
Abstract
Independent living depends on basic self-care tasks, yet their impairment has not been quantified at the national level in Saudi Arabia. This study aimed to estimate the national prevalence of self-care difficulty among Saudi citizens and identify associated factors across demographic (sex, age, education, marital status), geographic (administrative region), clinical (severity, cause, duration, chronic disease), and family/household indicators (relationship to household head, consanguinity) using the 2017 Saudi National Disability Survey. A retrospective cross-sectional analysis was conducted using the 2017 Saudi National Disability Survey (N = 20 408 362 Saudis). Thirteen Washington Group indicators were extracted; design-based χ² tests and survey-weighted logistic regression assessed associations. Overall, 238 984 individuals (1.2%) reported difficulty with bathing, dressing, or toileting—1.1% of males (112 319) and 1.3% of females (126 665). Most cases co-occurred with additional disabilities (227 609; 1.1%); isolated self-care difficulty was uncommon (11 375; 0.1%). Adjusted odds were higher in Asīr (AOR = 1.42, 95% CI 1.30-1.55) and Ḥāʾil (AOR = 1.36, 95% CI 1.22-1.53) relative to Al-Riyadh, rose sharply with severe/extreme limitation (AOR = 6.11, 95% CI 5.71-6.54), and were elevated among individuals from first-cousin marriages (AOR = 1.58, 95% CI 1.48-1.68). Disease-related aetiology, disability duration ≥ 25 years, and receipt of Ministry of Labour benefits were independent correlates, whereas tertiary education unexpectedly predicted higher risk. Self-care difficulty affects a modest proportion of Saudis, yet the absolute burden approaches a quarter-million people, clustering in peripheral provinces and among long-standing, severe cases. Targeted rehabilitation, premarital genetic counselling, and regionally equitable service expansion will be essential to fulfil Vision 2030 equity goals. Routine national monitoring of activity-of-daily-living limitations is needed to guide person-centred resource allocation.
Keywords
Highlights
● Self-care difficulty affected 1.2% of Saudi citizens (≈239,000 people), most often in combination with other disabilities.
● Higher severity, disability duration ≥25 years, disease- or delivery-related causes, consanguinity, and residence in Aseer or Hail were independent predictors.
● Women were overrepresented in multi-disability cases and relied more on day- and home-care services, while men more often reported milder deficits and received in-kind benefits.
● Regional and gender disparities in prevalence and service uptake indicate systemic inequities in disability support.
● Results highlight the need for targeted rehabilitation, premarital genetic counselling, and regionally equitable expansion of services under Vision 2030.
Introduction
Self-care denotes the cluster of basic activities of daily living—bathing, dressing, toileting, eating, and related routines—that people ordinarily perform independently to maintain personal hygiene and health. 1 In the International Classification of Functioning, Disability and Health, the World Health Organization (WHO) locates self-care within the activities and participation component, emphasising that tasks such as washing, drying, and looking after one’s body constitute a discrete domain of functioning. 2 Consistent with that framework, the ICD-11 introduces the category “Difficulty or need for assistance with self-care” (QF24) to identify individuals whose impairment in these tasks warrants clinical attention or support services. 3 The WHO Disability Assessment Schedule 2.0 (WHODAS 2.0) operationalises this construct through items on washing, dressing, eating, and managing daily routines, each rated on a 5-level severity scale that yields domain-specific and global functioning scores.4,5 These classification systems underscore that limitations in self-care are not merely private inconveniences but observable, measurable restrictions in activity that can trigger health-care utilisation and social disadvantage. Even diagnostic manuals such as the DSM-5-TR recognise that motor or cognitive impairments become clinically significant when they “persistently interfere” with age-appropriate self-maintenance. 6 Together, these converging definitions provide a coherent conceptual scaffold for examining population patterns of self-care difficulty and for situating empirical findings within global disability discourse. Accordingly, the present study aims to quantify the national prevalence and severity of self-care difficulty among Saudi citizens, to map its sociodemographic and clinical correlates, and to identify independent predictors that can guide targeted interventions and policy reform. To maintain focus, the background that follows is deliberately selective and serves 2 purposes: (i) to specify the mechanisms and contexts that motivate our 13 Washington Group–aligned indicators (clinical severity, aetiology, chronicity; demographic factors; administrative region; household structure/consanguinity; and service receipt), and (ii) to justify the a priori hypotheses tested. International evidence is cited only insofar as it clarifies mechanisms; emphasis is placed on the Saudi policy and service environment because our outcomes are national in scope.
Beyond traditional rehabilitation and environmental supports, AI-enabled assistive technologies are increasingly used to monitor and support activities of daily living, personalise prompts, and enhance independence—especially for people with cognitive, neurodevelopmental, or mobility limitations. Recent reviews report substantial potential alongside ethical and implementation challenges; these tools may complement population-level strategies by reducing unmet support needs in self-care. Although AI was not evaluated in this study, we note its growing relevance for future service planning (eg, Refs.7 -9).
We interpret self-care difficulty within established models of disability, notably the Disablement Process and the International Classification of Functioning, Disability and Health (ICF). In this view, health conditions and impairments interact with personal factors (eg, age, sex, education, marital status) and environmental factors (eg, region-level access, family structure/consanguinity, service receipt) to influence Activities such as self-care and downstream Participation. Our covariates were therefore selected to represent these domains and to test how body functions/structures (severity, cause, duration, chronic disease) and contextual factors (region, education, household relationships) are associated with self-care difficulty at population scale.9 -12 Guided by the framework, we hypothesised that self-care difficulty would be more likely among: (H1) individuals with greater functional severity; (H2) those reporting longer duration and/or chronic disease as a cause; (H3) residents of higher-burden regions; (H4) those in households with consanguinity; and (H5) older adults and those with lower education. We also explored sex and marital status differences without directional a priori expectations.
Self-Care Epidemiology
This subsection highlights mechanisms most directly linked to our outcome (self-care difficulty) and covariates, focusing on evidence that informs measurement choices and expected directions by age, sex, and comorbidity. Building on this conceptual definition, studies reveal 2 epidemiological threats in self-care. Cramped bathrooms amplify musculoskeletal stress during toileting transfers, injuring caregivers12 -14 and justify spatial adaptations and aids. 15 Concurrently, inadequate hygiene sustains infection: household microbe spread remains substantial, 16 and hand-washing varies by gender, class, and mental health.17 -19 Rural pupils lacking WASH knowledge face more diarrhoea, 20 while integrated soap-water-education halves disease in remote Aboriginal children. 21
Further, self-care activities—bathing, dressing, toileting—pose environmental constraints and manual-handling risks for home caregivers 12 and threaten autonomy in institutions when physical or cognitive decline erodes dignity.22,23 Assistive innovations such as garment-handling walkers lessen burden and restore privacy. 24 Nonetheless, hospital and community surveys reveal high functional deficits, 25 predicted by grip strength after stroke 26 and worsened by geriatric syndromes in nursing homes. 27 Sustained self-care supports well-being 28 and is culturally anchored in family caregiving, as in Turkey. 29
Extending the preceding discussion, age stratification exposes pronounced gradients in personal-care limitation. U.S. trends show modest increases at 55 to 64 years, stability at 65 to 84, and sharp escalation past 85 years. 30 French data confirm that, net of impairment, bathing-and-dressing restrictions surge after 70 and are higher for institutionalised men under 70. 31 Globally, PURE participants aged 50+ report more activity limitations and lower assistive-device use in lower-income settings, 32 while Australian registers document rising home- and transition-care uptake among adults <65. 33 Knowledge gaps persist in Botswanan schoolchildren. 34 Young women endured higher stress and poorer self-care during COVID-19, 35 whereas mid-life male carers adopted unhealthier diets while assisting co-residents. 36 Among middle-aged Iranians with diabetes, inadequate education predicted weaker self-care routines. 37 These age-linked disparities foreshadow the health consequences of inadequate self-care addressed in the next section.
Following the life-course disparities already highlighted, inadequate self-care precipitates wide-ranging harm. Sub-optimal hygiene and inactivity accelerate diabetes, hypertension, and heart-failure progression; they also raise HbA1c and body-mass index in newly diagnosed diabetes.38 -40 Indonesian data link poor skin-, nail-, and hand-cleansing to dermatitis. 41 Depression undermines self-efficacy in heart-failure cohorts, while overstretched personal-care attendants experience high stress that can erode care quality.42,43 Low health literacy, unprepared caregivers, and insecure WaSH conditions intensify morbidity, gender-based violence, and social withdrawal.44 -46
Extending the discussion of health impacts, assisting with bathing, dressing, and toileting is hindered by intersecting structural, client, and workforce barriers. Home-care aides describe rigid visit times, lone working, and dementia-related refusals that thwart task completion. 47 Even advanced scheduling algorithms cannot fully resolve urban matching problems, while rural users face labour shortages and long travel distances.48,49 Low pay, uneven regulation, and scant training fuel recruitment gaps and turnover.50,51 Carers must also preserve dignity during intimate tasks, absorb emotional labour, and manage violence, infection risk, and multicultural communication challenges.52 -54 COVID-19 disruptions exposed the workforce’s fragility and heightened unmet needs, 55 setting the stage for how cultural contexts further shape assistance practices.
Cultural scripts strongly shape how assistance with bathing, dressing, and toileting is negotiated. Language differences may slow instruction-giving and provoke resistance, yet older residents often describe migrant personal-care attendants as more observant and sociable than local staff despite limited English. 56 Where speech falters, mismatched non-verbal cues and divergent norms about touch can breed misunderstanding, underscoring the need for team protocols that foreground cross-cultural communication. 57 Transcultural-care models advocate trained cultural mediators to bridge world-views and protect dignity.58,59 Recognising patients’ explanatory beliefs fosters trust and adherence, 60 while family-centred approaches remain pivotal for ethnically diverse caregivers navigating formal services. 61
Self-Care Practices in Saudi Arabia
This subsection foregrounds Saudi-specific prevalence, service distribution, and regulatory context that plausibly shape regional and sex-stratified differences in self-care difficulty, thereby motivating inclusion of region, education, marital status, and service uptake in our models. Turning to Saudi Arabia, the context of this paper, a national household survey places disability prevalence at 3.3%, highest among men and adults aged 60+. 62 Urinary incontinence illustrates self-care challenges: 44% of women in the western region and 41% in Jeddah are affected, driven by multiparity, obesity, ageing, and pelvic surgery.63,64 Coverage is uneven—urban Riyadh and Makkah host more continence and rehabilitation services than peripheral provinces, and most women never seek help.65,66 Vision 2030 reforms, including workforce Saudization, machine-learning cost modelling, and primary-care expansion, aim to narrow these gaps.67,68
Following the service-gap picture outlined above, Saudi policy now rests on a 2-tier foundation: a rights-based legal framework and the Vision 2030 quality-of-life agenda. The 2023 Saudi Law on the Rights of Persons with Disabilities obliges providers to ensure “reasonable accommodation,” yet a review notes weak enforcement and scant gender-specific provisions. 69 Vision 2030 action plans have prioritised inclusive education and health, but recent audits still find poor toilet, ramp, and signage compliance in a tertiary hospital 70 and only 83% structural accessibility in newly built primary-care centres versus 67% in rented clinics. 71 Community surveys echo these deficits in the wider built environment, 72 dental clinics,73,74 and school mental-health support. 75 To close these gaps, scholars call for stronger monitoring, mandatory disability-design standards, and workforce training that aligns national statutes with UN Convention benchmarks.76,77
The Present Study
Although Vision 2030s pledge to improve disability surveillance, Saudi research on self-care has been confined to small clinical samples—principally urinary incontinence among women—leaving national prevalence, geographic distribution, and multifactorial determinants unknown.62,63 Using the 2017 Saudi National Disability Survey, the present analysis closes this gap by delivering the first population-based profile of self-care difficulty across 20.4 million citizens. Seven tables quantify overall and regional prevalence (Table 1), disentangle single versus multiple-disability cases (Tables 2 and 3), and relate self-care status to education, marital status, consanguinity, aetiology, duration, and Ministry-of-Labour service uptake (Tables 4 and 5). Sex-stratified χ² tests (Table 6) and a fully adjusted logistic model (Table 7) identify independent demographic, geographic, and clinical predictors drawn from 13 indicators. By mapping both clinical (severity, cause, chronicity) and non-clinical (education, region, social support) correlates, this study aims to inform targeted rehabilitation, early-screening initiatives, and equity-oriented policy reform in Saudi Arabia.
Distribution of Individuals with Self-Care Difficulty (Bathing, Dressing, or Using the Toilet) by Administrative Region and Gender, Saudi Arabia.

Note. Data from General Authority of Statistics. (2017). Disability Survey 2017. This table includes all individuals with self-care difficulty, whether as a single disability or in combination with other disabilities (n = 238 984).
Distribution of Individuals With Self-Care Difficulty as a Single Disability by Indicator and Gender, Saudi Arabia.

Note. Data from General Authority of Statistics. (2017). Disability Survey 2017. This table includes individuals with self-care difficulty as a single disability only (n = 11 375).
Distribution of Individuals With Self-Care Difficulty as Part of Multiple Disabilities by Indicator and Gender, Saudi Arabia.

Note. Data from General Authority of Statistics. (2017). Disability Survey 2017. This table includes individuals with self-care difficulty as part of multiple disabilities (n = 227 609).
Distribution of Individuals With Self-Care Difficulty as a Single Disability by Educational and Marital Status, Saudi Arabia.
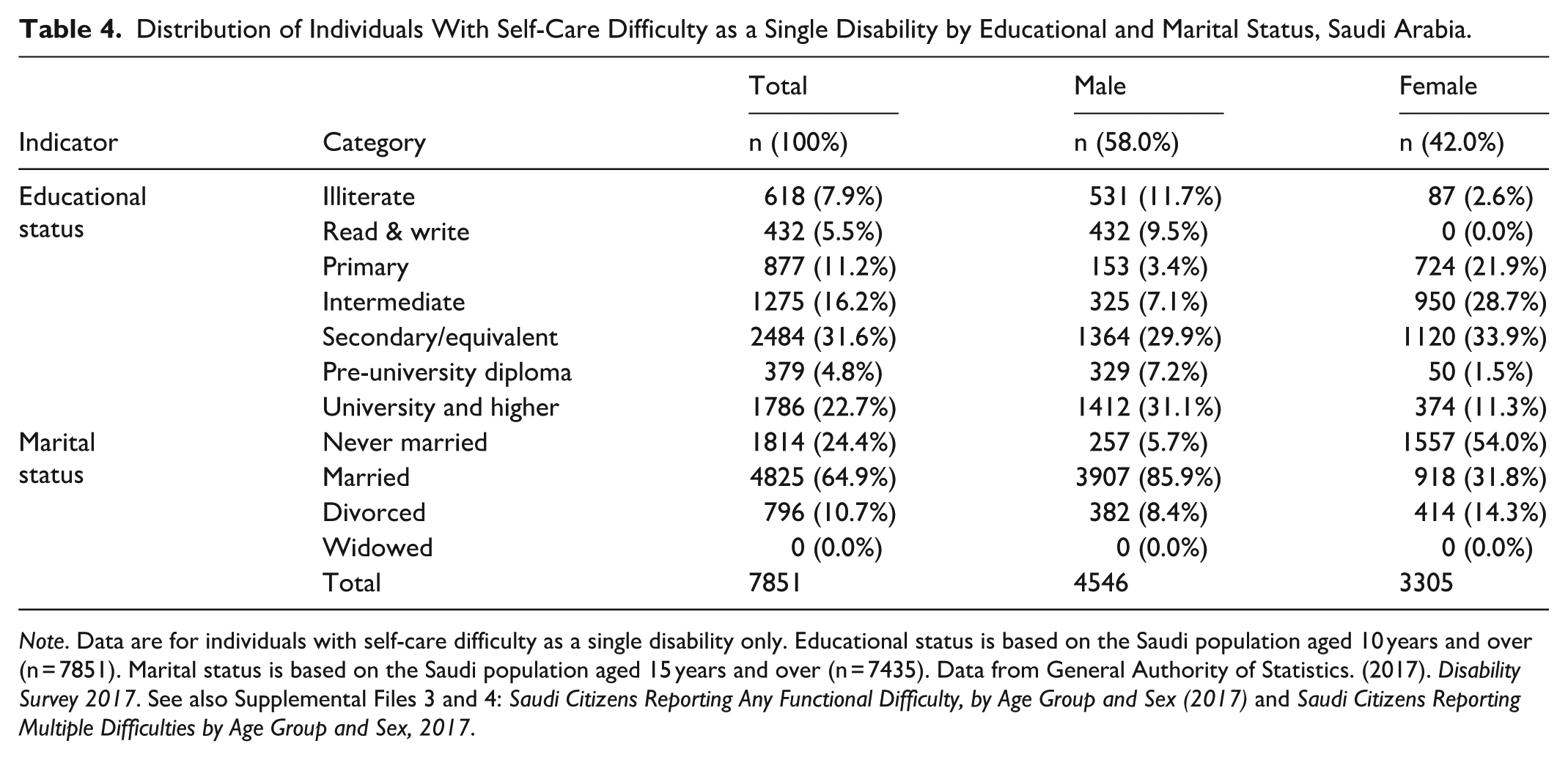
Note. Data are for individuals with self-care difficulty as a single disability only. Educational status is based on the Saudi population aged 10 years and over (n = 7851). Marital status is based on the Saudi population aged 15 years and over (n = 7435). Data from General Authority of Statistics. (2017). Disability Survey 2017. See also Supplemental Files 3 and 4: Saudi Citizens Reporting Any Functional Difficulty, by Age Group and Sex (2017) and Saudi Citizens Reporting Multiple Difficulties by Age Group and Sex, 2017.
Distribution of Saudi Individuals With Self-Care Difficulty Who Receive Services From the Ministry of Labor and Social Development, by Gender.
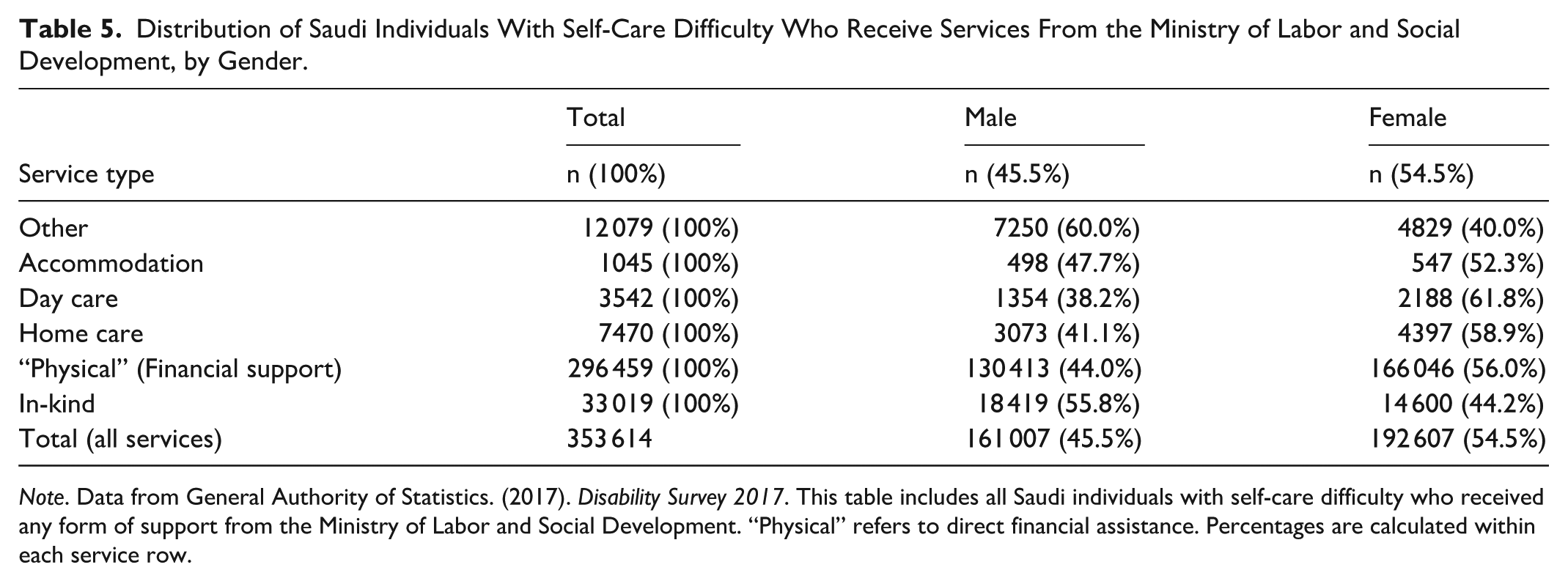
Note. Data from General Authority of Statistics. (2017). Disability Survey 2017. This table includes all Saudi individuals with self-care difficulty who received any form of support from the Ministry of Labor and Social Development. “Physical” refers to direct financial assistance. Percentages are calculated within each service row.
Chi-Square Tests for Sex Differences in Self-Care Difficulty Across 13 Indicators, Saudi Arabia.
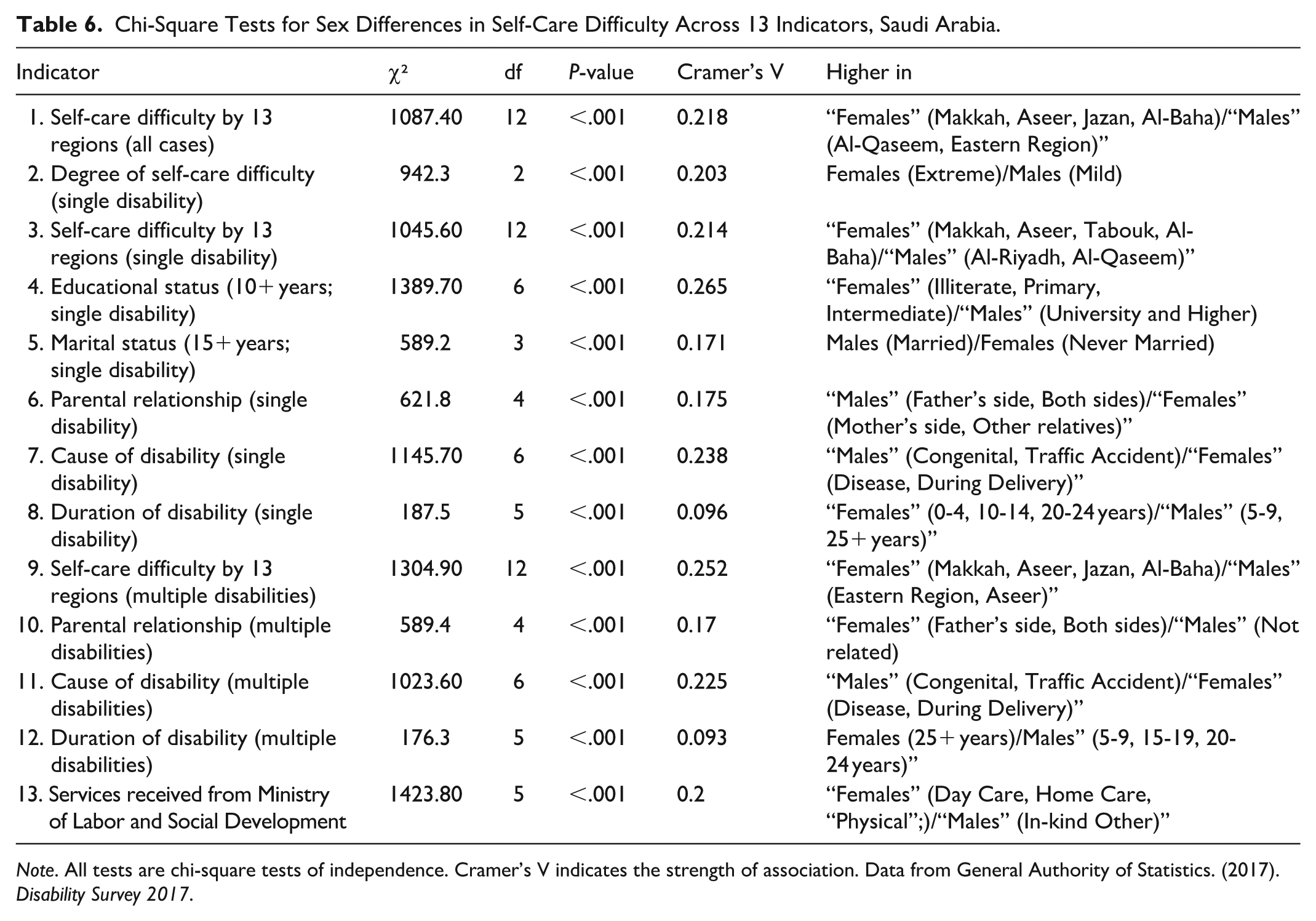
Note. All tests are chi-square tests of independence. Cramer’s V indicates the strength of association. Data from General Authority of Statistics. (2017). Disability Survey 2017.
Multivariable Logistic Regression Analysis of Factors Associated with Self-Care Difficulty in Saudi Arabia.

Note. Model adjusted for all variables listed. Reference categories: Mild, Illiterate, Never Married, Not related, Congenital, 0 to 4 years, No. Data from General Authority of Statistics. (2017). Disability Survey 2017.
As there were no widowed individuals in the sample reporting self-care difficulty, it was not possible to estimate the association between widowhood and self-care difficulty. Additionally, if the number of widowed individuals in the sample is insufficient, the regression model may lack the statistical power required to calculate odds ratios or confidence intervals for this category.
Methods
Design
The present investigation employed a population-based cross-sectional design grounded in secondary analysis of the 2017 Disability Survey. A cross-sectional approach is well suited to estimate the point prevalence of self-care difficulty and to compare affected and unaffected groups across socio-demographic, geographic, and clinical strata because all variables are measured contemporaneously.78,79 The Disability Survey was administered by the Saudi General Authority for Statistics to all Saudi households using a multistage probability strategy, yielding nationally representative data on 20.4 million citizens. Leveraging this single-time-point census frame minimises recall bias, precludes attrition, and facilitates the generation of sex- and region-specific prevalence estimates necessary for public-health surveillance and resource allocation. Although causal inference cannot be drawn, the design is appropriate for identifying high-risk subpopulations and generating hypotheses for longitudinal research.
Because the study analysed an existing governmental database, it constitutes an observational study that conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) recommendations for cross-sectional research (See Supplemental File 1.). 80 Secondary data analysis capitalises on previously collected information, thereby reducing respondent burden, research costs, and time, while allowing investigators to address novel questions that were not the primary focus of the original survey.81,82 Adopting this design also enhanced external validity, as the SNDS employed uniform disability modules derived from the World Health Organization’s Washington Group Short Set, ensuring comparability with international datasets. 83 To uphold methodological rigour, we predefined analytic procedures, documented all deviations from the original sampling plan, and interpreted findings within the recognised constraints of cross-sectional secondary research.
Sample
The parent dataset was generated by the General Authority for Statistics (GASTat) through the 2017 Disability Survey, a nationwide household enquiry that employed a 2-stage, stratified cluster design anchored to the 2010 Population and Housing Census frame. In the first stage, 1344 primary sampling units—statistical areas that are internally homogeneous—were drawn with probability proportional to size within each of the Kingdom’s 13 administrative regions. During the second stage, trained fieldworkers used systematic random procedures to select and interview up to 25 occupied households per unit, yielding 33 575 households that together represented 20.4 million Saudi residents when weighted. Interviews with household heads were completed on tablet computers between 14 April and 18 May 2017, and all responses were calibrated with sampling weights that adjust for unequal selection probabilities, regional non-response, and post-stratification to census controls.84,85 The design follows best practice for large-scale disability surveillance, offering statistically efficient estimates while controlling survey costs. 86
In the official GAStat documentation, the 2017 Disability Survey allocated 1344 primary sampling units (PSUs) across all 13 administrative regions—for example, Makkah (242 PSUs), Riyadh (217), Eastern Region (168), and Al-Bahah (60)—with up to 25 households per PSU (33 575 households total). Interviews were conducted in person with the household head using an electronic (tablet) questionnaire from 17/7/1438 to 22/8/1438 AH (14 April-18 May 2017). The frame included Saudi households nationwide and Saudis temporarily abroad who remained household members, and functional-difficulty modules were administered to persons aged ≥5 years. All analyses applied the provided strata, PSU identifiers, and expansion weights to retain national and region-level representativeness. 84
For the present secondary study, we obtained the anonymised public-use micro-dataset from the GASTat open-data portal and restricted the analytic file to Saudi respondents with complete disability information (N = 20 408 362). Guided by the Washington Group Extended Set, we extracted 13 binary indicators that capture functional limitations linked to self-care. Individuals were classified as having a self-care difficulty when they reported at least “a lot of difficulty” or reliance on help to wash, dress, or perform other personal-care tasks. Case selection and variable coding were performed a priori in Stata/SE 17, and all prevalence estimates were weighted with the GASTat expansion factors to retain national representativeness. Using an open governmental database minimises respondent burden and promotes transparency, yet we adhered to Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidance for cross-sectional studies and its extension Standardized Reporting Of Secondary data Analyses (STROSA) for secondary analyses and documented every data-handling decision to maximise reproducibility.80,83,87
Measures
The primary outcome—self-care difficulty—was drawn from the Washington Group Extended Set (WG-ES) module, which asks adults, “Do you have difficulty with self-care such as washing all over or dressing?” and codes responses on a 4-level scale (no, mild, severe, cannot do at all; See Supplemental File 2). Following WG analytic guidance, we treated any report of at least “a lot of difficulty” or total inability as a positive screen for self-care difficulty, while retaining the original gradations to construct Indicator 1 (regional prevalence and severity) and Indicator 2 (sex-specific prevalence by severity). Eleven additional indicators captured complementary facets of self-care functioning that map onto the International Classification of Functioning, Disability and Health (ICF) domains of body functions, activities, participation, and environmental facilitators (eg, assistive-device use). 88 Specifically, Indicators 3-5 disaggregated self-care difficulty by co-occurring impairments, educational attainment (10 years +), and marital status (15 years +); Indicators 6-8 described familial consanguinity, medically reported causes, and duration of difficulty; Indicators 9-12 repeated these stratifications for respondents reporting multiple functional limitations; and Indicator 13 tabulated the uptake of 5 categories of services from the Ministry of Labour and Social Development.
Three baseline files supplied denominators and covariates for weighting and adjustment. Baseline 1 enumerated the Saudi household population by sex and administrative region, providing post-stratification totals for sex-specific prevalence estimates; Baseline 2 cross-tabulated the same population by 18 five-year age bands (0-84 years) and thereby permitted indirect age standardisation; Baseline 3 summarised regional counts of residents with and without any reported difficulty, ensuring consistency between the analytic sample and national disability totals. All indicators were merged with these baseline tables in Stata/SE 17, recoded as binary or ordinal variables as appropriate, and multiplied by GASTat expansion factors to restore national representativeness. Continuous plausibility and range checks were performed, and coding decisions were logged to meet the Washington Group’s transparency recommendations for secondary data use. 83
Operational definition (GAStat): “Self-care” covers skills and practices of maintaining appearance and health (eg, washing hands/face, brushing teeth, ablution, dressing). We used the SNDS self-care item from the Washington Group—Extended Set on Functioning (WG-ES): Do/does [you/he/she] have difficulty with self-care, such as washing all over or dressing? Would you say: 1 No difficulty, 2 Some difficulty, 3 A lot of difficulty, 4 Cannot do at all.’ We coded self-care difficulty as present for responses “a lot of difficulty” or “cannot do at all.” Other survey covariates (GAStat categories): cause of difficulty (congenital, disease, pregnancy, delivery, traffic accident, other accident, other), duration (0-4, 5-9, 10-14, 15-19, 20-24, 25+ years), and parents’ kinship (first-degree—father’s side, first-degree—mother’s side, both, other relatives, none). For regression, we operationalised consanguinity as any kinship versus none. 84
Procedure
The micro-dataset for the 2017 Disability Survey was obtained in March 2025 from the General Authority for Statistics (GASTat) open-data portal, which distributes all household surveys under a permissive national open-government licence. After downloading the anonymised files, accompanying data dictionary, and the official Methodology and Quality Report (PDF), we imported the records into Stata/SE 17 and linked household, person, and disability modules by their unique identifiers. Consistent with best practice for secondary data management, we screened for structural errors (eg, orphan records, duplicate IDs), out-of-range values, and logical inconsistencies using a 3-step cycle of screen–diagnose–edit. 89 We then restricted the analytic file to Saudi citizens with complete information on the 13 self-care–related indicators and merged the 3 baseline weighting tables described earlier. All data-handling decisions were logged in a reproducible script that accompanied the manuscript submission.
We conducted (1) descriptive statistics (counts, weighted percentages) for all indicators; (2) survey-weighted Pearson’s χ² tests with Cramér’s V to compare self-care difficulty across demographic, geographic, and clinical subgroups; and (3) a survey-weighted multivariable logistic regression estimating adjusted odds of self-care difficulty as a function of region, sociodemographics, severity, cause, duration, chronic disease, and consanguinity (reporting AORs with 95% CIs). No geospatial thematic mapping, principal component analysis, or machine-learning models (eg, random forests, bagging) were used in this study.
Survey data were analysed using the svy suite to adjust for the 2-stage cluster design, including primary sampling units, strata, and weights. Weighted frequencies and 95% confidence intervals described national and sex-specific prevalence; design-based χ² tests, accompanied by Cramer’s V with Cohen’s conventional thresholds, compared distributions across the 13 indicators. To isolate independent correlates of self-care difficulty we fitted multivariable logistic-regression models that included demographic, geographic, and clinical covariates; model fit was assessed with the F-adjusted mean residual test, and multicollinearity was ruled out with variance-inflation factors < 5. Analyses followed contemporary recommendations for complex-survey inference 90 and logistic modelling of binary health outcomes. 91 Because the dataset is released under an open-data licence, 92 contains no direct identifiers, and is already aggregated below the disclosure threshold, the study is exempt from institutional review-board review. The reuse complies with international guidance on ethical secondary analysis of public data and Saudi open-government-data principles, and therefore posed no copyright or confidentiality concerns.93,94
Results
The 2017 Saudi National Disability Survey, which analysed a total population of 20 408 362 Saudis, found that 92.9% (n = 18 962 639) reported no disabilities or functional limitations. Among those who indicated at least one difficulty, 7.1% (n = 1 445 723) were identified as having some form of disability. Notably, 238 984 individuals (1.2%) faced challenges with self-care activities such as bathing, dressing, or toileting, whether as a singular issue or in conjunction with other impairments. Out of this group, 227 609 (1.1%) had multiple disabilities that included self-care difficulties, while 11 375 (0.1%) reported self-care challenges as their only disability. Analysing gender differences, males comprised 7.3% (n = 755 235) of individuals reporting at least one difficulty, while females accounted for 6.9% (n = 690 488). This analysis is focused solely on the Saudi population and excludes 12 143 974 non-Saudi residents for whom data on disabilities were unavailable. The results section offers a thorough examination of self-care difficulties across various dimensions, such as severity, region, education, marital status, consanguinity, causes, duration, and access to social services.
The findings are structured into 7 tables. Table 1 outlines the overall distribution of self-care challenges categorised by severity and region. Tables 2 and 3 provide data on individuals with self-care difficulties, distinguishing between those with a single disability and those with multiple disabilities, while also including breakdowns by region, parental relationship, cause, and duration. Table 4 analyses the distribution of self-care difficulties in relation to educational and marital status for individuals with a single disability. Table 5 investigates the provision of services from the Ministry of Labor and Social Development, shedding light on access to social support and gender-based patterns in service utilisation. Table 6 features chi-square tests assessing sex differences across all 13 indicators, revealing significant disparities. Finally, Table 7 presents the outcomes of a multivariable logistic regression analysis aimed at identifying independent predictors of self-care difficulties, taking into account regional, demographic, and clinical factors.
Table 1 illustrates the distribution of self-care difficulties across Saudi Arabia, including all individuals experiencing this functional limitation, whether independently or in conjunction with other disabilities. The data indicates significant regional disparities, with the highest number of cases reported in Al-Riyadh and Makkah Al-Mokarramah, followed by the Eastern Region, Aseer, and Al-Madinah Al-Monawarah. Mild difficulties were the most commonly reported severity level, accounting for more than half of the total cases, whereas extreme difficulties were the least frequently observed. A notable gender difference is present, with females comprising a slightly larger percentage of cases compared to males, especially in areas like Makkah Al-Mokarramah and Al-Baha. This trend might indicate variations in reporting practices, access to services, or different underlying health conditions.
The profile of individuals with self-care difficulties stemming from a single disability is detailed across essential demographic and clinical areas (Table 2). Mild difficulties were the most frequently reported severity level, particularly among males, while extreme difficulties, though less common, still represented a significant portion. A regional analysis showed a high concentration of cases in Al-Riyadh and Makkah Al-Mokarramah, with notable gender disparities—females were more prevalent in areas like Aseer and Al-Baha, whereas males were more prominent in Al-Qaseem and Al-Jouf. Consanguinity played a significant role, especially in first-degree relationships on the paternal side, which were more prevalent among males. Disease emerged as the primary cause of disability, followed by congenital issues and traffic-related incidents; males were more likely to report accidents, while females tended to report congenital or delivery-related disabilities. Most individuals had lived with their disabilities for over 25 years, suggesting that these conditions often begin early and persist over time.
Table 3 outlines the characteristics of individuals experiencing self-care difficulties as part of multiple disabilities across important demographic and clinical areas. Mild difficulty was the most frequently reported severity level, followed by severe and extreme difficulties. There was a notable regional concentration in Al-Riyadh and Makkah Al-Mokarramah, with females being predominantly represented in most areas, especially in Al-Baha and Najran. Consanguinity emerged as a significant factor, particularly among males, where first-degree relationships on both maternal and paternal sides were common. Notably, disease was identified as the primary cause of disability, revealing a significant gender gap: females were more than twice as likely to report disease-related disabilities compared to males. Additionally, the majority of individuals had lived with their disabilities for over 25 years, suggesting that these conditions often begin early in life and persist over time.
Table 4 presents the distribution of individuals facing self-care difficulties as a single disability, categorised by educational background and marital status. A notable gender imbalance is apparent: males are disproportionately represented among university graduates, while females are more likely to have only completed primary or intermediate education. Additionally, illiteracy and the ability to “Read & Write” are more prevalent among males, while females demonstrate higher levels of primary and intermediate education. In terms of marital status, a significant number of females fall into the never-married category, indicating potential delays in marriage or social obstacles, whereas males tend to be predominantly married, aligning with traditional family norms. No individuals were reported as widowed, which may be attributed to underreporting or the presence of protective social structures.
Table 5 illustrates the distribution of services provided by the Ministry of Labor and Social Development to individuals experiencing self-care difficulties, broken down by gender. A significant majority of the services were financial (“Physical”), with females receiving a higher percentage (56.0%) compared to males (44.0%). Furthermore, females were more likely to benefit from home care (58.9%) and day care (61.8%), while males tended to receive more in-kind and unspecified services. Accommodation services were relatively evenly distributed between the genders. These results indicate that women with self-care difficulties are more inclined to utilise institutional and home-based support, potentially reflecting greater caregiving responsibilities or higher levels of social vulnerability. Conversely, men appear to depend more on direct financial assistance.
The chi-square tests presented in Table 6 indicate significant differences between genders concerning the distribution of self-care difficulties across all 13 indicators (P < .001), highlighting gender as a key factor in the epidemiological landscape of this condition. The most substantial effect sizes were seen in educational attainment (Cramer’s V = 0.265) and services accessed (V = 0.200), pointing to significant disparities. Women were more likely to be illiterate, possess only primary or intermediate education, and experience severe difficulties, while men were disproportionately represented among university graduates and those reporting mild difficulties. Regarding marital status, men were primarily married, whereas women predominantly reported never being married, indicating potential delays in marriage or social exclusion. Women were also more likely to receive home care, day care, and financial assistance, which reflects increased dependency or caregiver burden, whereas men received more in-kind and unspecified support. Disease and delivery-related causes were more frequently attributed to women, while congenital issues and traffic accidents were more common among men. Additionally, a long duration of self-care difficulties (25+ years) was notably associated with women in both single and multiple disability categories, suggesting early onset and lasting consequences.
The multivariable logistic regression analysis presented in Table 7 indicates that difficulties in self-care are significantly linked to various demographic, geographic, and clinical factors. Individuals residing in high-prevalence areas like Aseer and Hail experience almost twice the likelihood of facing self-care challenges, even when other variables are taken into account, pointing to possible disparities related to genetics, environment, or healthcare access. Among the strongest predictors are disease and delivery-related factors, with disease particularly correlated to self-care difficulties, likely due to the impact of chronic illnesses such as diabetes, arthritis, and stroke. A prolonged duration of disability (over 25 years) considerably raises the odds, suggesting that early onset has a lifelong effect. Consanguinity, particularly among first-degree relatives, is a notable risk factor, which aligns with the genetic influences on developmental and neurological issues. Interestingly, higher educational attainment correlates with an increased likelihood of self-care difficulties, which may indicate improved detection, reporting, or access to services rather than a higher prevalence. The significant association with assistance from the Ministry of Labor and Social Development (AOR = 1.84) highlights the connection between functional impairments and the need for social support.
Discussion
National self-care difficulty is modest in prevalence yet large in absolute burden; most cases occur with co-occurring limitations, and regional differences persist after adjustment. Clinically, greater severity, longer duration, and disease- or delivery-related causes are strongly associated with difficulty, consistent with international evidence on ADL progression and chronicity. Socially, patterns are gendered (including differential service uptake), consanguinity remains an independent correlate, and an apparent education gradient likely reflects detection, survival, or urban-service factors rather than a causal effect.
Our national prevalence estimate is considerably lower than the 3.3% overall disability rate reported in the 2016 Demographic Survey, confirming that personal-care impairment represents a subset of the broader disability burden. 62 Even so, the absolute number of affected individuals is comparable to the entire Saudi population aged 85 years and older, underscoring the public-health relevance. The concentration of cases in Riyadh and Makkah echoes earlier evidence that health-service density and diagnostic capacity are greatest in those provinces, 66 yet the elevated adjusted odds in ʿAsīr and Ḥāʾil align with spatial analyses linking high disability rates to mountainous terrain, transport barriers, and entrenched consanguinity. 72 Internationally, long-standing functional loss is known to erode compensatory capacity and raise care needs 30 ; our finding that odds quadrupled after 2 decades’ duration reproduces that dose–response in the Saudi context. Recent evidence also shows dynamic transitions among ADL states and reinforces the bidirectional links between frailty and ADL disability, aligning with our chronicity findings.95,96
Sex-specific patterns deserve particular attention. Women’s dominance among multi-disability cases and their higher uptake of formal services mirror Saudi continence studies in which women bore the greater symptomatic burden yet seldom sought medical help until limitations compounded. 63 Once dependency rises, however, cultural expectations that daughters and female relatives provide intimate care may make women more visible to the welfare system, explaining their higher receipt of day- and home-care benefits. 47 Conversely, men’s over-representation among university graduates with mild difficulty may reflect detection bias: highly educated men may recognise minor deficits earlier or feel less stigma in reporting them, a pattern noted in European ageing cohorts. 31
Consanguinity remained a robust correlate of self-care difficulty after adjustment. Contemporary Saudi studies continue to report high consanguinity exposure and variable awareness of genetic risk—underscoring the value of premarital screening and counselling.97 -99 This synergy between genetic susceptibility and environmental exposures reinforces calls for premarital counselling and carrier-screening programmes. Disease-related and delivery-related aetiologies together accounted for more than half of all cases, dovetailing with national surveillance attributing 39% of Saudi disabilities to chronic conditions and highlighting obstetric complications in peripheral hospitals. 65
The apparently paradoxical association between higher education and self-care difficulty is consistent with the “survivor” hypothesis: individuals with greater educational resources often live longer with chronic illness, reaching ages at which self-care difficulty becomes more likely. 30 In Saudi Arabia, tertiary education is concentrated in large cities; thus, the education effect may partially capture urban residence and better diagnosis rather than causal influence per se. Service-use differences reflect both cultural norms and supply-side factors. Female preference for facility-based assistance accords with qualitative reports that Saudi women shoulder disproportionate caregiving loads and seek formal respite when available, 61 while men’s greater receipt of in-kind benefits aligns with workforce studies showing male preference for material over relational support. 51
Finally, our findings intersect with the capacity of direct-care systems: current reports document persistent shortages and turnover among home- and community-based workers, with wage and retention pressures constraining delivery of personal-care supports—pressures that can widen regional and gender inequities.100 -102 Architectural audits of medical facilities reveal poor compliance with accessibility standards, 70 and qualitative accounts from home-care aides highlight the emotional labour of preserving dignity during intimate tasks. 52 By quantifying the magnitude, geography, and multilevel predictors of self-care difficulty, the current study extends previous Saudi research beyond single-site clinical samples and sets the empirical stage for future work on targeted rehabilitation and equitable resource allocation. Our interpretation also accords with updated population studies reporting recent shifts in disability and limitation patterns across adulthood, complementing earlier cohorts. 103
Limitations and Strengths
This analysis benefits from a nationally representative sampling frame, a large denominator that permits stable sex- and region-specific estimates, and the use of 13 indicators that capture both clinical and social dimensions of self-care. Nonetheless several caveats warrant mention. First, the cross-sectional design precludes causal inference and leaves uncertain whether consanguinity, chronic disease, or social position precede—or result from—self-care difficulty. 79 Second, self-care was self-reported by household informants; misclassification is possible because proxy respondents may under- or over-state mild deficits, and the survey excluded expatriate residents who constitute one-third of the Kingdom’s population. Third, our threshold (“a lot of difficulty” or “cannot do”) omits individuals with moderate problems who may still require preventive support, potentially under-estimating need. Fourth, covariates such as income, home modifications, and caregiver availability were unavailable, limiting contextual explanation. Finally, the dataset dates to 2017; although the most recent national source, service coverage has since expanded under Vision 2030, so prevalence may have shifted. Adherence to STROBE guidelines, transparent weighting, and sensitivity checks mitigate but do not eliminate these limitations. 80
Policy Implications
Findings point to a number of priority arenas for Saudi disability policy. First, regional equity: elevated odds in ʿAsīr and Ḥāʾil underscore the need to accelerate Vision 2030s primary-care roll-out and to extend the emerging national accessibility code beyond Riyadh and Makkah. 66 Second, gender-responsive programming: women’s heavier reliance on day- and home-care services suggests that respite entitlements, continence clinics, and caregiver stipends should be scaled with explicit female uptake targets, while men’s preference for material benefits could be met through adaptive-device vouchers. Third, risk modification: the independent effect of close-kin marriage and long-term disease argues for integrating premarital genetic counselling, chronic-disease self-management education, and early functional-screening into family-health centres.62,63 Workforce Saudization plans should embed competency-based training in intimate care and culturally sensitive communication, 67 and hospital-licencing audits must enforce toilet, ramp, and signage standards already mandated by the 2023 Disability Rights Law. 69 Collectively, these measures can shift Saudi personal-care provision from reactive welfare to proactive, rights-based rehabilitation. Further, the concentration of cases within major urban centres may point to possible correlations with population density, healthcare availability, or environmental factors, which warrant further investigation in future research.
Conclusion
Self-care difficulty affects about 1.2% of Saudi citizens, with disproportionate burden among women, peripheral provinces, and long-duration/severe cases driven by clinical and contextual factors. To translate these findings into practice—without repeating our detailed Policy Implications—we underscore 3 priorities: equity-focused scale-up of rehabilitation and day/home-care capacity, integration of premarital genetic counselling and chronic-disease self-management, and routine national monitoring of ADL limitations to track progress under Vision 2030.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251382005 – Supplemental material for Epidemiology and Factors Associated With Self-Care Difficulty in a National Saudi Sample: A Retrospective Study
Supplemental material, sj-docx-1-inq-10.1177_00469580251382005 for Epidemiology and Factors Associated With Self-Care Difficulty in a National Saudi Sample: A Retrospective Study by Ahmed Alduais, Hind Alfadda and Hessah Saad Alarifi in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-3-inq-10.1177_00469580251382005 – Supplemental material for Epidemiology and Factors Associated With Self-Care Difficulty in a National Saudi Sample: A Retrospective Study
Supplemental material, sj-docx-3-inq-10.1177_00469580251382005 for Epidemiology and Factors Associated With Self-Care Difficulty in a National Saudi Sample: A Retrospective Study by Ahmed Alduais, Hind Alfadda and Hessah Saad Alarifi in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-4-inq-10.1177_00469580251382005 – Supplemental material for Epidemiology and Factors Associated With Self-Care Difficulty in a National Saudi Sample: A Retrospective Study
Supplemental material, sj-docx-4-inq-10.1177_00469580251382005 for Epidemiology and Factors Associated With Self-Care Difficulty in a National Saudi Sample: A Retrospective Study by Ahmed Alduais, Hind Alfadda and Hessah Saad Alarifi in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-2-inq-10.1177_00469580251382005 – Supplemental material for Epidemiology and Factors Associated With Self-Care Difficulty in a National Saudi Sample: A Retrospective Study
Supplemental material, sj-pdf-2-inq-10.1177_00469580251382005 for Epidemiology and Factors Associated With Self-Care Difficulty in a National Saudi Sample: A Retrospective Study by Ahmed Alduais, Hind Alfadda and Hessah Saad Alarifi in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors would like to acknowledge the financial support from the ongoing research funding programme (ORF- 2025-251) King Saud University, Riyadh, Saudi Arabia.
Ethical Considerations
This research did not require an IRB approval.
Consent to Participate
Neither human nor non-human subjects were involved directly in this research. Therefore, an informed consent was not required.
Author Contributions
Conceptualisation, A.A.; Data curation, A.A.; Formal analysis, A.A.; Funding acquisition, H.S.A. and H.A.; Investigation, A.A., H.S.A. and H.A.; Methodology, A.A.; Project administration, H.S.A. and H.A.; Resources, A.A.; Software, A.A.; Supervision, H.S.A. and H.A.; Validation, A.A.; Visualisation, A.A.; Writing—original draft, A.A., H.S.A. and H.A.; Writing—review & editing, A.A., H.S.A. and H.A. All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded by King Saud University, Riyadh, Saudi Arabia, under the research project (ORF- 2025-251).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available in General Authority for Statistics, Saudi Arabia at https://www.stats.gov.sa/en/home. These data were derived from the following resources available in the public domain: - Social Statistics, ![]() .
.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.