
Abstract
This systematic review and meta-analysis evaluated how exergaming (EXG) compares with various conventional physical therapies in improving balance and reducing fall risk among prefrail and frail older people. We searched 6 databases PubMed, Medline, CINAHL Complete, Scopus, the Cochrane Library, and Web of Science up to April 2025. Study quality and evidence certainty were appraised using PRISMA, TESTEX, Rob 2, and GRADE. For meta-analysis, Hedge’s g effect sizes were computed for balance and fall risk outcomes. We chose fixed- or random-effects models and conducted subgroup analyses based on therapy dosage (sessions per week and minutes per session). The protocol is registered in PROSPERO (CRD420251009891). From 2434 records, 10 RCTs (n = 400; mean and standard deviation age 75.7 ± 5.9 years) met inclusion criteria. Overall and subgroup meta-analyses (4 each) showed significant EXG benefits for the Mini-BESTest (P < .01), Timed Up-and-Go (TUG; P < .05) and Fall Efficacy Scale-International (FES-I; P < .05). No statistically significant change was found for the Berg Balance Scale (BBS; P = .05). When stratifying by dosage, EXG outperformed controls in TUG specifically for protocols with fewer than 3 sessions/week and under 50 min/session (P < .01). Dosage did not significantly influence FES-I outcomes. EXG is an alternative therapy that improves balance by reducing the fall risk, as measured by the Mini-BESTest, TUG, and FES-I, compared with conventional physical therapies (ie, physiotherapy, balance training, strength training, aerobic training, multicomponent training). Notably, protocols with <3 weekly sessions of <50 min each yielded the most pronounced TUG improvements.
Highlights
● EXG reduces the fall risk.
● EXG improves performance on TUG.
● EXG is an effective alternative therapy.
Introduction
Frailty is a worldwide public health problem in the aging population World Health Organisation Clinical Consortium on Health Ageing. 1 A systematic review that analyzed 62 countries worldwide with a total of 1 755 497 participants reported a prevalence of prefrailty of 50% in people older than 60 years and 23% frailty. 2 Frailty is a cumulative decline in physiological systems, leading to a state of increased vulnerability to stressful events, 3 having multiple clinical and social consequences, and its dynamic nature, 4 increasing balance problems and increasing the fall risk such as fractures and hospitalization. 5 Therefore, it is important to apply therapies that improve physical and functional parameters in older people with frailty. 6
Physical activity is one of the most commonly used therapies for frail older people. 7 Using physiotherapy (PT), balance training, strength training, aerobic training, and multicomponent training (MCT) are the most common conventional therapies for physical activity.8,9 In a systematic review conducted by Silva et al 9 in frail community-dwelling older people, PT interventions were reported to be effective in decreasing levels of physical frailty compared with control interventions with minimal physical activity. In a systematic review conducted by Cadore et al, 10 different therapies applied in frail older people were analyzed, including strength training, aerobic training, balance training and MCT, and the results revealed that MCT was more effective in improving balance and gait ability and reducing fall risk. Similarly, a meta-analysis conducted by Yang et al 11 in frail older people reported significant improvements in physical function in terms of muscle strength (P < .05), gait speed (P < .001), balance (P = .02), Timed Up-and-Go (TUG, P < .001) and frailty status (P < .05) through MCT compared with those of the active control groups. Although these conventional therapies have positive effects on physical function and fall risk in frail older people, they are not easily accessible. 12 Therefore, novel alternatives, such as interventions using virtual reality or exergaming (EXG),13,14 have positive effects on physical functional parameters in older people with frailty.15,16 In a systematic review conducted by Zheng et al 16 in frail older people, EXG using consoles Nintendo® Wii and Xbox 360® improved balance and mobility compared with active/inactive control groups. Compared with the control group, the EXG combined with strength training group presented an increase in muscle strength. Similarly, a meta-analysis conducted by Alhasan et al 15 in older people with frailty reported significant improvements in the Berg Balance Scale (BBS, P < .001) and TUG (P = .03) in favor of EXG using the Nintendo® Wii console compared with conventional physical activity.
There is evidence of the positive effects of EXG interventions on physical functional parameters in older people with frailty.15,16 Owing to the importance of updating scientific evidence in public health settings in older people, 17 as well as the importance of subgroup analyses in meta-analyses, the response to general analyses by variable may vary. 18 Therefore, this systematic review with meta-analysis aimed to analyze the effects of EXGs concerning different types of conventional physical therapies (ie, PT, balance training, strength training, aerobic training, and MCT) on balance and fall risk in prefrail and frail older people. Second, the effects of EXG on balance and fall risk should be analyzed by training dosage as a type of conventional therapy.
Methods
Protocol and Registration
The PRISMA guidelines were followed in this systematic review with meta-analysis. 19 PROSPERO (International Prospective Register of Systematic Reviews; ID code: CRD420251009891) has the protocol registered.
Eligibility Criteria
The systematic review and meta-analysis incorporated original, peer reviewed articles published up to April 2025, with no restrictions on language or year of publication. Excluded materials comprised conference abstracts, books and book chapters, editorials, letters to the editor, protocol records, reviews, case reports, and trials. The study selection and data extraction were guided by the PICOS framework (Population, Intervention, Comparator, Outcomes, Study design) Table 1.
Selection Criteria Used in the Systematic Review With Meta-Analysis.

Note. BBS = Balance Berg Scale; TUG = timed Up-and-Go; FES-I = Falls Efficacy Scale-International; CG = control group; EXG = exergaming.
Information Search Process and Databases
A comprehensive literature search was carried out from November 2024 to April 2025 across 6 major databases PubMed, Medline, CINAHL Complete, the Cochrane Library, Scopus, and Web of Science (Core Collection). Both U.S. National Library of Medicine MeSH terms and complementary free-text keywords were applied to capture studies on EXG, conventional physical therapies, balance, fall risk, and prefrail or frail status in older people. The search string used was as follows: (“exergames” OR “exergaming” OR “active video games” OR “virtual reality” OR “nonimmersive virtual reality” OR “immersive virtual reality” OR “wii” OR “Kinect” OR “playstation”) AND (“physiotherapy” OR “physical therapy” OR “physical exercise” OR “exercise” OR “traditional therapy” OR “balance training” OR “multicomponent training” OR “resistance training” OR “strength training” OR “gait training” OR “physical activity intervention” OR “physical activity program”) AND (“functional independence” OR “functional dependence” OR “functional mobility” OR “health condition” OR “falls” OR “fall risk” OR “risk of fall” OR “falling risk” “balance” OR “static balance” OR “dynamic balance”) AND (“elderly” OR “older people” OR “older adults” OR “older subject” OR “aging” OR “aging” OR “aged”). Two sport science experts (each holding a PhD and with peer reviewed publications on physical performance either across diverse populations or in impact-factor journals per Journal Citation Reports®) independently evaluated the selected studies and our inclusion/exclusion criteria. To minimize bias, we did not share our search strategy with them. Finally, on April 10, 2025, we checked relevant databases for any retractions or errata associated with the included papers.
Study Selection and Data Collection Process
Studies were exported from EndNote X9 (Clarivate Analytics, Philadelphia, PA, USA). Independently, JHM and ICC ran the searches, removed duplicates, screened titles and abstracts, and reviewed full texts identifying no discrepancies. The same steps were applied to studies recommended by external experts and those found in reference lists. Finally, full texts of all potentially eligible papers were assessed, and reasons for excluding those that did not meet the selection criteria were recorded.
Methodological Quality Assessment
TESTEX, a tool for exercise-based intervention studies, 20 was used to assess the methodological quality of the chosen studies. One potential exclusion criterion was TESTEX results. 20 According to Smart et al, 20 there is a 15-point rating system (5 points for study quality and 10 points for reporting). Two authors (JHM, ICC) carried out this process separately, whereas a third author (EVC) served as a referee for cases that were borderline and needed further validation from another author (PVB).
Data Synthesis
The following data were obtained and analyzed from the selected studies: (i) author and year of publication; (ii) country of origin; (iii) study design; (iv) sex and mean age of the sample; (v) number of participants in the intervention and CG; (vi) type of console and game; (vii) health status; (viii) training volume (total duration, weekly frequency and time per session); (ix) training intensity; (x) balance; (xi) fall risk (xii); adverse events; and (xiii) adherence.
Risk of Bias in Individual Studies
Two independent researchers (JHM and ICC) evaluated the risk of bias version 2 (RoB 2) of the included studies, and a third researcher (PVB) analyzed the results. The Cochrane Handbook for Systematic Reviews of Interventions’ recommendations for RCTs (randomized controlled trials) was the foundation for this evaluation. 21 On the basis of the randomization procedure, departures from the planned interventions, missing outcome data, outcome assessment, and choice of the reported result, the risk of bias was categorized as “high,” “low,” or “some concerns.”
Summary Measures for Meta-Analysis
The meta-analysis procedures are fully detailed in PROSPERO (CRD420251009891). Following Valentine et al, 22 we only synthesized outcomes reported by at least 3 studies. Hedge’s g effect sizes for each balance and fall risk measure were derived from pre to post intervention means and SDs, with scores standardized by their change-score SD. Effect sizes are shown with 95% CIs and classified per Hopkins et al 23 thresholds: trivial (<0.2), small (0.2-0.6), moderate (>0.6-1.2), large (>1.2-2.0), very large (>2.0-4.0), and extremely large (>4.0). 23 To accommodate between-study variability, we used a random-effects model (Der Simonian–Laird) implemented in Comprehensive Meta-Analysis v2.0 (Biostat, Englewood, NJ, USA). Statistical significance was set at P ≤ .05. 24 For each outcome (BBS, Mini-BESTest, TUG, FES-I), standardized mean differences and raw mean differences comparing EXG versus control were pooled only when at least 3 studies reported comparable data. 25
Heterogeneity between trial results was tested with Cochran’s Q test Ruppar 26 and the I2 statistic. I2 values of <25%, 25%-50%, and >50% represent small, medium, and large amounts of inconsistency, respectively. 27 Egger regression tests were performed to detect small study effects and possible publication bias. 28
Moderator Analysis
Potential sources of heterogeneity affecting training outcomes were predefined and identified via an a priori univariate analysis under a random effects framework.
Sensitivity Analyses
To assess the robustness and stability of the results, sensitivity analyses were conducted for all meta-analyses that included at least 4 studies. A leave-one-out approach was applied, whereby the pooled effect size was recalculated after sequentially excluding each individual study, using the same DerSimonian–Laird random-effects model applied in the main analysis. For each iteration, changes in the overall effect size, statistical significance (p-value), and heterogeneity parameters (τ², Q, and I²) were evaluated. In addition, targeted sensitivity analyses were performed by excluding studies identified as potentially problematic, based on 2 predefined criteria: (i) High risk of bias: studies classified as “high risk” in the overall assessment using the RoB 2.0 tool were excluded. This analysis was only performed when their removal left at least 3 studies in the meta-analysis; (ii) Outlier or influential studies: identified through a combination of visual inspection of forest plots and quantitative influence diagnostics. 29 A study was considered an outlier if its effect size substantially deviated from the pooled confidence interval or if it exerted disproportionate influence on the overall estimate, as indicated by extreme values in 1 or more influence metrics. Specifically, the following thresholds were applied: DFBETAS > |1|, indicating substantial impact on model coefficients; Cook’s distance > 4/n, where n is the number of studies (values > 0.5 were also considered in small samples); and hat values > 2k/n, where k is the number of predictors (typically k = 1 in random-effects models). Studies exceeding 1 or more of these thresholds were flagged and excluded in additional sensitivity analyses to assess the robustness of the pooled effects.
Subgroup Analysis
Given the differences that may exist regarding the intervention applied by the control group versus the experimental groups both in balance and fall risk,30,31 the types of interventions in the control group versus the experimental groups were compared. Similarly, the dosage of training (weeks, sessions per week and minutes per session) 32 was considered a possible moderating variable.
Certainty of Evidence
Studies were categorized as having high, moderate, low, or very low confidence on the basis of their assessment of the GRADE scale. 33 Because studies with RCT designs were included, all analyses began with a high degree of certainty and were downgraded if there were concerns about bias, consistency, accuracy, precision, directness of results, or risk of publication bias. 33 JHM and ICC each conducted independent study assessments, with any conflicts adjudicated by a third reviewer (EVC).
Results
Study Selection
Figure 1 details the search process for the studies. A total of 2434 records were found. Duplicates were subsequently eliminated, and the studies were filtered by selecting the title, abstract, and keywords, resulting in 1019 references. In the subsequent analysis phase, 884 articles were excluded because the texts did not meet the search criteria, leaving 135. A total of 117 studies were subsequently excluded: 61 descriptive studies, 13 non-randomized controlled trials, 17 interventions in older people with other pathologies, 21 systematic reviews in apparently healthy older people, and 5 studies in other age groups. After this process, 18 potential studies remained, of which 8 were excluded for other types of interventions in prefrail and frail older people. Ten studies met all the selection criteria.34 -43
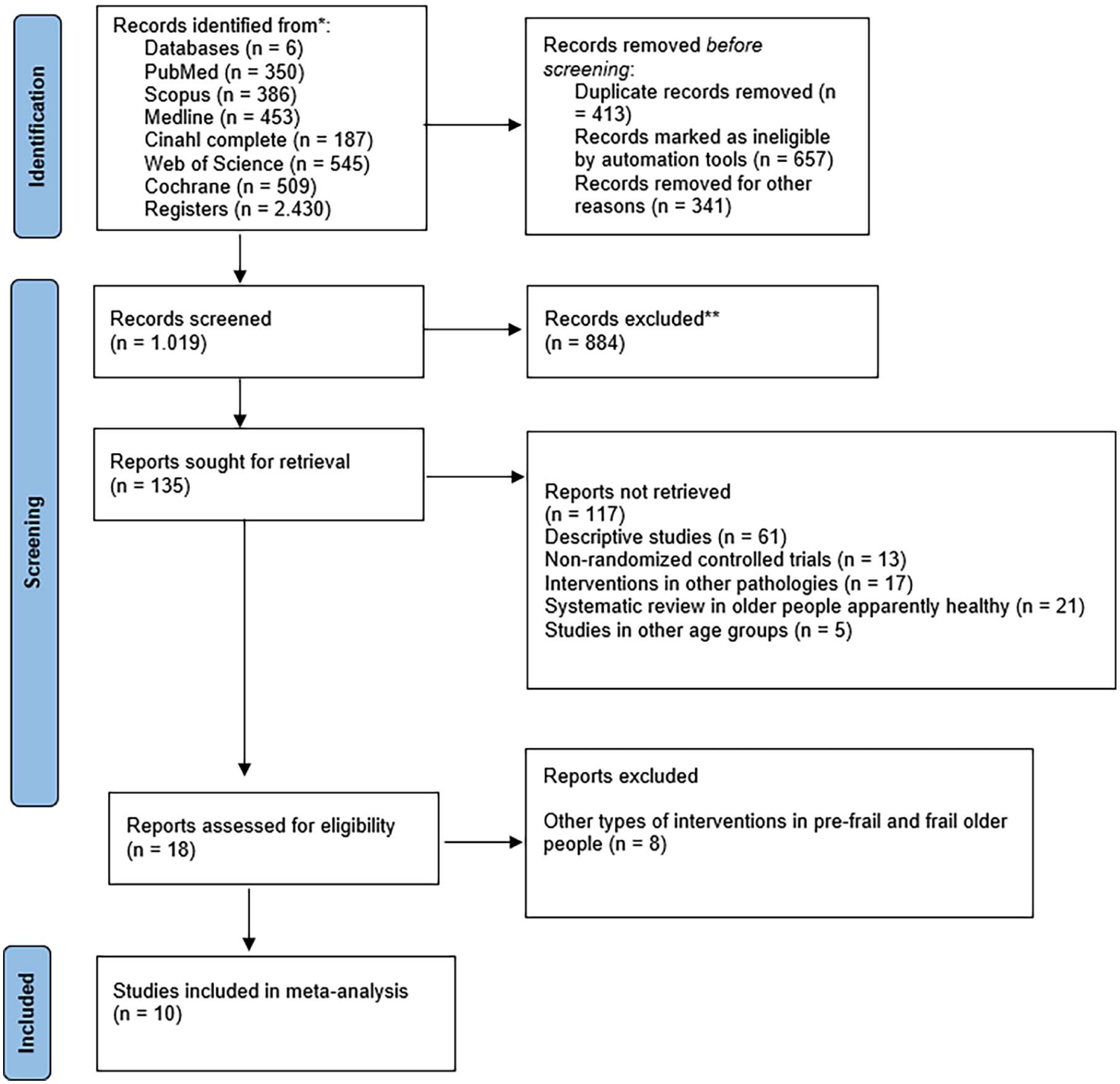
Flowchart of the review process.
Methodological Quality
The 10 selected studies were analyzed via the TESTEX scale (Table 2). All the studies achieved a score equal to or greater than 60% on the scale,34 -43 namely, 10/1537,41 -43, 11/1535,39, 12/15,36,38,40 and 14/15. 34
Study quality assessment according to the TESTEX scale.

Three points are possible: 1 point if adherence >85%, 1 point if adverse events were reported, and 1 point if exercise attendance was reported.
Two points possible: 1 point if the primary outcome is reported and 1 point if all other outcomes are reported.
Total out of 15 points. TESTEX: Tool for assessing study quality and reporting in exercise.
Risk of Bias
Two studies were assessed as having a low risk of bias across all domains.38,43 Six studies reported some concerns in 1 or more domains.34 -36,40 -42 Two studies were classified as having a high risk of bias.37,39 Overall, the risk of bias was moderate, with most studies presenting some concerns and only a few demonstrating low risk across all domains. Figures 2 and 3 present the risk of bias.

Risk of bias within studies.

Risk of bias summary: Review the authors; judgments about each risk of bias item in each included study.
Studies and Sample Characteristics
All studies were RCTs, with the majority (5 studies) being conducted on the continent of Asia,34,35,38,42,43 followed by North America (2 studies),37,41 South America (2 studies),36,39 and Europe (1 study). 37 With a mean age of 75.7 ± 5.9 years and the highest percentage of sex analyzed being women > 80%, the total sample size was 400 participants (EXG: 197 and CG: 203). The types of virtual reality used by the EXG included 8 studies34 -40,43 involving non immersive virtual reality with Nintendo Wii or Xbox Kinect consoles and 2 studies41,42 involving semi-immersive virtual reality with computer games (under pressure) or the NIRVANA virtual reality interactive system (balance games) compared with conventional therapy by PT,34,36,41,43 MCT,38 -40 and conventional balance training.35,37,42 The training duration ranged from 6 to 12 weeks, with a frequency of 2 to 3 sessions per week, with 30 to 90 min per session. Only one study 39 reported a training intensity of 10 to 15 RPE with a score of 20. These results are presented in Table 3.
Effects of Exergaming Versus Conventional Physical Therapies on Balance and Fall Risk in Older People Prefrail and Frail.
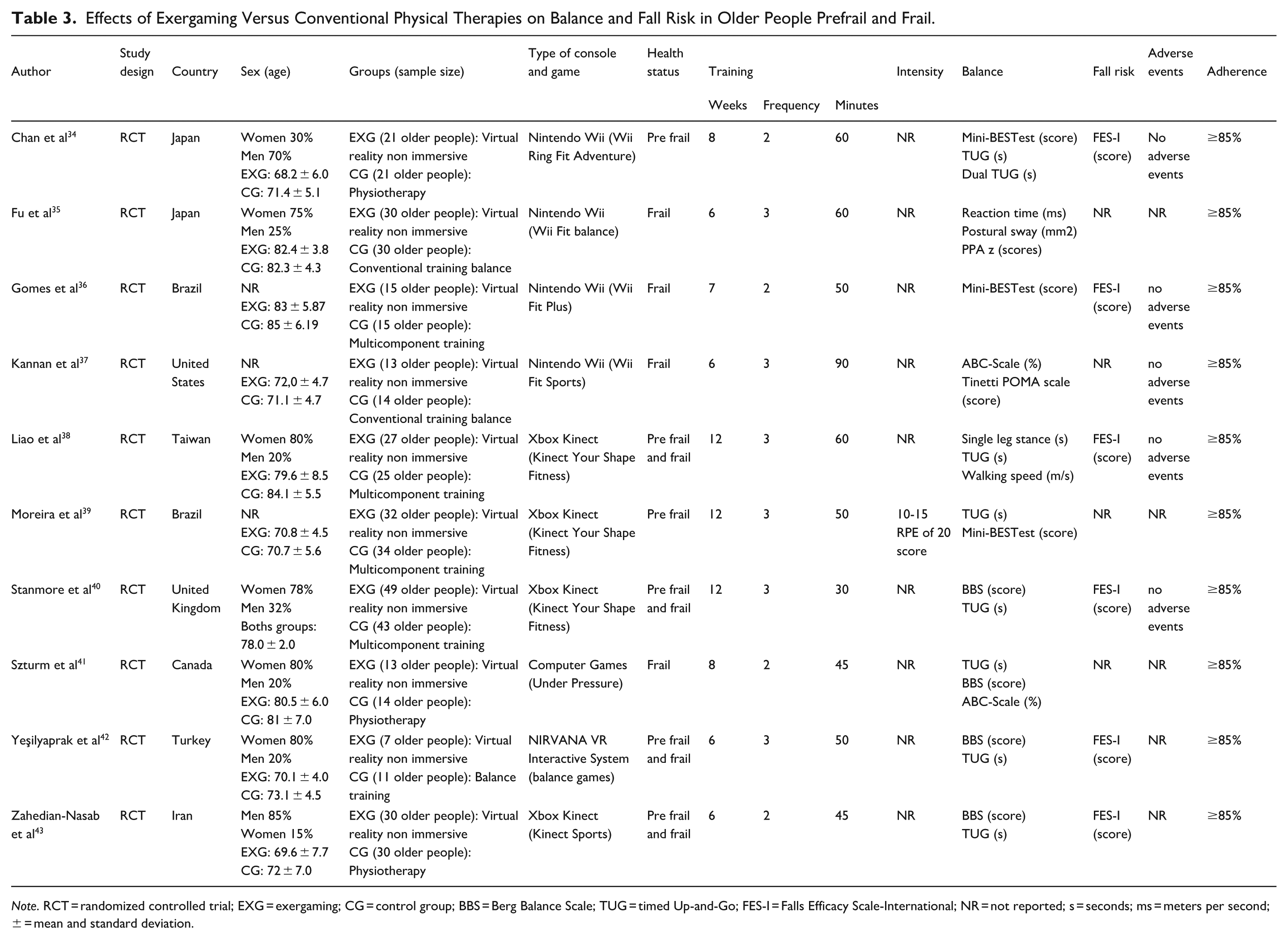
Note. RCT = randomized controlled trial; EXG = exergaming; CG = control group; BBS = Berg Balance Scale; TUG = timed Up-and-Go; FES-I = Falls Efficacy Scale-International; NR = not reported; s = seconds; ms = meters per second; ± = mean and standard deviation.
Meta-Analysis Results
For the global meta-analysis, when comparing EXG versus conventional therapy in balance variables, significant improvements (P < .05) with large effects (ES = 0.70-0.74) are presented in the Mini-BESTest and TUG in favor of EXG. For fall risk, significant improvements (P = .02) were reported in the FES-I, with a moderate effect (ES = 0.45) in favor of EXG. There were no significant improvements (P = .49) in the BBS, with a very small effect (ES = −0.66). These results are presented in Table 4 and Supplemental Appendices (Supplemental Figures S1 to S4), as a forest diagram graphically representing the results.
Effects of Exergaming Versus Conventional Therapies on Balance and Fall Risk in Older People Prefrail and Frail.

Data indicate the number of studies that provided data for analysis, the number of experimental groups, the number of control groups, and the total number of older people prefrail and frail included in the analysis, respectively.
Meta-Analysis Results With Sensitivity Analysis
For dynamic balance, the TUG test revealed a large and statistically significant effect in favor of EXG (ES = 0.70, 95% CI [0.07, 1.33], P = .030; I² = 84.3%). Sensitivity analyses confirmed the robustness of this result: although the study by Zahedian-Nasab et al 43 was identified as influential, its exclusion only slightly reduced the effect size (ES = 0.39) and heterogeneity (I² = 44.6%), while the result remained significant (P = .038). Excluding Moreira et al 39 had minimal impact, confirming the consistency of the finding. For fall risk, the FES-I showed a moderate and significant effect (ES = 0.46, 95% CI [0.06, 0.85], P = .023; I² = 52.1%). However, this outcome was sensitive to the inclusion of Zahedian-Nasab et al, 43 which was flagged as influential. Its removal led to a loss of statistical significance (P = .10) and a notable drop in heterogeneity (I² = 29.2%), suggesting that this result should be interpreted with caution. Regarding static balance, measured with the BBS, no significant effect was observed (ES = –0.67, 95% CI [–2.59, 1.25], P = .496; I² = 94.5%). The study by Szturm et al 41 was identified as a high-influence outlier. Its exclusion reversed the direction of the effect (ES = 0.82), reduced heterogeneity to zero (I² = 0%), and rendered the overall result non-significant (P = .95), indicating that the pooled estimate was disproportionately affected by this single study. Finally, for Mini-BESTest, a large and significant effect was observed (ES = 0.74, 95% CI [0.19, 1.30], P < .01; I² = 21.4%). However, due to the limited number of studies included in the meta-analysis (n = 3), sensitivity analysis could not be conducted. Removing a single study would reduce the sample to only 2, severely compromising the ability to assess between-study variance and the stability of the effect. Therefore, these findings should also be interpreted with caution.
Training Dosage
When the subgroups were analyzed by training dosage, significant improvements (P < .01, ES = 1.29) were reported in the TUG test, with 3 sessions per week and a duration of 50 min per session (P < .001, ES = 1.31) in favor of EXG. However, no significant differences in fall risk according to training dosage were found according to the FES-1 score. These results are presented in Supplemental Appendices (Supplemental Figures S5 to S10), as a forest diagram graphically representing the results.
Types of Conventional Therapy
When balance and fall risk were analyzed via the TUG test according to the type of conventional therapy, there were significant improvements in favor of EXG concerning PT, with a very long effect (ES = 1.30, P < .01), whereas when EXG was compared with MCT, there were no significant differences. These results are presented in Appendix (Supplemental Figure S7), as a forest diagram graphically representing the results.
Certainty of Evidence
The certainty of evidence for EXG was moderate for balance and fall risk. Although the studies were RCTs, some concerns about the risk of bias reduced the certainty. The results indicate a positive impact on prefrail older people (Table 5).
Certainty of Evidence.

Discussion
The aim of this systematic review with meta-analysis was to analyze the effects of EXG concerning different types of conventional physical therapies (ie, PT, balance training, strength training, aerobic training, MCT) on balance and fall risk in prefrail and frail older people. Second, the effects of EXG on balance and fall risk were analyzed using the training dose as a conventional therapy. The overall meta-analysis comparing EXT with conventional therapy in terms of balance variables revealed significant improvements (P < .05), with a significant moderate effect (ES = 0.70-0.74) in the Mini-BESTest and TUG in favor of EXG. Similarly, significant improvements were reported in the FES-I test, with a moderate effect (ES = 0.45; P = .02) in favor of EXG. Moreover, no significant improvements in BBS were identified (ES = −0.66; P = .49), with a very small effect.
The leave-one-out and influence diagnostics confirmed the robustness of the results for the TUG outcome. The magnitude and direction of the pooled effect remained statistically significant (P < .05) after sequentially removing individual studies, and only one study Zahedian-Nasab et al 43 was identified as influential. Although its exclusion slightly reduced the effect size and heterogeneity, the benefit of EXG on dynamic balance persisted, supporting the stability of this finding. In contrast, the results for the FES-I outcome were more sensitive. The exclusion of Zahedian-Nasab et al. 43 led to a loss of statistical significance and a notable drop in heterogeneity (I² = 29.2%), suggesting that this variable’s pooled estimate was disproportionately affected by a single study. For the BBS outcome, the study by Szturm et al 41 had a considerable impact on the overall result. Its removal reversed the direction of the effect and eliminated heterogeneity (I² = 0%), indicating that the non-significant result initially observed was largely driven by this outlier. Regarding the Mini-BESTest, sensitivity analysis could not be conducted due to the limited number of studies included in the meta-analysis (n = 3). Excluding a single study in this context would leave only 2 data points, severely restricting the model’s capacity to estimate between-study variance and assess the stability of the overall effect. Therefore, the results for this outcome should be interpreted with caution, taking into account this methodological limitation.
On the other hand, the subgroup meta-analysis according to the training dose reported significant improvements in the TUG test with <3 weekly sessions (ES = 1.29; P < .01), with a duration of <50 min per session (ES = 1.31; P < .001) in favor of the EXG. In terms of fall risk, no significant differences were found according to training dose according to the FES-I score. The subgroup analysis according to the type of conventional therapy revealed significant improvements in the TUG test in favor of EXG concerning PT, with a very prolonged effect (ES = 1.30; P < .01), whereas the comparison of EXG with MCT did not reveal significant differences.
Berg Balance Scale
No significant improvements were observed for BBS in favor of EXG. Alhasan et al 15 in a review with a meta-analysis that investigated the effects of interactive video games on postural control and fall risk in prefrail and frail older people, reported significant improvements in BBS (P < .001) in favor of EXGs compared with traditional therapeutic exercises. This finding is similar to what was reported by Liu et al 44 in a meta-analysis on the effects of Wii Fit exercise on balance in older people, who reported significant improvements in BBS (P < .05) compared with no-exercise conditions. This is in line with what was reported by Hernandez-Martinez et al 13 in an overview of systematic reviews and meta-analyses on the effects of EXG on physical performance in older people who reported significant improvements in BBS (P = .02) compared with control conditions. The BBS test includes actions such as standing with one’s feet together, standing on only one leg, turning one’s body, walking in different directions, and retrieving an object from the ground, among others. 45 In this sense, the largest body of evidence available has suggested that EXG, through degrees of freedom applied in different directions, cause participants to constantly shift their center of pressure, challenging balance. 46 In addition, the movements performed during EXG involve constant visual, auditory, and proprioceptive feedback, which stimulates the sensorimotor system with the aim of maintaining the stability of the joints used during body movements. 47 Our findings are striking since they contradict the current evidence on the effects of EXG on the BBS in prefrail and frail older people. However, this may be attributed to the high heterogeneity of the studies in our meta-analysis (94.4%), whereas the 2 meta-analyses15,44 reported moderate and low heterogeneity (31% and 16%, respectively). In this context, the different study designs, as well as the intensity and characteristics of the participants and the type of EXG used, may have hindered the identification of significant improvements in our meta-analysis. Conversely, the sensitivity and influence analyses conducted for the BBS outcome revealed that the study by Szturm et al 41 had a high impact on the pooled estimate. Specifically, excluding this study reversed the direction of the effect, resulting in a significant benefit in favor of EXG (ES = 0.82; 95% CI [0.41, 1.22]; P < .001) and eliminated heterogeneity (I² = 0%). This suggests that the non-significant and highly heterogeneous result observed in the main analysis (ES = –0.67, P = .49, I² = 94.4%) is highly sensitive to the inclusion of Szturm et al, 41 whose extreme effect size in favor of the control group (ES = –5.73) substantially distorts the pooled estimate. Therefore, while caution is warranted when interpreting the overall BBS findings, the consistency across the remaining studies points toward a potential benefit of EXG in improving static balance in prefrail and frail older people.
Mini-BESTest (score)
Significant improvements were found for the Mini-BESTest (P = .000, ES = 0.74) in favor of EXG compared with conventional therapy conditions. This is different from what was reported by Chen et al 47 in a meta-analysis comparing the effects of EXG versus conventional physical activity in older people, who reported no significant differences in physical and cognitive function between the groups analyzed. To our knowledge, this is the first meta-analysis to compare the effects of EXG therapy with those of conventional therapy in prefrail and frail older people, including the Mini-BESTest. However, it is important to mention that our meta-analysis included only 3 studies34,36,39 and that only one study reported the activities performed by the control group, making comparisons between the interventions difficult. 39 Specifically, Gomes et al 36 and Chan et al 34 reported that the control groups in their studies only continued their usual physical therapy care without detailing the activities performed. Moreira et al 39 reported that the control group performed an MCT programed with strength exercises involving a predominance of the lower limb muscles. The authors reported that the EXG group and the control group that received MCT did not present significant differences in balance. However, they highlighted the novel EXG approach, which is an innovative, fun and relatively safe strategy for execution by older people. 48 The literature has reported that balance impairments in prefrail and frail older people can be reduced and improved by performing physical activities that involve postural control, temporal reactions, and reactive recovery actions. 49 In this sense, EXG interventions involve older people interacting with a fictional environment and focusing on the demands of the games to reproduce movements and elaborate responses according to the required stimuli. 50 Interacting with the game environment and observing the avatar’s movements offer constant feedback that can contribute to better processing of the sensory capacity necessary to maintain balance.51,52 Jorgensen et al 53 reported that EXG challenge older people to control their center of pressure in multiple directions. For this reason, EXG can stimulate the integration of the vestibular, proprioceptive, auditory, and visual systems, which is necessary to improve balance. 54 On the other hand, sensitivity analysis could not be conducted due to the limited number of studies included in the meta-analysis (n = 3). Therefore, the results for this outcome should be interpreted with caution, taking into account this methodological limitation.
Timed Up-and-Go
Compared with conventional therapy, EXG significantly improved the TUG score. This finding is similar to that reported by Alhasan et al 15 in a systematic review with a meta-analysis that investigated the effects of interactive video games on postural control and fall risk in prefrail and frail older people, who reported significant improvements in the TUG test (P = .03) in favor of EXG compared with traditional therapeutic exercises. Similarly, Chen et al, 47 in a systematic review with meta-analysis comparing the effects of EXG interventions with those of conventional physical activity, reported significant improvements in the TUG test (P = .02) in healthy older people. Similarly, Hernandez-Martinez et al, 13 in an overview of systematic reviews and meta-analyses on the effects of EXG on physical performance in older people, reported significant improvements in TUG (P < .01) in favor of EXG compared with control conditions. The evidence presented consistently suggests that EXG can improve TUG performance in prefrail and frail older people compared with conventional therapy conditions. This fact is relevant, given that older people able to complete the TUG in less than 10 s have been reported to have a low fall risk. 55 Our findings indicate that the improvements in the TUG test in favor of EXG over conventional therapy can be attributed to the motor actions of the games, which involve a constant change in the center of pressure in older people.46,56 Like what was reported in the Mini-BESTest, EXG stimulated participants’ motor control, as they must correctly reproduce the movements to succeed in the games. Compared with conventional therapy, constant visual and auditory feedback implies greater participation of the sensorimotor system, in addition to incorporating afferent components, central integration and processing processes, and efferent responses, with the purpose of maintaining joint stability during actions performed in games. 57 This, added to the fun and innovative way in which older people can exercise and simulate the practice of different sports, becomes beneficial for improving balance and reducing fall risk. 58
Regarding the influence analysis, the study by Zahedian-Nasab et al 43 was identified as influential. Excluding this study substantially reduced heterogeneity (from I² = 84.3% to 44.6%) and slightly decreased the overall effect size (from ES = 0.70-ES = 0.39; P = .038). Despite this reduction, the pooled effect remained statistically significant in favor of EXG. These findings suggest that although Zahedian-Nasab et al. 43 amplifies the observed benefit of EXG on dynamic balance, the result remains robust even when this study is excluded. On the other hand, excluding the study by Moreira et al, 39 which was identified as having a high risk of bias, led to a slight increase in the overall effect size (from ES = 0.70-ES = 0.76) and a modest reduction in heterogeneity (I² decreased from 84.3% to ~80%). The pooled effect remained statistically significant (P < .05), suggesting that this study did not substantially distort the direction or significance of the results. Therefore, the beneficial effects of EXG on TUG performance in prefrail and frail older people appear to be consistent, albeit with some sensitivity to individual studies of large magnitude.
Falls Efficacy Scale-International
Compared with conventional therapy conditions, significant improvements in the FES-I score (P = .02; ES = 0.45) were found in favor of EXG. Similarly, Chen et al, 47 in a meta-analysis review comparing the effects of EXG interventions with those of conventional physical activity in healthy older people, reported significant improvements in fall efficacy (P = .002) in favor of EXG. Similarly, Ge et al, 59 in a systematic review on the effectiveness of EXGs on fall risk in older people, reported significant improvements in the fear of falling in favor of EXGs compared with control groups. Importantly, the FES-I scale has been shown to be valid and reliable for clinical assessments of fall risk in older people.60,61 The FES-I does not represent the actual incidence of falls but only assesses worry and fear of falling, with questions limited to daily household activities and social activities outside the home.60,61 In this context, EXG interventions, compared with conventional physical therapy, can generate greater confidence in daily tasks that require balance, such as walking on uneven surfaces, getting up from a chair, picking up an object from the floor, or going up and down stairs. 62 This may be attributed to real-time feedback on older people’s body movements and performance in games. 54 Specifically, positive reinforcement for the actions performed or the score achieved can favor participants’ self-confidence. 63 This is relevant, given that older people may feel more secure and confident in their motor actions for their daily activities, being more aware and able to perceive the relationship between the characteristics of their environment and motor control in their actions. 54 Regarding the sensitivity analysis, the study by Zahedian-Nasab et al 43 was identified as influential. Excluding this study reduced the overall effect size (from ES = 0.46-ES = 0.31) and rendered the result non-significant (P = .10), while also decreasing heterogeneity (from I² = 52.1% to 29.2%). These findings suggest that Zahedian-Nasab et al 43 contributed disproportionately to the pooled effect and may have driven the statistical significance of the result in favor of EXG. Although the remaining studies follow the same trend, the loss of statistical significance highlights the need to interpret the FES-I results with caution. Further high-quality trials are warranted to confirm whether EXG interventions consistently reduce fear of falling in prefrail and frail older people.
Subgroup Analysis According to Training Dose
When subgroups according to training dose were analyzed, significant improvements in TUG performance were observed with <3 weekly sessions (ES = 1.29; P < .01), with a duration of <50 min per session (ES = 1.31; P < .001) in favor of EXG. However, no significant improvements in the TUG score were reported with ≥3 weekly sessions with a duration of ≥50 min per session. This finding is relevant since it suggests that there may be an optimal training dose to improve dynamic balance in prefrail and frail older people. This can be explained by the visual and auditory stimuli provided by games that stimulate real-time feedback mechanisms through the development of vestibular and cognitive functions. 64 It is possible that a higher weekly frequency and duration of training sessions overstimulate older people, causing physical and mental fatigue due to the lack of recovery between training sessions, limiting the effectiveness of EXG. 65 Furthermore, during the initiation of EXG interventions, motivation and enjoyment are key factors for generating adherence in older people. 63 Training sessions lasting more than 1 h could cause less enjoyment and concentration in the activity, affecting the adherence of participants.63,65 This is supported by Buyle et al 63 in a meta-analysis review on the role of motivational factors in EXG interventions for fall prevention in older people, who reported that motivational factors are key to improving TUG test results.
Regarding fall risk via the FES-I, no significant differences were found according to the training dose between studies with durations of >7 weeks and ≤7 weeks and studies with frequencies of <3 weekly sessions and those with durations of ≥3 weekly sessions. This could suggest that EXG may be effective in reducing fear of falling in older people when it has a duration of at least 6 weeks of training42,43 and a minimum frequency of 2 weekly sessions.34,43 As mentioned in the previous sections, the FES-I assesses worry and fear of falling with questions limited to daily household activities and social activities outside the home.60,61 In this sense, on the basis of our results, the increase in confidence in older people may be independent of the duration and frequency of the interventions, as it is more related to psychological and perceptual aspects. 66 Furthermore, the improvement in confidence and sense of security in daily motor activities may vary from person to person, with some older people requiring less or more time to feel confident in controlling their movements. This individual variability could reduce the differences between the studies analyzed. 67
Finally, it is important to highlight that most of the included interventions were short-term (6-12 weeks), which limits the ability to assess the long-term effectiveness and sustainability of EXG. Future studies should incorporate follow-up assessments beyond the intervention period and explore whether the benefits in balance and adherence are maintained over time. Addressing these variables will help determine whether EXG is not only an innovative and motivating strategy but also a sustainable and effective long-term therapeutic approach for prefrail and frail older people.
Subgroup Analysis According to the Type of Conventional Therapy
When balance was analyzed via the TUG test according to the type of conventional therapy, significant improvements were observed in favor of EXG over PT, with a very long-lasting effect (ES = 1.30; P < .01), whereas when EXG was compared with MCT, no significant differences were observed. The differences in favor of EXG versus PT may be attributed to the fact that EXG interventions cover both physical function and important functions for improving dynamic balance (eg, motor coordination and cognitive function). 64 Compared with analytical and isolated exercises performed during PT, visual and auditory stimuli provided by games may be superior in improving feedback mechanisms and the regulation of movement control in real-life everyday situations.64,68 Furthermore, when this occurs in conjunction with greater enjoyment and motivation for the activity, its effects may be enhanced. 63 On the other hand, the fact that no significant differences were observed when EXGs were compared with MCTs may be because both types of training have been shown to be effective in improving dynamic balance through the TUG test.13,69 MCT exercise is characterized by the incorporation of resistance, strength, balance, and flexibility training, 70 which has demonstrated positive changes in gait, balance, and cognitive executive function in older people.11,71 In this context, MCT has been recommended by physical activity experts as one of the best strategies to improve physical capacity and reduce falls in older people. 70 On the basis of our findings, although there were no significant differences between EXGs and MCTs, it is important to mention that motivation has been shown to be key to maintaining the frequency and intensity of interventions. 11 Most therapeutic programs are supported by extrinsic motivation. 72 However, the characteristics of EXGs stimulate intrinsic motivation to improve scores obtained in games. That is, participants are interactively challenged and encouraged to surpass their own marks. 73 Fitzgerald et al 74 compared intrinsic motivation levels between EXG and conventional therapy and reported similar effects on balance. However, the EXG group obtained higher levels of intrinsic motivation. 74 This is important, given that EXGs can help improve adherence to physical activity in older people through greater enjoyment, motivation and social interaction than can conventional physical therapy. 73
Limitations and Strengths
Our systematic review with meta-analysis had certain limitations: (i) the number of studies included in the meta-analyses was low, which limits the statistical power and generalizability of the results; (ii) the risk of bias was moderate, most studies presented some concerns, and only a few demonstrated a low risk; (iii) only one study reported the intensity of EXG interventions; and (iv) the duration of the interventions did not exceed 12 weeks, which underscores the need for longer-term research to examine the chronic effects of EXG. On the other hand, the strengths of our systematic review include (i) a methodological quality above 60% in the analyzed studies; (ii) the use of methodological processes governed by PRISMA, PROSPERO, TESTEX, RoB 2, and GRADE; (iii) the use of 6 generic databases: PubMed, Medline, CINAHL Complete, Cochrane library, Scopus, and Web of Science (core collection); (iv) the performance of meta-analyses by subgroups according to training dose; and (v) the comparison of subgroups according to the type of conventional physical therapy.
Practical Applications
Physical and occupational therapists can now be confidently able to incorporate EXG as either a supplement to or a replacement for conventional exercise. The beauty of EXG lies in its ability to keep patients engaged, increasing their motivation and commitment to therapy. This engagement translates to tangible benefits: better balance, fewer falls, and an overall improvement in the patient’s physical fitness. In addition to clinical settings, there is a significant opportunity to develop EXG programs that can be performed at home. With the right guidance, older people can use readily available gaming consoles such as the Nintendo Wii or Xbox Kinect to follow exercise routines designed to improve their balance and mobility. This approach not only makes exercise more accessible but also empowers older people to take control of their health and maintain their independence.
Community-based wellness programs are another area ripe for EXG integration. Community centers, senior living facilities, and retirement homes offer group EXG sessions. These sessions provide a fun and social environment, encouraging older people to stay active while fostering social connections. The benefits here are twofold: improved physical health and enhanced social well-being. Personalization is key to maximizing the effectiveness of EXG. By carefully assessing an individual’s physical fitness, frailty status, and cognitive function, we can tailor EXG programs to meet their needs. This personalized approach ensures the therapy is safe and optimized to deliver the best possible results.
Finally, telehealth offers a way to extend the reach of EXG even further. By incorporating EXG into telehealth platforms, we can deliver remote rehabilitation services to those with difficulty accessing traditional care. Remote monitoring and feedback mechanisms can ensure that exercises are performed correctly and safely, leading to better patient outcomes and reduced healthcare costs.
It is important to remember the systematic review’s findings on dosage and frequency. EXG appears most effective in moderation—fewer than 3 sessions a week, each lasting less than 50 min. This insight is crucial for designing practical interventions that balance effectiveness and feasibility.
The systematic review with meta-analysis also sheds light on the type of conventional therapy being compared. Compared with conventional PT, EXG resulted in particularly significant improvements in the TUG test, suggesting that it may be a superior alternative in some cases. However, compared with MCT, the differences were less pronounced, indicating that both approaches can be effective.
Moreover, EXG has a notable psychological impact. It can increase confidence in daily tasks that require balance, which is particularly important for older people, who may fear falling. This increase in confidence can significantly improve their quality of life and independence. While the systematic review has limitations, such as the relatively small number of studies included and some concerns about bias, the overall methodological quality was high, and the findings are compelling. Future research should focus on longer-term studies to better understand the chronic effects of EXG and refine our intervention strategies.
Conclusion
EXG is an alternative therapy that improves balance by reducing the fall risk, as measured by the Mini-BESTest, TUG, and FES-I, compared with conventional physical therapies (ie, PT, balance training, strength training, aerobic training, MCT). Regarding dosage being <3 sessions per week with duration < 50 min per session leads to improvements in TUG. This is an effective alternative and minimally invasive therapy to apply in prefrail and frail older people.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251372362 – Supplemental material for Benefits of Exergaming Regarding to Conventional Physical Therapies on Balance and Fall Risk in Prefrail and Frail Older People: A Meta-Analysis of Randomized Controlled Trials
Supplemental material, sj-docx-1-inq-10.1177_00469580251372362 for Benefits of Exergaming Regarding to Conventional Physical Therapies on Balance and Fall Risk in Prefrail and Frail Older People: A Meta-Analysis of Randomized Controlled Trials by Jordan Hernandez-Martinez, Izham Cid-Calfucura, Edgar Vásquez-Carrasco, Braulio Henrique Magnani Branco, Tomás Herrera-Valenzuela and Pablo Valdés-Badilla in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580251372362 – Supplemental material for Benefits of Exergaming Regarding to Conventional Physical Therapies on Balance and Fall Risk in Prefrail and Frail Older People: A Meta-Analysis of Randomized Controlled Trials
Supplemental material, sj-docx-2-inq-10.1177_00469580251372362 for Benefits of Exergaming Regarding to Conventional Physical Therapies on Balance and Fall Risk in Prefrail and Frail Older People: A Meta-Analysis of Randomized Controlled Trials by Jordan Hernandez-Martinez, Izham Cid-Calfucura, Edgar Vásquez-Carrasco, Braulio Henrique Magnani Branco, Tomás Herrera-Valenzuela and Pablo Valdés-Badilla in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The author PVB acknowledges the National Research and Development Agency (in Spanish, ANID) of Chile for the awarded FONDECYT (code: 11220035) project.
Author Contributions
Conceptualization, J.H.-M., and P.V.-B.; methodology, J.H.-M., B.M.-B., I.C.-C., and P.V.-B.; software, J.H.-M., E.V.-C., and P.V.-B.; formal analysis, J.H.-M., B.M.-B., I.C.-C., E.V.-C., and P.V.-B.; investigation, J.H.-M., B.M.-B., I.C.-C., E.V.-C., A.G.-H, T.H.-V., B.H.M.B., and P.V.B.; writing—original draft preparation, J.H.-M., B.M.-B, I.C.-C., and P.V.-B.; writing—review and editing, J.H.-M., B.M.-B., I.C.-C., E.V.-C., A.G.-H., T.H.-V., and P.V.-B.; supervision, J.H.-M. and P.V.-B. All the authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current research are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.