
Abstract
This study aimed to identify unique social connection factors associated with cognitive impairment among older adults. Longitudinal data from the 2010 to 2020 Health and Retirement Study were used. Discrete-time survival models were applied to examine the impact of the social factors like loneliness, depression, positive and negative support from family and friends, volunteerism, attending sports or social clubs, charity work, and computer use on cognitive impairment. The sample included 15 548 adults aged 50 and older, with 11.4% living in poverty. Key factors associated with cognitive impairment were loneliness, depression, charity work, participation in sports or social clubs, computer use, positive family support, and negative family support. In adults living in poverty, depression and computer use were most strongly linked to cognitive impairment. These results underscore the need for interventions and educational programs that help older adults maintain or improve cognitive function through enhanced social connections.
● There is a well-established relationship bewteen cognitive impairment and social connection.
● Social disconnection can be a major source of chronic stress, leading to physiological changes that negative affect brain function.
● This study highlights a complex and significant relationship between various social connection factors and the development of cognivie impairment in older adults.
● Key factors influencing cognitive impairment include loneliness, depression, familiy support, participating in social activities, charitable work, and computer use.
● Social connection factors, particularly computer use and loneliness, may inform the development of targeted interventions and educational programs aimed at maintaining or improving cognitive function in older adults.
● Among older adults living in poverty, depression and computer use were especially influential. Addressing depression in this populatuion may help mitigate the risk of cognitive decline.
Introduction
Cognitive decline in aging, recognized by the National Institute on Aging as a form of Alzheimer’s Disease and Related Dementias, 1 leads to functional limitations, increased falls, caregiver burden, and nursing home admissions. 2 Annually, 8% to 15% of older adults with mild cognitive impairment progress to more severe forms of dementia. 3 As the United States (US) population continues to age, understanding modifiable factors that can mitigate cognitive deterioration and improve quality of life has become increasingly important.4-6
Among modifiable risk factors, social connection and loneliness have emerged as key determinants of health. In 2023, the United States (US) Surgeon General declared loneliness to be a national public health crisis, citing its link to premature mortality, cardiovascular risk, and mental health challenges. 7 A large and growing body of literature shows that social isolation, defined as an objective lack of contact, and loneliness, which is the subjective perception of being disconnected, are independently associated with accelerated cognitive decline, depression, and reduced life satisfaction.8-21
The COVID-19 pandemic further exposed and intensified the health risks associated with loneliness and social isolation.22-24 Social distancing mandates disproportionally affected older adults, reducing both formal and informal interactions.
In addition to age and gender, socioeconomic status (SES)—for example, income, education, and insurance status—shapes the relationship between social connection and cognitive health. 25 Lower SES is linked to barriers in education, healthcare access, and nutrition, and often intersects with early life adversity and chronic stress that are known to accelerate cognitive aging. 8 Racial and ethnic minority groups, people experiencing financial insecurity (ie, unemployed, uninsured, lower income), and individuals managing chronic health conditions (including depression), are especially vulnerable to both social isolation and cognitive impairment. 26
While previous studies using Health Retirement Study (HRS) data have shown the impact of loneliness and social isolation on cognitive function,18,19,27,28 few have assessed a broader set of social connection dimensions, including social participation, digital communication, and computer use, particularly in the context of poverty and major societal disruptions like the COVID-19 pandemic. Our study addressed this gap by examining how various dimensions of social connection associate cognitive decline among older adults. The primary focus of this study was to explore the complex interplay between social connection and cognitive impairment. We aimed to identify key social connection factors associated with the development of cognitive impairment in aging, and how these factors differ by poverty status, particularly in the context of the COVID-19 pandemic and demographic factors. We hypothesized that certain social connection factors, such as loneliness or depression, are associated with cognitive impairment, regardless of poverty status.
Methods
Study Population and Data Source
We conducted a secondary data analysis using publicly available cohort study data from the HRS, a nationally representative biannual longitudinal panel survey. The HRS, which began in 1992, follows individuals aged 50 years and older with biannual interviews. A core questionnaire collects detailed data on health, income, and other topics, complemented by a questionnaire on family relationships. The HRS employs a complex, multi-stage national probability sampling, with intentional oversampling of Blacks and Hispanic individuals, as well as Florida residents. A new cohort of individuals aged 51 to 56 is added every 6 years. Sample weights are used to correct for unequal selection probabilities and to adjust for survey nonresponse and post-stratification, aligning the HRS sample with national population benchmarks such as Current Population Survey (CPS), American Community Survey (ACS), and National Health Interview Survey (NHIS). Initial interview rates are approximately 73%, with follow-up response rates ranging from 80% to 90%. To produce national estimates, HRS harmonizes key variables across the ACS, CPS, and NHIS (eg, age, birth year, gender, education level, race/ethnicity, and self-rated health). For detail, see Fisher and Ryan. 29
Our study included older adults who were interviewed between 2010 and 2020. Half of the participants were asked to complete the Leave Behind (LB) survey in each panel, while the other half completed it in the following panel. This design allowed each individual to answer the LB survey approximately every 4 years. The inclusion criteria were: (1) older adults aged 65 or older; (2) participation in the LB survey at least once between 2010 and 2020; and (3) completion of cognitive tests. Participants were excluded if they had cognitive impairment, Alzheimer’s disease, or dementia at the start of the study. Among the 28 057 respondents who answered at least 1 HRS survey during the study period, 8672 were excluded for not completing the LB survey at least once. Of the remaining 19 385 who completed the LB survey, 3837 were removed due to baseline cognitive impairment, Alzheimer’s disease, or dementia, leaving a total of 15 548 participants. Figure 1 presents a flow chart of the final analytic sample.
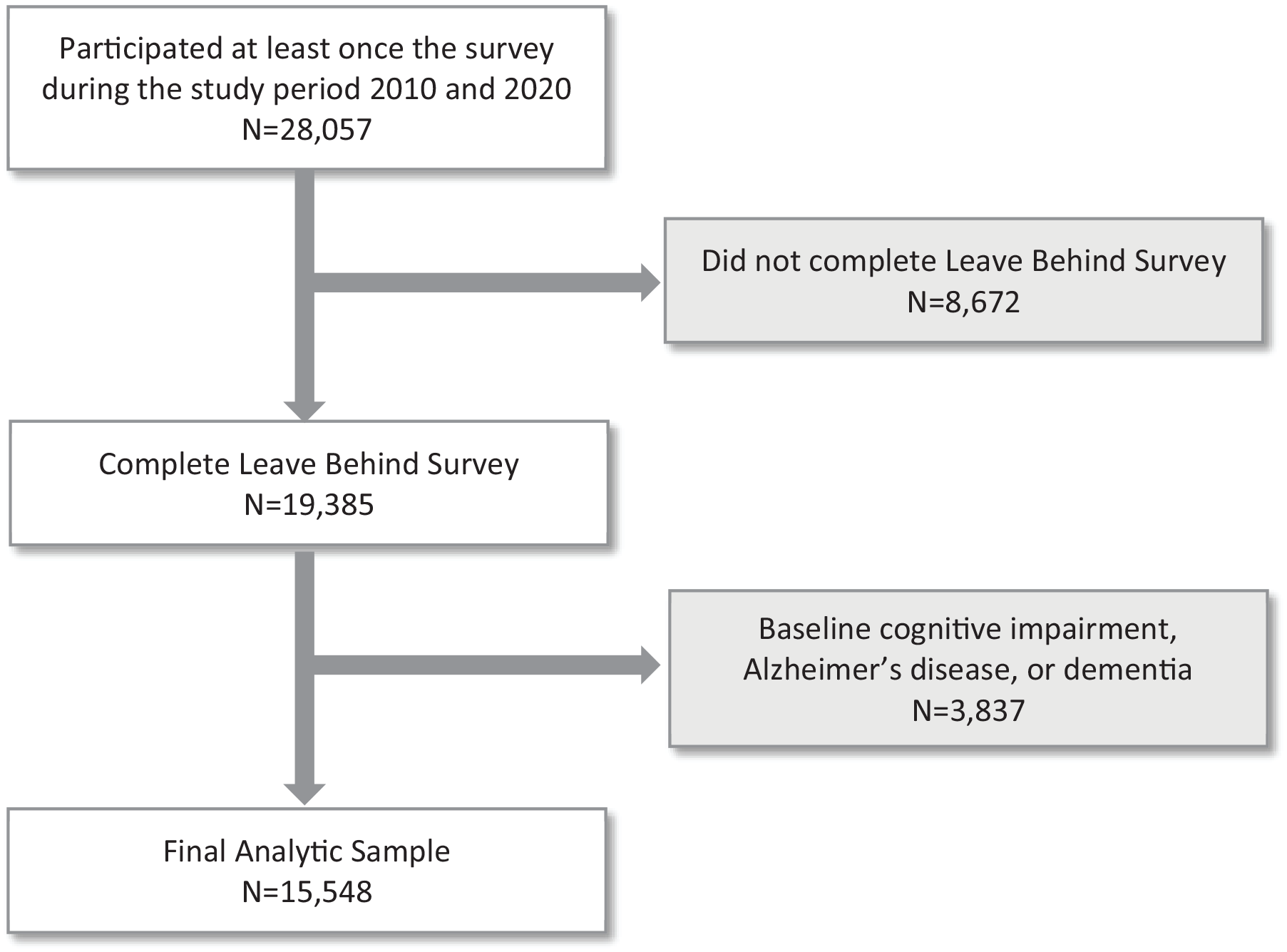
Flow chart of final analytic sample.
Variables
The following variables in the HRS were used for this study.
Cognitive Impairment
Cognitive function was assessed using the 27-item Langa-Weir Classification Scale (range: 0-27). The scale includes (1) immediate and delayed 10 nouns to assess memory (0-20 points); (2) the serial 7’s subtraction test to assess working memory (0-5 points), and (3) backward counting from 20 to assess processing speed (0-2 points). The tasks collectively measure aspects of executive functioning. 30 Cognitive impairment was defined as a score less than 12 (1 = Yes, 0 = No). 27 Participants completed these cognitive tests in each wave, providing biannual data for this measure.
Social Connection Variables
The following variables were included for social connection variables: loneliness, the Centre for Epidemiological Study Depression (CES-D) scale, positive family support, negative family support, positive friend support, negative friend support, and 9 single social participation items. These social connections variables, except for the CES-D, were collected in the LB survey, indicating data are available every 4 years.
Loneliness was composed of 11 items: lack of companionship, feeling left out, feeling isolated from others, being in tune with others, feeling alone, having people you can talk to, having people you can turn to, having people understand you, having people you feel close to, feeling part of a group, and having a lot in common with people. 31 Each item was scored as “1 = often,” “2 = some of the time,” and “3 = hardly ever or never.” Some items were reverse-scored, and the average was calculated. It ranges from 1 to 3, with higher scores indicating greater feelings of loneliness. It has a good reliability (Cronbach’s alpha = 0.88 in 2020).
The CES-D consists of 8 items: felt depressed, everything was an effort, sleep was restless, was happy (reversed), felt lonely, felt said, could not get going, and enjoyed life (reversed). To reduce burden, the HRS survey asked participants to respond with yes or no to each item, scoring 1 for yes. Thus, the total score ranges from 0 and 8, with higher scores indicating greater level of depression.
Positive social support consisted of 3 items, while negative social support included 4 items. Each item was rated on a scale from 1 to 4, where “1 = a lot,” “2 = some,” “3 = a little,” and “4 = not at all.” There were 2 domains for each type of social support—family and friend—resulting in a total of 4 domains. The positive support items include: family members/friends understand me, I can rely on them if there is a problem, and I feel comfortable opening up to them. Negative support items included: they place too many demands on me, they criticize me, they let me down, and they get on my nerves. Scores were calculated by reversing the ratings for the items, with higher scores indicating greater positive or negative support. Positive social support ranged from 1 to 12, while negative social support ranged from 1 to 16. Both measures demonstrated good reliability, with Cronbach’s alphas ranging from 0.77 to 0.84 in 2020.
The social participation variables were: (1) caregiving for a sick or disabled adult, (2) doing activities with grandchildren, (3) charity work, (4) attending an educational or training course, (5) attending sports or social clubs, and (6) using a computer for email, internet, or other tasks. Each item was scored on a 7-point Likert scale (1 = never-7 = daily). We also included another item scored on a 6-point Likert scale—writing emails to a friend (1 = less than once a year or never to 6 = 3 or more times a week). These variables were reverse-scored to indicate that a higher score reflects greater strength of the variable.
Covariates
For demographic variables, age, gender, education, race/ethnicity, marital status, and poverty status were included. Race/ethnicity was defined as Non-Hispanic (NH) White, NH Black, Hispanic, and Other. Education was categorized as 4 categories: less than or equal to high school graduate, associate or less than bachelor, bachelor, and graduate. Marital status was categorized as 3 groups—married or partnered; separated, divorced, or widowed; and never married.
Health-related variables considered were 8 following chronic conditions: (1) hypertension, (2) diabetes, (3) cancer or a malignant tumor of any kind except skin cancer, (4) chronic lung disease except asthma, (5) heart problems (eg, heart attack or congestive heart failure), (6) stroke or transient ischemic attack, (7) mental problems (eg, emotional, nervous, or psychiatric problems), and (8) arthritis or rheumatism.
In addition, the COVID-19 pandemic was defined as a binary variable: data from 2010 to 2018 were classified as pre-pandemic, while data from 2020 were classified as pandemic.
Data Analysis
Descriptive statistics were performed, including weighted percentages and unweighted frequencies for categorical variables, as well as weighted means and standard deviations (SDs) for continuous variables. Time-to-event analyses were conducted with cognitive impairment as the event of interest, with death and loss to follow-up treated as censored events. Missing follow-up data on cognitive function were treated as loss to follow-up and treated as right-censored in the analysis.
Social connection and health-related variables, as well as age and marital status, were considered time-dependent. Discrete-time survival analyses were used for the binary event, employing a complementary log-log link to calculate the hazard ratio (HR). The HR and 95% confidence interval (CI) were reported to show the strength of each variable. Both univariable and multivariable analyses were conducted, with time always included as a categorical variable. Subgroup analyses were also conducted based on baseline poverty status. To address missing data in independent variables and covariates, we conducted a sensitivity analysis using multiple imputation. Twenty imputed datasets were created, and discrete time-to-event analyses were performed on each dataset and subsequently pooled to compare with results from the complete data analyses. A P-value of less than .05 was considered statistically significant. All analyses were performed in R version 4.3.2. For the discrete time-to-event analysis, we used the svyglm function from the survey package, accounting for the HRS sampling design to reduce selection bias and ensure nationally representative estimates.
Results
The analytic data included 15 548 older adults. Table 1 presents the descriptive statistics at baseline. The weighted mean age was 63.1 years (SD = 10.0) and the weighted mean cognitive function score was 15.7 (SD = 4.4). Among the participants, 53.3% were women, 79.1% were White, 66.5% were married or partnered, 64.3% had a high school education or less, and 11.4% lived below the poverty line. The average follow-up time was 3.9 years (SD = 3.4).
Participants’ Characteristics.

Note. The number range in parentheses indicates the possible value range for the relevant variable.
N = 15 548; NH = non-Hispanic; AA = associate degree; CES-D = Centre for Epidemiological Study Depression.
Higher score indicates a stronger or more frequent presence of the variable. For example, a higher score of family positive support reflects stronger positive support from the family.
The time-to-event analysis results for the entire study sample are presented in Table 2. All social connection variables were found to be significant, except for caring for a disabled adult. In the multivariable model, the following social connection variables were significantly associated with the development of cognitive impairment: loneliness, CES-D, charity work, attending sports or social clubs, using computer, and both positive and negative family support. For each unit increase in loneliness, CES-D, positive family support, and negative family support, the hazards of cognitive impairment increased by a factor of 1.23 (95% CI = 1.16-1.41), 1.07 (95% CI = 1.04-1.10), 1.03 (95% CI = 1.01-1.05), and 1.02 (95% CI = 1.00-1.05), respectively. Notably, positive family support was positively associated with development of cognitive impairment. Conversely, charity work, attending sports or social clubs, and computer use were negatively associated with cognitive impairment, indicating that each unit increase in these factors was associated with a decrease in the hazards of cognitive impairment by a factor of 0.94 (95% CI = 0.90-0.98), 0.96 (95% CI = 0.93-0.99), and 0.84 (95% CI = 0.83-0.86), respectively.
Hazard Rates for Cognitive Impairment from Discrete Time-to-Event Model.
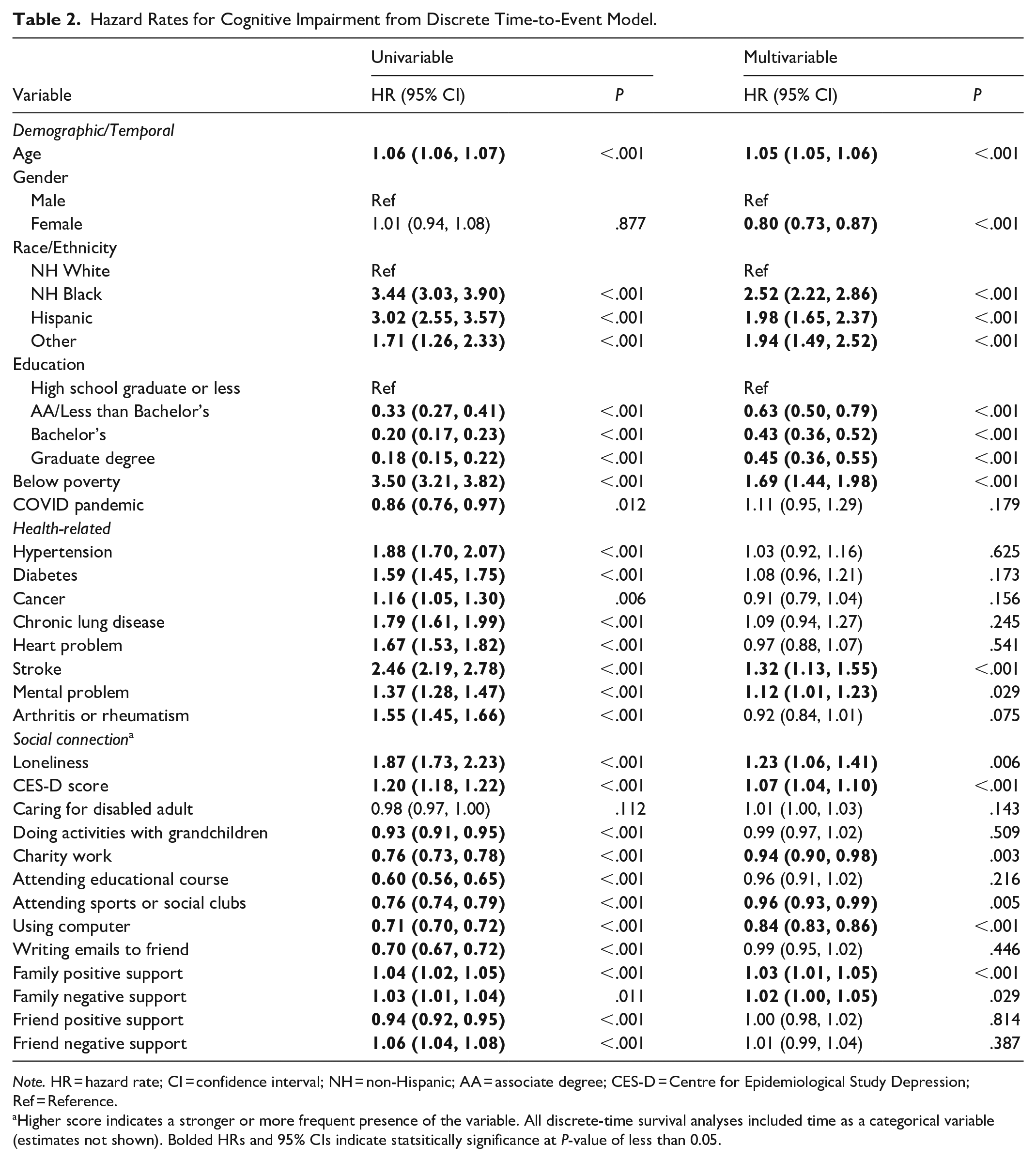
Note. HR = hazard rate; CI = confidence interval; NH = non-Hispanic; AA = associate degree; CES-D = Centre for Epidemiological Study Depression; Ref = Reference.
Higher score indicates a stronger or more frequent presence of the variable. All discrete-time survival analyses included time as a categorical variable (estimates not shown). Bolded HRs and 95% CIs indicate statsitically significance at P-value of less than 0.05.
Regarding covariates, age, gender, race/ethnicity, poverty status, education, chronic lung diseases and the COVID pandemic were significant risk factors for developing cognitive impairment. Notably, the risk of cognitive impairment was 1.69 times higher for individuals below the poverty line (95% CI = 1.44-1.98). The risk was 2.52 times higher for NH Black individuals (95% CI = 2.22-2.86), 1.98 times higher for Hispanics (95% CI = 1.65-2.37), and 1.94 times higher for Other racial/ethnic group (95% CI = 1.49-2.52), compared to NH Whites. Individuals who ever had a stroke or mental problem had a higher risk of developing cognitive impairment (stroke: HR = 1.32, 95% CI = 1.13-1.55; mental problem: HR = 1.12, 95% CI = 1.01-1.23).
Table 3 presents the results from the subgroup analyses based on poverty status. Similar to the multivariable model for all participants, the same set of social connection variables were significantly associated with the development of cognitive impairment: loneliness, CES-D, charity work, attending sports or social clubs, and both positive and negative family support. The HRs of these variables were consistent with those observed in the multivariable model for all participants. However, the final model for individuals below the poverty line included 5 variables: age, race/ethnicity, education, CES-D, and computer use. The hazard of cognitive impairment increased by a factor of 1.07 (95% CI = 1.03-1.12) for each unit increase in CES-D, while it decreased by a factor of 0.84 (95% CI = 0.81-0.88) for each unit increase in computer use.
Results from Subgroup Analyses by Poverty Status.

Note. HR = hazard rate; CI = confidence interval; NH = non-Hispanic; AA = associate degree; CES-D = Centre for Epidemiological Study Depression; Ref = reference.
Higher score indicates a stronger or more frequent presence of the variable. The discrete-time survival analyses included time as a categorical variable (estimates not shown). Bolded HRs and 95% CIs indicate statsitically significance at P-value of less than 0.05.
Missing data rates for the variables ranged from 0% (for age) to 23.4% (for friend negative support). We used the multiple imputation to handle missing data (Table 4). The results were similar to those obtained from the complete-case data analysis in terms of magnitude and significance. A few variables emerged as statistically significant. Specifically, chronic lung disease was significantly associated with cognitive impairment among older adults living above poverty line and in the overall sample. In addition, caring for a disabled adult was significantly associated with cognitive impairment among older adults living in poverty (HR = 1.05, 95% CI = 1.02-1.09).
Sensitivity Analysis: Results from Multiple Imputation.

Note. HR = hazard rate; CI = confidence interval; NH = non-Hispanic; AA = associate degree; CES-D = Centre for Epidemiological Study Depression; Ref = reference.
Higher score indicates a stronger or more frequent presence of the variable. The discrete-time survival analyses were used on 20 imputed datasets, adjusting for the complex sampling design. Bolded HRs and 95% CIs indicate statsitically significance at P-value of less than 0.05.
Discussion
Our study aimed to deepen our understanding of how different aspects of social connection are associated with cognitive impairment, using data from the 2010 to 2020 HRS. We also sought to explore the potential implications for socioeconomically disadvantaged populations. Our findings highlight a complex and significant relationship between social connection factors—specifically loneliness and social participation—and the development of cognitive impairment in older adults. Loneliness, along with depression as measured by the CES-D, was found to worsen cognitive function. This can be explained by the Social Stress Model 32 which provides a useful framework for understanding these dynamics. According to the model, social disconnection can act as a major source of chronic stress, triggering physiological changes that negatively impact brain function. Loneliness and reduced social engagement can create a feedback loop of stress and cognitive deterioration, underlining the need for interventions or education that promote stronger social connections among older adults.
These findings highlighting the multifaceted impacts of social isolation and loneliness are consistent with prior literature. A scoping review by Kassam and McMillan found that social isolation and loneliness during the pandemic were correlated with cognitive decline. 23 Similarly, Clair et al found associations between perceived isolation and reduced life satisfaction, work-related stress, and lower trust in institutions. 24
The lack of social connection can lead to chronic stress, inflammation, and unhealthy lifestyle choices such as poor diet, lack of exercise, and disrupted sleep, all of which can accelerate cognitive aging.33-36 Loneliness and isolation are also linked to depression and anxiety, 37 which further contribute to cognitive impairment. Moreover, loneliness and social isolation have been shown to affect brain regions involved in emotional processing and cognition.10,20,21,38-40
Recent longitudinal research emphasizes how changes in social isolation and loneliness affect health. Using 12 years of Korean Longitudinal Study of Aging data, Kim and Hwang found that transitions into social isolation due to a lack of informal contact or loneliness led to significantly greater cognitive decline that the benefit of transitioning out of these states. 41 These findings suggest that preventing the onset of disconnection may be more effective than attempting to reverse it later in life. Another study using Korean Longitudinal Study of Aging found that prolonged isolation across multiple time points was strongly associated with desecrated life satisfaction in older adults, especially women. 42 These findings underscore the disproportionate burden of gender with chronic social disconnection and point to the importance of early, sustained interventions. Consistent with this longitudinal evidence, our findings reinforce that factors such as computer use and participation in social or sports clubs may serve as protection against cognitive decline, particularly among older adults in poverty.
The negative relationship between computer use and cognitive impairment is perhaps unsurprising, given its likely association with educational level and higher socioeconomic status. However, it is worth emphasizing, particularly in today’s increasingly technological world. Computer and internet use can not only support the performance of other instrumental activities of daily living (IADLs) but also facilitate familial and societal interactions. Although we cannot be certain that computer use reported by the participants was for socially-related engagement, older adults are likely to use their computers or mobile devices for social connections. 43 Investigating whether interventions aimed at increasing computer use for social engagement can slow or even reverse cognitive impairment would be a valuable area of research.
Interestingly, positive family support was associated with increased cognitive impairment. This may initially seem paradoxical; family support is typically considered a positive form of social connection. However, poor health and cognitive impairment often create a need for assistance from family members, and dementias are, in part, defined by functional status impairments. Therefore, it is understandable that cognitive impairment may lead to a greater need for family support and greater stress on all involved. 44
Among various types of social participation activities, charity work and attending sports or social clubs were significantly associated with a lower risk of cognitive impairment. These activities promote social engagement, foster a sense of purpose, and provide opportunities for mental stimulation and physical activity, all of which may contribute to better cognitive health. Given these findings, incorporating charity work and social club participation into intervention programs could be highly beneficial in preventing cognitive decline and dementia. By encouraging older adults to engage in these social activities, we can help build stronger social networks, reduce isolation, and create a more supportive environment that enhances overall cognitive well-being. Such interventions could play a critical role in public health strategies aimed at improving cognitive outcomes among older populations.
In our subgroup analysis, we found only computer use and CES-D were the significant social connection variables associated with the development of cognitive impairment among older adults in poverty. Socioeconomically disadvantaged individuals often experience lower levels of social connection and face an elevated risk of cognitive decline compared to more affluent groups.45-48 Despite growing recognition of social connection as a national public health priority, and the well-documented disparities affecting socioeconomically disadvantaged populations, the relationship between various dimensions of social connection and cognitive impairment in these groups remains largely underexplored. Given the ongoing challenges posed by the pandemic, further research is needed to better understand these dynamics and inform targeted interventions for vulnerable populations.
It is important to note that individuals living below the poverty line did not show associations between loneliness, family support, and cognitive impairment. The reasons for this remain unclear. For example, it may be presumptuous to assume that those below the poverty line have less supportive family members than those living above it. It is plausible that individuals in poverty face more urgent, unmet needs, such as lack of access to healthcare and nutritious food, which could make factors like loneliness and family support less significant in comparison. Further research in this area would be beneficial to better understand these dynamics.
Limitations
There are several limitations to our study. First, the data from the HRS are based on interviews, which are susceptible to recall bias. Second, the time-to-event was conducted using longitudinal data, with the LB surveys being administered approximately every 4 years alternatively. As such, this relatively long interval between surveys could miss important fluctuations or early signs of cognitive decline or shifts in social engagement that could be associated with the outcomes. As a result, the analysis may not fully reflect the dynamic and potentially rapid nature of these changes. Third, some data would benefit from additional context; for example, more detailed information on race and ethnicity would be useful. Fourth, computer use encapsulates a wide range of activities, each with different cognitive and social demands. For instance, watching a movie requires different skills than organizing a group on social media, but such nuances are not captured in the HRS data. Fifth, we acknowledge that the study may not account for important potential confounding factors due to the limited number of variables available in the HRS. While the analysis adjusts for several covariates, other relevant factors—such as ApoE4 gene, socioeconomic disadvantage, personality traits, or access to healthcare—could be also associated with both social engagement and cognitive outcomes. Further research is needed to explore with potential confounding variables. Sixth, multiple imputation assumes that data are missing at random. Although the results from multiple imputation and complete case analysis were similar, it is possible that the missing data were not missing at random. Lastly, a longer study period may be beneficial. Since 2020 marked the beginning of the COVID-19 pandemic, it is possible that the full effects of prolonged isolation were not fully realized at that time.
Despite these limitations, our study has a strength. We explored various dimensions of social connection using the HRS, a large, nationally representative longitudinal dataset. The comprehensive nature of the HRS data offers valuable insights into factors that have not been extensively studied concerning cognitive impairment among older adults.
Conclusion
Our study identified several factors significantly associated with the development of cognitive impairment in adults aged 50 and older. Specifically, loneliness, depression, and family support - both positive and negative - along with engagement in social activities, charity work, and computer use, all played notable roles. Of particular interest, a subgroup analysis of adults living in poverty revealed that depression and computer use were especially important in predicting cognitive decline. These results underscore the complex interplay of social, psychological, and behavioral factors in cognitive health, suggesting that interventions and educational programs targeting mental health and social engagement may help reduce the risk of cognitive impairment in older adults.
Footnotes
Ethical Considerations
This study is a secondary analysis of publicly available data from the Health and Retirement Study (HRS). The HRS data are de-identified and made accessible to researchers under the study’s data use policies.
Consent to Participate
As this study does not involve direct interaction with human participants or the collection of new data, obtaining individual consent was not required. The University Ethics Committee approved this project as non-human subjects research (Committee reference number: 2023-00686). The raw data can be accessed through the Health Retirement Study site (![]() ).
).
Author Contributions
E.L., D.T., J.D., and K.J.K were responsible of the study conceptualization; E.L., J.D., and K.I. acquired data and conducted data analysis; and E.L. and M.U wrote the main manuscript text. All authors reviewed and critically edited the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by PIKO Admin Supplement (U54GM138062) from the National Institute of General Medical Sciences and in part by Ola HAWAII (U54MD007601) from the National Institute on Minority Health and Health Disparities. The authors confirm that the funding sources have had no involvement in the conduct of this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.