
Abstract
This study includes clinical cohort data on 202 People Living with HIV/AIDS (PLWHA) in Izmir, Turkey. Study is conducted at the Izmir Bozyaka Education and Training Hospital, Department of Infectious Diseases and Clinical Microbiology and analyzes the impact of demographic, socio-economic, and clinical factors of HIV stigma, which includes three dimensions of stigma: internalized, anticipated, and enacted. This paper uses clinic data recorded by patients and healthcare professionals of the outpatient clinic. In order to obtain socio-economic measures, patients were interviewed face-to-face. We employ a logistics regression model that aligns with our binary stigma variables. Robustness checks include Ordinary Least Squares and Ordered Logistics models. Our results show that age and marital status are the 2 important demographic factors that affect stigmatized attitudes. Divorced PLWHA have a higher degree of both internalized and anticipated stigma. We find that educated people have a lower degree of internalized stigma. In addition, a higher-income level is found to be inversely associated with enacted stigma. Our results also reveal that LGBTs, drug users, and people who have chronic illnesses have experienced higher stigma levels. This paper explores the complex ways socioeconomic factors contribute to stigma in the Turkish context, addressing a significant gap in the literature since the cultural and social dynamics of stigma in Turkey are frequently overlooked. Recognizing the protective influence of education and income, policies such as integrating HIV education into school curricula and offering financial assistance to PLWHA, especially those from low-income backgrounds, can help reduce stigma.
Keywords
Introduction
Impact of stigma on current HIV data trends are emphasized and well documented in the literature.1 -8 According to Turkish Ministry of Health records, between 1985 and 2024, 45 835 individuals were diagnosed with HIV (+), and 2438 had AIDS. Males constitute about 82% of all cases, with sexually transmitted infection being the most common form of transmission at 94.4%.
This study includes clinical cohort data on PLWHA and analyzes the impact of demographic, socio-economic, and clinical factors of HIV stigma, which includes 3 dimensions of stigma: internalized, anticipated, and enacted.
United Nations Program on HIV/AIDS (UNAIDS) 1 emphasized HIV-related stigma and discrimination are causing persistent barriers to addressing the AIDS epidemic, restricting access to prevention, testing, and treatment services for those most at risk. 9 Eliminating all forms of HIV-related stigma and discrimination is fundamental to achieving the Sustainable Development Goals (SDG) and targets of the Joint UNAIDS by 2030, including ending AIDS. According to the UNAIDS, HIV-related stigma is the most serious issue for the PLWHA. UNAIDS created a guidance for national governments and key stakeholders on the issues of HIV stigma and emphasized how stigma and discrimination cause harm. UNAIDS SDG outlined the importance of socio-economic factors, in particular under the 10 SDG areas. These are ending poverty and hunger, ensuring universal health coverage, quality education, gender equality, promoting economic growth, reducing inequality, make cities safe and resilient, promoting peaceful and inclusive societies, and creating affordable HIV commodities and medicine.
Four decades later, stigma and discrimination continue to hamper access to and acceptance of HIV prevention services and reduce adherence to antiretroviral therapy. Therefore, UNAIDS prioritizes eliminating HIV-related stigma and discrimination to achieve the goal of ending AIDS as a public health threat by 2030. To reach this goal, it is crucial to identify the characteristics of people living with HIV and set country-specific stigma reduction targets accordingly. Furthermore, stigma level is relatively higher in developing countries, where it is critical to invest in the most effective interventions. To this end, this study aims to analyze the demographic and socio-economic determinants of HIV-related stigma in Turkey.
Methods
Design
The study was approved by the University of Health Sciences Turkey, Izmir Bozyaka Training and Research Hospital’s Local Ethics Committee with the approval number (2020-172) and date 20/05/2020. Informed consent was obtained from all participants included in the study. This cohort study of 202 PLWHA was conducted at the Izmir Bozyaka Education and Training Hospital, Department of Infectious Diseases and Clinical Microbiology (Izmir, Turkey), between June and December 2021.
In Izmir, where our cohort is based, approximately 1000 HIV/AIDS patients were recorded. HIV treatment is covered by social security in Turkey. HIV testing is compulsory for blood/organ donors and sex workers, and voluntary for pre-operative tests, before pregnancy, before applying for a health-related job, before marriage, and in health screening before taking any job. 5 Although HIV testing before starting a job is supposed to be voluntary, many people report the unofficial loss of their job after rejecting the test. Very often, job candidates face disclosure or stigma at the time of job applications. 8 Stigma and disclosure in the workplace are also affecting the employability of PLWHA.10,11
The cohort members have visited the outpatient clinic at regular intervals since their time of diagnosis. Demographic characteristics, stage of the disease, and treatment processes were obtained from the hospital files of each patient. To obtain socio-economic measures, patients were interviewed face-to-face. Any updates on other characteristics were recorded during the face-to-face interviews. The data was collected from the entire sample group. The inclusion criteria were all individuals who were HIV positive, at least 18 years old, visited the clinic at least 3 times a year, and received Antiretroviral therapy for at least 6 months (ART). Patients who were not compliant with treatment were excluded from the study. This is because HIV itself, particularly when not well managed, can lead to neurocognitive disorders, as can other conditions such as psychiatric disorders and organic diseases, which may also cause cognitive decline. The aim of this exclusion is to minimize errors in the assessment scales. We used the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) cohort checklist when writing our reports. 12
Data
We use the HIV Stigma Framework proposed by Earnshaw and Chaudoir, 13 which includes 3 dimensions of stigma: internalized, anticipated, and enacted. To measure these dimensions, we adopt the 3 stigma scales by Earnshaw et al. 14 The items for measures were adapted from previously validated scales.15,16 Table 1 depicts responses to individual items of these stigma scales.
Stigma Scales.

Note. The highest frequency (%) for each item is in bold.
The 6-item internalized stigma scale has a response format varying from (i) strongly disagree to (iv) strongly agree. The items include negative feelings and beliefs (such as feeling ashamed and unclean) associated with HIV. Mean scores indicate that participants disagree that they have internalized stigma. The frequency of “strongly disagree” items range from 23% to 48% and “strongly agree” responses range from 3% to 17%. For example, 48% of the participants strongly disagreed that having HIV is disgusting to them and 17% strongly agreed that they felt ashamed that they have HIV.
Anticipated stigma scale is a 9-item scale that assesses whether PLWHA expect discrimination and prejudice from others (for eg, avoidance and different treatment) in the future. Responses vary from (i) very unlikely to (iv) very likely. The average scores range from 1.92 to 3.39. The frequency of “very unlikely” items ranged from 10% to 49% and “very likely” items from 5% to 13%. For example, 49% of the participants thought that it is very unlikely that family members will look down on them and 13% thought that it is very likely that community/social workers will discriminate against them.
Enacted stigma scale, a 9-item scale, explores whether the person has already experienced and/or is currently experiencing such discriminative behavior from others. Responses vary from (i) never to (iv) very often. The “never” responses vary from 31% to 75% and “very often” from 0.5% to 10%. While 75% of the participants reported that family members never avoided them, 10% reported that family members looked down on them very often.
Using the 3 stigma scales, we construct 3 different indices (Internalized HIV Stigma Index [ISI], Anticipated HIV Stigma Index [ASI], and Enacted HIV Stigma Index [ESI]) for each stigma dimension. As each item is scored from 1 to 5, ISI ranges from 6 to 30, and both ASI and ESI range from 9 to 45. However, in our sample, the ISI score ranges from 6 to 29, the ASI score ranges from 9 to 24, and the ESI score ranges from 9 to 34, with higher scores indicating greater stigma. The median (p50) values are 12, 24, and 15 for internalized, anticipated, and enacted stigma indices, respectively (The mean values are 13, 24, and 16 for internalized, anticipated, and enacted stigma indices, respectively. Visual inspection of the histograms show that stigma scores are not normally distributed (Figure 1).).
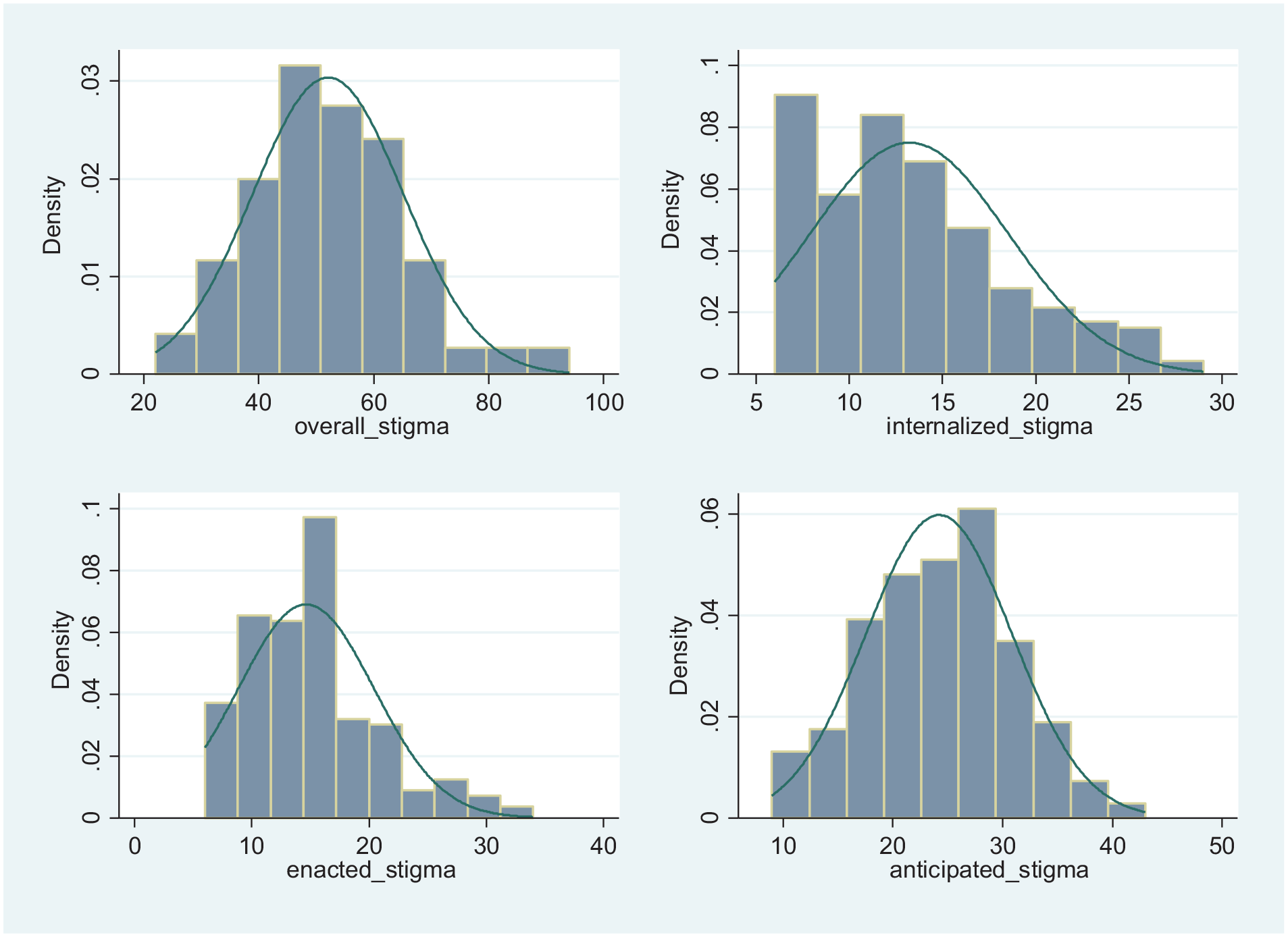
Histogram of HIV stigma indices.
Analysis
To analyze the demographic and socio-economic determinants of HIV-related stigma, we use the following logit model to examine binary outcomes of stigma (Probit model is also commonly used in binary choice models. Since the choice between the two does not make much difference, we choose the logit model for mathematical convenience (Greene, 2012).):

where
Table 2 presents the complete list of variables and summarizes the key characteristics of the sample. Pairwise correlations of these variables are reported in Table 3 indicating that there is little to no multicollinearity between the variables. The highest level of stigma is reported for internalized/perceived stigma. Participants are educated (completed high school or university), but economically disadvantaged (more than 60% earned minimum wage or less). The majority of the participants are older than 35years old (55%), single (56%), and identify as LGBT (53%). In addition, 23% of the participants have a chronic illness (such as diabetes, hypertension, cancer, and heart disease) and 13% have a CD4 count less than 200 cells/mm3 meeting the criterion for AIDS diagnosis.
Baseline Characteristics of Participants.

Enacted stigma items had non-responses; 144 participants responded to all 9 items.
Pairwise Correlations.

P < .1, **P < .05, ***P < .01.
Results
Data were analyzed using STATA 14.2. Table 4 presents the results. To calculate average marginal effects (AMEs), we first compute the marginal effect for each case and then average all the computed effects.
22
Therefore, AMEs express the average effect of an independent variable
Results, Logit.

Note. Standard errors in parentheses.
P < .1, ** P < .05, *** P < .01.
AMEs in Table 4 reveal that the factors that increase the probability that a person will experience internalized stigma are being divorced (22% higher compared to singles) and having a chronic illness (20% higher). On the other hand, age and education are negatively associated with self-stigma levels. Stigma decreases with age (42% lower for people aged 55+ compared to the youngest group) and education level (28% lower for university graduates compared to those who do not have formal education or graduated from primary school). A younger individual newly diagnosed with HIV may feel more shame or self-blame compared to older individuals who have had more time to develop coping mechanisms. Thus, younger people living with HIV can benefit from programs that promote self-acceptance and resilience. Support groups, mentorship programs with older mentors who have HIV, and counseling designed for younger individuals can help reduce stigma for this group. In addition, our results also highlight that policies that promote HIV awareness and reduce stigma in schools, along with educational campaigns aimed at the general public, could help lower stigma levels in less-educated populations.
Similarly, anticipated stigma decreases with age (40% lower for age group 35-44) and increases with marital status (divorced people anticipate 39% higher stigma).
Lastly, the probability of experiencing enacted stigma is significantly lower (47%) in the highest income group compared to that of patients earning minimum wage or less. Therefore, socioeconomic inequalities increase stigma. Initiatives to alleviate poverty and financial support programs for PLWHA could indirectly lessen their exposure to stigma. This underscores the necessity of incorporating stigma reduction strategies into wider social and economic policies. We also find that sexual orientation (LGBTs experience 14% higher stigma compared to heterosexual people), drug addiction (13% higher), and having a chronic illness (20% higher) exert a significantly positive effect on stigma level. The latter suggests the need for integrated healthcare approaches that address both coexisting health conditions and the associated stigmas. Enacted stigma is the only stigma scale that is not related to the patient’s age. We also controlled for the biological health status of patients by using CD4 levels as a predictor of stigma. Higher CD4 count is associated with lower levels of enacted stigma, as expected, but higher levels of anticipated stigma.
However, we do not find any evidence of a significant impact of gender or smoking status on any of the stigma measures.
Robustness
To check the robustness of our results, we use the 3 indices (ISI, ASI, and ESI) as indicators of HIV-related stigma. Since the dependent variables are continuous stigma scores—internalized, enacted, and anticipated stigma—we employ linear regression. We obtain similar results in these regressions (Table 5).
Results, OLS and Ordered Logistic.

Note. Standard errors in parentheses.
The cut points for the ordered logistic model are not reported, as they are not of substantive interest to the analysis. They are available upon request.
P <. 1, ** P < .05, *** P < .01.
To further enhance the robustness of the analysis, we also employed an ordered logistics regression. We created categorical stigma values based on responses to 3 stigma indices as described previously. For instance, if a patient answers “1: strongly disagree” to all 6 of the internalized stigma questions, the index value would be 6, and the corresponding categorical value would be 1. Conversely, if a patient responds “5: strongly agree” to all these questions, the index value would be 30, and the corresponding categorical value would be 5(For OLOGIT estimations: Internalized Stigma=1 if index<7, is="2" if 624; Anticipated Stigma=1 if index<10, as=”2” if 936; Enacted Stigma=1 if index<10, es=”2” if 936.). Therefore, higher values indicate greater levels of HIV-related stigma.
Moreover, pairwise correlations in Table 3 indicate that there is little to no multicollinearity between the variables. To further confirm this, we have computed the Variance Inflation Factor (VIF) in our regression model as an additional robustness check. All VIF values are below 5, reinforcing that multicollinearity is not a significant concern. 24
Thus, our results are robust for the choice of stigma measures and different estimation techniques.
Discussion
Our results show that age and marital status (divorced) are the 2 important demographic factors that affect stigmatized attitudes. Both internalized and anticipated stigma decrease with age (Figure 2). However, we do not find a significant relationship between age and enacted stigma. These results may be explained by protective factors such as self-acceptance and self-compassion that increase with age. Mature age may also provide resilience against stigma.25,26 These findings are consistent with previous studies that also found that older adults experience higher levels of internalized sigma but not enacted stigma. 27 One policy implication is the need for social support resources that “leave no one behind” and that focus on prejudice and discrimination for PLWHA of all ages.

Average stigma scores by age.
Marital status (divorced) is also an influencing factor of internalized and anticipated stigma (Figure 3). Earlier studies also find similar results for South Asia and Nepal.28,29
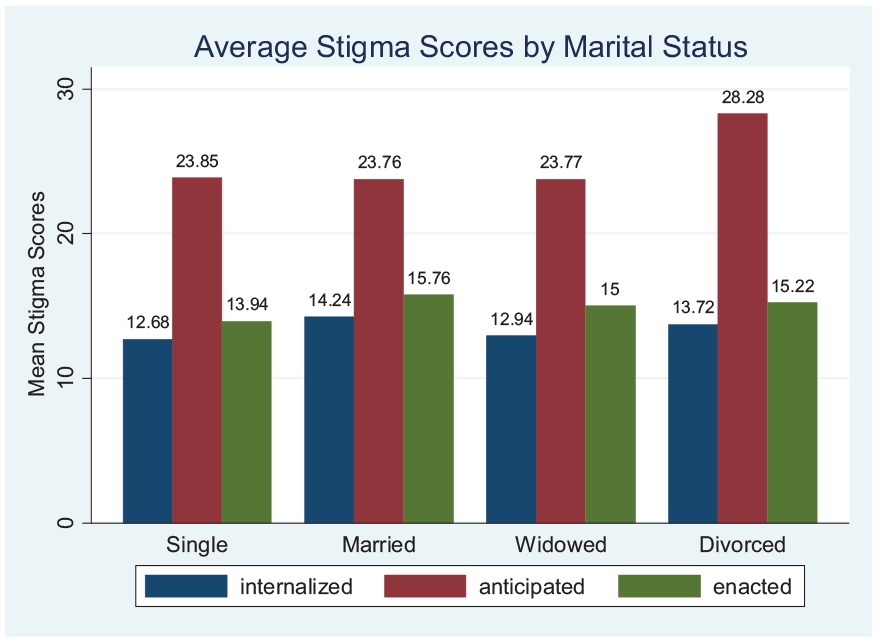
Average stigma scores by marital status.
Education and income are among the most important factors that contribute to reducing HIV-related stigma in Turkey (Figures 4 and 5). Thus, addressing socio-economic factors should be an integral part of HIV control program strategies. The finding that internalized stigma is negatively correlated with increasing education level is consistent with the literature which discuss that higher education is a protective factor against self-stigma. 30 Moreover, educated people are more knowledgeable about HIV prevention.31,32 Thus, education through the provision of information about HIV (utilizing social marketing and mass media) can be implemented as an effective intervention strategy.33 -35
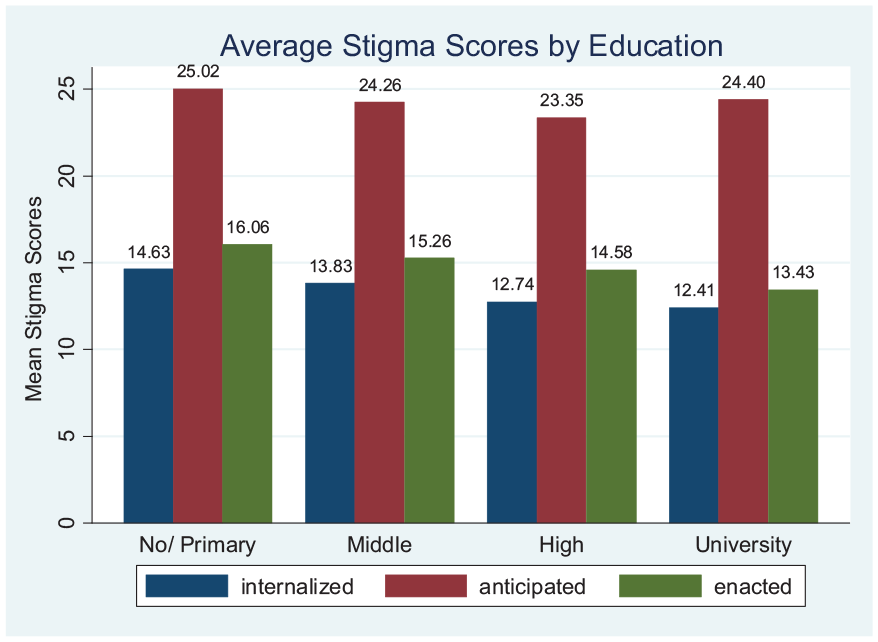
Average stigma scores by education.

Average stigma scores by income.
A higher-income level is found to be inversely associated with enacted stigma which supports the view that people with higher socio-economic status may have fewer experiences of HIV-related stigma. 36 Additionally, socio-economic inequalities increase both the perception of HIV-related stigmatizing attitudes and the use of high-cost health care.7,37
According to UNAIDS, members of key populations (sex workers, people who inject drugs, transgender people, prisoners, gay men, and other men who have sex with men) are at elevated risk of acquiring HIV infection, in part due to discrimination and social exclusion.38 -40 Similarly, people who have other chronic illnesses (such as diabetes, hypertension, cancer, and heart disease) have stigmatized identities and endorse stereotypes and prejudice associated with their chronic illness.14,41,42 Our results also reveal that LGBTs, drug users, and people who have chronic illnesses have experienced higher stigma levels (Figures 6 and 7). Our findings support previous work on stigma intersectionality, which argues that 2 or more co-existing stigmas interact to present greater oppression than their simple summation. 43 For example, people who inject drugs, men who have sex with men, or people living with sexually transmissible infections may face additional stigma related to their behavior or identity.44 -48 These results demonstrate the importance of designing social support systems for these unique groups of individuals who are disproportionately affected by HIV.
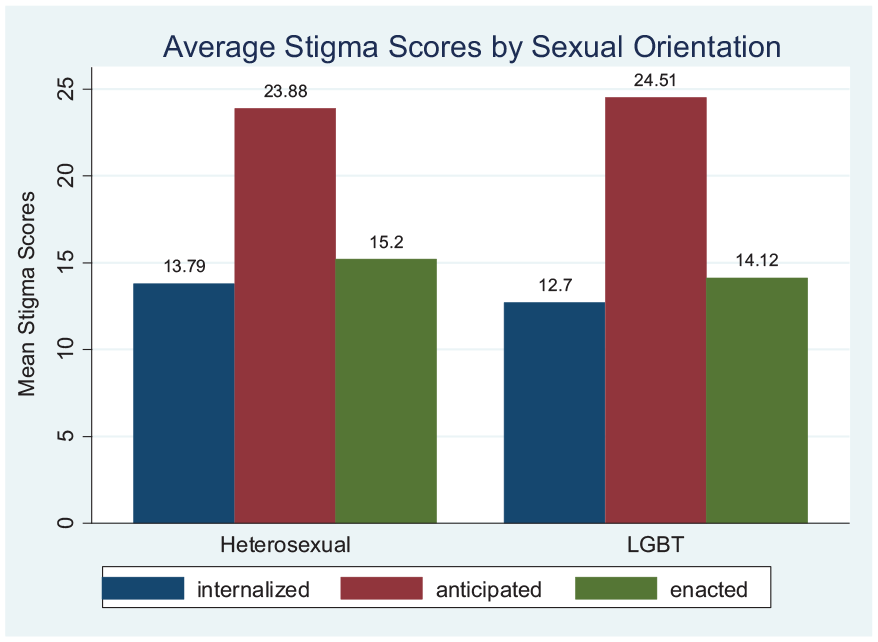
Average stigma scores by sexual orientation.

Average stigma scores by chronic illness status.
Lastly, our results reveal that better health status, as measured by CD4 count, is associated with lower levels of experienced/enacted stigma. As treatment of HIV increases productivity and the chance of employment, 8 PLWHA may experience less stigma as their health status improves. Studies also show that anticipated stigma is much more frequent than stigma previously experienced in employment and intimate relationships, 49 which explains the positive association between CD4 count and anticipated stigma.
HIV-related stigma remains a global challenge, with various studies applying the Earnshaw and Chaudoir stigma framework. Research has explored HIV-related stigma on virally suppressed individuals in Sweden, 50 HIV-related stigma within migration-related and racial stigma among Sub-Saharan African immigrants in Belgium, 51 and how HIV stigma intersects with racism, sexism, and homophobia among young adults in the U.S., 52 revealing common themes of enacted, internalized, and anticipated stigma. Overall, these findings underscore the importance of addressing stigma at individual, community, and systemic levels to enhance health outcomes for people living with HIV worldwide.
Despite the fact that HIV/AIDS exists in every culture, in Muslim countries like Turkey, it is much more pronounced. In these countries, harm reduction is underutilized as stigma prevents those at risk from seeking counseling, testing, and treatment. 53
Our findings suggest the need to develop strategies to address HIV stigma in Turkey to minimize harm reduction and control the spread of HIV. These strategies should include amending Turkey’s restrictive HIV disclosure laws as a structural intervention to reduce HIV stigma and promote safe disclosure for PLWHA. Community-led campaigns such as Undetectable = Untransmittable (U = U) involve healthcare workers and people living with HIV/AIDS (PLWHA) in reducing the number of new HIV infections. These efforts help alleviate anxiety about transmitting HIV to sexual partners and may also decrease stigma. 54
Adaptations of the Earnshaw and Chaudoir stigma framework in India highlighted the effects of cultural norms and discussed that culturally specific beliefs, such as accepting one’s fate, make education-based strategies more complicated. 55 Similarly, HIV-related stigma in Turkey is deeply ingrained in societal norms that prioritize traditional family structures and conservative cultural values. These norms often lead to misconceptions about HIV, linking it to behaviors that are viewed as socially unacceptable, such as drug use or non-heteronormative sexual orientations. Öktem 6 emphasizes the importance of family support for the well-being of people living with HIV/AIDS (PLWHA), pointing out that stigma within the family can intensify feelings of isolation and shame. This creates a challenging environment for PLWHA, where their struggle with the virus is compounded by the negative attitudes of those closest to them. Other studies also point out that family plays a crucial role in providing emotional support, which can significantly improve the quality of life of PLWH in collectivist countries like Turkey. 56
Intersectional stigma adds additional layers of challenges for certain groups, such as LGBT individuals and drug users. These individuals face multiple forms of discrimination, not only as people living with HIV/AIDS (PLWHA) but also because of their marginalized identities. Several studies highlight that effectively addressing stigma involves recognizing the interconnected systems of discrimination that influence the experiences of these populations.57,58 In Turkey, where societal attitudes toward LGBT individuals are predominantly conservative, stigma against LGBT individuals who are PLWHA is particularly pronounced.
Limitations and Future Research
One limitation of the study is that no formal power analysis was performed for sample size calculation. However, there are around 1000 PLWHA in the Izmir region where this study was conducted, so we think our sample is a good representation of the population.
Another limitation is the lack of data on socioeconomic indicators such as a person’s job security and type of occupation, which would capture the full picture of a person’s economic stability. We also lack detailed data on educational levels and gender identities. Future studies data use a more detailed dataset can explore how stigma might differ among gender-diverse populations.
Conclusion
This study analyzed the demographic and socioeconomic determinants of HIV-related stigma among 202 PLWHA in Izmir, Turkey. Our findings show that key interventions should include amending restrictive HIV disclosure laws and providing tailored protections for vulnerable groups such as divorcees, individuals with chronic illnesses, younger populations, and those with lower education levels. Policy recommendations focus on reducing poverty, offering protective measures for LGBTQ+ individuals, and addressing drug addiction inclusively. People diagnosed with AIDS face unique challenges, including higher anticipated stigma. Therefore, effective solutions must involve the meaningful inclusion of PLWHA in policy-making and intervention design.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251319926 – Supplemental material for The Impact of Socioeconomic Factors on the HIV-Related Stigma of People Living With HIV in Turkey
Supplemental material, sj-docx-1-inq-10.1177_00469580251319926 for The Impact of Socioeconomic Factors on the HIV-Related Stigma of People Living With HIV in Turkey by Hülya Özkan Özdemir, Fatma Nur Karaman Kabadurmuş and Durmuş Özdemir in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580251319926 – Supplemental material for The Impact of Socioeconomic Factors on the HIV-Related Stigma of People Living With HIV in Turkey
Supplemental material, sj-docx-2-inq-10.1177_00469580251319926 for The Impact of Socioeconomic Factors on the HIV-Related Stigma of People Living With HIV in Turkey by Hülya Özkan Özdemir, Fatma Nur Karaman Kabadurmuş and Durmuş Özdemir in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We are thankful to the participants of All Izmir Workshop in Economics 2021 for their valuable comments on earlier drafts of the manuscript. The authors acknowledge all the participating patients in the Izmir region of Turkey for their tremendous cooperation. Thanks, are also due to Ali Onur Peker for carefully transferring raw data to Excel tables.
Authors’ contributions
Durmuş Özdemir (D.Ö), Hülya Özkan Özdemir (H.Ö.Ö), Fatma Nur Karaman Kabadurmuş (F.N.K.K) designed the study. Durmuş Özdemir (D.Ö.), Fatma Nur Karaman Kabadurmuş (F.N.K.K) performed the analysis and the data. All authors read and approved the manuscript.
Data Availability
The dataset used and analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and informed consent
The study was approved by the University of Health Sciences Turkey, Izmir Bozyaka Training and Research Hospital’s Local Ethics Committee with the approval number (2020- 172) and date 20/05/2020. Informed consent was obtained from all participants included in the study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.