
Abstract
Asian countries are prioritizing community and home end-of-life care (EoLC) as populations age and care preferences shift. Asian community-based EoLC’s effectiveness is questionable due to cultural, institutional, and healthcare system challenges that affect access and quality. This systematic review seeks components. This makes EoLC effective in Asia. The disparities in care models, how they combine with healthcare institutions, and cultural and family variables are examined. Systematic review (PROSPERO ID: CRD42025644698). The electronic databases PubMed, CINAHL, Scopus, and ScienceDirect were searched in January 2025, evaluating community- or home-based EoLC programs in Asian countries. Twenty articles (8 qualitative studies, 2 quantitative randomized controlled trials, 3 quantitative non-randomized, 6 quantitative descriptive, and 1 mixed methods) fulfilled the inclusion criteria. The review identified the following key aspects of EoLC in Asian communities: symptom management, advance care planning (ACP), family and professional care, cultural sensitivity and spiritual care, healthcare system integration, education, and training. Although EoLC interventions have contributed substantially to improving care quality, the related evidence is inconclusive. Effective EoLC in Asian communities is related to culturally sensitive approaches, the crucial role of family and caregivers, and collaborative decision-making among patients, families, and healthcare professionals. Limited resource access, especially in rural locations, and inconsistent caregiver training and assistance remain issues. Healthcare, healthcare institutions, community resources, and standardized yet flexible criteria that respect spiritual, emotional, and cultural requirements are critically needed to provide fair, high-quality, and person-centered EoLC.
Introduction
The global population is aging, leading to significant demographic changes that profoundly impact health systems worldwide.1,2 Concomitantly, there has been a steady increase in the incidence of non-communicable diseases. 3 While advancements in medical technology have improved survival for chronic illnesses.4,5 Prolonging a patient’s life when there are no chances of recovery may increase the anguish of patients and their caregivers. 6 Therefore, it is essential to refocus from curative treatments to palliative care (PC), which concentrates on managing symptoms and providing holistic care, including physical, emotional, psychological, social, and spiritual support. This approach aims to relieve suffering, fulfill the patient’s final wishes, and enhance their quality of life (QoL).6-8
PC is vital for terminally ill patients and their families, as it provides holistic support during a loved one’s final moments. PC is a multidisciplinary approach to improving patients’ QoL suffering from life-threatening illnesses by addressing their physical, psychological, social, and spiritual needs. 6 However, despite its importance, the WHO 6 reported that only 14% of terminally ill patients globally have access to PC. EoLC is a key component of PC that focuses on terminally ill patients with a life expectancy of 6 months or less. EoLC should be started early in disease progression to ensure a dignified and compassionate death. 9
The WHO 8 reported that community-based EoLC improves the QoL and satisfaction for patients and their families and reduces healthcare costs; however, access to EoLC remains limited, particularly in low- and middle-income countries. 10 In Asian countries, while the need for EoLC at home and in communities increases, a lack of adequate community health services, inequities in access to care, and insufficient pain management resources hamper the provision of appropriate EoLC7,11,12 EoLC in the community in the Asian context is not well documented. Therefore, there is an urgent need to explore existing care approaches and guidelines and identify concerns regarding access inequities. The findings from this review might be beneficial for developing effective community-based strategies for improving the QoL of patients in communities in Asian countries.
Methods
Search Strategy and Selection Criteria
We conducted an extensive literature search across the PubMed, CINAHL, Scopus, and ScienceDirect electronic databases to extract full-text articles related to EoLC published between 2014 and 2025. The Boolean operator “OR” was used for a joint set of synonyms, and “AND” was used for conjunctions. Search terms: “End of life in community” AND “Hospice care” OR “Terminal Care” OR “End of life Care” AND “Quality of life” OR “Family satisfaction” OR “Symptom management.”
Inclusion criteria: (1) articles published from 2014 to 2025, (2) availability of full text, (3) English language, (4) conducted in Asia, and (5) community-based/home-based. Exclusion criteria: (1) Review articles and (2) Commentaries.
Search Outcomes
Two researchers independently screened the extracted results based on titles and abstracts using Rayyan. Rayyan is a technology that makes the screening process easier in systematic reviews. Rayyan automatically finds and removes duplicate research after importing search results from several databases. It lets several reviewers independently and quickly looks at titles and abstracts. AI helps them decide which records are most important, but the reviewers make all the decisions on which records to include. The platform makes everything more open and consistent, and any differences are worked out through conversation. This makes sure that the review has a credible and full list of research to consider. Duplicate publications were deleted. For this systematic review, we defined the following results related to EoLC in Asian countries Symptom management, Advance Care Plaining (ACP), Family Caregivers and Professional Care Staff, Cultural Sensitivity and Spiritual Care, Healthcare System Integration. Figure 1 presents the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram depicting the search strategy. 13

PRISMA (Preferred Reporting Item for Systematic Reviews and Meta-Analyses) flow diagram for study selection.
Data Extraction
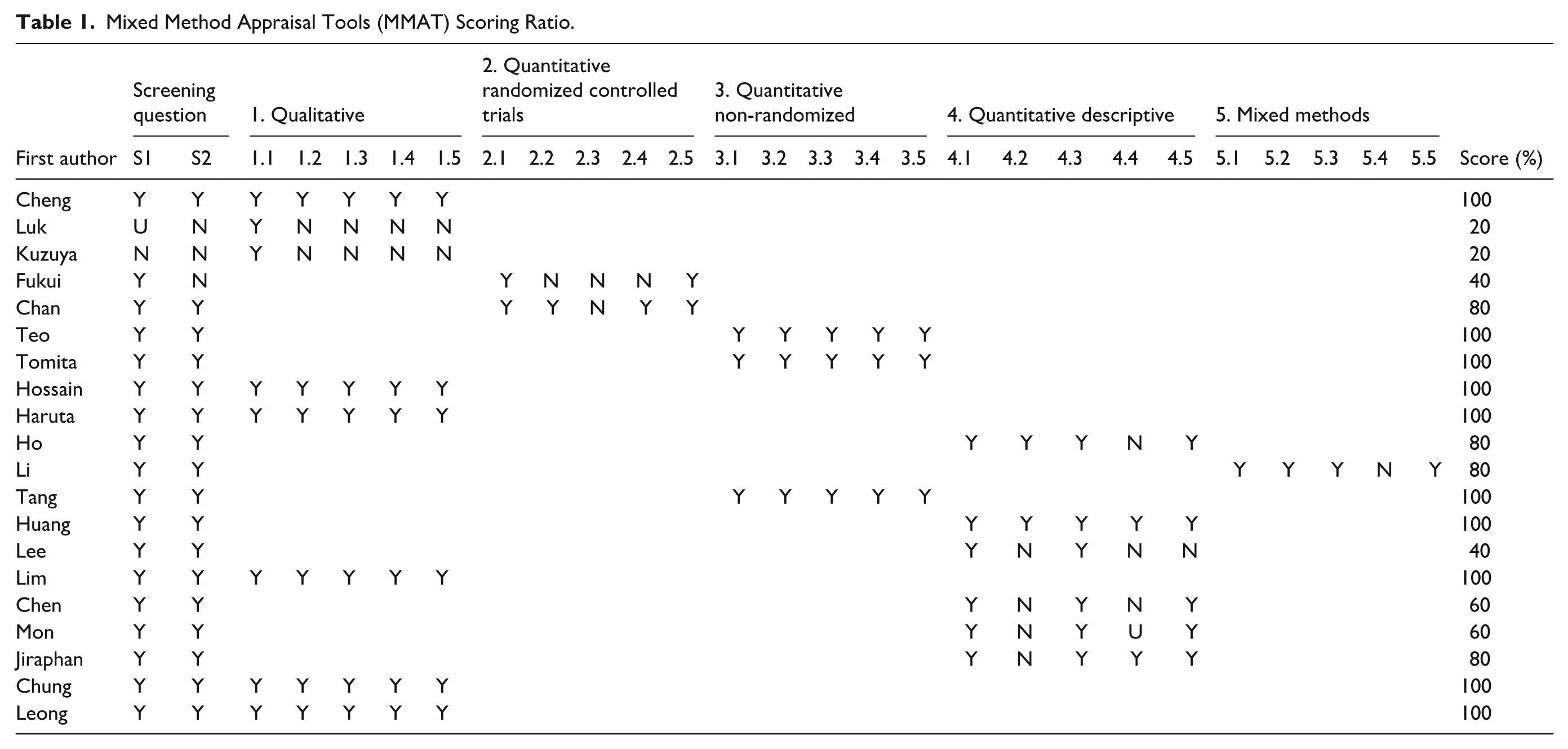
A dedicated Microsoft Excel (for Microsoft 365 MSO, Version 2503 Build 16.0.18623.20116) data extraction form was developed to collect and manage the following data from the included studies: study design and methodology (study purpose, research design, and outcome measures), participant demographics and baseline characteristics, the number of events or measures of effect (as applicable), country of origin, year of publication. The 2 researchers independently extracted data from the included studies to ensure accuracy and reliability (Table 1); duplicate extractions were compared, and any discrepancies or anomalies were discussed and resolved through consensus. If disagreements persisted, a third reviewer was consulted to make the final decision.
Mixed Method Appraisal Tools (MMAT) Scoring Ratio.
Data Synthesis and Integration
To obtain a holistic view of the effectiveness of EoLC in the community and its impact on QoL, we examined the following outcomes: QoL of the patients and their families, satisfaction among the patient and family, symptom management, emotional support, psychosocial support, spiritual support, and the concept of dying with dignity. These outcomes were selected to provide a comprehensive understanding of the characteristics of care contributing to the success of EoLC in community. 14 For data synthesis, we used Cochrane Methodology for Systematic Reviews. 15 Because of the heterogeneity among the included studies in terms of samples, methods, interventions (different models of community-based EoLC across Asia), study designs, and outcome measures, a meta-analysis could not be performed. Instead, we conducted a narrative synthesis to integrate and interpret the findings, allowing for a detailed exploration of the diverse evidence base 16 and providing meaningful insights into the effectiveness of EoLC in the community. For narrative synthesis using a structured approach, we organized the data by grouping studies based on key themes, such as ACP, symptom management, family caregivers and professional care staff, cultural sensitivity and spiritual care, and education and training. Additionally, we explored the characteristics of care and the success of EoLC in communities in Asia.
Results
Characteristics of the Included Studies
Using the aforementioned search strategy, we extracted 225 articles from the databases. After removing duplicates, we screened the study titles and checked for the availability of full texts; finally, 20 relevant articles were selected for review (Figure 1). Eight of these studies were qualitative (Table 2; study no: 1-3, 8, 9,15, 19, and 20), 2 articles were quantitative randomized controlled trials (study no: 4 and 5), 3 articles were quantitative non-randomized (study no: 6, 7, and 12), 6 articles had a quantitative descriptive design (study no: 10, 13, 14, and 16-18), and 1 article used mixed methods (study no: 11). In terms of geographical location, there was 1 study from Thailand (study no: 18), 2 from Malaysia (study no: 19 and 20), 4 from Hong Kong (study no: 1, 2, 5, and 10), 3 from Taiwan (study no: 11,13, and 16), 4 from Japan (study no: 3, 4, 7, and 9), 2 from South Korea (study no: 14 and 15), 2 from Singapore (study no.: 6 and 12), 1 from Myanmar (study no: 17), and 1 article covering Bangladesh, India, and Pakistan (study no: 8). Table 2 presents a summary of the characteristics of the included studies.
Summary of the Articles Included in the Systematic Review (n = 20).

Symptom Management
Symptom management in EoLC is primarily aimed at reducing distress in terminally ill patients. Six studies specifically addressed symptom management in EoLC (study no. 14-17, 19, and 20). In Malaysia, subcutaneous infusions and family care were primarily used to enhance home pain management, reduce emergency visits, and increase comfort. 17 A study from Myanmar reported that tools such as Functional Assessment of Cancer Therapy General (FACT-G) and pain scales were used for structured symptom control. 18 A Korean study highlighted the need to address the physical, psychological, social, and spiritual needs of patients with chronic illness and stated that lower Palliative Performance Scale scores reflect a greater need for support. 19 Another Malaysian study described that spirituality aided in offering peace to patients, highlighting the need for culturally sensitive care such as respecting religious beliefs, facilitating traditional healing practices, accommodating rituals related to EoL, and supporting family involvement in decision-making 20 In Taiwan, family caregivers play a key role in symptom management and preferences for home death; accordingly, providing adequate support to caregivers through training reduces anxiety and enhances care quality for the patient is essential. 21
Leong et al also stated that community services were essential for aiding caregivers and facilitating home EoLC in Malaysia. Patients with low-income struggle to access pain medication, leading to poor pain management. 17 Notably, rural areas often lack PC services, worsening symptom management. 18 Caregivers usually struggle to manage complex symptoms without adequate support, leading to emotional distress. 20 Huang et al 22 noted that barriers within healthcare systems include low participation levels in professional discussions related to EoLC, which limit the effective integration of symptom management. Similarly, in Japan, healthcare professionals found it difficult to adopt ACP due to language-related challenges, which also influenced the low effectiveness of symptom management. 23 Additionally, cultural and communication barriers cause complicated discussions about care planning and decision-making. 20 These issues indicate a significant need for improved education and communication strategies within healthcare systems to support EoLC. This is a region-specific problem. In Taiwan, hospice services are frequently overlooked, restricting the scope of symptom management and creating gaps in healthcare delivery. 21 Such limitations reflect broader regional trends within parts of Asia, where disparities in access to EoLC resources are evident. Rural areas, in particular, face significant resource shortages compared to urban areas, accentuating the need for systemic improvements to equitable care delivery. Symptom management at the EoL remains a substantial challenge, especially in home and community settings, where caregivers often struggle with complex pain crises and must administer anticipatory subcutaneous injections with limited support. The lack of easily accessible palliative care services, inadequate training, 24 and concerns about medication safety can contribute to distress among both patients and family caregivers, highlighting the urgent need for comprehensive support systems and education to ensure effective and dignified symptom control at home.17,24
Advance Care Plaining (ACP)
ACP is an essential process in PC that allows individuals to indicate their preferences for EoLC in advance. Six studies specifically addressed ACP in EoLC (study no: 3, 5, 8, 10, 11, 19). It comprises the following key components: (1) shared decision-making, (2) documentation of preferences, (3) advance directives, (4) cultural and contextual influences, and (5) predictors of discussion frequency. The success of EoLC depends heavily on effective communication between patients, families, and healthcare professionals.23-26 Shared decision-making is a crucial step that reflects the values of patients and their families through open conversations.23-26 It emphasizes aligning healthcare decisions with the patients’ and their families’ unique cultural, ethical, and personal values. Preference documentation involves writing or recording a person’s specific preferences for their desired treatment and care options during EoLC. 27 Over recent years, there has been an increase in the completion of advance directives and “do-not-attempt cardiopulmonary resuscitation” documentation in Asia. This trend indicates a shift toward formalizing patients’ wishes regarding EoLC.
Advance directives 26 refer to legal documents that specify future healthcare wishes if patients cannot decide for themselves. These ensure that the patient’s treatment preferences are respected. However, Ho et al reported that over 70% of participants from some regions in Asia—for example, Hong Kong, Japan, and Korea—opted not to formalize their EoLC decisions, raising concerns about the understanding and utilizing ACP. Cultural and contextual influences23,26,28 affect patients’ EoLC-related decisions. These findings indicate the importance of tailoring ACP approaches to incorporate individual values and beliefs 20 Studying factors influencing advance directive discussion helps us understand how crucial conversations between patients, families, and providers can be improved. Increased patient confidence in EoLC has led to more discussions about advanced directives among caregivers and residents with dementia. 25 However, many healthcare providers report infrequent engagement in these discussions, 27 highlighting a communication gap. This gap reflects differences in ACP understanding and treatment-related decision-making.27,28 Furthermore, different age groups showed varying participation levels in treatment decisions. Many individuals desire to be informed about their condition and avoid burdening their families, a preference underscoring the need for clarification and inclusive communication in ACP.23,27 These findings illustrate the complexities associated with ACP, emphasizing the need for effective communication, cultural sensitivity. 25 Healthcare providers work closely with patients, taking time to listen and understand their values and preferences, so that every aspect of care truly reflects what matters most to each individual.
Family Caregivers and Professional Care Staff
Family caregivers (study no: 5, 7, 8, 10, 14, and 20) and healthcare staff (study no: 1, 7, 12,13, 15, and 19) play a crucial role in delivering effective EoLC in community settings. Several studies have emphasized the importance of collaborative approaches that empower families17,19,29,30 respect cultural values25,26,31 and improve communication between family members and healthcare providers.21,22,32 Addressing these aspects can significantly enhance the QoL and support during EoLC. 33
Furthermore, collaboration among different sectors—such as healthcare systems, community organizations, and social services—was identified as vital for meeting caregiver and staff needs and enhancing service integration. 33 Notably, many patients rely on non-governmental organizations (NGOs) due to inconsistent public healthcare funding and limited governmental resources. 33 NGOs often provide vital psychological support, spirituality, and social activity programs, which fill the gaps left by public healthcare systems. The combination of public healthcare services and NGO support creates a more comprehensive care network, addressing both medical and emotional needs for patients and their families. 33 Family preferences25,26 and cultural contexts play a significant role in EoLC decision-making by influencing how families engage in care processes.25,26,31 Hence, culturally sensitive support is essential for diverse families in EoLC planning. 26 Some authors have also described the importance of effective communication between families and healthcare providers to enhance care quality.20,29 Hossain et al 25 reported that a lack of knowledge about dementia hinders the provision of support for families and staff. Therefore, empowering caregivers by providing training can improve EoLC experiences at home and aid nurses in better supporting the patient.19,32 Healthcare professionals should regularly visit such patients to provide consistent support, even if families may overlook the importance of professional care.
Cultural Sensitivity and Spiritual Care
EoLC should address the patient’s and families’ emotional, psychological, and spiritual needs. Moreover, key components of EoLC in Asia are influenced by cultural and religious values. Eight studies highlighted the importance of cultural sensitivity and spiritual care in community-based EoLC in Asia (study no: 3, 8-10, 11, 15, 18, and 19). Chung et al described that spirituality aided Malaysian patients in finding peace during their final moments, especially in culturally diverse settings; they also stated that holistic care addresses emotional and existential concerns. 20 Lim and Chang 32 noted that spiritual care helps patients accept their mortality and maintain dignity. Likewise, patients from Bangladesh, India, and Pakistan stated that religious practices like prayer provided them comfort and helped maintain their cultural identity. 25
Family involvement is crucial in EoLC decisions in some Asian cultures.18,31 In Japan, family preferences often overshadow the patient’s, highlighting the need to ensure collective decision-making. 31 In Malaysia, involving families in care planning was associated with fostering trust and helped align the expectations of EoLC. 17 Haruta et al. 34 concluded that community engagement in Japan through narrative-based education promotes reflection on mortality and a community-focused approach to EoLC. In summary, despite communication barriers and cultural stigma related to EoLC, integrating spiritual care, and fostering sensitivity can enhance the quality of EoL and ensure compassionate and dignified support for patients and their families. 34
Healthcare System Integration
Healthcare systems in Asia differ widely in terms of resources, policies, and cultural contexts, making healthcare system integration crucial for enhancing the quality and equity of EoLC. Twelve of the 20 studies (study numbers 1-9, 13, 16, and 20) discussed the challenges and strategies of integrating EoLC into community settings, identifying key focus areas such as cost-effectiveness and resource optimization. For instance, Singapore’s national frameworks support the incorporation of EoLC into healthcare systems by offering funding, training, and guidelines. A report on Singapore’s Project CARE on nursing home residents showed significant economic benefits by reducing hospital admissions and healthcare costs while improving the quality of care in nursing homes during patients’ final months. 35 Integration ensures better resource allocation and patient outcomes while improving access to EoLC in communities. In Malaysia, integrating EoLC initiatives at the community level allowed patients to receive care at home, easing pressure on hospital systems. 17 Similarly, community programs in Hong Kong provide comprehensive EoLC by reducing service fragmentation and collaborating with social services to offer holistic support tailored to patients’ diverse needs.33,36 These efforts to build better-integrated systems are pivotal for addressing the gaps in EoLC service provisions, particularly in community settings.
Discussion
Success of EoLC in Communities in Asia
The effectiveness of community-based EoLC in Asia fundamentally depends on the successful integration of healthcare systems. Multiple studies included in this review highlight that gaps in coordination between hospitals, primary care providers, community health resources, and specialist PC services often result in fragmented care and suboptimal outcomes.17,33,35,36 For integration to work, there need to be clear roles for interdisciplinary teams, efficient referral paths, and accessible health records.35,36 Initiatives such as integrated care networks and community-based palliative outreach demonstrate potential to bridge these divisions and ensure continuity of care for patients in their preferred settings.17,35 Furthermore, coordinated funding mechanisms and unified training standards across sectors may help standardize quality and access across diverse geographic and organizational contexts.30,33 Beyond system-level organization, cultural considerations have a significant influence on EoLC delivery in Asian communities. Many Asian societies place a high value on family-led decision-making and collective approaches to care, which shapes not only treatment preferences but also communication patterns between care teams and families. Respecting these cultural norms—such as involving family members in discussions about prognosis and care planning—is essential for ensuring satisfaction and minimizing distress at the EoL. 17 However, healthcare systems must find ways to respectfully engage with these cultural expectations while upholding ethical principles of autonomy and informed consent.17,23
Another critical finding from this review is the essential role of caregiver support. Most EoLC in the community rely heavily on family caregivers, who frequently experience significant physical, emotional, and financial burdens.17,20,25 Several studies reported inadequate access to respite care, insufficient caregiver training, and limited psychosocial support networks.17,25 Without targeted interventions—such as structured caregiving education, psychological counseling, and financial assistance, caregiver strain can jeopardize both patient outcomes and the sustainability of community-based EoLC. Policymakers and healthcare providers should prioritize the development of accessible, flexible caregiver support services embedded in EoLC models.17,25
Finally, disparities in resource access continue to be a substantial barrier to effective EoLC in Asian communities. Rural areas, in particular, often lack specialist PC teams, essential medications, and reliable transport for home visits. Economic constraints and uneven resource allocation within health systems further exacerbate these disparities. Innovative solutions, such as telehealth and regional resource-sharing initiatives, have shown promise but require greater investment and policy support to be widely sustainable. Achieving equitable resource distribution is crucial for ensuring that all communities—regardless of location or socioeconomic status—have access to dignified, high-quality EoLC.
In summary, advancing EoLC in Asia requires not only better-integrated healthcare systems but also culturally responsive care, enhanced support for caregivers, and improved access to resources. Addressing these interconnected challenges holistically will help close existing gaps and move toward more equitable, person-centered EoLC throughout the region.
Conclusion
The effectiveness of Asian EoLC is related to cultural beliefs, family roles, system efficiency, and professional support. This study suggests that EoLC quality depends on collaboration and adaptability among healthcare facilities, families, and professionals to meet patients’ needs and address their diverse beliefs. Group and family decision-making in Asian cultures affects patient treatment. Family, patients, and medical professionals must collaborate on EoL decisions and preparation to honor dignity. Limited resources, access, especially in rural regions, and caregiver education and support remain challenges. The systematic review suggests that standardized yet flexible solutions for the diverse spiritual, emotional, and social needs of different groups are urgently needed. To empower families and professionals, public healthcare, NGOs, and community networks must collaborate on caregiver training, psychological support, and symptom management. Develop evidence-based recommendations for equitable and high-quality EoLC in Asian communities, considering patient and caregiver perspectives. Develop and train family caregivers and healthcare staff to enhance their skills and support. Healthcare providers, community groups, and legislators should collaborate to strengthen access and organization. Managing these complex concerns will make EoLC more person-centered, respectful, and effective for Asians.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251382394 – Supplemental material for Effectiveness of End-of-Life Care in the Community in the Asian Context: A Systematic Review
Supplemental material, sj-docx-1-inq-10.1177_00469580251382394 for Effectiveness of End-of-Life Care in the Community in the Asian Context: A Systematic Review by Kanlayawee Anonjarn and Yaowarat Matchim in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Ethical Considerations
Not applicable.
Consent to Participate
Not applicable
Consent for Publication
Not applicable.
Author Contributions
Kanlayawee Anonjarn: Conceptualization, Methodology, Validation, Formal analysis, Investigation, Data curation, writing e original draft, Writing e review & editing, Project administration. Yaowarat Matchim: Conceptualization, Methodology, Validation, Formal analysis, Resources, Data curation, Writing e review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Research Unit in Palliative care for Adults and Older Adults, Faculty of Nursing,Thamasart University.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.