
Abstract
The employed family caregivers juggle caregiving and work responsibilities constantly, highlighting a growing concern for their financial and professional well-being. Compared to the rich studies on the caregiving impact on the mental and physical health of caregivers, the intricacies of the work-family relationship have been limited, particularly concerning the dementia caregivers. This study investigates the effects of caregiver intervention on various quality-of-life measures using a first-hand dementia dataset, collected through a 6-month, evidence-based, multicomponent intervention, and targeting the well-being of family caregivers who care for loved ones with dementia. The intervention demonstrated a statistically significant positive impact, as evidenced by decreased distress, depressive symptoms, subjective burden and, notably, decreased family-to-work conflict, and financial stress. Additionally, caregiver self-efficacy scores exhibited a significant increase. This study suggests that the caregiver intervention improves the quality-of-life measures and reduces caregiver stress. Addressing the well-being of caregivers is essential for enhancing overall societal health and productivity.
There are two sources of conflict creating caregiver stress. One source comes from family responsibilities, the other from work responsibilities. This study shows that family caregiving stress can be defined and managed through individual coaching sessions. It is equally important to design matching stress reduction efforts at workplaces and more research is needed to identify sources of stress stemming from the workplace.
Introduction
More than 1 in 5 Americans (21.3%) are caregivers, having provided care to a sick or older adult or child with special need and 1 in 5 full-time employees handle both their job and caregiving responsibilities. 1 With a rapidly aging population in the U.S., more Americans are transitioning into the role of a caregiver for family members of blood or choice every year. The Population Reference Bureau has projected that the number of Americans who are 65 years old or older will double from 52 million (16% of the total population) in 2018 to 95 million (23% of the total population) by 2060. 2 Caregivers are vulnerable to productivity loss, which can be costly to their families and employers.3 -6 Particularly, the work-family conflict is one major challenge that dementia caregivers are more likely to face: dementia caregivers were less likely to be employed and more likely to be retired than non-dementia caregivers; they also experienced more employment complications and a family-work conflict than the non-dementia caregivers. 7 Because of the characteristics of the disease, dementia patient care can last for a significant period of time, and generally gets more and more intensive over time as dementia progresses, eventually reaching a point where they may need around-the-clock support for basic daily activities. 8 For many years, scholars have studied the impact of caregiving on caregivers’ mental and physical condition9,10 and how particular interventions can mitigate the unfortunate burdens of caregiving,11 -13 but to date, the understanding of the intricacies of work-family relationship concerning dementia caregivers have been comparatively limited.
Work-family conflict is defined as “a form of inter-role conflict in which the role pressures from the work and family domains are mutually incompatible in some respect.” 14 That is, participation in the work role is made more difficult by virtue of participation in the family role. This conflict exists in three major forms: time-based conflict – devoting time to one role makes it difficult to devote time to another role; strain-based conflict – one role negatively affects one’s performance in the other role; and behavior-based conflict – specific patterns of in-role behavior are incompatible with behavioral expectations in another role. The time-consuming nature of caregiving is a major source of conflict with regular employment. Time-based conflict leads to caregivers quitting their jobs or reducing hours to provide care. The work-family conflict is bidirectional, that is, work-to-family and family-to-work. The general demands of time, devoted to, and strain created by the job (family) interfere with performing family (job)-related responsibilities. 14
Importantly, the work-family conflict leads to stress that may jeopardize the mental and physical health of caregivers. According to the Conservation of Resources theory, when an individual’s resources become exhausted, that individual will experience psychological strain, which may affect an individual’s general health. 15 Studies have highlighted the association between work-family conflict and poor mental and physical health of caregivers.9,16,17 The expenses involved in caregiving force some caregivers to put their personal needs, health, and expenses aside. Meanwhile, limitations on a caregiver’s ability to participate in valued activities and interests also resulted in more emotional distress. 18
The heavy pressure attached to the dual roles of family caregivers and the consequences associated with this pressure demand a better understanding of work-family dynamics. In one recent study, Kayaalp et al 19 tested a mediational model explicating the process through which caregiver burden impacts mental health through work-family conflict. Neubert et al 7 identified factors related to caregiving that influence employment, through reviewing a mixed-studies on dementia caregiving and employment. The authors state that although the impacts of these factors on caregivers’ employment are mostly negative (eg, stopped/reduced work, decreased job performance), working may provide relief and counterbalance the caregiving strain.
Given the comparatively high salience of work-family conflict, this is an especially key area in which to focus evidence-based interventions aimed at alleviating caregiver stress. This paper presents an analysis using first-hand dementia caregiver data collected via the Rosalynn Carter Institute for Caregivers (RCI) – Hilarity for Charity (HFC) caregiver coaching project project. Using this data set, below we examine the impact of the caregiver intervention on several major caregiver quality-of-life measures, including work-to-family conflict, family-to-work conflict, financial stress, caregiving capabilities, and mental health, and also observe the relation of different quality-of-life indicators to each other, as well as caregiver demographics and caregiving-related characteristics at baseline and end of the program. Our main goal is measuring the effect of caregiver intervention on either work-to-family conflict, family-to-work conflict, or both and understanding if there are positive impacts and how significant the impacts are, comparing to the effect on other caregiving stressors. Using this data we also want to assess work-family conflict interaction with other stress indicators and thereby understand the overall potential effectiveness of caregiver support (or lack of) on caregiver wellbeing.
Research Design and Methods
Design and Participants
This study is an analysis of RCI Resources for Enhancing Alzheimer’s Caregiver Health (RCI REACH) programmatic data from the 2020 to 2021 RCI-HFC caregiver coaching project. It is a 6-month, 1 on 1, evidence-based, multicomponent caregiving intervention that targets the well-being of family caregivers who care for their loved ones with the Alzheimer’s Disease and other dementias. RCI REACH is a translation of the REACH II intervention, which was a randomized controlled trial originally sponsored by the National Institute on Aging and the National Institute on Nursing Research, and it combines the proven components of the original REACH clinical trial. RCI REACH was piloted through the RCI with similar outcomes to the original clinical trial. The translation was then replicated through an Area Agency on Aging in Coastal Georgia beginning in 2010 and has been implemented nationally since that time.20,21
The RCI REACH program was further developed under the 2020 to 2021 RCI-HFC caregiver coaching project. First, the program delivery format transformed from in-person to virtual, to serve more dementia caregivers in more places, particularly under the COVID-19 pandemic situation. Several changes consequently took place to accommodate this change. Some of the most notable changes were with coach training. While core content remained the same, coaches must learn how to utilize tools on the virtual delivery platform and different learning style methods to close the gap between in-person and virtual program delivery. “Virtual Empathy” component was created and added onto the training sessions. The coaches learned to be virtually empathetic, create a virtual safe space, and ensure caregiver comfortability to discuss difficult issues in dementia caregiving through a computer screen. Another change to this program was to the feedback protocols, most notably with safety concerns. This new safety protocol includes items, such as what is reportable in virtual program delivery, how to report safety concerns from opposite sides of the country, and ensuring appropriate documentation is kept. In additional, per IRB approval, coaches read the program consent form to each caregiver, had the consent pulled up for caregivers to read along, and caregivers were also sent the consent form before the session and after the session. Caregivers were also given RCI program supervisor contact information for any follow-up questions and also were given the IRB contact information.
The coach designation process for this program became more intense to include additional skills required by the virtual coaching. Program coaches were required to have experience working with individuals diagnosed with dementia and family caregivers and achieve certification through a multi-step training and evaluation procedure, including a demonstration of skills session with the master trainer. Each coach must complete and pass a Learning Process Worksheet and role play scenario. Each role play scenario has a grading method and points assigned to each section to show the coach’s mastery of the topic. These evaluations were scored with a required score of 75% or higher to achieve certification. Throughout the project period, coaches received technical assistance from RCI master trainers and met regularly with other project coaches and supervisors for case consultation, resource needs, and problem-solving (Figure 1).

Structure of the RCI REACH program.
Trained program coaches met with the caregiver for up to 12 (at least 9) sessions – 9 (at least 5) sessions face-to-face via videoconferencing, approximately 1 h each, and 3 (up to 7) telephone sessions, approximately 0.5 h each. Sessions were held every 2 weeks to allow for home practice. During sessions, coaches and caregivers worked on a variety of set topics to aid in their caregiving journey. These sessions revolved around self-care, stress management, navigating difficult dementia behaviors, and problem-solving. At the initial session and final session, assessment data was collected by the program coach, including demographics and assessment of caregiver mental health, caregiving capabilities, financial stress, work performance, and work-family conflict (if the caregiver is employed in a professional position).
Particularly, in coaching sessions, coaches and caregivers work through barriers to finding and keeping employment. These types of sessions involved recognizing barriers to employment such as exploring employment opportunities and understanding employment requirements, while navigating working while caring. Another part of these coaching session is to also understand what seeking or remaining employed means for the caregiver/care-recipient dyad with ensuring the care-recipient is cared for and the employment adds value to the caregiver’s life without having to sacrifice a caregiver’s role, physical health, or emotional wellbeing. These sessions can take form in looking at the best way for a healthy home ecosystem.
Caregiver participants included rural and urban caregivers who provided at least 4 h of care per day for a person with memory deficits and reported a stress level of 5 or greater on a 10-point Likert scale. Exclusions included caregivers who planned to place their patient in a residential facility within 6 months or could not commit to complete the full intervention (12 sessions over 6 months). The Georgia Southwestern State University Institutional Review Board provided institutional oversight for this project. Baseline assessment was conducted at the beginning of the program, and the end-of-program assessment was done at its end. The study flow diagram summarizes this project – there were 154 caregiver referrals via the online referral form, 95 caregivers enrolled in the program, and 71 of the 95 enrolled caregivers completed the program (Figure 2).
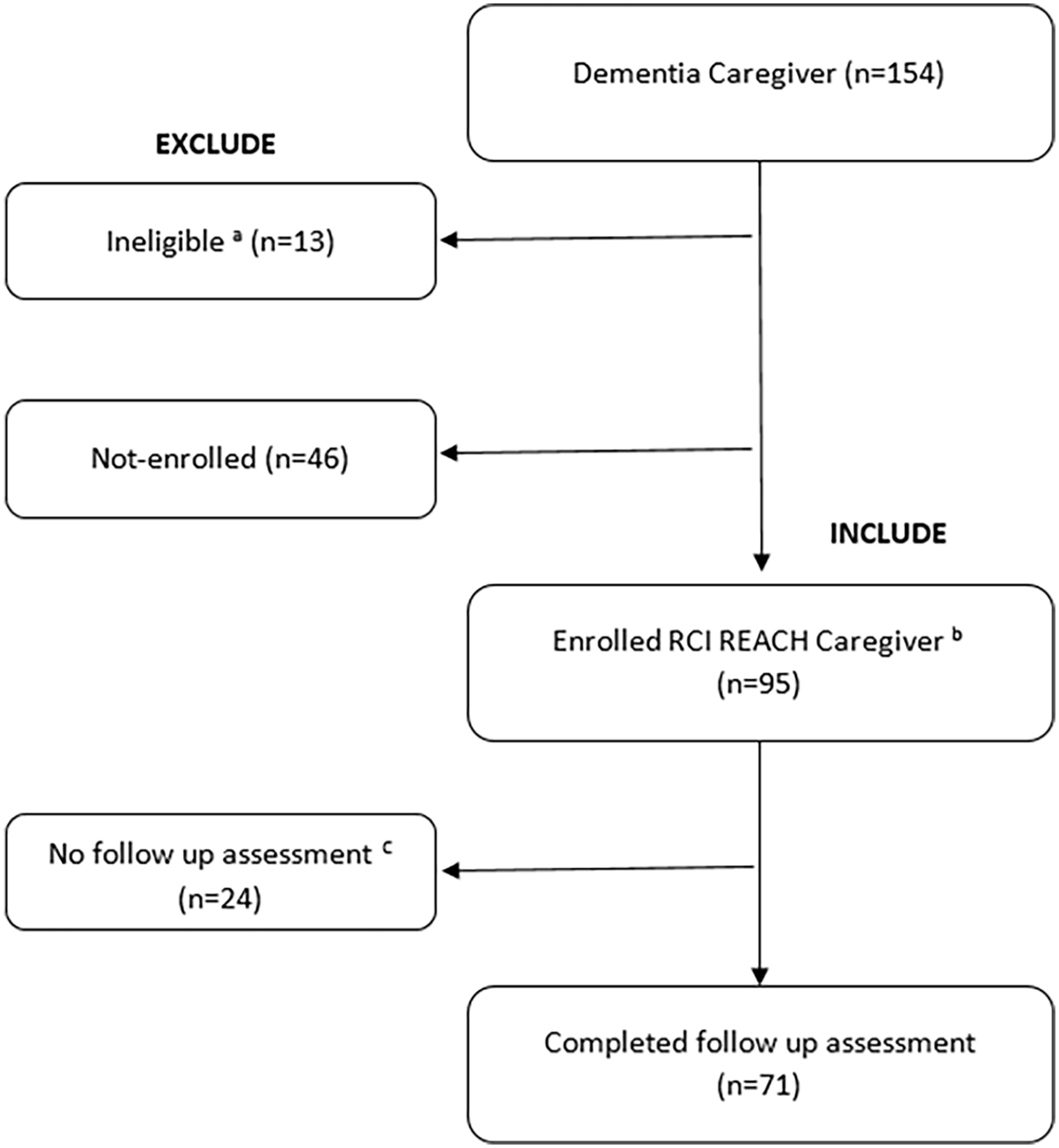
Study flow diagram.
Measures
Quantitative assessment instruments were used to measure pre- and post-intervention caregiver mental health, caregiving capabilities, financial stress, work performance, and work-family conflict (if the caregiver is employed in a professional position). Both the baseline and end-of-program assessments were conducted via video conferencing.
The mental health condition of caregivers was measured principally via 2 assessments: The Center for Epidemiologic Studies Depression Scale (CESD-10) and the Revised Memory and Behavior Problems Checklist (RMBPC-24). The caregiving capabilities of caregivers were measured via the Zarit Burden Interview (ZBI-12) (from the perspective of caregiver role strain) and the Revised Scale for Caregiving Self-Efficacy (from the perspective of caregiver role confidence). The caregiver’s perceived financial stress was measured via the Financial Resources Subscale from Caregiver Reaction Assessment; perceived work performance was assessed via the Absenteeism and Presenteeism Scale; and work-family conflict was evaluated via the Work-Family Conflict (bidirectional) Scale. Below, we discuss each of these measures in turn.
Analysis
First, to provide a big picture of the features of the caregivers in this study, descriptive statistics for caregiver demographics and caregiving-related characteristics were calculated. Summary statistics including frequency (N) and percentage (%) for categorical variables (eg, gender, race, and ethnicity) and mean and standard deviation (SD) were reported for continuous variables (eg, average age and number of household occupants). To assess the program impacts, caregiver measure scores were calculated for baseline, end of program, and the difference between baseline and end of program. Because caregiver measures use a different unit of scale, to compare and understand which factors have a greater change throughout the program, the standardized mean difference (SMD) was used to standardize the results to a uniform scale in the study. A standardized mean difference was calculated for each measure by subtracting the sample’s baseline mean for that variable from the follow-up mean values, then dividing by the sample baseline standard deviation. Statistical testing for change was evaluated using one-sample paired t-tests. Data normality was checked prior to applying t-tests; for the non-normally distributed metric data from paired observations, the non-parametric test, Wilcoxon signed rank test, was applied.
Two independent sample t-tests or one-way analysis of variance (ANOVA) were used to examine the associations between caregiver demographic variables (age, gender, race, ethnicity, and education) and the baseline assessment scores. This allows us to see if caregiver condition at baseline was related to some demographic features. The same methods were also used to test the associations between demographics and the score differences between baseline and end-of-program assessment scores. This allows us to see if one group of participants achieved comparatively better results from the program than others. The effect size measures, Cohen’s d (Cohen’s f for continuous variable, ie, age), were included to reflect the significance of the changes observed.
To understand if care work intensity and caring duration affect caregiving capacities and the work-family conflict, general linear models (GLM) were used to test the correlations between caregiving-related characteristics (hour of daily care, number of household occupants, and year of caring) and baseline assessment scores, as well as the pre-post score differences. The relations between the pre-post score differences among the measures were also studied to understand how the intervention works on improving caregiver conditions and thereby mitigating the work-family conflict. Statistically significant associations were identified. All analyses were performed in SPSS v26 and set significance at α = .05.
Results
Descriptive Statistics
Ninety-five caregivers enrolled in the RCI REACH program, and seventy-one out of ninety-five completed the program (thirty-two of seventy-one completers held a professional job at the time of completion). This leads to 95 baseline assessments and 71 paired baseline and end-of-program assessment with work-related measure results). The demographics and caregiving-related characteristics of the caregivers are reported in Table 1.
Descriptive Characteristics at Enrollment (N = 95).

Note. N = 95, including all enrolled caregivers who completed the data assessment at baseline.
aIncludes “changed to work from home,” “changed work schedule,” and “changed work district.”
bADL = activity of daily living; IADL = instrumental activity of daily living.
To capture the impact of caregiving on their work status, the participants were asked “Has there been any change in your work status since becoming a caregiver?” and “if yes, what changed?” 52 of 95 participants reported that their work status was impacted because of caregiving responsibilities, including quitting their job, reducing work hours, or retiring early. Among the 43 participants who reported “no” work status change, 18 of them had a job prior to becoming a caregiver and the remaining 25 had no job prior to and during caregiving. Therefore, among the participants who had a job prior to becoming a caregiver (n = 70), 74% (n = 52) experienced negative impact on work when they took the role of caregiver. These summary statistics are also detailed in Table 1.
The demographics of the care recipients were not listed in Table 1 but are summarized as below: the average age of the care recipient was 76 years old (SD = 10.63), 52 (54.7%) of them were female, 90 (94.7%) were Non-Hispanic, 72 (75.8%) were White and 14 (14.7%) were Black. 17 (17.9%) of them were veterans.
Baseline to End-of-Program Score Changes in Caregiver Measures
For each measure of caregiver well-being, our assessment data are reported as raw values for baseline mean, end-of-program mean, and the mean difference between baseline and end-of-program measures, as well as a standardized mean difference (Table 2). From baseline to end-of-program, caregiver measures showed significant (P < .05) decrease (improvement) in distress, depressive symptoms, financial stress, subjective burden, and Absenteesim and significant increase (improvement) in self-efficacy. More specifically, the mean caregiver depressive symptoms score was 12.4 at baseline and 7.5 at end-of-program, with an average decrease of 4.9 points (SD = 4.6, P < .0001). A cutoff of 10 is widely used to classify participants with an elevated risk for depression. A decreased score indicated that the participants improved with support from the RCI REACH program. Similarly, the mean caregiver subjective burden score was 24.9 at baseline and 17.6 at the end-of-program, with an average decline of 7.3 points (SD = 8.3, P < .0001). A cutoff of 20 is used to identify participants at a high degree of burden, the score decline indicated improvement.
Change in Caregiver Well-being Between Baseline and End of Program.

Note. Lower score indicates better outcome (improvement): absenteeism, caregiver distress, depressive symptoms, perceived financial stress, and subjective burden.
Higher score indicates better outcome (improvement): perceived family-work conflict, perceived work-family conflict, and self-efficacy.
N = 71, including all enrollees who completed the follow up assessment.
N = 32, including all completers who had a professional job.
Non-normally distributed metric data from paired observations; the non-parametric Wilcoxon signed rank test was applied accordingly. Bold values indicate statistical significance.
The work-related measures showed an increase (improvement) in presenteeism and a decrease (improvement) in absenteeism, family-to-work conflict, and work-to-family conflict. However, among these improvements, the improvement of family-to-work conflict reached statistical significance (P = .005), while the rest had not.
The standardized difference mean scores of the measures were calculated to compare and find which pre-post changes were the greatest among all the measures. The comparison results showed most improvement on depressive symptoms, subjective burden, and self-efficacy, followed by improvements in caregiver distress, financial stress, and family-to-work conflict.
Associations Between Caregiver Demographics and Baseline Score, Pre-Post Score Differences
Participant data showed no significant association between caregiver demographics and caregiver baseline measure scores. Namely, the caregivers, regardless of their age, sex, race, ethnicity, or education background, reported similar impact of caregiving on their mental health when they enrolled in the program. Caregiving and financial stress, and perceived work-family conflict were at similar levels, too (These non-significant statistics were not listed in Table 4 due to space limitation).
At the end of program, however, there was significant positive correlation between caregiver age and the change of depressive symptoms (B = 0.095, SE = 0.047, f = 0.25, P = .048) and family-to-work conflict (B = −0.052, SE = 0.023, f = 0.41, P = .027): the younger the caregiver, the greater improvement in caregiver depressive symptoms and family-to-work conflict (Table 3). For Cohen’f, a value of 0.25 indicates a medium effect size and a value of 0.4 indicates a large effect size. This may be because the knowledge, taught in the coaching sessions (eg, coping strategies and the problem-solving skills as well as caring resources), are particularly new for the younger caregivers. By learning about and applying them to navigate the dual responsivities, the younger caregivers more effectively alleviate mental and work stress than the older ones.
Demographics and Change in Self-reported Caregiver Outcomes Between Baseline and Post-assessment.

Meanwhile the White caregivers showed greater subjective burden decrease than the non-White caregivers (a decrease of 8.5 points (SD = 7.9) vs 2.9 points (SD = 8.4), d = 0.69, P = .019). As we have a closer look at these 2 groups, we noticed that although the average ages of the caregivers were quite similar (59.5 for the White and 58.1 for the non-White) between 2 groups, their relationships to the care recipients were significantly different: 73% of the non-White caregivers cared for their parents (20% for spouses/partners), while only 23% of the White caregivers cared for their parents (57% for spouses/partners). This suggest that the care recipients of the non-White caregivers were comparatively older and required more care work from their caregivers than those of the White caregivers. Caring a patient whose illness deteriorates significantly with aging, the caregivers with older patients may find more difficult to reduce caregiver burden than those with younger patients.
Correlations Between Caregiving-Related Characteristics, Baseline Score, and Pre-Post Score Differences
In addition to caregiver demographics, this study also investigated the relationship between caregiving-related features and the baseline and pre-post changes of the measures. One of the findings is that there was a significant positive correlation between “hours of care” and caregiver financial stress. Specifically, the more daily caring hours, the higher perceived financial stress at baseline, and the smaller decrease of financial stress at the end of program (Table 4). As the caregivers spent more time on caring at home, they would have to reduce work hours or quit working, either way would likely lead to reduced income and financial resources.
Correlation Between Caregiving Characteristics and Baseline, Pre-Post Differences.

P < .05. **P < .01.
However, there was no significant correlation between “years of care” and the pre-post differences of the measures. In other words, the participants benefited from the program equally regardless of whether they just started caregiving or had been in the role for years. “Years of care” was not associated with the baseline scores either.
In terms of correlations between the pre-post differences of the measures, the data showed that improvements in caregiving capabilities (reflected via the caregiver subjective burden and self-efficacy scores) were positively correlated with the improvement in caregiver mental health (reflected via depressive symptoms and caregiver distress scores), as well as improvements in financial stress and family-to-work conflict. Thus, the caregivers who reported a greater decrease in subjective burden and a greater increase in self-efficacy, tended to report a greater decrease in depressive symptoms, distress, and financial stress, and a greater decrease in the family-to-work conflict.
Discussion and Implications
Caregiver measure outcomes showed significant improvements in caregiving capabilities (decreased subjective burden and increased self-efficacy), and caregiver mental health (decreased depressive symptoms and distress) and family-to-work conflict. Thanks to the coping and problem-solving strategies, together with the dementia caring skills that caregivers learned through the coaching sessions, the caregivers improved their caregiving capabilities and the mental wellbeing and more effectively navigate the caring-working dual roles. In addition, the caregivers learned to positively recognize the meaning of seeking/remaining employed for the caregiver-care recipient dyad and appreciate the values and rewards that employment adds to the caregiver’s life.
First, greater self-efficacy and a lower level of subjective burden are strongly correlated with a decline in symptoms of depression and distress in dementia family caregivers.34 -37 According to the Stress/Health Model, caregiver stress results from the caregiver’s assessment of the demands of caregiving being greater than the caregiver’s assessment of their capabilities to meet those demands. 38 Therefore, when caregivers gained coping skills and management strategies through the intervention, they assess their abilities as greater than the demands (adequate self-efficacy), and therefore experience less strain and better mental health. 39
Meanwhile, when caregivers felt more confident in their ability to successfully complete tasks at home and perceived a lower level of caregiving burden, they felt stronger mentally and had more confidence in performing better and being focused on the workplace. This does not necessarily mean that caregiving work was quantitively reduced at home; instead, caregiving work was perceived as less burdensome because caregivers gained more skills, strategies and support due to the intervention. This positive outcome of the intervention is particularly important, considering the data were gathered during the COVID-19 pandemic period (February 2020–May 2021), when the work force in general (and caregiving employees in particular) faced a surge in work-family challenges nationwide.
That the improvement in work-to-family conflict, however, did not reach statistical significance may suggest that more supportive work policies need to be provided from the intervention. It is hard to move the needle of work-to-family conflict if the support is offered only at home.
It is also worth noting the correlation between the number of household occupants and work-family conflict change. Specifically, the more adults there were at home, the greater decrease in family-to-work and work-to-family conflict at the end of the program. Meanwhile, the more children there were at home, the higher family-to-work conflict at baseline and the greater decrease in caregiver depressive symptoms and subjective burden at the program completion. The outcomes here indicated that the “Sandwich generation” caregivers (half of the participants in this study took care of their parents), who were pressed by the demands of the generations above (aging parents) and below (children or grandchildren) faced more severe work-family conflict and felt more “caregiving crush.” The skills and knowledge offered by the intervention evidently helped the caregivers in such households effectively. These are encouraging findings. Although the “Sandwich-family” phenomenon is not universal as it may depend on socio-economic and cultural factors, the findings here show that more tailored caregiver interventions can be particularly beneficial for the Sandwich-family caregivers.
Finally, the comparison of caregivers who had to leave work or reduce work hours because of caregiving responsibility and those who did not, shows that the former reported significantly (t(93) = 0.316, P = .013) lower distress (M = 1.44, SD = 0.68) at baseline than the latter (M = 1.82, SD = 0.79), and significantly (t(93) = 0.595, P = .005) higher financial stress (M = 3.12, SD = 1.34) at baseline than the latter (M = 2.33, SD = 1.32). It is understandable that the caregivers felt less overwhelmed by the caring responsibilities at home after leaving or reducing work; however, they were consequently challenged with higher financial strain as their income reduced because of unemployment or work-hour reduction. However, there was no significant difference between these 2 groups on pre-post score changes on their burden, self-efficacy, depression, distress, and financial stress. This is consistent with the findings of a military-caregiver-intervention study, 40 where no significant differences were found in program outcomes among the participants who had external jobs (either full- or part-time) and who had no external jobs.
Limitations
As a non-clinical study, there was a lack of control group in this study. One alternative explanation of our results is the effect of time on caregiver capabilities – namely, it is possible that the more experience and time for adjustment caregivers have, the more likely caregiver capabilities (and the positive outcomes associated with them) will have developed naturally. This is especially important given the protracted length of our 6-month program. However, a statistical analysis showed no significant correlation between length of caring time (measured in years) and caregiver outcomes on any of our dependent variables.
Another limitation of this study is the high education level and the disproportionate number of female caregivers and Hispanic caregivers in the sample, which may limit generalizability. However, a statistical analysis showed no significant correlation between education level and caregiver outcomes. It is worth noting that our statistical analysis did not see a significant difference between the male and female dementia caregivers. This is not consistent with previous findings that female caregivers report more stress because of caregiving than male caregivers.41,42 Female caregivers tend to provide greater types of caregiving tasks and more hours of caring work. They also tend to use emotional coping strategies which could account for greater average burden scores. 43 The major reason for this inconsistency, we believe, is that 86.3% of the participant dementia caregivers in this study were female caregivers, over 25% higher than that (61%) of the general female caregiver percentage. 5 Due to the small number of male caregivers, the difference between female and male caregivers may not be statistically significant. Noteworthily, the feminization of caregiving is not unique to this program participants. Not only is caregiving responsibility disproportionately landed on the shoulder of women, but the caregiving intensity is higher among the female caregivers than male ones. 44 The Hispanic caregivers in the sample were 8.4%, which was much lower than the Hispanic percentage of the general American population (18.7%) and that of the general American caregiver population (17%). This disproportion also limited our findings on the potential significant differences between these 2 groups under this study.
Last, work-family interface includes not only negative but also positive aspects, such as, enhancement, facilitation, positive spillover and enrichment, in addition to employment as a relief or a counterbalance for caregiving strain. 45 Caregivers may feel fullfillment and satisfaction when they manage both efficiently. A positivity-oriented scale is needed for this study to capture the positive impact of employment on caregivers.
Conclusions
This study’s findings show positive outcomes from 1-on-1, virtual caregiver intervention provided by the 2021 to 2022 RCI REACH caregiver coaching project. Supported by the first-hand data, participant dementia caregivers experienced not only significantly decreased dementia caregiver subjective burden, depressive symptoms, distress, and increased self-efficacy, but also significantly decreased financial stress and family-to-work conflict. These findings encourage us to expand tailored caregiver intervention to other types of family caregivers and to working caregivers trying to balance work and caregiving demands.
Meanwhile, the lack of effectiveness in decreasing the work-to-family conflict requires us to further explore the resources and methodologies that intervention could utilize to tackle this problem, including collaboration with the employers, government, and local communities. We are eager to develop and test the new components of the intervention, thereby more effectively helping family caregivers, the unsung heroes.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251332766 – Supplemental material for Caregiver Support Program May Decrease Work-Family Conflict: An Intervention Study
Supplemental material, sj-docx-1-inq-10.1177_00469580251332766 for Caregiver Support Program May Decrease Work-Family Conflict: An Intervention Study by Ke Wang, Toni P. Miles, Jennifer M. Olsen and Lezlie Poole in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Ethical Considerations
Georgia Southwestern State University Institutional Review Board provided institutional oversight for this project, reference number is FA19-13RENW.
Consent to Participate
A written consent was obtained from the participant prior to the start of the intervention.
Author Contributions
Study conception and design: Ke Wang, Jennifer Olsen, Lezlie Poole
Data collection: Ke Wang, Lezlie Poole
Analysis and interpretation of results: Ke Wang
Draft manuscript preparation: Ke Wang, Toni Miles.
All authors reviewed the results and approved the final version of the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author, [KW]. The data are not publicly available due to their containing information that could compromise the privacy of research participants.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.