
Abstract
This study explores how undergraduate health care students in Taiwan observe others’ needs and what factors influence their prosocial behavior in the context of priority seating. Using a qualitative descriptive design with thematic content analysis, structured open-ended questionnaires were distributed to 146 students from 3 health-related departments at a college in Taiwan. Thematic content analysis was conducted based on a pre-defined coding framework. Participants’ reasoning reflected both normative categories (eg, older adults, pregnant women) and situational judgments based on observed needs (eg, signs of fatigue or injury). Voluntary seat-offering was the most common behavior and was strongly associated with internalized personal values. Decisions were also shaped by the perceived demeanor of the person in need. Visual cross-theme analyses highlighted how these factors interacted in cases involving older adults and people with mobility impairments. Health care students’ decisions to offer their seat were influenced by a mix of internal moral orientations, interpersonal cues, and context sensitivity. While cultural norms may inform reasoning, students actively negotiated social expectations with personal judgment. These findings suggest a need for further educational attention to everyday moral decision-making in the development of professional identity.
Keywords
● Healthcare students’ value formation often occurs in informal, everyday situations outside structured clinical training.
● Priority seating in public transportation presents morally relevant scenarios requiring interpretation of others’ needs and prosocial decision-making.
● Limited research exists on how healthcare students respond to ambiguous signs of need in routine public spaces, especially in East Asian cultural contexts.
● Healthcare students in Taiwan use both categorical thinking (older adults, pregnant women) and situational empathy (mobility impairments, illness signs) to determine priority seating eligibility.
● Personal values primarily drive seat-offering behavior (67.6%), while recipient demeanor significantly influences decisions (26.7%).
● Students show strong moral responsiveness to visible needs, but interpersonal dynamics and emotional responses mediate their prosocial actions.
● Healthcare education should integrate moral reasoning exercises addressing everyday ethical decisions to strengthen professional identity development.
● Clinical training must prepare students to maintain empathy with difficult patients, recognizing that moral behavior involves complex interpersonal dynamics beyond perceived need.
● Educators should develop adaptive moral reasoning through problem-based learning involving competing values and situational judgments applicable to clinical practice.
Background
Health care professionals are expected not only to possess clinical expertise but also to demonstrate a high degree of social sensitivity and interpersonal awareness.1 -3 As future members of a caregiving workforce, health care students must cultivate the ability to perceive others’ needs, 4 interpret social cues, and respond with empathy and appropriateness5,6 in both clinical and everyday settings. The cultivation of such soft skills is increasingly recognized as a vital component of professional formation, complementing the acquisition of medical and technical knowledge.
In the context of health care education, efforts to strengthen students’ ethical reasoning, moral sensitivity, and prosocial orientation are often implemented through formal coursework 7 or clinical training. 8 However, much of students’ value formation may also occur in informal, everyday situations 9 where they encounter social expectations 10 and ethical dilemmas 11 outside of structured learning environments. These ordinary encounters provide insight into how students translate abstract professional ideals into concrete behavior. The social dynamics observed in public transportation settings can be understood through the lens of dramaturgical sociology, particularly Goffman’s concept of “presentation of self in everyday life.”12,13 In these public spaces, individuals engage in social performances where their actions are subject to observation and judgment by others. The decision to offer or withhold a seat becomes a form of “impression management” where healthcare students must navigate between personal comfort, social expectations, and professional identity presentation.14,15 This dramaturgical framework helps explain why participants in our study were particularly attentive to the “audience” of fellow passengers and the social consequences of their behavioral choices in these highly visible public settings.
Previous research has examined helping behavior (eg, Refs.16,17) and some studies have focused on emergency situations 18 or explicit requests for assistance. 19 Less is known about how individuals, especially those in health-related disciplines, respond to ambiguous or indirect signs of need in routine public spaces. This question takes on added cultural significance in East Asian societies, where Confucian values emphasizing respect for older adults, social harmony, and role-based obligations may shape individuals’ interpretations of others’ needs and their own sense of duty.20,21 Understanding how health care students make sense of such situations can provide a valuable window into their developing professional identity and social responsiveness.
This study addresses this gap by qualitatively exploring health care students’ real-life experiences of noticing and responding to others’ needs in everyday public settings. As a case example, it uses the context of priority seating—a designated section in public transportation where certain seats are marked to be given up for individuals with specific needs, 22 such as older adults 23 or people with disabilities. 24 These designated seats are commonly seen in public transportation systems in East Asian 22 and European 25 cities, where signs or symbols encourage passengers to give up their seats for those in greater need. This study analyzes how students interpret others’ needs in these settings and what factors motivate or inhibit their seat-offering behavior. Through open-ended questionnaires, the research seeks to understand how future health professionals behave when confronted with subtle social cues in morally relevant yet non-clinical situations.
Method
Design and Participants
This study employed a qualitative descriptive design using a structured paper-based questionnaire with open-ended questions. Purposive sampling was employed in this study to investigate the perspectives of healthcare professional students. The objective was to explore healthcare students’ observations and behavioral motivations in priority seating scenarios. A total of 146 undergraduate students were recruited from 3 health-related departments at a college in Taiwan: Nursing (n = 49), Medical and Health Sciences (n = 45), and Optometry (n = 52). Participants were aged between 18 and 19 years, with 28 participants (19.2%) identifying as male and 118 participants (80.8%) identifying as female. Students who were unfamiliar with the concept of priority seating or who had never encountered or used it in real-life contexts were excluded from the study.
Procedures
Data were collected using a structured, open-ended questionnaire administered in paper format. Each participant completed the questionnaire within approximately 15 min in a classroom setting. The structured, open-ended questionnaire used in this study was developed specifically for this research. The questionnaire consisted of 2 main questions designed to elicit detailed responses about participants’ experiences with priority seating. Given the exploratory nature of this qualitative descriptive study and the specific cultural context of priority seating in Taiwan, we developed original questions to capture participants’ authentic experiences and perspectives. The questionnaire included 2 main questions: (1) “Please describe your view on priority seating in public facilities (eg, public transportation, government agencies, or hospitals),” and (2) “Please describe in as much detail as possible your most memorable experience related to priority seating.” Participants’ responses were transcribed verbatim for analysis. The study was conducted in March, 2025, and all participants provided written informed consent prior to participation. This study followed the Consolidated criteria for reporting qualitative research (COREQ) guidelines to ensure comprehensive and transparent reporting of our qualitative research methodology and findings. 26
Data Analysis
A content analysis approach was employed using deductive coding with pre-defined categorical frameworks based on research questions and literature review. The content analysis process involved multiple systematic coding techniques following established methodological guidelines27,28:
1) Coding scheme construction: Pre-defined coding categories were established based on literature review and refined through pilot coding with sample responses to clarify meanings and adjust subcategories as needed.
2) Open coding: Each transcript was systematically reviewed to identify all segments related to our 3 main themes. Mechanically, this involved reading each participant response in its entirety and marking any text that addressed: (a) perceptions of appropriate priority seat users, (b) seat-offering behaviors, or (c) reasoning behind decisions.
3) Categorical coding: Identified segments were then assigned to specific subcategories within our pre-defined framework (see Table 1). For example, mentions of “older people” were coded under “Specific groups,” while descriptions of “someone looking tired” were coded under “Observation and empathy for needs of others.”
4) Multiple coding: Rather than exclusive coding, each response segment could receive multiple codes when participants mentioned several concepts within the same theme, with each theme coded at most once per participant response.
5) Exhaustive coding: All transcripts were re-examined multiple times for each coding theme to ensure comprehensive capture of relevant content, with coders working independently before comparing and discussing results.
Coding Schema for the Current Study.

Coding was conducted independently by the first author and a second trained coder. Prior to the formal coding process, inter-coder reliability was assessed using Cohen’s Kappa, yielding a value of .89. All internal consistency coefficients for the coding categories exceeded .80, indicating high reliability. 29 Coding discrepancies were discussed and resolved through consensus. The purpose of the analysis was to comprehensively capture and categorize participants’ representations and reasoning related to the use of priority seating, and to transform qualitative observations into structured and interpretable data patterns. The coding scheme table is shown in Table 1.
Results
The following findings are organized by coding themes and categories, as summarized in Table 2.
Coding Results of the Current Study.

Theme 1: Types of Individuals Perceived to Be (or Not) Appropriate Users of Priority Seating
Participants’ perceptions of who should be granted priority seating revealed 2 major coding categories: specific groups and observation and empathy for the needs of others, comprising 48.3% and 51.7% of the total 774 coded instances, respectively. Within the “specific groups” category (n = 374), the most frequently cited appropriate recipients of priority seating were older adults (n = 123), followed by pregnant women (n = 92), children (n = 36), young people (n = 17), and people with disabilities (n = 16). These responses suggest that many participants relied on conventional, socially recognized markers of vulnerability or deservingness to determine whether someone was eligible for a priority seat. Interestingly, while pregnant women were frequently cited as appropriate priority seat users (n = 92), several participants also mentioned mothers with children (n = 3) as deserving consideration. This pattern suggests that some participants implicitly associated seating needs with female caregiving roles, potentially reflecting lingering traditional gender expectations in Taiwanese society where childcare responsibilities might be viewed as primarily maternal duties.
In contrast, the “observation and empathy for the needs of others” category (n = 400) reflected a more situational and dynamic approach to need recognition. Participants frequently mentioned giving up a seat for individuals with mobility impairments (n = 70), people feeling unwell (n = 51), or those with visible injuries (n = 25). Interestingly, a smaller subset of responses (n = 13) referred to people who behave impolitely, which often served as a justification for not offering a seat. This suggests that participants’ seat-offering behavior was influenced not only by perceived need but also by moral judgments about the other person’s demeanor. No responses were coded as “unable to be categorized” in this theme, indicating that all statements could be reasonably classified into the 2 established categories.
Theme 2: Whether Participants Chose to Offer Their Seat in a Recalled Situation
When describing their past experiences with offering seats, participants were categorized into 3 behavioral groups: voluntarily offering a seat, reactively offering a seat, and not offering a seat. Among the 774 total coded instances, this theme accounted for 774 codes as well, reflecting multiple mentions of seat-offering behaviors across different recalled situations. The majority of responses (n = 481, 62.1%) indicated that participants had voluntarily offered a seat, often without being prompted or requested. Many described a strong sense of internal responsibility or habitual moral action. One participant noted,
I saw an elderly man get on the bus, and before he even looked around, I stood up and told him he could sit here.
Others emphasized quick, instinctive responses:
It just felt natural—I didn’t even think twice.
A smaller portion (n = 56, 7.2%) described instances where participants offered a seat reactively, usually in response to external cues, social pressure, or non-verbal requests. In some cases, participants reported feeling influenced by the public setting itself:
It was on the MRT, and since it’s a public space, I felt like whatever I did was visible to everyone. I didn’t want to come across as rude, so I stood up.
In other cases, non-verbal communication from the potential seat recipient played a role:
An older man stared at me with a clearly displeased look. I felt awkward and stood up to avoid conflict.
These accounts suggest that reactive seat-offering behavior is not always driven by internal motivation, but rather by situational cues and concern for social impression or tension.
Notably, nearly one-third of responses (n = 237, 30.6%) described situations in which participants did not offer their seat. The motivations behind inaction were varied and are further elaborated in Theme 3. Some participants cited personal discomfort:
Honestly, I was really tired and just didn’t have the energy to stand that day.
Others justified the decision based on perceptions of the other person:
He looked fine to me, not like someone who needed help.
Together, these findings illustrate the range of behavioral responses students reported, and suggest that seat-offering behavior is shaped not only by internalized norms, but also by dynamic social cues and personal judgment.
Theme 3: The Reasons Behind Participants’ Decisions
Participants’ explanations for their seat-offering decisions were coded into 6 categories. The majority (n = 523, 67.6%) referenced personal values as the core driver of their actions. Many described internalized beliefs about kindness, responsibility, or doing the “right thing.” For example, participants stated,
I just naturally feel it’s my duty to give up my seat. To me, it’s just something you ought to do. I don’t even think twice about it.
The second most frequent category was behavior and attitude of the requester or observed person (n = 207, 26.7%). Participants often referred to whether the other person seemed polite, disruptive, or emotionally aggressive. One participant wrote,
There was a kid jumping around and yelling loudly the whole time. I didn’t feel like offering my seat at all.
Another described a more confrontational encounter:
An elderly man asked for the seat but immediately started scolding me, saying I was disrespectful. That really put me off.
Environmental factors (n = 20, 2.6%) were also mentioned, such as vehicle crowding, seat location, or ride conditions. For instance:
It was too hard to move around in the crowded bus, so I didn’t even try.
A few participants cited their own physical or mental condition (n = 18, 2.3%) as a reason for not offering a seat, including pain, fatigue, or stress. Very few responses fell under social factors (n = 5, 0.6%). Last, only 1 instance (0.1%) was marked as unclassifiable or ambiguous. These findings reveal that while many students were guided by internal moral frameworks, their decisions were often shaped by a complex mix of situational cues, perceptions of the other person, and their own physical state.
Cross-Theme Analysis: Seat-Offering Behaviors and Motivations Toward Older Adults
As shown in the results of Theme 1, older adults were the most frequently mentioned group in the specific groups category, with 123 references out of 374 coding instances. Given their prominent representation, a cross-theme analysis was conducted to further examine how participants described their seat-offering behavior and underlying motivations in situations involving older adults. This analysis integrates data across 3 major coding themes: recognition of others’ needs, behavioral responses, and reasons for action or inaction. The interrelations among these categories are visually summarized in Figure 1.
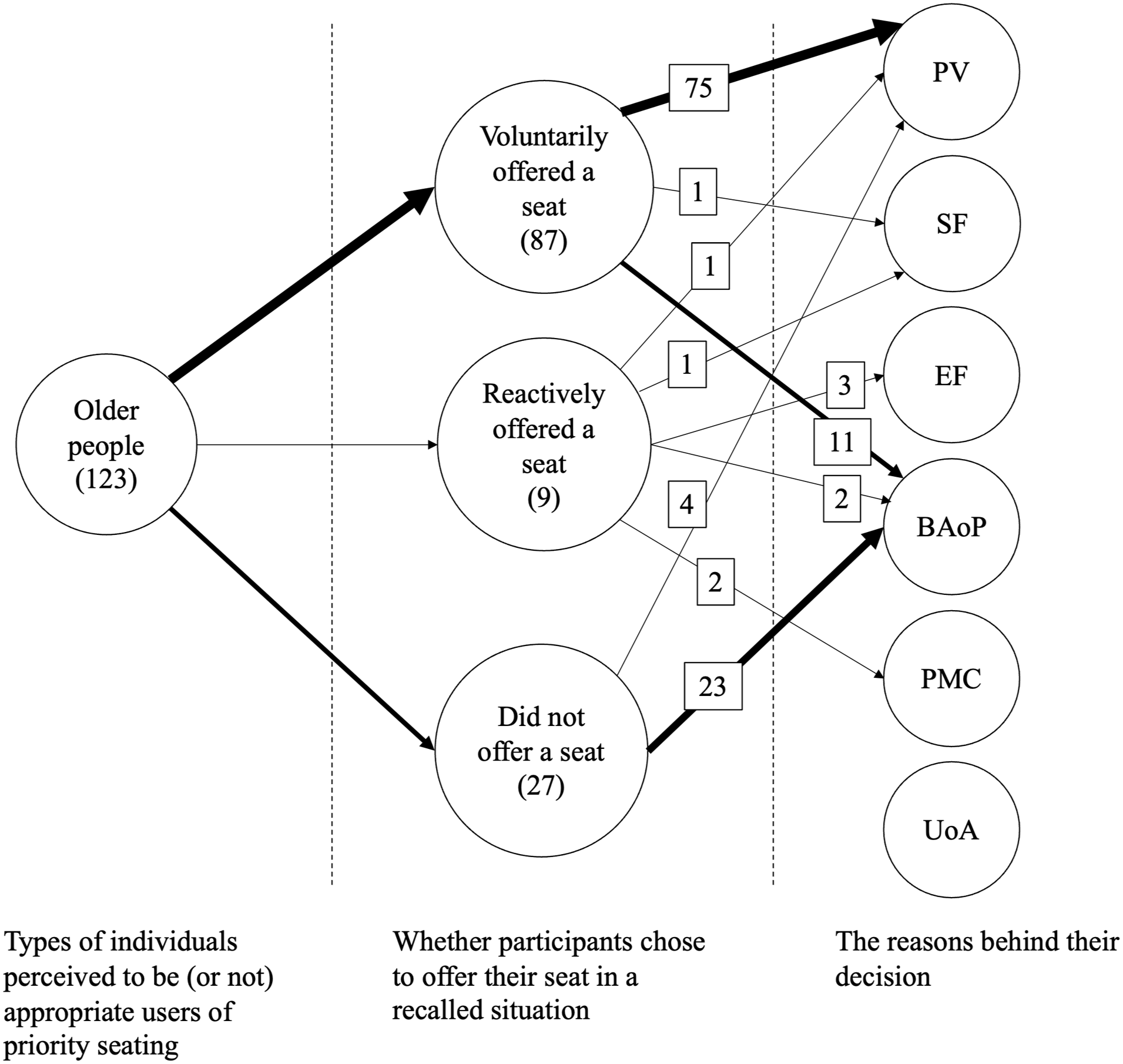
Visual mapping of coded relationships among factors influencing seat-offering decisions toward older adults.
Among the 75 instances coded as involving older adults, the majority were associated with actual seat-offering behavior, either voluntarily or reactively. Participants frequently cited personal values (PV)—such as respect for elders, moral obligation, or ingrained cultural norms—as a key reason for giving up their seat. One participant noted,
It’s automatic for me to stand up when I see older people.
However, not all responses reflected positive interactions. Several participants described negative emotional responses stemming from how older adults behaved when requesting a seat. These were commonly coded under Behavior and attitude of the requester or observed person (BAoP). One participant shared,
An elderly man didn’t ask politely—he just glared at me and pointed at the seat. It made me uncomfortable, so I pretended not to notice.
In a smaller number of cases, participants mentioned environmental factors (EF) or their own physical or mental condition (PMC) as reasons for inaction. Last, mentions of social factors (SF) were rare in these contexts, suggesting that peer or public pressure played a lesser role when older adults were involved. Only 1 response was categorized as unclassifiable or ambiguous (UoA). This analysis highlights how participants’ decisions regarding older adults are shaped by the interplay of perceived need, personal norms, and social interactions. While many students described a strong sense of internalized responsibility, others emphasized the emotional complexity of encounters involving older passengers, especially when those interactions included judgment, tension, or discomfort.
Cross-Theme Analysis: Seat-Offering Behaviors and Motivations Toward People With Mobility Impairments
As indicated in the results of Theme 1, people with mobility impairments were the most frequently mentioned group under the subcategory Observation and empathy for the needs of others, with 70 instances out of 400. To explore how participants responded to such observations, a cross-theme analysis was conducted to examine the associated behavioral decisions and underlying motivations. The relationships among these coding categories are visualized in Figure 2.

Visual mapping of coded relationships among factors influencing seat-offering decisions toward people with mobility impairments.
Among the responses in which participants referred to individuals with mobility impairments—such as those using canes, walkers, or showing visible difficulty walking—voluntary seat offering was the most common behavioral outcome. These actions were strongly associated with personal values (PV), with 57 co-occurrences, indicating that participants often described such decisions as driven by internalized beliefs about care, respect, or moral responsibility. For example, 1 participant stated,
When I saw someone struggling to walk, I didn’t hesitate. It just felt like the right thing to do.
A small number of participants referred to behavioral or verbal cues from the person in need (BAoP), especially when individuals communicated their limitations explicitly. These instances reflected how participants relied not only on observation, but also on clear interpersonal interaction. For example:
She told me she couldn’t stand for long because of her leg condition, so I immediately gave her my seat.
Mentions of participant’s own physical condition (PMC), environmental factors (EF) and social factors (SF) were rare, suggesting that actions taken in these contexts were primarily shaped by empathetic observation and personal moral frameworks, rather than external pressure or physical limitations. This analysis underscores the role of perceived physical vulnerability in prompting action. When mobility difficulties were visible and unambiguous, participants tended to rely on moral intuition rather than social expectation, and described their decision-making as swift and unquestioned.
Discussion
This study explored how health care students in Taiwan observe and respond to others’ needs in public settings, using the context of priority seating as a case example. The findings shed light on the values, perceptions, and situational reasoning that guide students’ prosocial behavior in non-clinical environments. Figures 1 and 2 further illustrate how these behaviors and motivations are interrelated in specific types of seat-offering situations. A key finding is that participants relied on both categorical thinking and situational empathy when determining whether someone was eligible for a priority seat. While many students referred to socially recognized categories (eg, older adults, pregnant women) as appropriate users, others highlighted the importance of observing physical cues, such as signs of illness or difficulty standing. This distinction reflects the coexistence of normative knowledge and context-sensitive reasoning in participants’ everyday moral decision-making.
The prominence of personal values as a motivating factor supports previous literature emphasizing moral sensitivity30,31 and internalized prosocial norms 32 among health professions students. In particular, voluntary seat-offering was the most frequently described behavior, often expressed as an instinctive or automatic action. These findings suggest that many participants view seat-offering not as a deliberative process, but as an extension of their personal and professional identity. This supports arguments from professional ethics education that stress the integration of moral habits into everyday conduct.33,34 Figure 2, which focuses on contexts where participants voluntarily offered their seats, illustrates the central role of personal values in driving action, particularly when needs are clearly recognized.
At the same time, results of the current study reveal important nuances. For example, some participants withheld seat-offering when perceiving negative attitudes from potential recipients, such as entitlement or rudeness. This underscores that moral behavior is not only shaped by perceived need but also mediated by interpersonal dynamics 35 and emotional responses. 36 In contrast to the lower frequencies of coding related to social or physical constraints, categories such as personal values and perceptions of the recipient’s behavior were more dominant in shaping participants’ decisions. The prominence of these factors—particularly evident in Figures 1 and 2—suggests that health care students’ actions might be driven less by external circumstances and more by internalized norms and interpersonal judgments. This finding emphasizes the salience of moral identity and relational interpretation over generalized environmental or social influences. Notably, participants were more likely to act when the need appeared unambiguous and observable, as in cases involving people with visible mobility impairments. In such situations, personal values were activated with little hesitation. This pattern echoes theories of moral salience, where the clarity of need might directly influences moral responsiveness. 37
Figure 1, which focuses on situations involving older adults, highlights how both personal values and the behavior of the seat recipient (eg, attitude, politeness) interact to shape participants’ decision-making, especially in emotionally charged encounters. Figure 1 shows that personal values were frequently co-coded with participants’ reflections on the demeanor of older adults, suggesting that both internal moral orientation and the specific characteristics of older adults as social actors shape students’ moral behavior. This highlights the central role of older adults in triggering ethical deliberation and relational interpretation among health care students.38,39 In particular, when older adults were perceived as either respectful or demanding, participants responded not only with empathy or irritation, but also engaged in value-based reasoning that reflected their emerging professional identity.
Cultural context also plays an important role in interpreting these findings. In East Asian societies influenced by Confucian values, public behavior is often informed by expectations of respect for older adults and social harmony.20,21 These values may amplify the moral weight of public encounters, particularly in structured social spaces such as public transportation. However, the results of the current study also reveal tensions—between norm adherence and emotional authenticity, between social obligation and self-preservation. Such tensions suggest that even within collectivist cultural frameworks, moral behavior remains situational and negotiated. Together, the findings highlight the importance of preparing health care students to navigate ethical ambiguity not only in clinical practice but also in everyday public life. Future research and educational practice could consider developing interventions that promote moral reflection, empathy, and situational awareness, as such efforts may help bridge the gap between professional ideals and real-world social behavior. By training students to recognize and respond to diverse forms of human vulnerability in public contexts, educators may foster a more humanistic and socially responsive generation of health professionals.
Beyond Confucian influences, several other cultural frameworks could illuminate the moral decision-making patterns observed in our study. Buddhist and Taoist philosophical traditions, deeply embedded in Taiwanese society, 40 emphasize compassion and harmonious action that may reinforce prosocial behavior toward vulnerable individuals. 41 The Buddhist concept of merit-making through kind acts and the Taoist principle of wu wei (effortless action aligned with natural order) may explain why many participants described seat-offering as “automatic” or “natural” behavior. Collectivist versus individualist cultural orientations provide another lens for understanding our findings. Taiwan’s collectivist culture emphasizes group harmony and social responsibility, 42 which may explain the prominence of personal values (n = 523, 67.6% of responses) in driving prosocial behavior. In contrast, more individualistic societies might show greater emphasis on personal choice and explicit reciprocity expectations. Cross-cultural structural considerations suggest that our findings may vary in different societal contexts. Similarly, cultures with different aging demographics, urban density patterns, or public transportation norms would likely produce distinct patterns of moral reasoning and prosocial behavior. Future comparative research could explore how healthcare students in Western individualistic societies or other East Asian collectivist cultures navigate similar moral dilemmas in public spaces.
Limitations
Several limitations of this study should be acknowledged. First, although the study included a relatively diverse sample of health care students from 3 departments, all participants were recruited from a single college in Taiwan. This may limit the generalizability of the findings to health care students in other regions or cultural contexts. Moreover, our sample showed a significant gender imbalance, with approximately 81% female and 19% male participants. This distribution, while reflecting the typical gender composition of healthcare programs, particularly nursing (eg, Refs.43,44), may limit the generalizability of our findings to more gender-balanced populations. The predominance of female participants may have influenced the patterns of moral reasoning and prosocial behavior observed in our study, as research suggests potential gender differences in empathy, moral sensitivity, and helping behaviors.45,46 Future studies should examine whether these findings hold across more gender-diverse samples of healthcare students.
Second, the study relied on participants’ self-reported experiences and reflections, which may be subject to recall bias or social desirability bias. Participants may have been inclined to present themselves in a morally favorable light when describing seat-offering behaviors. In addition, the use of a structured questionnaire format may have restricted the depth of exploration for certain nuanced experiences. While our study successfully identified factors influencing seat-offering behavior, our data collection approach focused primarily on participants’ priority seating experiences and moral reasoning processes. This focus may have limited participants’ spontaneous discussion of other potential social characteristics that could influence prosocial behavior, such as detailed gender considerations, socioeconomic indicators, or ethnic factors. Future research could employ more targeted questioning or observational methods to systematically explore how these additional social characteristics shape healthcare students’ prosocial decision-making in public transportation and other everyday settings.
Third, this study did not observe actual behavior but instead explored students’ narrated experiences. As such, it reflects students’ moral reasoning and retrospective interpretations rather than direct observations of behavior in real-time public settings. Finally, while the study identified culturally shaped patterns of moral reasoning, it did not compare these findings with students from non-Confucian societies. Future cross-cultural research could further elucidate how cultural values influence public moral behavior across different regions. Last but not least, the questionnaire used in this study was not formally validated or pilot-tested prior to data collection. While this approach allowed us to capture authentic, context-specific responses relevant to our research questions, future studies would benefit from pilot-testing instruments to further refine question clarity and comprehensiveness.
Implications
The findings of this study have several important implications for healthcare provider education and clinical pedagogy. First, given that personal values were the primary driver of prosocial behavior (67.6% of responses), healthcare education programs should incorporate explicit moral reasoning and values clarification exercises beyond traditional clinical skills training. Rather than assuming that professional ethical behavior will emerge naturally, curricula should include structured opportunities for students to examine their own moral decision-making processes in everyday contexts.
Second, our finding that students’ behavior might be influenced by the demeanor and attitude of those in need (26.7% of responses) suggests that clinical training should address the challenge of maintaining empathy and professional care when working with difficult or demanding patients. Simulation exercises and case-based learning could help students practice providing compassionate care regardless of patient behavior or attitude. Finally, the prominence of situational judgment and contextual sensitivity in participants’ responses indicates that healthcare education should move beyond rule-based ethical training to develop adaptive moral reasoning skills. This could include problem-based learning scenarios that require students to navigate competing values, cultural expectations, and individual needs—skills directly applicable to clinical decision-making.
Conclusions
This qualitative study examined how health care students in Taiwan observe, interpret, and respond to others’ needs in the everyday context of public seating. Through an analysis of structured narrative responses, the study identified how students draw on both categorical norms and situational empathy to determine whether and when to offer their seat to others. The findings highlight the central role of internalized personal values and perceived recipient demeanor in shaping moral behavior. Notably, participants often acted based on intuitive moral impulses, while still attending to contextual cues and interpersonal dynamics. The study also underscores the specific role of older adults and individuals with mobility impairments in triggering seat-offering behavior, especially when need was clearly observable.
By illuminating the interplay between professional identity development and moral responsiveness in public life, this study contributes to a deeper understanding of how health care students internalize and enact prosocial behavior. The findings point to the value of educational efforts that cultivate ethical awareness, interpersonal sensitivity, and real-world moral judgment as essential components of health care professionalism.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251381578 – Supplemental material for Personal Values in Everyday Prosocial Situations Among Healthcare Students: A Qualitative Content Analysis
Supplemental material, sj-docx-1-inq-10.1177_00469580251381578 for Personal Values in Everyday Prosocial Situations Among Healthcare Students: A Qualitative Content Analysis by Chih-Chi Liu in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580251381578 – Supplemental material for Personal Values in Everyday Prosocial Situations Among Healthcare Students: A Qualitative Content Analysis
Supplemental material, sj-docx-2-inq-10.1177_00469580251381578 for Personal Values in Everyday Prosocial Situations Among Healthcare Students: A Qualitative Content Analysis by Chih-Chi Liu in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The author would like to acknowledge the participants who participated in this study.
Ethical Considerations
This study was approved by Research Ethics Committee, National Taiwan Normal University with IRB protocol/human subjects approval number 202412ES065 (Approval Date: March 13, 2025).
Author Contributions
Chih-Chi Liu: Visualization, Software, Methodology, Formal analysis, Writing—original draft, Supervision, Project administration, Funding acquisition, Conceptualization, Writing—review & editing, Validation, Resources, Investigation, Data curation.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by the National Science and Technology Council in Taiwan [NSTC 114-2410-H-570-001-MY2]
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation. The data are not publicly available due to restrictions their containing information that could compromise the privacy of research participants.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.