
Abstract
Bundled payment programs aim to align the incentives of acute and post-acute providers during an episode of care. Prior studies of the impact of bundled payments on hospital length of stay (LOS) were mixed, and none evaluated hospital exposure to bundled payments across all payers (public and commercial). In this study, we used the American Hospital Association survey data for 2016 to 2022 to compare the LOS of hospitals that participated in bundled payments to those that did not participate. We used regression analysis with interaction terms to compare the changes in LOS of hospitals that participated in bundled payments with concurrent changes in LOS of hospitals that did not participate in bundled payments. The models included hospital and year fixed effects. We also conducted subgroup analyses by payer type. All-payer LOS was not associated with participation in bundled payment (ATT 0.08 days; 95% CI −0.34, 0.17; P = .54). Participation in bundled payments was associated with slightly longer LOS for stays paid for by Medicare (ATT 0.13 days, 95% CI 0.02, 0.25; P = .03), but not for the other payer types. Bundled payment program participation had a negligible impact on hospital LOS, acknowledging the limitation that the impact might be diminished due to evaluating average LOS across all admissions rather than condition-specific bundled payment programs.
Introduction
Efforts to improve the quality of care during transitions between hospital and community providers include alternative payment models that aim to better align financial incentives with patient needs. 1 One type of such realignment is bundled payments which reimburse providers for all care provided during an episode: from the initial hospital stay through the post-acute care period. Medicare and other payers implemented several iterations of hospital bundled payment models over the past decade. 2
Prior evaluations of Medicare’s bundled payment programs found that participation decreased the hospital length of stay (LOS). In a 2020 systematic review of the literature on Medicare’s bundled payment programs, 3 of the 10 studies that evaluated hospital LOS, 7 observed a decrease in LOS,4 -10 1 reported a decrease for 1 of 3 conditions studied, 11 and 2 studies did not observe a significant change in LOS.12,13 LOS is an important indicator of program performance as longer LOS is associated with increased risk of patient adverse outcomes such as hospital acquired infections and higher healthcare costs. Moreover, most of the studies were single-center, focused on the procedures and patients targeted by the Medicare bundled payment programs, and none evaluated hospital exposure to bundled payments on LOS across all payers (both, public – Medicare and Medicaid – and commercial).
In this study, we evaluated whether hospital participation in bundled payments is associated with acute care hospital LOS using hospital survey data. Hospital participation in bundled payments was assessed using self-reported participation in any bundled programs in the AHA survey (rather than a payor- or condition-specific bundled payment program). On the one hand, by combining payment for acute hospital and post-acute care, bundled payments may lower hospital LOS by incentivizing faster transitions to post-acute care in the community. On the other hand, because hospitals are at financial risk for poor outcomes in the post-acute period, they may hold on to patients longer to ensure they are ready for discharge, prolonging LOS. Moreover, in resource-restricted settings, efforts to expedite discharge of patients whose hospitalizations were paid for by bundled payments may have unintended spillover effects on the LOS of patients whose cases were excluded from bundled payment.
Methods
This cross-sectional study analyzed data from the 2016 to 2022 American Hospital Association (AHA) annual surveys. The AHA annual survey collects credible and consistent data about the nation’s hospitals, and covers more than 6200 hospitals and 400 health care systems. 14 The dataset provides hospital-level data regarding bundled payment participation and hospital length of stay. The question about bundled payment participation is worded as following: “Does your hospital participate in any bundled payment arrangements?.”
Our study sample included any hospital that met the following inclusion criteria: (1) participated in the AHA survey; and (2) provided a response to the question about participation in bundled payments. All hospitals that met the inclusion criteria in any year between 2016 and 2022 were included in the main analysis. In the first sensitivity analysis, we excluded the year 2020 from analysis to account for healthcare disruptions due to the COVID-19 pandemic; in the second sensitivity analysis, we included only those hospitals that responded to the question about bundled payments for all study years. Hospitals with missing data for this question for any of the years in this survey were excluded.
Our primary outcome was the all-payer LOS, which was calculated at the hospital level from the sum total of hospital days divided by the number of stays, excluding maternity stays. We used all-payer LOS because the bundled payments question in AHA was worded generally and did not specify any particular payor or program. We also calculated the LOS for hospitalizations covered by Medicaid and Medicare, separately. To account for outliers, the dependent variables were winsorized at the top 5%.
We used the Callaway and Sant’Anna 15 regression analysis with interaction terms approach to compare the changes in LOS of hospitals that participated in bundled payments with concurrent changes in LOS of hospitals that did not participate in bundled payments. The models included hospital and year fixed effects. Standard errors were adjusted for clustering at the hospital level.
This study did not involve human subjects and was exempt from review based on the University of Pennsylvania institutional review board guidelines. The study followed the STROBE reporting guideline for cross-sectional studies.
Results
Of the 5501 hospitals surveyed in 2016, 4275 (77.7%) answered the question about participation in bundled payments. Of the 5437 hospitals surveyed in 2022, 3364 (61.9%) answered the bundled payment question. Participation in bundled payments increased over the study period. Of the responders in 2016, 754 (17.6%) reported participating in bundled payments; whereas, of the responders in 2022, 826 (24.6%) reported participating in bundled payments (Figure 1).
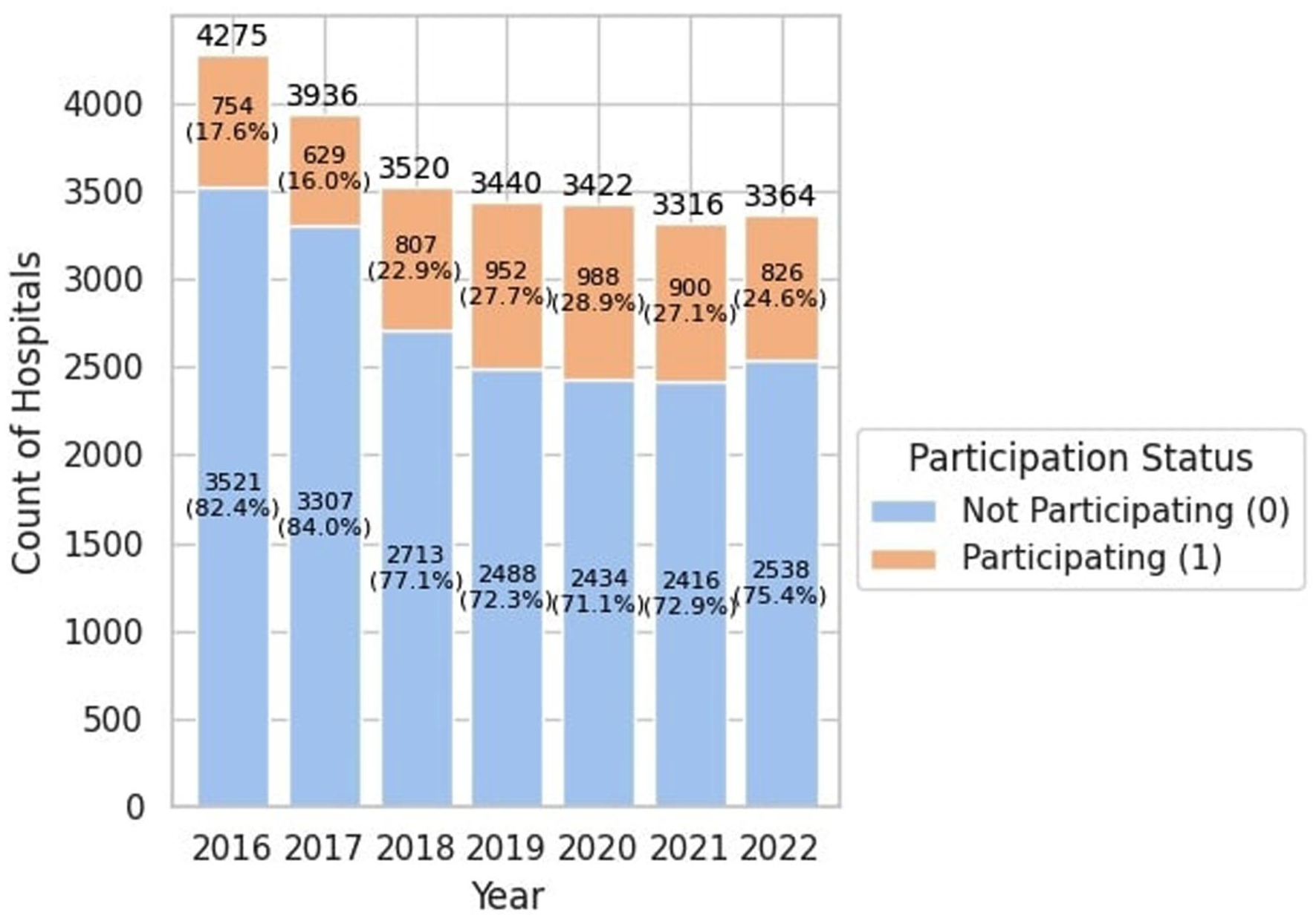
Status of participation in bundled payment among AHA hospitals in 2016 to 2022.
Table 1 shows the differences in facility characteristics between hospitals that reported participation in bundled payments compared to the hospitals that reported not participating in bundled payments, in 2022. Hospitals of smaller size (OR 0.53; 95% CI −0.87, −0.40; P < .001 for 100-399 beds and OR 0.21; 95% CI −1.78, −1.31; P < .001 for <100 beds, compared to ≥400 beds), in more rural locations (OR 0.38; 95% CI −1.24, −0.69, P < .001 for micro and OR 0.28; 95% CI −1.56, −1.01; P < .001 for rural, compared to metro), and non-teaching status (OR 0.24; 95% CI −1.42, 0.14, P < .001 ) were less likely to participate in bundled payments (Table 1).
Characteristics of Hospitals that Participated in Bundled Payments versus Hospitals that Did Not Participate, 2022.

Location categories: Central includes east north central, east south central, west north central states; East coast includes New England, Mid Atlantic, South Atlantic states and associated areas; Mountain includes Mountain states; Pacific includes West South Central, Pacific states according to the U.S. Census division.
A hospital is considered to be a teaching hospital if it has an American Medical Association-approved residency program, is a member of the Council of Teaching Hospitals (COTH) or has a ratio of full-time equivalent interns and residents to beds of 0.25 or higher.
The regression estimates are presented in Table 2. All-payer LOS was not associated with participation in bundled payment (ATT 0.08 days; 95% CI −0.34, 0.17; P = .54). Participation in bundled payments was associated with 0.13 days longer LOS paid for by Medicare (95% CI 0.02, 0.25; P = .03), but not for Medicaid-covered stays (ATT −0.10; 95% CI −0.65, 0.45; P = .72). The results of the 2 sensitivity analyses were consistent with the main results (Table 2).
Association of Hospital LOS and Bundled Payment Participation.

IQR: interquartile range.
ATT: average treatment effect for the treated.
Discussion
Overall, there was no significant difference in the mean all-payer LOS between hospitals that reported participation in any bundled payment programs compared to those of nonparticipating hospitals. Whether a hospital participated in bundled payments was not associated with a change in the LOS for stays covered by Medicaid. In contrast, hospitals that reported participation in bundled payments experienced a slight increase in the LOS for all Medicare-covered stays over the study period.
Our findings contrast several prior evaluations of Medicare bundled payment programs which found that they reduced acute hospital LOS for eligible admissions.4 -10 There are several potential explanations of these potentially conflicting findings. First, participation in bundled payment models puts an emphasis on the hospitals to ensure smooth transition of care to reduce emergency department visits and readmissions. Thus, while decreasing hospital LOS may reduce costs, efforts to provide lower cost post-acute care and ensure safe disposition may incentivize providers to prolong LOS to allow time for more thorough discharge planning.
Second, prior studies on bundled payment programs evaluated the outcomes of patients undergoing procedures or experiencing hospitalizations for conditions targeted by those programs. The observed effects of bundled payments on length of stay may not be generalizable to all patients. Moreover, although the targeted conditions represent a relatively small share of all Medicare acute hospital stays, our finding may represent unanticipated spillover effects. For instance, hospital efforts to reduce LOS for the conditions targeted by bundled payments may prolong LOS for other stays by diverting limited resources to prioritize those discharges.
Third, Medicare implemented multiple iterations of the bundled payments models between 2016 and 2022; some only including acute care hospital stay, while others including both acute care stay and post-acute care stay or home health care. The heterogeneity of the models and their rapid evolution may have forced hospitals to focus quality improvement efforts in specific areas, 16 with potential adverse consequences for patients excluded from the programs. For example, if hospitals facing staffing shortages prioritized physical therapy for the patients whose stays were covered by bundled payments, other patients may have experienced delays with physical therapy, which would have in turn delayed discharge.
Fourth, evaluations of Medicare bundled payment programs observed a shift from more costly facility-based post-acute care (e.g., in skilled nursing facilities) to discharge to home with or without home care. 3 For some older adults, discharge from acute care hospital to community-based post-acute care necessitates more complex planning and care coordination compared to a discharge to post-acute care in a skilled nursing facility. Furthermore, patients that require medical services available in a post-acute care facility (e.g., daily intravenous antibiotics) may prefer to be discharged directly home, even if that choice prolongs their acute hospital stay. The high differential in cost between facility-based and home-based care may incentivize hospitals participating in bundled payments to accommodate patient preferences.
There are several limitations to this study. First, many US hospitals did not answer the bundled payment question in the AHA survey. The majority of non-responder hospitals did not answer any of the survey questions, precluding comparison of their characteristics to the responders. The findings were robust to excluding hospitals that did not respond to the survey in any year during the study period. Nevertheless, the low response rate raises the possibility of selection bias. Second, the hospital-level survey measured whether a hospital participated in any bundled payment programs using a single survey question, and did not distinguish between program types, payers that sponsored the programs, or whether the bundled payments targeted specific medical or surgical episodes. Given that we measured bundled payment participation in general rather than participation in a specific bundled payment program, the current approach may underestimate the effects of individual programs. Similarly, we evaluated all-payer length of stay to match the general question about bundled payments, which may obscure changes in length of stay for subsets of patients targeted by specific bundled payment initiatives. Third, because the AHA survey question asked about bundled payments in general terms and did not specify unique initiatives, we were unable to validate the participation information reported by the hospitals. Future studies using episode level data should evaluate the impacts of hospital participation in specific bundled payment programs on the outcomes and costs of care for specific subgroups of patients, including potential unintended consequences for patients whose episodes were excluded from the programs.
Conclusion
Overall, this study found that bundled payment program participation by acute care hospitals had a negligible impact on the mean hospital LOS between 2016 and 2022. Our findings alleviate concerns that placing hospitals at financial risk for post-acute outcomes may prolong LOS.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251384529 – Supplemental material for Length of Stay in Hospitals Reporting Participation in Bundled Payment Programs: 2016 to 2022
Supplemental material, sj-docx-1-inq-10.1177_00469580251384529 for Length of Stay in Hospitals Reporting Participation in Bundled Payment Programs: 2016 to 2022 by Ye Tian, Jixinyi He and Kira Ryskina in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Ethical Considerations
The study was considered exempt from review by the Institutional Review Board because the research used a secondary dataset aggregated at the hospital level (i.e., not human subjects research). This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline.
Consent to Participate
Informed consent was not applicable to this research because it did not involve human subjects.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.