
Abstract
Maternal and child healthcare is a crucial dimension in healthcare delivery. A significant portion of government health expenditure is kept for improvement in infrastructure, service delivery and financial protection to reduce mortality and improve maternal healthcare. The current study aims at assessing the relationship between government health expenditure and maternal mortality in the South Asian context while considering expected years of schooling, fertility rate, government effectiveness, and gross domestic product as control variables. The retrospective panel data has been used from 2002 to 2020 for 8 South Asian Economies. Fixed-effect-model, Pooled-ordinary-least-square, Random-effect-model, Hausman-Test, Fully-Modified-Least-Square and Dynamic-Ordinary-Least-Square techniques have been applied for estimation. The results reveal that government health expenditure is negatively related to maternal mortality across all applied analytical models. The study concludes that a rise in government healthcare expenditure in South Asia can reduce maternal mortality.
Keywords
Highlights
● The present study highlights the relationship between government health expenditure and maternal mortality ratio in South Asia.
● The study uses fixed effect model and the robustness has been checked using FMOLS and DOLS.
● The study revealed that in South Asia, government health expenditure and government effectiveness reduces maternal mortality. This implies that increased government health expenditure coupled with effective governance in South Asian economies may improve healthcare systems.
● The study also revealed that a rise in fertility rate increases maternal mortality rates in South Asian economies. This may be attributed to the fact that these economies are undergoing demographic transition.
● Fertility rates in these economies are steadily dropping but are still higher when compared to maternal mortality rates.
Introduction
Maternal mortality is one of the most critical and serious challenges. Maternal deaths remain a global concern despite significant progress in medical research and public health efforts. These deaths are a reflection of systemic deficiencies as well as inadequacies in healthcare delivery. The importance of public healthcare expenditure, resource distribution, and their effect on maternal health outcomes are crucial aspects of this complex problem.
Globally, Maternal Mortality (MM) has been reduced, however, in low and middle-income nations there are still major variations carrying the majority of burden. In this regard, government funding for healthcare becomes an important consideration in determining the health of a woman.
Maternal and infant death rates determine the nation’s overall health status. This is an important reflector of the nation’s socioeconomic status, standard of care, population health, and deprivation. Owusu et al, 1 carried out an analysis between the period 2000 to 2017 in which it was revealed that the maternal mortality ratio has reduced between 342 and 311. However, near about 85% of all maternal deaths have been recorded in South-Asian economies and Sub-Saharan economies, which is, higher than other nations worldwide.
Sustainable Development Goal Third (SDG 3), aims to decrease mortality to 70 for every 100 000 live births and to ensure that all people, regardless of age, live healthy lives by 2030. 2 Thus, a better healthcare system is need of the hour, where significant focus has to be given on the healthcare financing aspect also.1,3 With investment in the health sector, positive health outcomes are expected, plus improved social and political stability, which in turn creates job opportunities and contributes to the expansion and advancement of the economy.4 -6
Resource scarcity compels governments in developing nations, especially those in South Asia, to underspend on health in their budget plans. 7 In recent decades, scientists and researchers have examined the association between spending on health and health outcomes, given the significance of public medical care and its impact on the country’s economy.8,9 In this regard, numerous investigations have been carried out in the past.10 -12 Some research studies13,14 found no such association, while others 15 observed that spending on healthcare enhances health results. Thus, the link between spending on healthcare and health outcomes is unclear because healthcare spending and patterns fluctuate a lot. Therefore, the discussion regarding healthcare spending and health results is still debatable, 16 leading to the need for further investigation. In spite, of the increase in health spending in developing nations, MM remains higher. This has inspired researchers to determine the fundamental cause of maternal deaths to allocate and use health spending wisely.
Maternal mortality can be reduced by ensuring that all birth-giving women should have advanced facilities including skilled healthcare workers and emergency services. Besides, there is a need to improve prenatal care so that it will reduce high-risk pregnancies and train healthcare workers. Furthermore, the engagement of communities in support of birth-giving women and the provision of transportation facilities in times of emergencies is essential to reduce the maternal mortality ratio.
Considering the need for more clarity, the proposed study is a relational analysis of Maternal Mortality (MM) and Government Health Expenditure (GHE) in the South Asian context from 2002 to 2020 by using econometric models like Pooled Ordinary Least Square (POLS), Fixed Effect Model (FEM), Random Effect Model (REM), Hausman Test (HT), Fully Modified Least Square (FMOLS), and Dynamic Ordinary Least Square (DOLS) to observe the long-run effect of healthcare expenditure upon maternal mortality by considering Expected Years of Schooling (EYS), Fertility Rate (FR), Government Effectiveness (GE) and Gross Domestic Product (GDP) as control variables.
Review of Literature
As per the World Health Organization, a woman’s death during or within 42 days of pregnancy due to any pregnancy causes / complications or its management, except death caused by accidents or incidental factors, is termed Maternal Mortality. 17 Till 2020, per day nearly 800 women lost life from pregnancy and childbirth-related avoidable causes. Every 2 min a woman lost her life in 2020 due to pregnancy-related issues. From 2000 to 2020, the global MM was reduced by almost 34%. The literature provides us with a better understanding of how maternal mortality rates have changed over the period in different regions. Huang et al, 18 used the Logistic Regression Model technique for the 2000 to 2019 time period and found that in the United Nations, maternal mortality overall increased especially in American Indian and Black women. Wang et al, 19 find that the US has experienced a change in the underlying causes of pregnancy-related deaths, there has been a rise in mortality resulting from a fall in the cardiovascular system and pre-existing medical disorders. Ward et al, 20 studied 200 countries from the 2016 to 2020 data period by using the Global Maternal Health Micro simulation model and found that globally maternal fatalities are anticipated to decrease by 167 in 2023 with 58 nations ranking higher than 140. There has been a reduction in Maternal mortality in other regions as well. Like, in Eastern Europe and Southern Asia, there has been a decline in MM ratio by 70% and 67% respectively between 2000 and 2020.
The government is spending more on health to reduce maternal mortality and other health-related issues. It becomes important to study whether government healthcare spending impacts controlling maternal mortality or not. The association between GHE and MM has been the subject of several studies conducted over some time, either for a single country (time series) or a group of nations (eg, Sub-Saharan Africa, OECD). Although multiple data sets and methodologies were employed in this field, however, the results varied, particularly when it came to the maternal mortality ratio. 1 Numerous relational studies have been conducted analyzing GHE and MM. There is a general assumption that more government health spending can reduce maternal mortality, as the government spends to build good health infrastructure, provide affordable healthcare services, etc. Numerous studies have been conducted to find the relationship between government health spending and maternal mortality. The literature reveals mixed observations for the relationship between the said variables. Sáenz et al 21 found a reduction in MMR in the region (Latin America and the Caribbean) under analysis in a heterogeneous manner between 1990 and 2019, whereas, the GHE, Government Domestic Product (GDP), and Human Resource for Health (HRH) availability increased heterogeneously. Two-step least squares (2SLS) applied to the demand function for health was employed by Boundioa and Thiombiano 22 for 7 nations in the West African Economic and Monetary Union (WAEMU) between 1996 and 2018, wherein, public healthcare expenditure showed a negative significant relationship with MM. Atuhaire et al, 23 examined data period from 1985 to 2019 for Uganda by using the Auto-regressive Distributive lag model and observed that maternal mortality is greatly decreased by domestic government spending on maternal health issues. Chidinma 24 in Zimbabwe examined the link between government spending and MM from 1980 to 2011. The findings show that government spending has a statistically significant relationship with maternal death, with higher rates of maternal death being linked with lower government expenditure on health. Another study by Owusu et al, 1 used data from 2000 to 2015 for 177 countries in which the researchers found that there is a drawback of health spending on death across all percentiles. The percentage of infant death falls from 0.19% to 1.45%, and maternal death falls from 0.09% to 1.91%. According to this study, health spending is expected to cut maternal and new-born death rates in lower- and middle-income nations, helping to achieve SDG 3 of guaranteeing good health and well-being for all individuals. Sultana et al, 25 employed Vector Autoregression with Exogenous Variables technique to analyze data from Bangladesh, spanning the years 1990 to 2019. The study indicates that there is a positively significant effect of health spending (per capita) and the number of doctors on life expectancy, and child and maternal health. Similarly, Arthur and Oaikhenan 26 showed that spending on health significantly increased life expectancy and decreased mortality among children under 5 and mothers. Samuel and Amadi 27 analyzed data for Nigeria from 1981 to 2022 and found that the distribution of government funds to the health sector has a negatively significant effect on the rate of death for women. Chidinma 24 studied data from 2002 to 2021 for Nigeria by using the Auto Regressive Distributed Lag (ARDL) and Bound testing technique and revealed that the overall government spending on health during the long term has a negative and significant association with MM. In Nigeria (25 States) from 2003 to 2015, Nwankwo 28 used Panel Data regression analysis that shows spending on public health is vital for lowering the rate of death of women in Nigeria. Few studies are revealing contrasting results against the above states. Using the regression approach, Patrick et al, 29 investigated data for Rwanda from 1990 to 2015 and found a significantly positive relationship between maternal mortality and healthcare expenditure. Aziz et al, 30 studied data from 2000 to 2017 for South Asian Economies and observed that a 1% increase in health spending increased MM by 1.95%. Some studies observed no relationship among the variables under discussion.14,31 Nicholas et al, 32 found that there is no discernible effect of health spending on the death of a woman.
From the above studies, it has been found that except for a few studies most of the cited literature showed a negative relationship between GHE and MM. Furthermore, it has been found that different econometric methodologies have been used but not revealing entirely unambiguous results. Thus, to find the latest explicit relationship between Government healthcare spending (GHE) and MM, the study analyzed data from South Asian Economies.
After evaluating the relevant literature and co-occurrence map, the study has also considered the control variables like fertility rate, expected year of schooling, government effectiveness, and gross domestic product. Government healthcare expenditure is one of the important variables and it can directly as well as indirectly impact the maternal mortality of South Asian countries. Thus, it becomes important to study whether government healthcare expenditure positively or negatively impacts maternal mortality in the region under analysis. Therefore, the following hypothesis is proposed and will be tested empirically:
H0: There is no significant relationship between government healthcare expenditure and maternal mortality
H1: There is a significant relationship between government healthcare expenditure and maternal mortality
After reviewing the relevant literature there are certain gaps related to the data time period, econometric tools applied, region of study taken, variables, and findings. The Data period taken by the studies Aziz et al, 30 Rana et al, 33 Maruthappu et al, 34 Huang et al, 18 Boundioa and Thiombiano, 22 and Sultana et al, 25 is only upto the year 2019 whereas our study made an addition by taking data upto 2020. Most of the studies Maruthappu et al, 34 Huang et al, 18 Boundioa and Thiombiano, 22 and Sultana et al, 25 have used econometric tools like multivariate regression analysis, Logistic regression models; 2-step least squares (2SLS); Vector Autoregression with Exogenous Variables (VARX) model), whereas our studies use FMOLS, DOLS, fixed and random effect model and Hausman Test for robust results. Similarly, studies like Aziz et al, 30 Rana et al, 33 Mouinou and Mendy 35 ; Maruthappu et al, 34 Huang et al, 18 Chidinma, 24 and Boundioa and Thiombiano 22 have used the different region for studying such relationship. There is a dearth of studying such relationships in developing regions, particularly in the South-Asian context. Our study contributes by analyzing the relationship in the said required regional context. While studying the relationship between healthcare expenditure and maternal mortality, various other variables have been considered like; economic growth, population sanitation, clean fuel technology, life expectancy, infrastructure, skilled health professionals, incidence of HIV/AIDS, No. of doctors, etc. keeping in view the requirement of controlling other important factors like impact of education, fertility, and effectiveness of the government in terms of its institutions and system, our study contributes the existing literature by taking expected years of schooling, fertility rate, government effectiveness and gross domestic product as control variables. After reviewing the literature different findings have been revealed by various studies in the South-Asian context. Some concluded health expenditure to have a negative relationship with maternal mortality, and some found a positive relationship, whereas, few put forth mixed findings. In such a scenario, there is a need to further evaluate such a relationship, and the current study is an attempt to fill this required gap.
Data and Methodology
Data Source
The variables under analysis have been included in Table 1 under the variable list. The data for each indicator has been acquired from the United Development Program (UNDP), World-Governance-Indicators (WGI), and World-Development-Indicator (WDI). For comprehensive study and evaluation, we have provided both descriptive statistics and an exhaustive list of variables. The research used data spanning from 2002 to 2020 for South Asian Economies (Afghanistan, Bangladesh, Bhutan, India, Maldives, Nepal, Pakistan, Sri Lanka). To understand the relationship of the variables in a larger context, that is why the South Asian region has been selected for analysis, where a good number of countries are still developing and need to improve a larger portion.
Variables and Their Description.

Source. Authors’ compilation. Variables (MMR) are in natural logarithmic form with (ln) except (DGHE, EYE, FR, GE, GDP).
Techniques Employed for the Data Analysis
The study made use of Panel Ordinary Least Square, 27 the Fixed Effect Model, 21 the Random Effect Model, the Hausman Test, etc. (Boachie et al, 36 Kiross et al, 37 Boundioa and Thiombiano, 22 and Dieleman and Templin 38 ). The reason for using this technique was the non-stationarity behavior of one of the variables specified in the model. Further, the test of robustness was conducted using FMOLS and DOLS. 30
Specifications of the Model
It is an important and well-acknowledged fact that an improved understanding of some economic factors influences the formulation of efficient economic policies. This includes a nexus among maternal mortality, domestic government health expenditure, expected year of schooling, fertility rate, government effectiveness, and gross domestic product. The following technique was created to find the link between GHE and MM in South Asian regions over the long term, accounting for factors such as expected year of schooling, fertility rate, government effectiveness, and gross domestic product.
The functional form used to assess how government health spending affects maternal mortality in South Asian Economies is as follows:

To examine how certain below-mentioned variables affect maternal mortality ratio, the variables are converted logarithmically to minimize data fluctuation.

Where MMR, DGHE, EYS, FR, GE, and GDP signify the maternal mortality ratio, expected year of schooling, fertility rate, government effectiveness and gross domestic product respectively. MMR is the dependent variable in this model; the coefficients of the lag in the MMR are βk (k = 1, 2, 3, 4,5), expected year of schooling, fertility rate, government effectiveness, gross domestic product and µit shows the error term. To prevent overfitting and enable the association between our core variables of interest to emerge, our model was limited to these variables.
Pesaran’s CADF test was employed, which has been formulated as:

where ti (N, T) represents CD-ADF statistic.
Pedroni 39 tests were used for panel cointegration analysis, which is expressed as follows:

variables
Pedroni’s 40 regression theory serves as the foundation for the models that are suggested for the investigation.

i = 1, 2, . . ., N t = 1, 2, . . ., T
The determinants in this case are cointegrated with slope →βi, which may or may not be uniform throughout→ i.
where lnMMRit →maternal mortality ratio with log natural, DGHE it →domestic general government health expenditure, EYS it →expected year of schooling, FR it →fertility rate, GE it →government effectiveness, GDPit →gross domestic product with time→ t, and ith →nations. The MMR and its determinants are cointegrated with slopes →βi, which may or may not be uniform throughout→ i.
Pooled ordinary least square (POLS) 27 or panel least square are as follows:


Fixed effect model (FEM) equations are as follows:

The random effect model (REM) can be written as follows:

Hausman Test
Several econometrics specification difficulties can be addressed with the generic test of Hausman’s 41 specification. Nonetheless, the application that quantifies the individual effects in the panel is the one that receives the most responses from him.
Hypothesis
H0: Random effect model is better than the fixed effect model
H1: Fixed effect model is better than the random effect model
When the null hypothesis (H0) is rejected, the FEM Sáenz et al 21 is used. Otherwise, the REM will be more relevant in this case. The FEM is used first, followed by the REM. And finally, the HT will be applied to opt for the appropriate model either fixed or random.
Fully Modified Ordinary Least Square and Dynamic Ordinary Least Square
These methods were used to check the robustness of our data. 30 The Fully Modified Ordinary Least Square (FMOLS) was created by Phillips and Hansen 42 to provide an ideal co-integrating regression estimate. Due to its ability to account for serial correlation and endogeneity bias, the Pedroni 43 for the panel cointegration regressions, the heterogeneous FMOLS estimator was employed in this investigation. For the panel that contains heterogeneous cointegration, FMOLS is the technique that Hamit-Haggar 44 believes is appropriate. Recalling that the coefficient β of model 1 had a panel FMOLS estimator of:

where,

and
Result and Discussion
Empirical Results and Analysis
Descriptive Statistics
Table 2 lists the variables utilized in this investigation along with their descriptive statistics. The results for the study nations highlight the max. & min. values of MM are approximately 7.152 and 3.367, respectively. The health expenditure of the examined countries ranged from a min. of 0.084 to a max. of 9.077, with a standard deviation of 1.565 and a mean value of around 1.599. The mean value of the expected year of schooling was valued at 10.702 with a standard deviation of around 2.253. The mean values for fertility rate, government effectiveness and gross domestic product were 3.043, −0.436 & 3.588 resp., with standard deviations (S.D) of 1.363, 0.583, and 5.498.
Table for descriptive statistics.
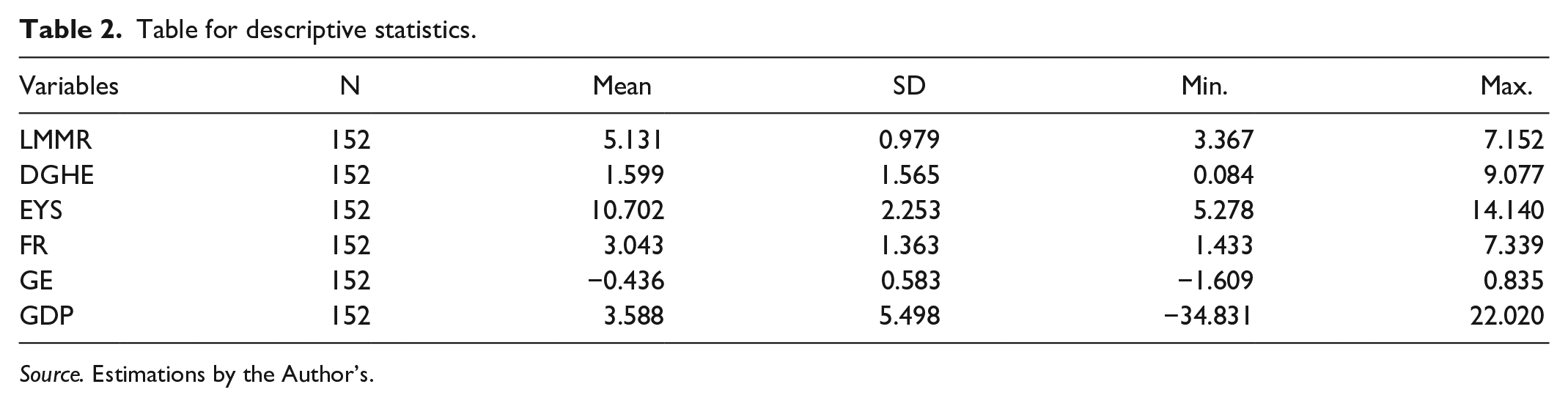
Source. Estimations by the Author’s.
Panel Data Results
Cross-Sectional Dependency Estimates and Unit Root Tests
The Cross-Sectional Dependency (CSD) test was used in this investigation before cointegration verification. Some have suggested that in data series with cross-section dependency, traditional unit root tests do not provide accurate results. Since all of the variables’ findings were shown to be significant at the 1% significance level, it was evident from the cross-sectional dependency test results that there was cross-sectional dependency among the variables (see Table 3). It recommends using a cross-sectional unit-root-test (CIPS and CADF) rather than the traditional Liven, Lin, and Chu (LLC); Im, Pesaran, and Shin (IPS) unit root test for panel data with cross-section dependency. As a result, the current study made use of the CIPS and CADF results, which demonstrated that every variable became stable at the first difference and assumed cross-section dependency within the panel data.46,47
Cross Sectional Dependency Test and Second Generation (CIPS, CADF) Unit Root Test Results.

Source. Estimation by Author’s (***→1%, **→5% and *→10% indicates significance levels).
Panel Cointegration Test
Panel data cointegration was valid to use when all variables’ stationarity properties were established. The Pedroni panel cointegration test was employed in the study to verify the cointegration. 48 Six of the 11 tests were significant at the 1%, and 5%, levels of significance with intercept, and with intercept and trend, according to Table 4’s results. These test findings clearly show that variables are co-integrated over the long term.
Results of Panel Cointegration Tests.
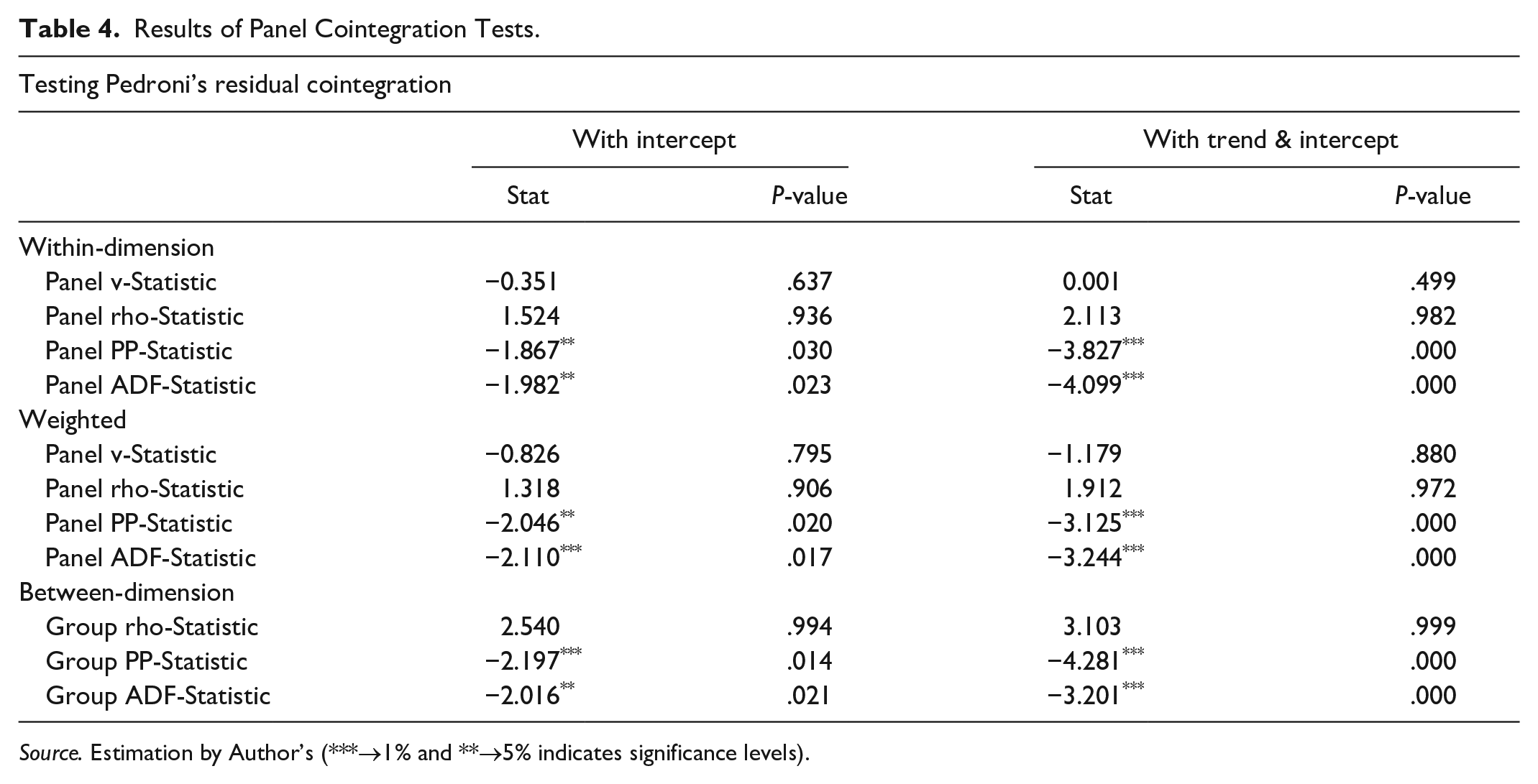
Source. Estimation by Author’s (***→1% and **→5% indicates significance levels).
Panel Estimation Results
Fixed Effect and Random Effect Results
Panel regression results are shown in Table 5. The table displays 3 sets of estimates: (1) POLS estimates; (2) FEM estimates; and (3) REM estimates.
Estimates of Parameters for Panel Regression Model.

Source. Estimation by Author’s (***→1%, **→5% and *→10% indicates significance levels).
The results for the POLS reveal that GHE and GE show a negative effect on MM while EYS FR and GDP show a positive effect on MM. Thus, an increase in government health expenditure and government effectiveness reduces maternal mortality. This implies that increased government health expenditure coupled with effective governance in South Asian economies may improve healthcare systems and result in improved access to quality maternal health services and thus may lower maternal mortality rates in the study area. In contrast, the rise in fertility rate increases maternal mortality rates in South Asian economies. This may be attributed to the fact that these economies are undergoing demographic transition. Fertility rates in these economies are steadily dropping but are still higher when compared to maternal mortality rates. When there is an increase in EYS and GDP the maternal mortality rate also increases as indicated by POLS. However, as indicated by the Fixed effect model there is a negative impact of EYS and GDP on maternal mortality rate. Generally, with higher education levels the maternal mortality rates must be reduced due to better healthcare awareness and improved decision making. The fixed effect model controls for country-specific factors so they may better point out the positive impact of education on maternal health. The study for fixed effect reveals that government health expenditure, expected year of schooling, government effectiveness and gross domestic product have negatively influenced maternal mortality in South Asian economies by 0.053%, 0.171%, 0.116%, and 0.005% respectively, and similar results are also revealed by random effects, with coefficients 0.106%, 0.033%, 0.323%, and 0.005% respectively. Thus, the test results reveal that an increase in health spending, expected year of schooling, government effectiveness and gross domestic product reduces maternal mortality while in contrast, the fertility rate shows unexpected results and reveals that an increase in fertility rate increases maternal mortality.33,49 -51 The REM indicates a similar relationship in sample nations.
Hausman’s Test Results
As shown in Table 6, the result of the HT statistic (Hausman 41 ): A low P-value favors the FEM and works against the null hypothesis that the REM is consistent. The p-value is lower than .05 shows that among tested models the FEM is appropriate in this case. The R2 coefficient is used in determining the explanatory power of our independent variables as related to changes in the dependent variable. For our model, R2 is .98 under the FEM. This means that about 98% of the variation in MM is explained by changes in government health spending, expected year of schooling, fertility rate, government effectiveness, and gross domestic product variables. Nevertheless, because the nations are different and do not have the same demographics, healthcare systems, medical advancements, or disease prevalence, heterogeneity and cross-sectional dependence affected the panel data. Outcomes based on fixed effects could be biased. FMOLS and DOLS were thus used in the investigation. Autocorrelation and heteroscedasticity in the panel data can be effectively overcome with these techniques.
Hausman’s Test.

Source. Estimation by Author’s (***→1% indicates significance level).
Fully Modified Ordinary Least Square (FMOLS) and Dynamic Ordinary Least Square (DOLS) Results
The estimates for FMOLS and DOLS are reported in Table 7, which shows that while the coefficients’ magnitudes vary, their signs remain identical. It was anticipated that a 1% increase in health spending would have a negative relationship of 0.07% of the MM on FMOLS and 0.06% of the MM on DOLS estimates for economies in South Asia. This implies that For FMOLS and DOLS, respectively, a 1% increase in fertility rate resulted in a 0.19% and 0.09% increase in maternal mortality, according to the fertility rate statistics. Results were found to be negatively significant when compared to the expected year of schooling, government effectiveness and gross domestic product as 0.17%, 0.17%, and 0.008% for FMOLS and 0.17%, 0.12% and 0.009% for the DOLS estimator, respectively.
Results for Long-Run FMOLS and DOLS.

Source. Estimation by Author’s (***→1%, **→5% and *→10% indicates significance levels).
The impact government health expenditure variables on the maternal mortality in long run, can be seen from the finding of the FEM, REM, FMOLS, DOLS model presented in Tables 5 and 7 and summarized in Table 8. As evident from Table 8, which depicts the impact of the independent variable of the study on maternal mortality, DGHE, EYS, GE, and GDP have a negative long-term effect on maternal mortality. On the other hand, FR have a positive effect on maternal mortality in the long run.
Summary of Long Run Impact of Independent Variables on the Dependent Variables.

“+” and “−” signs indicate the positive and negative impact, respectively.
Dependent variable: Maternal Mortality (lnMM).
Discussion
The present study highlights the relationship between MM and GHE. 30 We used the data for 8 South Asian Economies time spanning from 2002 to 2020 for FEM, 21 REM, FMOLS, and DOLS 30 estimation techniques.22,36 -38 The results showed that there is a fall in MM by increase in government health spending. Results from POLS 27 analysis showed that expenditure on health and government effectiveness are important factors in reducing MM for South Asian Economies. This implies that increased government health expenditure coupled with effective governance 51 in South Asian economies improves healthcare systems which results in improved access to quality maternal health services 52 and thereby significantly reduces maternal mortality rates in the study area. Fertility rate and MM have been found positively related. Here the relationship found is not to our surprise, since both the variables show decreasing values. 53 Theoretically, both variables should be positively related, because with declining fertility, the possibility of risky pregnancies also declines.49,50 PLOS results reveal a contrasting picture of a positive relationship with MM for the controlling variable EYS and GDP.
To get more reliable results, long-run FMOLS and DOLS analysis was carried out, where in addition to the above-discussed results, EYS and GDP is found to be negatively related to MM. More years of schooling is expected to reduce MM on the assumptions of increasing knowledge related to better and necessary healthcare utilization, 33 together with awareness of maternal healthcare facilities. 54 Further assumptions of more education and more financial health55,56 and better access to resources 57 will lead to reduced MM.
Conclusion and Policy Implications
Our study has established that government health expenditure lowers the mortality rate in the study area. This indicates that the existing expenditure in South Asian economies is effective. Therefore, in these economies, the government may consider to increase the proportion of their health budget. This additional investment may increase the benefits of mortality reduction and may involve investment toward the development of quality healthcare infrastructure. Besides, it can also contribute toward increasing accessibility to basic healthcare facilities and quality services and prioritizing preventive healthcare measures. Thus, the effective reduction of mortality rates in South Asia through government health expenditure highlights the dynamic role that healthcare investment plays in fostering the overall well-being of the economy. The study further revealed that the government’s effectiveness reduces the maternal mortality ratio in South Asia. This indicates that through effective governance, the Government in these economies prioritizes healthcare investment and their policies are designed toward increasing access to maternal healthcare services. Thus, in South Asia effective governance needs to be sustained for better health outcomes in general and reduced maternal mortality rate in particular. In addition to the above, the study also revealed that education plays an important role in reducing maternal mortality rates, so policymakers in this region need to design policies focusing on more female-inclusive-education while controlling female dropout ratio (particularly increasing number of years of schooling for marginalized population of the region). The study has also pointed out that in this region, fertility rates increase the mortality rates. This indicates that the high fertility rates in this region put pressure on existing healthcare services and therefore leave women in this region to face maternal health risks. Therefore, more investment is required to build adequate healthcare infrastructure to reduce maternal mortality.
Limitations and Future Directions
Since the study has concluded based on analyzed data from 2002 to 2020, due to the limitation of non-availability of previous data related to a few variables for the selected economies, there is an immense scope for more analysis for the same economies by considering large data period. The study can also be extended by including other important relevant control variables that affect maternal mortality rates. The study used the panel data set and future research can be based on longitudinal data, it can be associative research and it can be extended to study the mediate or moderating relationship between the variables.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251339069 – Supplemental material for Impact of Government Health Expenditure on Maternal Mortality: An Appraisal of South-Asian-Economies
Supplemental material, sj-docx-1-inq-10.1177_00469580251339069 for Impact of Government Health Expenditure on Maternal Mortality: An Appraisal of South-Asian-Economies by Azhar Jan, Meenakshi Gupta and Sheikh Aftaab-Ul-Maroof in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We are sincerely thankful to Editor-in-Chief Prof. Umair Shafique and four anonymous reviewers for insightful comments.
Author Contributions
Azhar Jan: Conceptualization, Data curation, Validation, Writing—original draft. Dr. Meenakshi Gupta: Conceptualization, Investigation, Supervision, Validation, Writing—review & editing. Dr. Sheikh Aftaabul Maroof: Conceptualization, Validation, Writing—review & editing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.