
Abstract
Effective medication management is essential for preventing complications and improving quality of life in individuals with chronic diseases. A comprehensive approach is required to support patients in improving their medication adherence. This study aimed to develop and validate personalized interventions, using technological tools, designed to support medication habit formation in patients with diabetes. The development process was guided by the Medical Research Council’s framework, which includes phases of development, intervention design, feasibility testing, and recommendations for future research. Twenty-five experts in healthcare and psychology were invited and participated in the evaluation. To illustrate the intervention, a 5-min video was produced, showcasing a patient’s experience through screen captures of individual components. The evaluation encompassed content validation, usability and usefulness assessments, and qualitative feedback. Expert evaluation identified key challenges and effective features relevant to digital interventions in diabetes care. The intervention, MediHabit, was designed based on digital behavior change principles and habit formation theories. It begins with personalized sessions aimed at establishing a consistent medication-taking routine. Direct and indirect cues are subsequently delivered via a mobile app and a smart medication dispenser, synchronized to ensure accurate and timely medication administration. Patients can self-monitor their adherence and receive motivational messages as rewards. Expert validation emphasized the strengths of customizability and individualization, affirming the content’s relevance and the app’s usability. However, experts also noted the need for improved accessibility across age groups and more meaningful use of patient-generated data. The findings indicate that the MediHabit intervention holds promising potential for improving medication adherence among diabetic patients. Further research is needed to evaluate its real-world effectiveness, long-term impact, and scalability across diverse populations.
Highlights
• The economic burden of diabetes mellitus (DM) treatment underscores the importance of interventions that promote medication adherence. It is closely linked to habitual behavior, which can be effectively supported by digital interventions.
• This study employed the Medical Research Council framework to guide the development of a theory- and evidence-based digital intervention. Intervention components were designed and refined through a multidisciplinary collaboration.
• Expert evaluations indicated the potential of the digital intervention to foster sustainable medication-taking habits, while highlighting the need for continued refinement to maximize its effectiveness.
Introduction
Diabetes mellitus (DM) is one of the leading noncommunicable diseases (NCDs) that significantly impacts healthcare costs and mortality rates of nations. There are over 41 million people killed by NCDs causing significant burden worldwide. 1 Evidence suggests that good medication adherence is associated with improved health outcomes. These behaviors play a critical role in preventing complications and hospitalizations, which can significantly alleviate the overall healthcare burden. 2 Low medication adherence is one of the most frequent issues, as not following prescribed treatment plans lead to side effects and significant deterioration.
Medication adherence is a complex behavior that requires patients to consistently follow their prescribed regimens. 3 When addressing patient-related factors, it is crucial to consider individual behavioral patterns to ensure that interventions are both effective and accessible while meeting each person’s unique needs. According to Horne et al’s 4 perceptions and practicalities approach, nonadherence can be categorized along 2 axes: perceptual and practical factors. Unlike participants’ misconceptions about their treatment, lack of support and daily routine disruptions have been identified as key practical barriers. 5 These challenges can often be mitigated through the use of memory aids, as well as improved convenience and accessibility to medication use.
Over the last decade, for the availability and accessibility of interventions, large number of mobile apps released to assistant regular medication taking of individuals. 6 Diverse features of apps were used to deliver education and assistance with reminders being the most frequently applied tool to support individuals in taking their medication on time.7 -9 Although the effectiveness of medication adherence interventions is evident, there are concerns about the short-lived nature of these effects. 10 Recent review studies also highlighted the ill-defined characteristics of intervention components of successful apps. 8
Habit formation can serve as a strategy for improving medication adherence in patients with chronic diseases by integrating medication routines into daily life, allowing them to occur automatically. 11 This process is explained through the cue-behavior association,12 -14 here repeated exposure to a stable cue (eg, preparing for a meal) strengthens the link to a behavior (eg, taking pre-meal medication), gradually forming a habit. Several studies highlight the importance of direct engagement in behavior.6,15,16 Context-dependent repetition is essential to habit formation, 17 requiring consistent cue-response pairings and sustained effort before the behavior becomes automatic. In addition, integrating motivational and action control techniques, such as goal setting and rewards, has been recommended to reinforce adherence. 18
Digital behavior change intervention (DBCI) has been introduced to promote individuals adopting and promoting positive behavior changes that the technology leveraged for maintenance and improvement of health behavior. 19 By leveraging mobile health technologies such as apps and other digital devices, interventions have become more tailored and interactive. 20 Moreover, meta-analyses have evidenced their greater effectiveness over in-person methods, highlighting advantages such as consistency, flexibility in time and location, and long-term applicability.21,22 In addition, various applications of DBCIs have been highlighted, including timely reminders and the detection of noncompliance.23 -26 Notably, electronic dispensers enhance medication adherence and safety, reducing the risk of misuse and overdose while optimizing oral medication use. 27
There has been a surge in mHealth apps for medication adherence, however, many existing apps lack a clear theoretical foundation, and the role of healthcare providers is often unclear. 28 Mostly adopt a one-size-fits-all approach, relying on 1-directional alerts with minimal customization, which limits their adaptability. 29 Moreover, accurately tracking actual medication intake remains a challenge, further questioning their effectiveness. 30 This study aims to develop a theory-driven intervention for medication habit formation by integrating in-person sessions, a mobile app, and a connected medication dispenser for precise adherence tracking. Developed through multidisciplinary collaboration with healthcare providers, software developers, and mechanical engineers, the intervention aims to promote long-term adherence through customizable reminders and adaptive features tailored to individual preferences and lifestyles.
Expert content validation and usability assessments were conducted to evaluate its effectiveness. The study is guided by the following research questions:
What foundational elements are necessary for a successful digital intervention to enhance medication adherence in individuals with diabetes?
What is the projected effectiveness of current interventions in fostering medication habit formation among individuals with diabetes?
Which aspects of existing interventions need to be refined and optimized for greater impact?
Method
An intervention “MediHabit” was developed by incorporating in person session, a mobile application and a dispenser to support habit formation for patients with diabetes. The development process followed the Medical Research Council’s (MRC) framework, 31 MRC suggest key elements as interactive development, contextual understanding, theory, and evidence based and continuous refinement of intervention. The process for the current study consisted of 4 phases: development, intervention design, feasibility and testing, and recommendations for future research (Figure 1). The development and feasibility and testing phases involved data and evidence generation through literature review and mixed methods research. In the development phase, literature reviews were conducted to gain deeper insights into patients’ experiences with digital interventions. In the feasibility and testing phase, a mixed methods approach involving expert participants was employed, using quantitative questionnaires, and qualitative feedback to evaluate the adequacy and usefulness of MediHabit’s content. The study adhered to relevant EQUATOR guidelines, specifically the PRISMA Extension for Scoping Reviews (PRISMA-ScR), 32 and the Good Reporting of a Mixed Methods Study (GRAMMS) framework for the mixed methods study. 33

Key elements of development and testing process based on MRC.
Phase 1 Development
Identifying the Evidence Base
This phase involved conducting both qualitative and quantitative reviews to gather evidence supporting the intervention including: (a) digital interventions designed for medication adherence, (b) factors influencing effectiveness, and (c) user experience.
A systematic review and meta-analysis were conducted to gather evidence on the quantitative effectiveness of specific features of digital interventions, as described in a published article. 30 Eight databases (EMBASE, PubMed, Cochrane Library, CINAHL, KISS, KoreaMed, RISS, and NDSL) were searched for articles published between 2013 and 2023 in English or Korean. The search terms “chronic disease,” “mobile application,” and “medication adherence” were used. The study included randomized controlled trials that investigated digital interventions aimed at improving medication adherence. Eligible studies focused on individuals taking medication for chronic diseases (P), employed app-based interventions (I), reported outcomes related to medication adherence (O), and were published in English or Korean. Each component was then analyzed quantitatively using Comprehensive Meta-Analysis (CMA) software, reporting standardized mean differences (SMDs), odds ratios (ORs), and confidence intervals (CIs).
Additionally, a separate electronic search and review of qualitative studies were conducted to gather evidence on effective approaches for engaging patients with digital and mobile interventions. This search was performed in Medline (via ProQuest) using the keywords “Digital,” “Mobile,” “mHealth,” “Health,” “Medication adherence,” “Experience,” and “Qualitative.” This review focused on patients’ challenges and suggestions for areas needing improvement to enhance user experience with mobile or digital technology-based interventions for medication adherence. Studies published in English or Korean between 2014 and 2024 were included if they met the following criteria: original research employing qualitative methods; focused on the perspectives of patients or caregivers taking medication for chronic diseases (P); utilized digital technologies aimed at supporting medication adherence (I); and reported qualitative data on user experiences and needs (O). Studies that reported only quantitative outcomes, as well as systematic reviews, meta-analyses, conference abstracts, and editorials, were excluded.
Phase 2 Intervention Design
Selecting Appropriate Theoretical Frameworks
The researcher examined major theories related to habit formation and behavior change, establishing selection criteria to encourage habit formation and improve medication adherence within a digital health environment. The first criterion for selecting a theory was whether the framework effectively supports the repetition of specific behaviors to facilitate habit formation. The second criterion was the alignment between digital technology features and behavioral goals. Given the nature of digital health tools, technological features need to be closely connected to the user’s behavioral objectives to maximize effectiveness. 34
Integrating Evidence and Theoretical Insights into Actionable Components
In this phase, the intervention components were structured into actionable elements designed to achieve optimal outcomes, with an approach that incorporated both in-person and digital interventions. A multidisciplinary team was formed to involve key stakeholders, including healthcare experts, software developers, a mechanical engineer, and a health practitioner who is also a chronic disease patient. This team collaboratively organized the intervention components and integrated digital health features. Through several co-creation workshops, the team developed appropriate technological tools and strategies to support the intervention components and address identified issues based on evidence. These workshops facilitated the development and maintenance of the intervention by incorporating input from a diverse range of stakeholders, ensuring that the solutions were both practical and well-informed. By applying theoretical principles, the roles of each component within the intervention were determined. The features of the mobile app and medication dispenser were aligned at an actionable level, with detailed descriptions of how each feature supports the formation of consistent medication habits.
A
The
Phase 3 Feasibility and Testing
This phase involved expert evaluation of a habit formation intervention. To facilitate understanding, the entire intervention process was filmed, demonstrating step-by-step procedures including the creation of routines, setting of goals, selecting alarms, placing the dispenser device, and using the mobile app to monitor medication intake and disease management indicators. The remaining features of the app were also described in detail, with explanations on how they assist in medication management. Structured questionnaires were administered to expert participants, comprising 2 main parts: 1 assessing the content validity of the intervention and the other evaluating its perceived usability and usefulness. Experts rated each item using a Likert scale and were also provided space to offer qualitative feedback, including justifications for the necessity of specific content, concerns, and suggestions for improvement.
Participants
This study was approved by the Institutional Review Board (IRB) of Mokpo National University in Korea (MNUIRB-240527-SB-009-01). Informed consent was obtained from all expert participants, and measures were implemented to ensure the anonymity of responses and the secure storage of all data. A total of 25 experts were recruited through purposive sampling. Inclusion criteria required participants to have at least 5 years of experience in healthcare or psychology, either through clinical practice or academic research. For healthcare professionals, direct experience in diabetes care was also required. Recruitment and data collection were conducted between August and November 2024.
The sample size was determined to identify at least 80% of usability issues, based on findings from previous studies.36,37 A total of 25 participants was deemed sufficient to ensure reliable results and accommodate potential variability and participant dropout, especially for usability testing based on ISO standards. Video demonstrations of the intervention were emailed to participants prior to the evaluation to ensure a consistent understanding of the intervention procedures.
Content Validity Evaluation
To assess the relevance of the intervention content, the Content Validity Index (CVI) was used. Experts evaluated 35 items in total. Of these, 27 items were assessed using a 4-point Likert scale: 1 = not relevant, 2 = revision required, 3 = relevant, and 4 = extremely relevant. In addition to these scaled items, 7 qualitative items were included to gather detailed feedback and suggestions for future research and intervention improvements. One multiple-choice item asked participants to select the most effective type of reminder for individuals developing a medication habit. The CVI for each item was calculated by dividing the number of experts who rated the item as either 3 or 4 by the total number of participants. Items with a CVI above 0.90 were considered excellent, those between 0.78 and 0.90 were acceptable, and those below 0.78 were identified as needing revision, in line with established benchmarks.38 -40
Usability Evaluation
The perceived usability of the intervention was evaluated using a 25-item structured questionnaire that integrated elements of the ISO usability framework and the System Usability Scale (SUS). 37 The questionnaire covered 3 key areas. First, 8 items assessed the ease of use of both the mobile app and the medication dispenser. Second, 6 items evaluated the practicality of the intervention, its usefulness in supporting habit formation, and its overall positive impact on medication adherence. Third, 11 items focused on individual features of the intervention components, including the workbook, the mobile app, and the dispenser device. This comprehensive evaluation aimed to capture both functional usability and subjective user perceptions.
Data Collection and Analysis
After obtaining informed consent, researchers emailed the evaluation materials to participants, which included the intervention videos and structured questionnaires. Participants completed the survey and returned it via email. Quantitative data were analyzed using SPSS version 27.0 (SPSS Inc., Chicago, IL), with descriptive statistics such as frequencies, percentages, means, and standard deviations calculated to summarize expert responses. Qualitative data were analyzed using thematic analysis, following an inductive and data-driven approach. Two researchers independently reviewed the qualitative responses, identifying key phrases and grouping them into themes and subthemes. Discrepancies were resolved through discussion with a third researcher. The analysis followed 5 structured phases: familiarization with the data, initial coding, categorization of related codes, refinement of emerging themes, and naming of final themes.
Phase 4 Recommendation for Future Research
This phase of the process focused on refining the intervention through iterative analysis of collected data and expert feedback. Additional co-creation workshops were conducted to further optimize the intervention and revise its components as needed. This iterative approach is designed to identify areas for improvement, ensuring the intervention is effectively tailored for practical end-user application. Ultimately, these efforts aim to establish the intervention’s conclusive effectiveness.
Results
Phase 1 Development
Identifying the Evidence Base: Summary of the Findings of the Review of Effectiveness of Prior Digital Interventions
A systematic review and meta-analysis of 26 RCTs involving 5174 individuals with chronic diseases. Based on articles published between 2013 and 2023, found that mobile health interventions appear to improve medication adherence and reduce the incidence of missed doses. The most frequently used technologies were reminder systems, followed by interactive strategies, data-sharing capabilities, and pill dispensers. The effectiveness of mobile app features was specifically examined, revealing through subgroup analyses that interactive strategies, advanced reminders, and data-sharing capabilities significantly improved medication adherence among patients with chronic diseases. Further details are available in the published article. 30
Summary of Findings of Prior Qualitative Studies of Patient Experience on Digital Intervention
Another literature review was conducted, retrieving 1,191papers, of which 9 were included for analysis (Appendix 1).41 -49 From the individual studies, themes and subthemes were extracted and organized to identify factors that could strengthen and reinforce previous digital interventions, with the aim of optimizing the patient experience, and enhancing the effectiveness of medication adherence. The articles related to patients’ experiences with digital interventions using mobile apps or medication dispensers were reviewed in terms of challenges and requirements (Appendix 2). Findings identified common barriers to medication adherence, including forgetfulness, changes in daily routines, and complex medication regimens. Participants suggested improvements for digital interventions, emphasizing the need for simplicity, ease of use, reliability, customizability, and larger medication storage capacity. Additional inquiries into preferred features highlighted the importance of reminders, monitoring (data tracking), personalized information, and interventions to help establish consistent medication habits (Appendix 3).
Phase 2 Intervention Design
Selecting Appropriate Theoretical Frameworks
Based on discussions among health experts and faculty members, theoretical frameworks were determined to best support the research goals, addressing both behavioral sustainability, and digital integration. The primary criterion for selecting a framework was its effectiveness in facilitating the repetition of specific behaviors while ensuring consistent performance without lapses. Reviewing habit theory, habits are formed through the contextual relationship between cues and repeated behaviors, eventually leading to the automatic enactment of the desired behavior.50,51 This process requires creating an environment that facilitates habit formation by associating cues with specific consequences, the consistent execution of the behavior.50,51 In addition to cue-induced behavioral response association, rewards have been suggested as a means of reinforcing contextual stability and promoting behavioral automaticity. 52 Given the need for a structured visual representation of this process, the Habit Loop framework was reviewed. This framework outlines a cycle of cue, routine, and reward, effectively reinforcing adherence behaviors through habitual repetition. 53 The Habit Loop framework, consisting of 3 components (cue, routine, and reward) explains how habits are formed and maintained. To establish a new habit of taking medication, a consistent and reliable cue initiates the behavior, which becomes routine when it is straightforward, clearly outlined, and reinforced with a meaningful reward.
The second criterion was the alignment between digital technology features and behavioral goals. Accordingly, the DBCI framework was identified as the optimal choice due to its ability to explain mechanisms of action, clarify how digital technology induces behavior change, and assess the effectiveness of individual components, including their functioning and potential synergistic effects. 54 The DBCI framework leverages digital tools to effectively promote behavior change. Key components include personalization, monitoring, tracking, support, and education. Digital tools enable interventions that are flexible, accessible, and capable of customization and context awareness, maximizing user autonomy, and preference. This approach facilitates self-initiated medication routines, empowering users to maintain a medication habit independently. A digital intervention, including a mobile app and a connected electronic medication dispenser, was chosen to engage users in forming medication habits. These digital tools were designed to enhance medication adherence by emphasizing simplicity, usability, and usefulness, making habit formation easier and more motivating.
Integrating Evidence and Theoretical Insights into Actionable Components
By translating the “habit loop” model into actionable components, specific tools were aligned with key properties of habit theory, each serving a distinct role in supporting habit formation (Table 1). By applying the process of habit formation and reinforcing routines through cycles of cue, routine, and reward, this intervention supports critical elements of behavior change, including action planning, motivation, behavior prompts, monitoring, reinforcement, and access to resources. Additionally, several features were added during the cocreation process. Healthcare providers emphasize the importance of understanding one’s medication regimen, leading to the inclusion of an “electronic capture of prescription” feature. Recognizing the added challenges of adhering to medication routines outside one’s usual environment, an “outdoor mode” was introduced. Additionally, there is a perspective that this need for intervention aligns with other essential health behaviors, such as recording physical activities and monitoring health indicators like blood sugar levels and HbA1c.
Framework Components: Intervention Tools, Content, and Roles in Theoretical Insight.

The prototype of intervention consisted of 3 components: a workbook, a mobile app, and a medication dispenser, all structured to create a “habit loop” for taking medication, incorporating appropriate digital technologies. First, we employed 3 different cues to signal users when it’s time to take their medication: (1) linking the medication time to an existing habit, (2) customizable reminders, and (3) visual prompts from the dispenser itself. Second, medication is released through user actions, either by (1) sending a signal via the mobile app or (2) pressing a button on the dispenser. This allows users to complete their medication intake. In addition to medication, other health routines were recorded on a self-initiated basis, including steps, blood sugar levels, and HbA1C. Finally, users can track their medication status daily and monthly through a status screen or calendar.
Figure 2 outlines an intervention designed to help individuals take their medication on time using an electronic dispenser and a mobile app. The process begins by setting a new medication routine and goals, filling the dispenser with packaged doses for each intake, and connecting it to the app. Users select their preferred reminder type: a timely reminder, a delayed alarm, both, or none. With the timely reminder option, the app sends notifications at the scheduled time. If the user responds by pressing a button on the app or dispenser, the medication is dispensed, and compliance is logged. If the delayed alarm is chosen, the app issues an additional reminder if the user misses the scheduled time, giving them a chance to take their medication within an allowable timeframe before it’s considered too late. If the user doesn’t respond to any reminders, it is recorded as non-compliance. This system supports users in developing a consistent medication habit by tracking each dose taken or missed.

MediHabit intervention.
Phase 3 Feasibility and Testing
Engaging Experts to Assess Contents Validity and Usability
Table 2 presents the demographic characteristics of the expert participants. A total of 25 experts participated in the study, with an average professional experience of 17.33 ± 6.85 years. The experts panel consisted of 8 healthcare providers (5 nurses, 3 physician), patients who is also healthcare provider (n = 7), psychologists (n = 7) and research professional (n = 3). The majority were female (88%) and mean age of 42.80 ± 7.14 years.
Socio-demographic Profile of Study Participants.

Content Validity and Usefulness Results
Table 3 presents the validity index for each of the 27 intervention components, along with 2 items related to alarm types. Experts evaluated these components, with most achieving an acceptable to excellent level of CVI, demonstrating their relevance, and adequacy. However, 2 components, “No alarm option” and “Daily step tracking” failed to achieve an acceptable level of agreement among experts as a suitable intervention for medication habit formation. The CVI score for both contents was 0.68, which is below the acceptable threshold of 0.78, indicating the need for further discussion regarding modification, or elimination.
Agreement Rate of Expert Participants and Contents Validity Index.

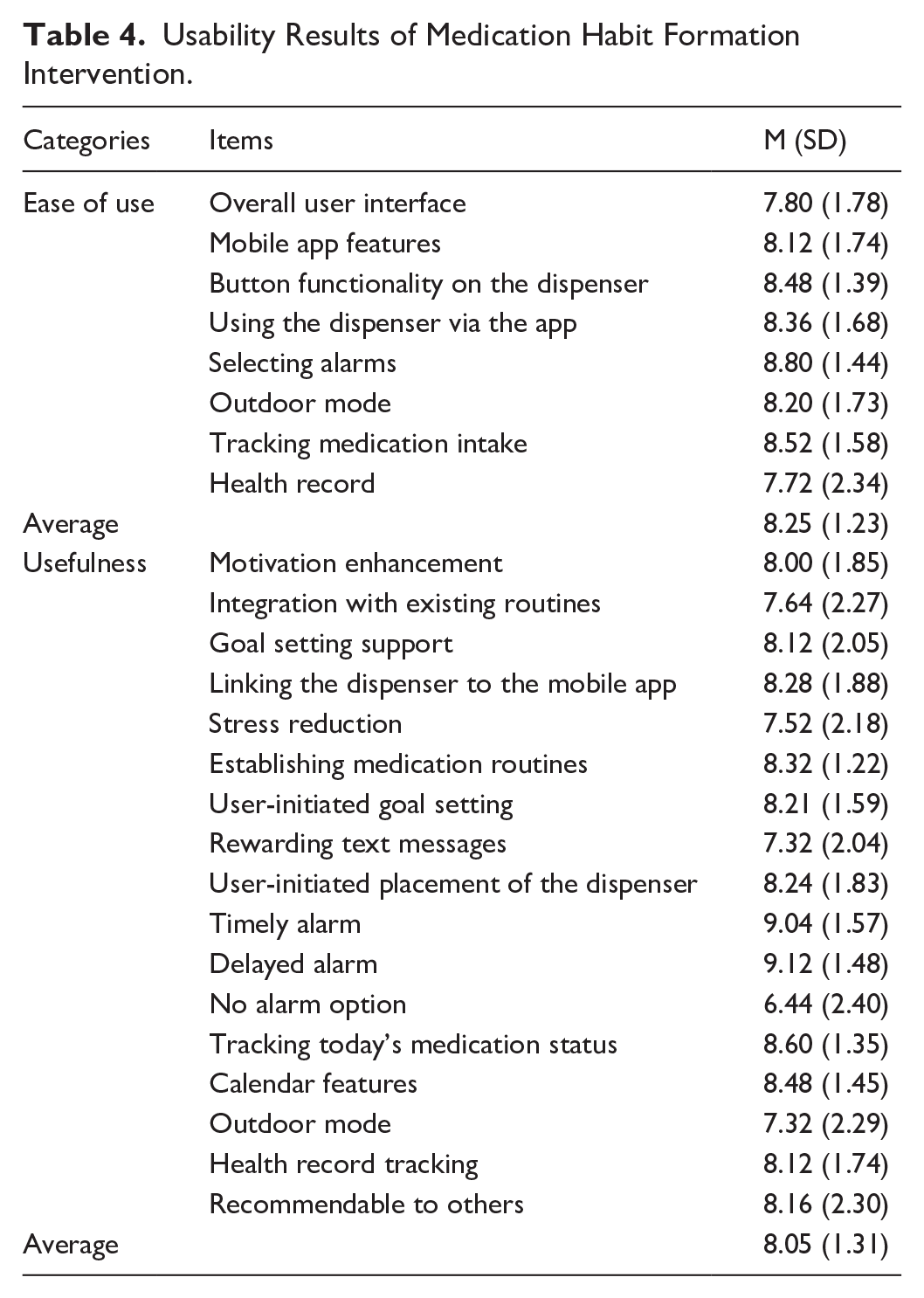
Perceived ease of use and usefulness were also assessed using 25 items (Table 4), with 72% (18 out of 25) receiving above-average scores of 8 or higher. Delayed alarm (9.12 ± 1.48) followed by timely alarm (9.04 ± 1.57) showed the highest usefulness score. The component with the lowest usefulness score was again “No alarm option” (6.44 ± 2.40), while the “Rewarding” message and “Outdoor mode” had the second-lowest score (7.32 ± 2.04) and (7.32 ± 2.29).
Usability Results of Medication Habit Formation Intervention.
Qualitative Analysis
Collecting a total of 490 responses and selecting 130 meaningful phrases for further analysis. The initial identification of 11 codes and 27 subcategories were identified and then a through further refinement, a final framework was developed, consisting of 4 themes, and 5 subthemes (Table 5).
List of the 4 Themes and 5 Subthemes with Examples of Statements.

Theme 1 Preventing Missed Doses Through Differentiated Strategies
Overall, the positive feedback highlighted the diverse strategic approaches, which were praised for being more tailored and motivational, with a strong focus on individual needs. Positive feedback on the workbook-based stage emphasized its effectiveness as a strategy for developing personalized routines that promote medication adherence efficiently and effortlessly.
Theme 2 User Convenience
The customizable alarm was praised for allowing individuals to maintain autonomy while also motivating them to take responsibility for their management behaviors. Several experts highlighted the missed alarm feature as particularly valuable, considering it an excellent solution for individuals struggling with forgetfulness, which is a common cause of medication nonadherence. The automated feedback feature was well-received for its potential to support self-regulation. Additionally, recognizing the importance of consistency in habit formation, experts regarded this feature as highly convenient and beneficial.
Theme 3 Sustained Motivation Intervention for Developing Medication Habits
Combined with personalized goals, the visualization of medication patterns and adherence was seen as an effective tool for strengthening habit formation. Experts noted that recognizing incremental achievements, from small to significant milestones, through the tracking system could help sustain optimal medication adherence over time.
Theme 4 Areas for Further Improvement
Experts expressed concerns about older users, citing their unfamiliarity with apps and potential difficulty engaging in digital interventions. To address this, they suggested incorporating family involvement to provide additional support and encouragement. Rather than offering rewards, some experts suggested providing warnings for users with poor medication adherence. They believed that such information would raise awareness about potential risks and could serve as a more meaningful motivator for improving adherence. Experts also recommended reinforcing medication confirmation, as relying solely on a medication dispenser does not guarantee that the medication has been taken. They emphasized that the current system cannot fully address the challenges of monitoring medication adherence without additional verification measures.
Phase 4 Recommendation for Future Research
The intervention for the future end-user effectiveness study was finalized in Table 6. First, the quantitative data was reviewed to identify intervention components that required revision, specifically those evaluated as “revision required,” including “no alarm” and “step tracking.” Additionally, qualitative responses were incorporated to further refine and enhance the intervention.
Intervention Modification Reflecting Expert Feedbacks.

Discussion
Guided by the MRC’s framework, current interventions focus on strategies that promote consistent medication adherence by formation of medication habit. Recognizing that habit formation is highly individual, the intervention focuses on enhancing customization and flexibility. 51 It aims to tailor the level of user involvement while providing a range of support through digital tools, ultimately engaging individuals in disease and medication management. 55 Expert evaluations confirmed the alignment of each component, with feedback highlighting both the intervention’s potential effectiveness and areas for further refinement.
The appropriateness of the intervention components was validated using the CVI, with all items scoring above 0.78, except for two components including the absence of an alarm. The alarm-related features were particularly praised for their intuitiveness and simplicity, reflecting the focus on simplicity during the development stage. Among reminder features, both timely and delayed reminders were identified as essential, while the absence of reminders received the lowest scores. Previous research on habit-based mobile interventions has demonstrated that timely reminders play a critical role in forming stronger habits, as patients are more likely to take their medication consistently when reminded on time. 56 Another explanation suggests that once a habit is established, the behavior becomes automatic, allowing patients to continue taking their medication without the need for further reminders. 56 To optimize the intervention, further analysis is planned to determine the specific time required for patients to establish a medication routine with the support of timely reminders.
Among the other features, the medication status screen scored the highest. The ability to track both taken and missed doses appears to strongly appeal to experts, as it has the potential to ensure the accuracy of adherence data. By providing objective metrics to measure the success of habit formation, 57 it fosters the sustainability of behaviors, thereby establishing a consistent routine. According to a previous review, unlike reminders, medication tracking features were only utilized in about half of mobile app interventions. 58 Future studies may explore how this data can be leveraged to further strengthen medication adherence behavior and assess whether the current presentation of tracked data is optimized for this purpose.
Unlike other lab-related monitoring features, the step-count tracking function was not well accepted. This can be attributed to its limited value as an indicator for medication management, as blood tests are widely regarded as the primary outcomes,59,60 and the insufficient robustness of walking data, which is often viewed as just 1 form of physical activity, to provide meaningful insights for disease management.61,62 Experts highlighted the need for a more robust integration of disease indicators. Therefore, the current app prioritizes the development of automated data tracking solutions and plans to integrate with additional health devices, such as blood glucose monitors, to minimize manual user input. These efforts enhance functionality, boost user engagement, and support proactive disease management. Without them, the intervention would be limited to addressing forgetfulness alone.
Further suggestions for interventions to improve medication habits emphasize the importance of leveraging family or peer support to strengthen behavior. A significant portion of the concerns focused on the elderly population, with experts highlighting challenges related to digital literacy and technology usage among older users. Although habit formation is a personal behavior, social support consistently identified as a key determinant.63 -65 This makes it crucial to incorporate strategies that integrate digital interventions with social support mechanisms to enhance adherence. Given the pivotal role that family support, 65 these insights must be thoughtfully incorporated. By addressing these considerations, further improvements can enhance the app’s usability and promote better adoption, particularly among elderly users.
The rewarding message received the second-lowest usefulness score, aligning with qualitative feedback that indicated the current reward system is weak and requires reinforcement. Several recommendations suggested leveraging data-driven awareness strategies, such as using data to alert individuals to the potential harms of non-adherence or to reinforce the benefits of good adherence through positive feedback. To raise the aforementioned awareness and serve as a form of reward, clear visualizations can be effective. 66 Emerging technologies now make it possible to present data in interactive and easily understandable formats, benefiting both experts and laypersons. 67 Future research should focus on integrating advanced visualization technologies while considering patient preferences. This approach could enhance understanding of health outcomes, improve medication adherence, and support comprehensive disease management.
Limitation
This is the first study to evaluate the content validity and usability of a habit formation intervention using a mobile app and an electronic medication dispenser. However, the study has certain limitations. First, there was no actual use of the mobile app or devices. One reviewer specifically noted the difficulty of understanding the app’s functionality without hands-on experience. While the study’s primary aim was to assess the content, this limitation arose due to restrictions on using the medication dispensers during the evaluation. Second, the participant group was unevenly composed, with experts from various fields, though participants from the healthcare sector made up the majority. The underrepresentation of participants with extensive clinical practice may have biased the results toward the usability aspects of the intervention, rather than its practical application in clinical settings. Lastly, as the app remains in the conceptual stage, we can only conclude that certain features, as evaluated by experts, have the potential to positively impact medication habit formation. However, actual patient use may yield different results, highlighting the need for ongoing research to ensure its usability and effectiveness in improving medication adherence and clinical outcomes.
Conclusion
MediHabit is a theory-driven mobile application designed to enhance medication adherence among patients with diabetes by fostering effective medication-taking habits. Based on an extensive review of the literature and robust theoretical frameworks, the app’s technical specifications were meticulously developed to ensure optimal usability and to maximize the intervention’s potential benefits. Moreover, a multidisciplinary approach was adopted, integrating user-centered design principles and iterative refinements informed by expert evaluations throughout the planning, implementation, and testing phases. Each component of the intervention was rigorously examined, with expert feedback highlighting its promise in supporting patient compliance while also identifying areas for further enhancement. Future research focused on patient perspectives will be essential to validate MediHabit’s practical efficacy and its role in improving both adherence and overall health outcomes.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251343785 – Supplemental material for Development of a Digital Intervention Incorporating Habit Formation Techniques for Medication Adherence
Supplemental material, sj-docx-1-inq-10.1177_00469580251343785 for Development of a Digital Intervention Incorporating Habit Formation Techniques for Medication Adherence by Sun Kyung Kim, Hye Ri Hwang, Kyung Seok Byun, Su Yeon Park, Su Hee Moon and Huiseok Lee in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580251343785 – Supplemental material for Development of a Digital Intervention Incorporating Habit Formation Techniques for Medication Adherence
Supplemental material, sj-docx-2-inq-10.1177_00469580251343785 for Development of a Digital Intervention Incorporating Habit Formation Techniques for Medication Adherence by Sun Kyung Kim, Hye Ri Hwang, Kyung Seok Byun, Su Yeon Park, Su Hee Moon and Huiseok Lee in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Appendix
Patient Experiences Reflected on MediHabit.

| Needs arising from patient experiences | Reflected on MediHabit | |
|---|---|---|
| Barriers on medication adherence | Forgetting | Utilizing various cues from existing habits, such as mobile reminders and placing the dispenser in a visible location, to support the new routine |
| Difficulty in changing the daily routine | A workbook as a guide for users in building a new routine. | |
| Complex regimen | Dispenser that a single dose is dispensed for each intake (not dispensing individual pills) | |
| Requirement on digital intervention | Simple | A simple UI with minimal user input required (e.g., no need to type individual medication names) |
| Reliable | Multidisciplinary development involving healthcare, computer engineering, and mechanical engineering | |
| Customizable | Customizable reminders with options for timely, delayed, or no reminder | |
| Large Storage | An electronic medication dispenser with the capacity to hold over a month’s supply of medicine. | |
| Preferred Features | Reminder | A mobile phone reminder that uses sound, vibration, and a screenshot message. |
| Monitoring | A data log for tracking and confirming medication intake. A calendar displaying reports on medication adherence and behavior. | |
| Personalized information | Frequently Asked Questions (FAQs) section. | |
Acknowledgements
We sincerely appreciate the contributions of all the study participants. This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT; RS-2022-NR070862).
Ethical Considerations
This study received Institutional Review Board (IRB) approval from M University in Korea (MNUIRB-240527-SB-009-01).
Consent to Participate
Informed consent was obtained from all expert participants, with measures in place to ensure anonymity of their feedback and secure storage of all data.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT; RS-2022-NR070862).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.