
Abstract
This study examined the interplay between physical workload, psychological stress, and the prevalence of work-related musculoskeletal disorders (WMSDs) among construction workers in Indonesia. This cross-sectional study used a purposive sampling technique to gather quantitative data from 409 respondents working in four construction companies through structured questionnaires. Data collection tools included the Copenhagen Psychosocial Questionnaire III (COPSOQ III), the K10 scale for psychosocial distress, and the Nordic Body Map for musculoskeletal symptoms. Independent variables encompassed demographic factors, physical work environment, and psychosocial aspects, while the dependent variable was the presence of work-related musculoskeletal disorders (WMSDs) symptoms over the past 7 days and 12 months. Descriptive statistics and logistic regression analyses were performed using IBM SPSS Statistics Grad Pack 29.0 PREMIUM. The study revealed a high prevalence of WMSDs among workers, with 36.2% reporting symptoms in the past 7 days and 31.5% in the past 12 months. These symptoms primarily affected the neck, shoulders, back, and waist. Both physical and psychosocial factors were found to the risk, with high levels of somatic stress and sleep disorders significantly increasing the likelihood of WMSDs. Psychological distress emerged as a particularly strong predictor to these disorders. The findings underscore the importance of implementing targeted interventions and safety policies to mitigate WMSDs risks and improve occupational health within the construction industry.
In Indonesia’s construction sector, WMSDs are prevalent due to ergonomic challenges and psychosocial stressors, affecting both health and productivity.
His study identifies physical and psychosocial factors contributing to WMSDs in construction workers, with logistic regression analysis revealing their prevalence and impact.
The findings advocate for integrated ergonomic and stress management interventions while outlining future research on longitudinal effects and industry-specific guidelines.
Introduction
The construction sector plays a crucial role in driving economic growth by creating employment opportunities and supporting the performance of other industries. As a significant contributor to a country’s Gross Domestic Product (GDP), global construction expenditure accounted for 13% of GDP in 2020, with projections suggesting this proportion will exceed 13.5% 2030. 1 In Southeast Asia, the construction sector is poised to reach a valuation of $450.1 billion by 2023, with steady annual growth rate of 4.9%. 2
In the region, Indonesia’s construction sector is the largest and serves as a cornerstone for infrastructure development, contributing significantly to the nation’s economic growth and global competitiveness. Prior to the COVID-19 pandemic, the construction sector accounted for 10.53% and 10.73% of Indonesia’s GDP in 2018 and 2019, respectively. 3 While the sector experienced a decline in 2020 due to the pandemic, the number of registered permanent workers continued to increase, from 880 146 workers in 2009 to 1 158 493 workers inc2022. 4 The actual workforce is likely even larger. As of 2023, Indonesia had 190 677 construction companies, with the majority (157 322) being small companies, followed by 31 413 medium-sized companies and 1942 large companies. 5
Despite its size and important socioeconomic contributions, the Indonesian construction industry experience a high rate of occupational incidents. A study analyzing incidents between 2012 and 2014 revealed that building projects had the highest incidence rates, with electrocution, falls from height, and being struck by objects as the most common types of incidents. These were largely attributed to frequent unsafe acts and conditions. The majority of incidents were categorized as fatal (68%), serious (16%), or catastrophic (14%). 6 Additionally, Furthermore, the sector suffers from a notable lack of safety research and implementation, contributing to over 30% of all recorded occupational injuries. Key issues include conflicts between production demands and safety priorities, inadequate safety communication, and acceptance of poor safety as the norm. 7
Among the many safety hazards faced by construction workers, a serious concern is the association between the demanding nature of their work and the heightened risk of work-related musculoskeletal disorders (WMSDs). 8 WMSDs refer to various conditions that affect the muscles, bones, tendons, ligaments, and other parts of the musculoskeletal system. Globally, the construction industry is notorious for its high prevalence of WMSDs, with approximately 80 000 construction workers reporting work-related illnesses, annually, over 50 000 of which are attributed to WMSDs, especially in the back, shoulders, and neck. 9 In the United States, WMSDs remain significantly higher in the construction sector compared to other industries, despite some improvements. 10 Similarly, studies from Sweden, South China, Pakistan, and Malaysia have consistently highlighted the global nature of this issue, reporting high rates of WMSDs across various construction roles and regions.8,11 -13 In addition, ergonomic challenges such as awkward postures, heavy lifting, force exertion, exposure to vibrations, and repetitive motions contribute to the physical strain experienced by construction workers. 14 Tasks involving manual handling of heavy objects, prolonged strenuous postures, and repetitive movements, especially in the hand-arm system, further elevate the risk of injuries. 15 Repetitive movement is another factor that tends to lead to a higher risk of injuries, especially in the hand-arm system. It is paramount for construction workers to be cognizant of these factors and proactively implement measures to mitigate physical stress and reduce the incidence of WMSDs.16,17
Construction workers face not only experience physical strain but also significant psychological strain, which contributes to the prevalence of WMSDs. 18 Research indicates a strong relationship between psychological factors and musculoskeletal health. For instance, workplace stress can exacerbate the severity of WMSDs symptoms, negatively affecting mental health and reducing work capacity. 19 Job stress has also been shown to trigger WMSDs, which in turn intensify stress level and diminish health-related quality of life. 20 Several studies in the construction industry,21 -23 have highlighted the complex relationship between physical and psychological strain and WMSDs, underscoring the importance of addressing both aspects for to effectively prevent and manage these conditions. Shift work is another critical factor exacerbating both physical and psychological health issues, including WMSDs, among construction workers. It disrupts sleep patterns, increases fatigue, and elevates stress, all of which contribute to musculoskeletal problems. Research show that shift workers are more vulnerable to mental health issues and chronic illnesses, which further amplify their physical strain. Therefore, acknowledging and addressing the impact of shift work is essential for understanding and mitigating WMSDs in the construction industry.24,25
Based on those situations, this research aims to examine the relationship between physical workload, psychological stress, and the occurrence of WMSDs among construction workers in Indonesia. Specifically, it will (1) analyze the incidence and types of WMSDs in the industry, (2) identify which workers and job roles are most at risk, and (3) investigate the key ergonomic and physical factors, such as work posture, manual handling, and job-related stress, that contribute to these disorders. Additionally, the study explores the role of psychosocial factors, including high job demands and stress, in exacerbating WMSDs and affecting worker health. The findings are expected to inform the development of targeted interventions and policies aimed at improving health and safety standards in the Indonesian construction sector, fostering sustainable practices, and enhancing worker welfare.
Materials and Methods
Research design and participants
This study utilized a cross-sectional research design, which is suitable for assessing the prevalence of WMSDs and identifying the factors associated with them at a specific point in time. The target population comprised 696 construction workers, both white-collar (construction professionals) and blue-collar (tradespeople and operators). Purposive sampling was employed to select participants who met the inclusion criteria, ensuring that the sample aligned with the study’s objectives. The sample size was determined using Slovin’s formula, with a 5% margin of error, 26 yielding a minimum required sample size of 254 workers.

Where:
N is the total population (696 workers)
e is the margin of error (set at 5%)
Workers who had been employed for at least 6 months with their current employer and had no prior history of musculoskeletal complaints at the time of recruitment were eligible for inclusion in the study. Conversely, workers with a history of musculoskeletal complaints or those employed for less than 6 months were excluded. Out of 430 workers were recruited, 409 met the inclusion criteria and were included in the final analysis.
To ensure the confidentiality, the survey was conducted anonymously, preventing employers from accessing any details of the participating employees. Eligible employees were given the option to decline participation without facing any repercussions. Prior to data collection, participants provided informed consent after being briefed on the study’s purpose and procedures. Data were collected using Indonesian structured questionnaires administered between July 2023 and January 2024 in a controlled environment to ensure consistency. Trained researchers were present to address any questions, minimizing potential biases associated with self-reporting.
Ethical approval for this study was granted by the Research and Community Engagement Ethical Committee of the Faculty of Public Health at Universitas Indonesia (approval number: 597/UN2.F10.D11/PPM.00.02/2023). The study adhered to key ethical principles, including justice (ensuring fairness and equal treatment), non-maleficence (preventing harm), beneficence (maximizing benefits), and autonomy (respecting voluntary participation). These principles ensured participant safety and meaningful contributions to both the participants and the wider community. 27 Additionally, this study followed the STROBE guidelines for reporting observational studies, and the completed checklist has been included as a Supplementary File.
Research Instrument
In this study, the dependent variable was the presence of WMSDs symptoms reported in the past 7 days and 12 months, assessed using the Nordic Body Map Questionnaire. The independent variables included demographic information (eight items), physical and work environment factors (10 items), psychosocial aspects (eight items), and musculoskeletal disorder complaints (28 items).
The physical and work environment factors identified in this study included maximum load lifted or carried, duration of maximum load, maximum load lifted with one hand, muscle exertion, exposure to vibration, vehicular operation, task completion difficulty, work posture (covering average postures such as working with overhead objects, kneeling, bending, squatting, neck flexion, and reaching). Dynamic tasks (standing) and static tasks (sitting) were also evaluated. The physical and environmental survey tool was adapted from two well-established instruments, namely the Quick Exposure Check (QEC) and the Rapid Entire Body Assessment (REBA). Both QEC and REBA are widely recognized and validated tools for assessing ergonomic risks and physical strain in workplace settings.28,29 The QEC focuses on evaluating workers’ postures, movements, and tasks in relation to musculoskeletal risks, while REBA assesses whole-body postural risks associated with different job activities.
The Copenhagen Psychosocial Questionnaire III (COPSOQ III) was utilized to evaluate various psychosocial factors, 30 while psychosocial distress was measured using the K10 scale, which ranges from “Never” to “Every time,” providing insights into participants’ psychological well-being. 31 The Indonesian version of the Copenhagen III questionnaire was used in this study, which has been validated and tested for reliability. The Cronbach’s alpha for the questionnaire was .844, indicating high reliability, and the validity test produced r-values ranging from .396 to .947, all exceeding the critical r-table value of .3494. 32
Lastly, participants were asked to evaluate their WMSDs symptoms over the past 7 days and 12 months using the Nordic Body Map Questionnaire. This questionnaire utilized a rating scale ranging from “Not at all” to “Frequent” to assess symptom severity across 28 body regions, including both the right and left sides of the body 33 Participants identified the severity of symptoms for each relevant body region. The Nordic questionnaire demonstrated validity, strong psychometric properties, with item validity ranging from .501 to .823 and a reliability coefficient confirmed by a Cronbach’s alpha of .726. 34 The WMSDs variable was categorized by summing the Likert scale responses and calculating the average score, which served as a threshold to classify participants into low-risk and high-risk categories.
Data Analysis
Univariate analysis was performed using frequency percentages to describe the data distribution. Bivariate analysis was conducted using chi-square tests to analyze associations between WMSD symptoms (7 days and 12 months) and various characteristics, including demographic factors, physical and work aspects (eg, manual handling, duration of manual handling, and exposure to vibration through work equipment), and psychosocial aspects (eg, emotional demands, role clarity, and cognitive stress). In the multivariate analysis, multiple logistic regression with the backward Logistic Regression( LR) method was used to applied the factors most influencing WMSDs symptoms over 7 days and 12 months. Odds ratios (ORs) were calculated, with values below 1 indicating protective factors and values above 1 indicating risk factors. All analyses were performed using IBM SPSS Statistics Grad Pack 29.0 PREMIUM.
Results
A total of 409 respondents participated in this study. The majority were male (98.3%) and blue-collar workers (78.0%). Most respondents were non-permanent employees (93.2%) with low educational attainment (88.0%), defined as having completed high school or below (Table 1).
Demographic and Employment Characteristics of Respondents.

A significant proportion of respondents engaged in manual lifting with varying loads, with 30.8 performing manual handling of very heavy loads (>20 kg). Workers reported adopting various work positions, including bending (67.7%), kneeling (52%), squatting (61.10%), or standing (90.50%).
Around 54.5% of respondents reported experiencing high physical work demands and cognitive stress, while 52.6% experienced somatic stress, 51.6% reported sleep disorders and 45% indicated low role clarity.
WMSDs symptoms were identified as high risk by 36.2% of respondents over the past 7 days and by 31.5% over the past 12 months (Table 2). Table 3 presents the body regions affected, with the waist and back emerging as the most frequently reported areas for WMSD symptoms during both time periods.
Prevalence of WMSDs in 7 Days and 12 Months.

Prevalence of WMSDs Symptoms by Body Region Over the Last 7 Days and 12 Months.

The chi-square analysis results presented in Table 4 revealed significant relationships between various factors and the risk of WMSDs. Employees from Construction B and Construction C exhibited significantly lower risks compared to those from Construction A and Construction D. Younger workers, particularly those under 25 years of age, were found higher risks of WMSDs compared to older workers in the 35 to 40 years and above 40 years age group. Workers with less work experience (≤6 years) were found to have a higher risk of WMSDs. Physical work aspects, such as high manual lifting loads, extended durations of manual lifting tasks, and task requiring high muscle strength were significantly associated with increased WMSDs risks. Psychosocial factors, including high emotional demands, somatic stress, cognitive stress, and sleep disorders, were also strongly linked to elevated WMSDs risks. Psychological distress emerged as the most influential factor for both 7-day and 12-month WMSDs, with odds ratios (OR) of 12.908 for WMSDs over 7 days and 16.008 for WMSDs over 12 months as shown in Table 4.
Characteristics and Risk Factors Associated with WMSDs Over the Last 7 Days and 12 Months.

Bold entries in table indicate p-values < 0.005, signifying statistically significant associations.
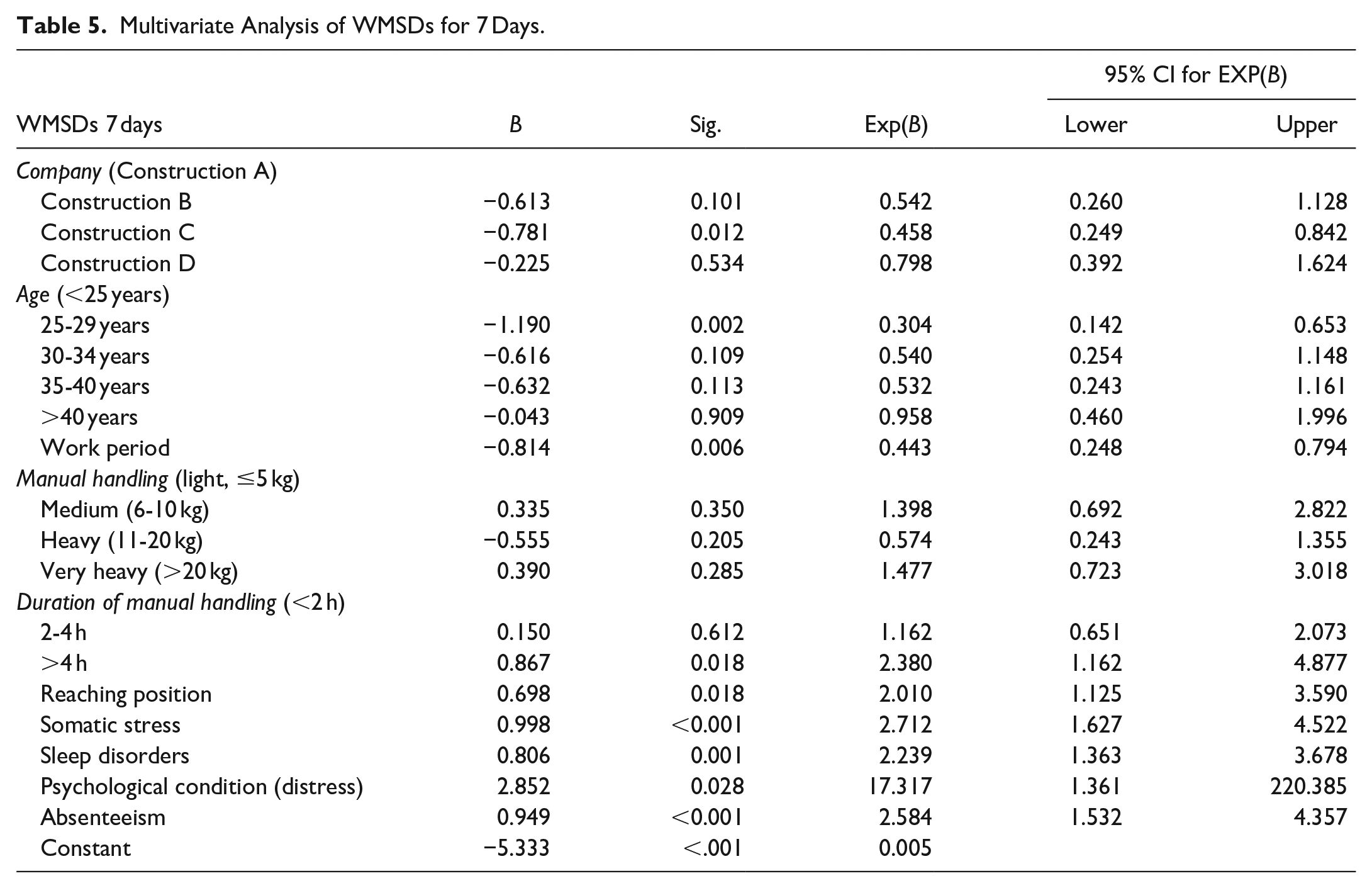
The multivariable analysis identified significant predictors of WMSDs over both 7-day and 12-month periods. These findings highlight the importance of examining diverse factors influencing WMSDs. Younger workers were found to have higher risks, while employees from companies like Construction B exhibited lower WMSDs risk. High somatic stress and sleep disorders were significant contributors to WMSDs risks, with psychological distress emerging as a particularly strong predictor. Workers with prior absences due to complaints were also at significantly higher risk. Additionally, lack of role clarity was identified as a key factor in the 12-month analysis, as shown in Tables 5 and 6 respectively.
Multivariate Analysis of WMSDs for 7 Days.
Multivariate Analysis of WMSDs for 12 Months.

Discussion
The study highlights critical findings on the risk of WMSDs among construction workers. Among the 409 participants, the majority were men and blue-collar workers, reflecting the characteristics of the Indonesian construction industry, which remains predominantly male-dominated and composed largely of workers with low educational backgrounds, particularly in trades and operator roles. Most respondents were under 40 years old, a significant proportion being young workers (less than 25 years old). In Indonesia, employment in the construction sector is often seen as a pathway to escape poverty, especially for individuals without formal education or specialized skills. 35
This research found that construction workers commonly experienced WMSD symptoms in areas such as the neck, shoulders, back, and waist. These findings are consistent with prior studies indicating that WMSDs predominantly affect the neck, shoulders, and lower back in the construction sector. 8 Specific job tasks identified in this study that contribute to these health issues include prolonged periods in uncomfortable positions, repetitive motions, and lifting heavy objects. Similarly, numerous studies have demonstrated that awkward postures, work at shoulder height, heavy lifting, and repetitive movements of the hands and wrists significantly increase the risk of neck and upper limb disorders.36,37
Our study further highlights that both the physical and psychosocial aspects of work significantly contribute to the risk of WMSDs. Construction workers often engage in physically demanding tasks, such as manual handling and maintaining strenuous body postures, which can lead to WMSDs. These finding align with previous studies indicating that the physically demanding nature of construction work, including frequent task repetition, uncomfortable working positions, and handling heavy objects, is a primary cause of pain and discomfort.8,38 In addition, psychosocial factors such as emotional stress, somatic stress, and sleep disturbances were also associated with an increased risk of WMSDs. This study is consistent with prior research showing that psychological factors are significant risk contributors to WMSDs in construction.39,40 Furthermore, four key work environment factors, including high job demands, limited control over decisions, lack of social support, and job uncertainty, were identified as drivers of increased stress, which in turn raises the risk of health problems. 41
Our findings on the relationship between physical and psychological strain and WMSDs are consistent with Karasek’s Job Demand-Control Model, which posits that jobs with high demands and low control are associated with elevated stress levels, increasing the risk of health issues such musculoskeletal disorders. 42 This model is particularly applicable to the construction industry, where workers encounter significant physical demands (eg, heavy lifting, awkward postures) coupled with limited control over job conditions. The high levels of somatic and sleep-related stress observed in this study further supports this framework, as psychological strain intensifies physical symptoms, perpetuating a cycle of increased WMSD risk. 41
Comparatively, our findings align with studies conducted in both developed and developing countries. For example, Reddy et al 37 reported a similar prevalence of WMSDs among construction workers in India, with lower back and shoulder pain being dominant, which mirrors the neck, back, and waist complaints observed in our study. Similarly, Holmström and Engholm 11 found that scaffold workers in Sweden experienced high rates of musculoskeletal issues due to the physically demanding nature of their tasks, consistent with our findings on the risks associated with awkward postures and manual handling. Additionally, Lee et al 8 observed similar patterns in South China, where psychological distress was significantly linked to increased WMSDs symptoms, underscoring the critical interplay between physical and mental health in occupational settings.
The connection between WMSDs and psychological factors, such as job stress and sleep disturbances, is well-documented in the literature. Jeong and Lee 20 reported that WMSDs are closely linked to occupational stress, which can both trigger and worsen their symptoms. This align with our findings, which indicate that workers experiencing high levels of psychological distress, especially younger workers, are more likely to report WMSDs symptoms. These comparison across these diverse contexts suggests that while specific risk factors may vary by region, the underlying mechanisms linking physical and psychological strain to WMSDs remain consistent across construction environments globally.
This study also found that younger workers, particularly those under 25 years old, experience a higher incidence of WMSDs. This may be attributed to expectations that younger workers perform harder and more physically demanding tasks. They are often assigned roles requiring greater physical exertion, which could explain their increased risk of WMSDs. In contrast, older workers tend to exhibit a lower risk, possibly due to their accumulated experience and familiarity with safer work practices. This aligns with prior research associating physical hazards during adolescence to musculoskeletal development, with risks potentially exacerbated by insufficient skills and knowledge.8,43 Additionally, differences in the characteristics of construction companies were found to influence WMSD risk. This highlights the critical role of an organization’s safety policies, procedures, and management systems in mitigating the occurrence of WMSDs. Specifically, this study reveal notable differences in WMSD risks among companies, with Construction Company B and C demonstrating lower risks than others. This may be attributed a strong safety culture, including the implementation of effective safety policies, regular training, and improved communication regarding occupational health and safety. 44 Further research is needed to explore the relationship between safety climate, safety culture, and the prevalence of WMSDs.40,44 Understanding the impact organizational factors on worker health can provide valuable insights for developing more effective policies to enhance workplace safety in the construction sector.
Interestingly, despite the expectation that blue-collar workers, who engage in more physically demanding tasks, would exhibit higher rates of WMSDs, our findings revealed a similarly high prevalence among white-collar workers. This can be attributed to the different risk factors white-collar workers face such as prolonged sitting, poor workstation ergonomics, and static postures during computer-based tasks. These factors are known to contribute to musculoskeletal issues, particularly in the neck, shoulders, and lower back. Research has shown that sedentary work, especially without proper breaks and ergonomic support, can result in musculoskeletal strain comparable to that experienced in physically demanding labor.45,46 Thus, while the nature of physical exertion differs between white-collar and blue-collar workers, both groups are at risk of developing WMSDs due to the specific of their work environments.
These findings have significant implications for improving health and safety in the construction sector. Notably, there is a critical need to raise awareness among construction workers regarding the risks associated with WMSDs. Implementing effective ergonomic practices, such as training on proper postures, using mechanical aids to reduce physical strain, and redesigning workspace to align with ergonomic principles, can be adopted across countries to reduce WMSD risks. Additionally, prioritizing comprehensive training programs that address stress management, mental health support, and flexible work policies is essential for alleviating the psychosocial pressures that often exacerbate musculoskeletal disorders. These results highlight the need for integrated strategies that combine physical and psychological approaches to foster safer and healthier work environments across different construction industry settings. In developing countries, where challenges are heightened by resource constraints and limited awareness, these strategies are particularly critical. This study significantly contributes to our understanding of the multifaceted factors influencing WMSD risks in construction, providing a strong foundation for the development of targeted interventions aimed at reducing work-related musculoskeletal injuries.
The limitations of this study include the potential for bias in self-reported and subjective measures, which may affect the accuracy of the findings. Additionally, the sample was restricted to online participants from four construction companies, limiting the generalizability of the results. The study also did not account for specific task variations within the construction field, such as differences between manual handling and calculation tasks. Moreover, confounding factors were not comprehensively examined, as the analysis focused solely on predictors. The study also did not account for specific task variations within the construction field, such as differences between manual handling and calculation tasks. Moreover, confounding factors were not comprehensively examined, as the analysis focused solely on predictors. Potential recall bias is another consideration, given the high similarity between WMSDs reported over the past 7 days and 12 months, particularly among respondents experiencing multiple aches and pains. While content validity was established through expert review, future studies should include reliability testing to ensure the consistency of the questionnaire across various contexts. To address these limitations, further research with larger, more diverse samples across different regions and advanced analytical techniques is needed for a more comprehensive understanding of the factors influencing WMSDs.
Conclusion
In conclusion, this study highlights the widespread prevalence of WMSDs in the Indonesian construction sector, particularly affecting areas such as shoulders, back, and waist. It underscores the urgent need for comprehensive occupational health interventions that address both physical ergonomic improvements and the management of psychological stressors. Integrating safety protocols, ergonomic practices, and mental health support is critical for reducing WMSD prevalence and enhancing overall worker well-being. Moving forward, policymakers and industry leaders should prioritize these holistic approaches to foster a safer and healthier work environment. Future research should explore the long-term impacts of such interventions across diverse construction settings and examine how factors such as shift work and organizational culture influence WMSDs. Such efforts are vital for promoting sustainable work practices and improving worker productivity in the global construction industry.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251315348 – Supplemental material for Impact of Physical and Psychological Strain on Work-Related Musculoskeletal Disorders: A Cross-Sectional Study in the Construction Industry
Supplemental material, sj-docx-1-inq-10.1177_00469580251315348 for Impact of Physical and Psychological Strain on Work-Related Musculoskeletal Disorders: A Cross-Sectional Study in the Construction Industry by Abdul Kadir, Riza Yosia Sunindijo, Baiduri Widanarko, Dadan Erwandi, Sjahrul M. Nasri, Bangga Agung Satrya, Stevan Deby Anbiya Muhamad Sunarno, Hardy Atmajaya, Popy Yuniar, Tubagus Dwika Yuantoko, Lailatul Qomariyah and Cynthia Febrina Maharani in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580251315348 – Supplemental material for Impact of Physical and Psychological Strain on Work-Related Musculoskeletal Disorders: A Cross-Sectional Study in the Construction Industry
Supplemental material, sj-docx-2-inq-10.1177_00469580251315348 for Impact of Physical and Psychological Strain on Work-Related Musculoskeletal Disorders: A Cross-Sectional Study in the Construction Industry by Abdul Kadir, Riza Yosia Sunindijo, Baiduri Widanarko, Dadan Erwandi, Sjahrul M. Nasri, Bangga Agung Satrya, Stevan Deby Anbiya Muhamad Sunarno, Hardy Atmajaya, Popy Yuniar, Tubagus Dwika Yuantoko, Lailatul Qomariyah and Cynthia Febrina Maharani in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-3-inq-10.1177_00469580251315348 – Supplemental material for Impact of Physical and Psychological Strain on Work-Related Musculoskeletal Disorders: A Cross-Sectional Study in the Construction Industry
Supplemental material, sj-docx-3-inq-10.1177_00469580251315348 for Impact of Physical and Psychological Strain on Work-Related Musculoskeletal Disorders: A Cross-Sectional Study in the Construction Industry by Abdul Kadir, Riza Yosia Sunindijo, Baiduri Widanarko, Dadan Erwandi, Sjahrul M. Nasri, Bangga Agung Satrya, Stevan Deby Anbiya Muhamad Sunarno, Hardy Atmajaya, Popy Yuniar, Tubagus Dwika Yuantoko, Lailatul Qomariyah and Cynthia Febrina Maharani in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We extend our gratitude to the Occupational Health, Safety, and Environmental Unit at Universitas Indonesia for their invaluable assistance throughout the duration of this study, with special recognition to Endah, Aini Attahiroh, Syaiful, Boan, and Tomy. Additionally, we would like to acknowledge the contributions of our fellow students Cindy Patricia Yosika, Salwa Fadhilah, Fathan Ramadhan Ismail, Adysty Safira Salma, Maharani Ayundhias, Muhammad Sayyid Hasan, Muhammad Schehan Al Azhar, Muhammad Athif Iszuhri, Puti Intan Sari, Salma Qonita Thifal, Haikal Muhammad Ariq, Zahratunnisa, and Gianina Afiqah Putri, who served as enumerators during the data collection phase.
Author Contributions
Conceptualization, A.K. and R.Y.S, B.W.; methodology, A.K., D.E., S.M.N.; software, A.K., B.A.S., S.D.A.M, H.A.; validation, A.K., H.A, P.Y. and T.B.Y.; formal analysis, B.A.S, A.K., L.Q., C.F.M.; investigation, A.K, H.A., ; resources, H.A.; data curation, R.Y.S, B.W., D.E.; writing—original draft preparation, all authors ; writing—review and editing, all authors; visualization, A.K., B,A,S; supervision, A.K., B.W., D.E., S.M.N.; project administration, H.A; funding acquisition, A.K. All authors have read and agreed to the published version of the manuscript.
Data Availability Statement
The data cannot be made available to the public due to confidentiality measures mandated by the Ethics Committee at Public Health, Universitas Indonesia. However, the datasets utilized or examined in this study can be accessed from the corresponding author upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is fully funded by the Directorate of Research and Development Universitas Indonesia under Hibah Publikasi Terindeks Internasional (PUTI) No.NKB-709/UN2.RST/HKP/05.00/2023.
Ethical Consideration
Prior to data collection, participants provided informed consent after being briefed on the study’s purpose and procedures. Ethical approval for this study was granted by the Research and Community Engagement Ethical Committee of the Faculty of Public Health at Universitas Indonesia (approval number: 597/UN2.F10.D11/PPM.00.02/2023).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.