revision. Gabriel Morais Xavier dos Santos and Cristiane Aparecida Gomes-Ferraz: organisation of sources and analyses, elaboration of the text. Ingrid Bacon: elaboration of the text; correction of the text. Marysia Mara Rodrigues do Prado De Carlo: elaboration of the text, correction of the text and final revision. All authors approved the final version of the text.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors disclosed the financial support for the research, by the Brazilian Federal Agency for Support and Evaluation of Graduate Education (CAPES), in the scope of the Program CAPES-PrInt (process number 88887.371124/2019-00).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Availability of data and materials Interviews contain personally identifiable information. To access please contact the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.